Abstract
Background: ABL1 tyrosine kinase inhibitor discontinuation securely became among the therapeutic goal for chronic myeloid leukemia chronic phase patients (CML-CP). To establish successful prognostic factors for treatment-free remission (TFR), it is necessary to diagnose the patients with high-risk molecular relapse, however, a biomarker for the achievement of TFR has not been completely elucidated. Recent investigations have determined that neutrophils function crucially in cancer immunology. Patients and Methods: The research was a multicenter retrospective observational study to examine the correlation between TFR and neutrophil counts before TKI discontinuation. The investigation included patients having Philadelphia chromosome-positive CML-CP who attempted the discontinuation of TKIs after a durable deep molecular response between January 2012 and July 2021 at four institutions in Japan. Results: 118 CML-CP patients in total discontinued TKIs and an estimated 36-month TFR rate was 65.1%. 52 patients received second-generation TKIs as frontline. Higher neutrophil count (>3210/μL) at TKIs discontinuation was determined as an independent prognostic variable for TFR in patients who received second-generation TKIs as frontline [(HR, 0.235 (95%, confidence interval (CI) 0.078–0.711); p = 0.010]. Conclusions: The neutrophil-mediated immunomodulation can be a significant component for the effective achievement of TFR in CML supported by our clinical observation.
1. Introduction
The introduction of ABL1 tyrosine kinase inhibitors (TKIs) has provided a favorable life expectancy for patients with chronic myeloid leukemia (CML-CP) similar to that of the general populations [1]. However, late adverse events (e.g., cardiovascular events and renal dysfunction) and high-medical costs have become a new medical issue due to long-term TKIs treatment. Stop Imatinib (STIM) study which was a pioneering TKI discontinuation study revealed 41% of the patients who achieved a durable deep molecular response (DMR; complete molecular response at that time) for at least 2 years maintained treatment free remission (keeping DMR) [2]. The A-STIM study revealed a trigger for resuming imatinib after the loss of major molecular response (MMR) was sufficient, then the loss of MMR was defined as a molecular relapse after imatinib discontinuation [3]. Next, first-line or second-line second-generation TKI discontinuation studies were reported. The results were similar to the TKI discontinuation study with imatinib [4,5,6,7]. These TKI discontinuation studies indicated that approximately half of the patients who attained a durable deep molecular response (DMR) could halt TKIs without molecular relapse [2,3,4,5,6,7,8], hence TKI discontinuation became among the therapeutic goals for CML-CP patients [9]. To establish successful prognostic factors for TFR, it is necessary to determine the patients who are high-risk molecular relapses, still, biomarkers for the achievement of TFR have been incompletely elucidated due to a lack of comprehensive assessment to diagnose the prognostic factors for TFR in CML.
Longer TKI treatment duration [2,8,10], longer DMR duration [8,11], lower BCR::ABL1 transcript levels [12,13], a lower Sokal score [2,4], higher natural killer (NK) cell counts at TKIs discontinuation [14,15], presence of withdrawal syndrome [10] may be a favorable prognosis factor for successful achievement of TFR. On the other hand, resistance to prior TKIs [4,5], e13a2 BCR::ABL transcript type [16] and higher regulatory T cell counts [17] may be associated with unfavorable prognostic factor.
Various shreds of evidence indicate that CML is sensitive to immunotherapy, including interferon α, allogeneic hematopoietic stem cell transplantation, and donor lymphocyte infusion, hence cancer immunosurveillance against CML is necessary to avert the relapse of patients with CML-CP. NK cells and T lymphocytes (T cells) are key components of the human immune system against viruses or cancers [18].
Recent studies have identified neutrophils also function critically in cancer immunology, although neutrophils are commonly known to function as antibacterial [19]. We earlier reported that higher neutrophil counts were a favorable prognostic factor for TFR in CML-CP patients [20]. The investigation was developed as a single center, retrospective analysis. We analyzed the association between neutrophil count and TFR outcome in patients with CML-CP.
2. Materials and Methods
2.1. Study Design and Patients
The research was a multicenter retrospective observational study to examine the correlation between TFR and neutrophil counts before TKI discontinuation. The investigation included patients having Philadelphia chromosome-positive CML-CP who attempted the discontinuation of TKIs (imatinib, dasatinib, nilotinib, or bosutinib) after a durable DMR between January 2012 and July 2021 at four institutions in Japan (Chiba University, Chiba, Japan; Hamamatsu University School of Medicine, Shizuoka, Japan; Nihon University School of Medicine, Tokyo, Japan; Oita Prefectural Hospital, Oita, Japan). CML was diagnosed following the World Health Organization classification of myeloid neoplasms and acute leukemia [21].
Baseline patient characteristics were obtained from hospital records such as general characteristics (age and sex), type of TKIs, laboratory data (complete white cell counts, neutrophil counts, and lymphocyte counts, molecular diagnosis (BCR::ABL1 mRNA transcript level), and Sokal risk score. The final follow-up date was 31 July 2021.
The clinical research was approved by the Institutional Review Board of each participating hospital (2021-12-R-04). Earlier published data was employed as control [20]. Two expert hematologists (HU and KK) reviewed all clinical data. All techniques involving human participants were undertaken following the principles of the Declaration of Helsinki. Informed consent was acquired by the opt-out method; information on the study, including the use of specimens objectives and the opportunity to opt-out, was made public, and no patients made objections.
2.2. Definition of Molecular Responses and Molecular Relapse
Molecular responses were defined based on BCR::ABL1 mRNA transcript levels by real-time quantitative-PCR (RQ-PCR) applying the international scale. A major molecular response (MMR) was defined as a BCR::ABL1 mRNA transcript level of ≤0.1%, MR4.0 was defined as ≤0.01%, MR4.5 was defined as ≤0.0032%, and undetectable minimal residual disease (UMRD) was defined as undetectable BCR::ABL1 mRNA transcript level. DMR was defined as MR4.0 or a deeper response, and molecular relapse was determined as loss of the MMR.
2.3. Statistical Analysis
The cumulative incidence of TFR was calculated by the Kaplan-Meier method and differences were assessed using the log-rank test. Cox’s proportional hazard model was employed to examine the association between TFR and each of the variables (All variables (continuous variables were dichotomised at median values), and two-sided p values < 0.05 were considered statistically significant. Statistically significant differences between three or more groups or variables were determined using the one-way ANOVA and the Bonferroni was used as multiple pairwise tests. The Mann–Whitney U test was utilized to determine statistically significant differences between the two groups. A comparison of clinical features was performed using Fisher’s exact test. All statistical analyses were conducted using EZR (ver. 1.61, Saitama Medical Center, Jichi Medical University), a graphical user interface for R [22].
3. Results
3.1. Patient Characteristics
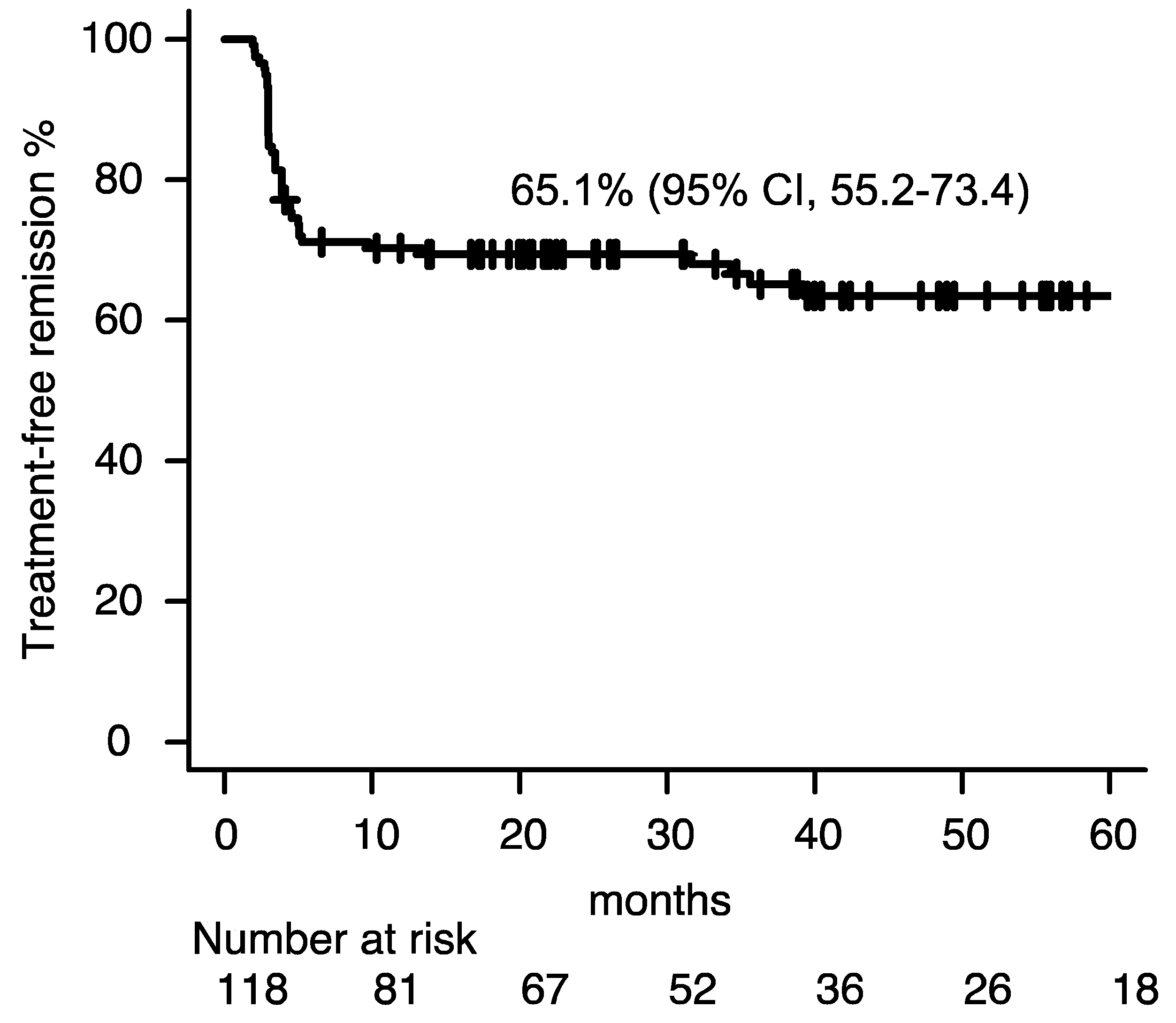
In total, 118 CML-CP patients discontinued TKIs. The median age was 60 years [interquartile range (IQR): 47–68 years)]; 71 patients were male and 47 were female; 44, 42, and 15 patients had low, intermediate, and high Sokal risk scores, respectively (17 patients had missing data). The frontline TKI was imatinib in 66 cases, dasatinib in 21, nilotinib in 21, and bosutinib in six. The TKIs at discontinuation was imatinib in 43 cases, dasatinib in 37, nilotinib in 37, and bosutinib in five; 83 patients were on a frontline TKI at TKI discontinuation (imatinib, 42; dasatinib, 17; nilotinib, 20 and bosutinib, 4). The duration of the DMR time and median TKI treatment duration was 49.0 months (IQR: 33.2–59.2 months), and 98.8 months (IQR: 62.3–136.8 months), respectively. An estimated 36-month TFR rate was 65.1% [95% confidence interval (CI), 55.2–73.4, Figure 1)] and the median follow-up time for TFR was 39.3 months (IQR, 20.5–62.2). Median white blood cell (WBC) count, neutrophil count, and lymphocyte count at TKI discontinuation were 5800/μL (IQR, 4708–7178), 3210/μL (IQR, 2656–4303) and 1685/μL (IQR, 1131–2181), respectively. Table 1 summarizes the detailed clinical characteristics.
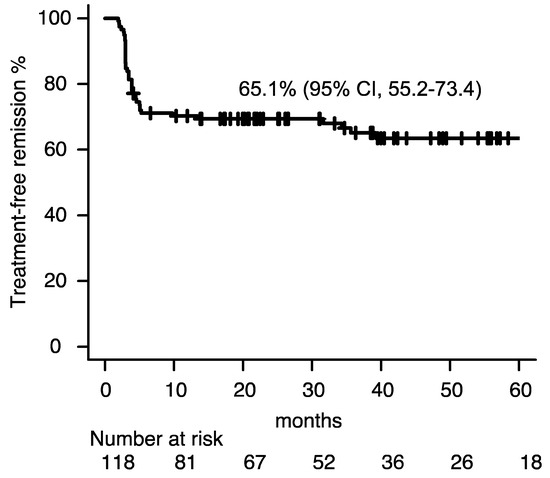
Figure 1.
Treatment free remission. Abbreviation; CI, confidence interval.

Table 1.
Patient characteristics.
3.2. No Clinical Factors Were Identified as Favorable Prognostic Indicators for TFR in Patients with CML-CP
We earlier reported that higher neutrophil counts were favorable prognostic factors for TFR in patients with CML-CP [20], thus we assessed white cell count, neutrophil count, and lymphocyte count at TKI discontinuation according to the using TKIs. Univariate analysis of the clinical properties for TFR (such as sex, age, Sokal risk score, use of frontline TKIs (imatinib or second-generation TKIs), TKIs at discontinuation (imatinib or second-generation TKIs), DMR duration at TKIs discontinuation, total TKIs treatment duration, depth of molecular remission [undetectable measurable residual disease (UMRD) or not] and white blood cell count, neutrophil count or lymphocyte count did not recognize any factor as a substantial prognostic variable for a lesser likelihood of molecular relapse (Table 2). Recently, the introduction of frontline second-generation TKI treatment enhanced the prognosis of patients with CML-CP compared with imatinib, hence we examined the prognostic variables for TFR in CML-CP split into patients with frontline imatinib and frontline second-generation TKIs.
Table 2.
Univariate analysis responsible for molecular relapse.
3.3. Higher Neutrophil Count at TKI Discontinuation Is a Favorable Prognostic Indicator for TFR in Patients with CML-CP Who Received Frontline Second-Generation TKIs
Sixty-six patients received imatinib as frontline TKI while 52 patients received second-generation TKIs as frontline. Patients who received second-generation TKIs as frontline exhibited longer DMR time (median, 51.0 vs. 46.8 months, p = 0.030) and treatment duration (median, 132.0 vs. 62.2 months, p < 0.001) than those who received imatinib, while age, sex, Sokal risk score, molecular remission at TKI discontinuation and TFR rate did not vary among the two groups (Table S1).
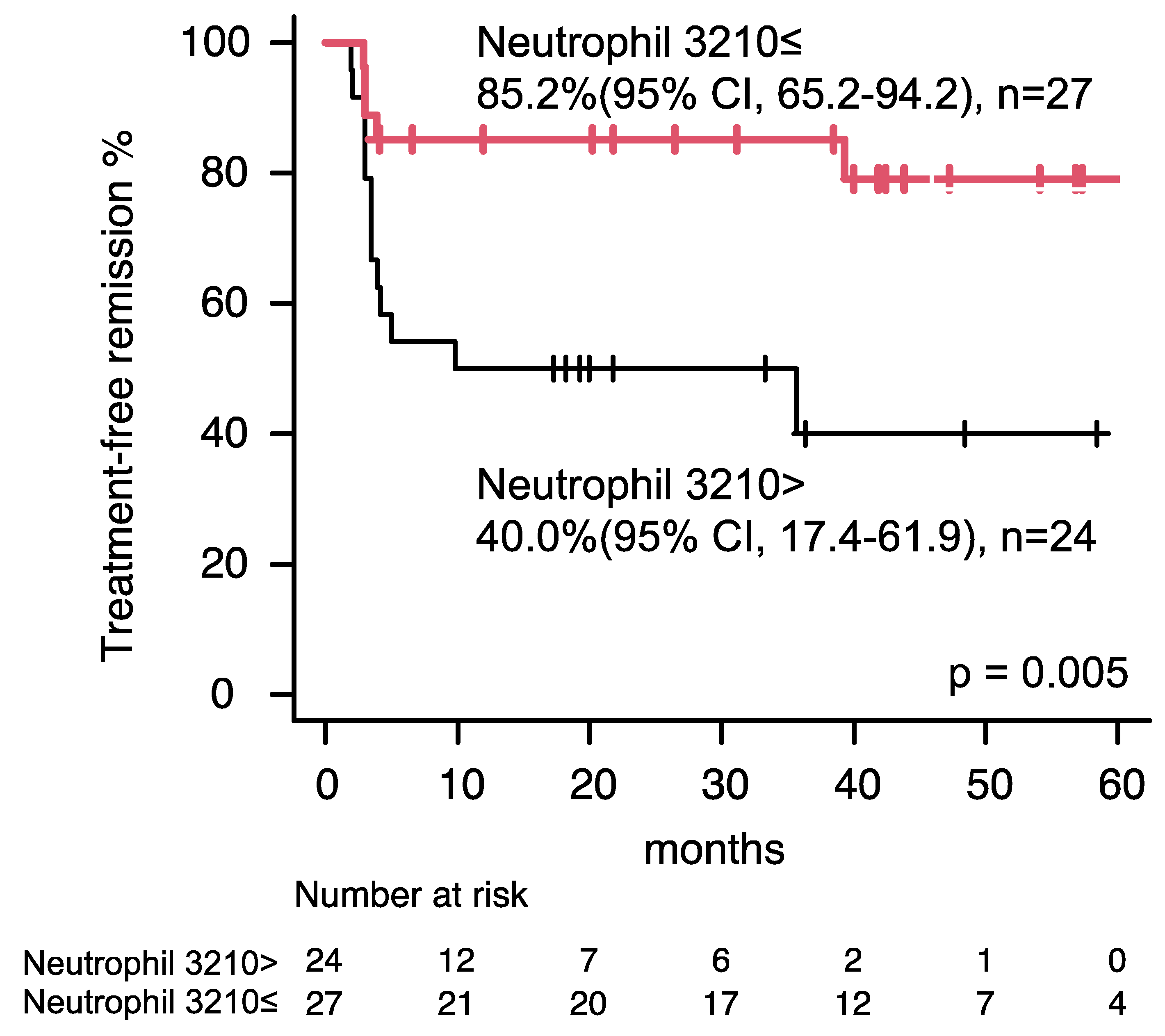
Univariate analysis of the clinical properties for TFR displayed extended TKI treatment duration (>98.8 months) was likely to be a favorable prognostic factor for TFR in patients who received imatinib as frontline [HR, 0.444 (95% CI, 0.186–1.060); p = 0.067], while did not identify any factor as an important prognostic variable for a lower likelihood of molecular relapse in patients who received imatinib as frontline (Table 3). Whereas, univariate and multivariate evaluation of the clinical characteristics for TFR portrayed higher neutrophil count (>3210/μL) was determined an independent prognostic factor for TFR in a patient who received second-generation TKIs as frontline [HR, 0.235 (95% CI, 0.078–0.711); p = 0.010, Table 4 and Figure 2]. We re-evaluated the earlier published data (other cohort) regarding neutrophil count at TKI discontinuation including 53 patients [20]. Patients who received second-generation TKIs as frontline with higher neutrophil count (>2439/μL) favorably acquired TFR [HR, 0.257 (95% CI, 0.080–0.825), p = 0.022, Figure S1], while the clinical impact of higher neutrophil count in patients who received imatinib as frontline was insignificant [HR 0.579 (95% CI, 0.174–1.927), p = 0.373], in line with the previous study. A higher neutrophil count can be a significant favorable prognostic factor for TFR in patients who received frontline second-generation TKIs supported evidence of the two independent cohorts.
Table 3.
Univariate analysis responsible for molecular relapse in patients who received imatinib as frontline treatment (n = 67).
Table 4.
Univariate and multivariate analysis responsible for molecular relapse in patients who received second generation tyrosine kinase inhibitors as frontline treatment (n = 51).
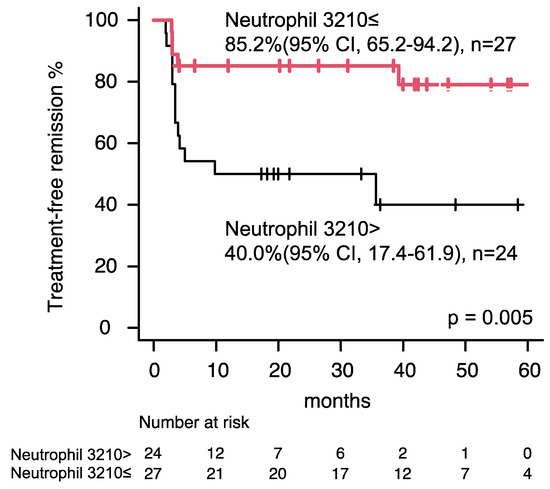
Figure 2.
Treatment–free remission in patients who received second-generation tyrosine kinase inhibitors as frontline treatment. Patients with higher neutrophil count (>3210/μL) achieved higher treatment–free remission. Red line indicates Patients with higher neutrophil count (>3210/μL) achieved higher treatment–free remission. Black line indicates patients with lower neutrophil count (≤3210/μL) achieved lower.
4. Discussion
Herein, we have demonstrated a multicenter retrospective study of patients with CML-CP who discontinued TKIs to recognize clinical features linked to sustained TFR. Our outcomes of a TFR rate of 65.1% were comparable to those of previous TKI discontinuation analysis, implying that our patients were a representative cohort [8].
Earlier, we noted a higher neutrophil count at TKIs discontinuation was correlated with the achievement of TFR in patients with CML-CP, whereas a higher neutrophil count at TKI discontinuation can be linked to the achievement of TFR in only patients with CML-CP who received second-generation TKI as the frontline in this research [20]. Remarkably, the magnitude of neutrophil counts did not influence TFR in patients who received imatinib as the frontline in both the previous and the present research, suggesting that higher neutrophil counts may be contributed to only patients with second-generation TKI treatment. Most patients received second-generation TKIs as frontline (31/53 cases, 58.5%) in prior studies, meanwhile, the current study encompassed only 51/118 patients (43.2%, p = 0.071). The discrepancy in the clinical impact of neutrophil count for CML-CP between the earlier and the current research may be influenced by the different proportion of patients who received second-generation TKI as frontline.
Neutrophils generally act as anti-bacterial via activation of the innate and adaptive immune system. Recently, tumor-associated neutrophils, particularly antitumor neutrophils have been recognized as a significant component of the cancer microenvironment [23]. The activation of neutrophils triggered reactive oxygen species production, causing potent tumor eradication independent from T-cell mediated immune response [24]. T-cell and/or NK cell immune responses partake in the treatment responses or achieving TFR in CML patient, the neutrophil-mediated immune response can also play an important role in CML [25].
Inhibition of the TGF-β pathway causes an accumulation of the antitumor neutrophil, and second-generation TKIs strongly suppress c-Kit and ABL1, a downstream mediator of TGF-β compared with imatinib [26]. The TKIs-activated off-target immunomodulation effects have demonstrated favorable clinical responses [27] and may control residual leukemic cells to attain successful TFR in CML, supported by our retrospective observation. Thus, higher neutrophil counts can be contributed to the patients only by using second-generation TKIs which have strong TGF-β pathway inhibition potential. Whereas, the positive impact of nilotinib which might influence the highest neutrophil counts for TFR was uncertain. Further research is required to clarify the biological mechanism to influence the achievement of TFR by anti-tumor neutrophils.
Our research had several limitations. First, the study was a retrospective observational investigation. Second, there was no assessment of other immune cell fractions (T-cells and NK cells). Third, the study comprised a relatively small cohort (118 patients) compared with other studies (e.g., EUROski) [8]. Fourth, the enrolled patients were all Japanese patients, thus the effects of the neutrophil did not evaluate according to race.
We conclude higher neutrophil count at TKI discontinuation was related to the achievement of TFR in patients with CML-CP who received second-generation TKI as frontline treatment.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/clinpract14040097/s1, Figure S1: Treatment–free remission according to frontline tyrosine kinase inhibitor (TKI) and neutrophil count at TKI discontinuation in the previous study; Table S1: Characteristics according to the frontline tyrosine kinase inhibitors.
Author Contributions
Conceptualization, H.U., Y.T., K.K., T.O., N.I., E.O., E.S. and S.K.; methodology, H.U., K.K. and S.K.; validation, H.U., K.K. and SK.; formal analysis, H.U., K.K. and S.K.; investigation, H.U., K.K. and S.K.; data curation, H.U., Y.T., K.K., T.O., N.I., E.O., E.S. and S.K.; writing—original draft preparation, H.U., K.K. and S.K.; writing—review and editing, H.U., Y.T., K.K., T.O., N.I., E.O., E.S. and S.K.; visualization, H.U., K.K. and S.K.; supervision, S.K.; project administration, H.U.; funding acquisition, T.O., N.I., E.S. and S.K. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by research grants from the Japan Society for the Promotion of Science Grants-in-Aid for Scientific Research (21K16245 to HU), and the Shinnihon Foundation of Advanced Medical Treatment Research (HU), Takeda Science Foundation (HU), the Medical Research Encouragement Prize of The Japan Medical Association (HU), the Japanese society of hematology research grant (HU) and Japanese foundation for multidisciplinary treatment of cancer (HU).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of Saga University (protocol code, 2021-12-R-04 and date of approval, 25 February 2022).” for studies involving humans.
Informed Consent Statement
Informed consent was acquired by the opt-out method; information on the study, including the use of specimens objectives and the opportunity to opt-out, was made public, and no patients made objections.
Data Availability Statement
All data can be accessed by contacting the corresponding author (H.U.).
Conflicts of Interest
T.O. reports honoraria from Bristol Myers Squibb, Celgene, Merck Sharp & Dohme, Ono, Otsuka, Novartis, Pfizer, and Takeda, and research funding from Celgene, Chugai, Kyowa Hakko Kirin, Merck Sharp & Dohme, and Ono. N.I. received honoraria and speaker fee from Bristol Myers Squibb, Pfizer, Novartis. E.S. received honoraria from Novartis, Pfizer, Takeda and Yanssen; and research funding from Chugai, Kyowa Hakko Kirin, and Eisai. S.K. received honoraria from Bristol-Myers Squibb, Novartis, Pfizer, and Otsuka Pharmaceuticals; and research funding from Bristol-Myers Squibb, Pfizer and Ohara Pharmaceuticals. The other authors declare no conflicts of interest.
References
- Bower, H.; Björkholm, M.; Dickman, P.W.; Höglund, M.; Lambert, P.C.; Andersson, T.M.L. Life expectancy of patients with chronic myeloid leukemia approaches the life expectancy of the general population. J. Clin. Oncol. 2016, 34, 2851–2857. [Google Scholar] [CrossRef] [PubMed]
- Mahon, F.-X.; Réa, D.; Guilhot, J.; Guilhot, F.; Huguet, F.; Nicolini, F.; Legros, L.; Charbonnier, A.; Guerci, A.; Varet, B.; et al. Discontinuation of imatinib in patients with chronic myeloid leukaemia who have maintained complete molecular remission for at least 2 years: The prospective, multicentre Stop Imatinib (STIM) trial. Lancet Oncol. 2010, 11, 1029–1035. [Google Scholar] [CrossRef] [PubMed]
- Rousselot, P.; Charbonnier, A.; Cony-Makhoul, P.; Agape, P.; Nicolini, F.E.; Varet, B.; Gardembas, M.; Etienne, G.; Réa, D.; Roy, L.; et al. Loss of major molecular response as a trigger for restarting tyrosine kinase inhibitor therapy in patients with chronic-phase chronic myelogenous leukemia who have stopped imatinib after durable undetectable disease. J. Clin. Oncol. 2014, 32, 424–430. [Google Scholar] [CrossRef] [PubMed]
- Imagawa, J.; Tanaka, H.; Okada, M.; Nakamae, H.; Hino, M.; Murai, K.; Ishida, Y.; Kumagai, T.; Sato, S.; Ohashi, K.; et al. Discontinuation of dasatinib in patients with chronic myeloid leukaemia who have maintained deep molecular response for longer than 1 year (DADI trial): A multicentre phase 2 trial. Lancet Haematol. 2015, 2, e528–e535. [Google Scholar] [CrossRef] [PubMed]
- Rea, D.; Nicolini, F.E.; Tulliez, M.; Guilhot, F.; Guilhot, J.; Guerci-Bresler, A.; Gardembas, M.; Coiteux, V.; Guillerm, G.; Legros, L.; et al. Discontinuation of dasatinib or nilotinib in chronic myeloid leukemia: Interim analysis of the STOP 2G-TKI study. Blood 2017, 129, 846–854. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.P.; García-Gutiérrez, V.; Jiménez-Velasco, A.; Larson, S.; Saussele, S.; Rea, D.; Mahon, F.-X.; Levy, M.Y.; Gómez-Casares, M.T.; Pane, F.; et al. Dasatinib discontinuation in patients with chronic-phase chronic myeloid leukemia and stable deep molecular response: The DASFREE study. Leuk Lymphoma 2020, 61, 650–659. [Google Scholar] [CrossRef]
- Hochhaus, A.; Masszi, T.; Giles, F.J.; Radich, J.P.; Ross, D.M.; Casares, M.T.G.; Hellmann, A.; Stentoft, J.; Conneally, E.; García-Gutiérrez, V.; et al. Treatment-free remission following frontline nilotinib in patients with chronic myeloid leukemia in chronic phase: Results from the ENESTfreedom study. Leukemia 2017, 31, 1525–1531. [Google Scholar] [CrossRef]
- Saussele, S.; Richter, J.; Guilhot, J.; Gruber, F.X.; Hjorth-Hansen, H.; Almeida, A.; Janssen, J.J.W.M.; Mayer, J.; Koskenvesa, P.; Panayiotidis, P.; et al. Discontinuation of tyrosine kinase inhibitor therapy in chronic myeloid leukaemia (EURO-SKI): A prespecified interim analysis of a prospective, multicentre, non-randomised, trial. Lancet Oncol. 2018, 19, 747–757. [Google Scholar] [CrossRef]
- Hochhaus, A.; Baccarani, M.; Silver, R.T.; Schiffer, C.; Apperley, J.F.; Cervantes, F.; Clark, R.E.; Cortes, J.E.; Deininger, M.W.; Guilhot, F.; et al. European LeukemiaNet 2020 recommendations for treating chronic myeloid leukemia. Leukemia 2020, 34, 966–984. [Google Scholar] [CrossRef]
- Lee, S.-E.; Choi, S.Y.; Song, H.-Y.; Kim, S.-H.; Choi, M.-Y.; Park, J.S.; Kim, H.-J.; Zang, D.Y.; Oh, S.; Do, Y.R.; et al. Imatinib withdrawal syndrome and longer duration of imatinib have a close association with a lower molecular relapse after treatment discontinuation: The KID study. Haematologica 2016, 101, 717–723. [Google Scholar] [CrossRef]
- Haddad, F.G.; Sasaki, K.; Issa, G.C.; Garcia-Manero, G.; Ravandi, F.; Kadia, T.; Cortes, J.; Konopleva, M.; Pemmaraju, N.; Alvarado, Y.; et al. Treatment-free remission in patients with chronic myeloid leukemia following the discontinuation of tyrosine kinase inhibitors. Am. J. Hematol. 2022, 97, 856–864. [Google Scholar] [CrossRef]
- Takahashi, N.; Tauchi, T.; Kitamura, K.; Miyamura, K.; Saburi, Y.; Hatta, Y.; Miyata, Y.; Kobayashi, S.; Usuki, K.; Matsumura, I.; et al. Deeper molecular response is a predictive factor for treatment-free remission after imatinib discontinuation in patients with chronic phase chronic myeloid leukemia: The JALSG-STIM213 study. Int. J. Hematol. 2018, 107, 185–193. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, N.; Nishiwaki, K.; Nakaseko, C.; Aotsuka, N.; Sano, K.; Ohwada, C.; Kuroki, J.; Kimura, H.; Tokuhira, M.; Mitani, K.; et al. Treatment-free remission after two-year consolidation therapy with nilotinib in patients with chronic myeloid leukemia: STAT2 trial in Japan. Haematologica 2018, 103, 1835–1842. [Google Scholar] [CrossRef] [PubMed]
- Rea, D.; Henry, G.; Khaznadar, Z.; Etienne, G.; Guilhot, F.; Nicolini, F.; Guilhot, J.; Rousselot, P.; Huguet, F.; Legros, L.; et al. Natural killer-cell counts are associated with molecular relapse-free survival after imatinib discontinuation in chronic myeloid leukemia: The IMMUNOSTIM study. Haematologica 2017, 102, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Ureshino, H.; Ueda, Y.; Fujisawa, S.; Usuki, K.; Tanaka, H.; Okada, M.; Kowata, S.; Murai, K.; Hirose, A.; Shindo, M.; et al. KIR3DL1-HLA-Bw status in CML is associated with achievement of TFR: The POKSTIC trial, a multicenter observational study. Blood Neoplasia 2024, 1, 100001. [Google Scholar] [CrossRef]
- D’Adda, M.; Farina, M.; Schieppati, F.; Borlenghi, E.; Bottelli, C.; Cerqui, E.; Ferrari, S.; Gramegna, D.; Pagani, C.; Passi, A.; et al. The e13a2 BCR-ABL transcript negatively affects sustained deep molecular response and the achievement of treatment-free remission in patients with chronic myeloid leukemia who receive tyrosine kinase inhibitors. Cancer 2019, 125, 1674–1682. [Google Scholar] [CrossRef] [PubMed]
- Irani, Y.D.; Hughes, A.; Clarson, J.; Kok, C.H.; Shanmuganathan, N.; White, D.L.; Yeung, D.T.; Ross, D.M.; Hughes, T.P.; Yong, A.S.; et al. Successful treatment-free remission in chronic myeloid leukaemia and its association with reduced immune suppressors and increased natural killer cells. Br. J. Haematol. 2020, 191, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Kafatos, F.; Janeway, C.; Ezekowitz, R. Phylogenetic perspectives in innate immunity. Science 1999, 284, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Giese, M.A.; Hind, L.E.; Huttenlocher, A. Neutrophil plasticity in the tumor microenvironment. Blood 2019, 133, 2159–2167. [Google Scholar] [CrossRef]
- Ureshino, H.; Kamachi, K.; Sano, H.; Okamoto, S.; Itamura, H.; Yoshimura, M.; Katsuya, H.; Ando, T.; Kimura, S. Higher neutrophil counts are associated with successful tyrosine kinase inhibitor discontinuation in patients with chronic myeloid leukemia. Hematology 2022, 27, 1171–1175. [Google Scholar] [CrossRef]
- Khoury, J.D.; Solary, E.; Abla, O.; Akkari, Y.; Alaggio, R.; Apperley, J.F.; Bejar, R.; Berti, E.; Busque, L.; Chan, J.K.C.; et al. The 5th edition of the World Health Organization Classification of Haematolymphoid Tumours: Myeloid and Histiocytic/Dendritic Neoplasms. Leukemia 2022, 36, 1703–1719. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Jaillon, S.; Ponzetta, A.; Di Mitri, D.; Santoni, A.; Bonecchi, R.; Mantovani, A. Neutrophil diversity and plasticity in tumour progression and therapy. Nat. Rev. Cancer. 2020, 20, 485–503. [Google Scholar] [CrossRef]
- Linde, I.L.; Prestwood, T.R.; Qiu, J.; Pilarowski, G.; Linde, M.H.; Zhang, X.; Shen, L.; Reticker-Flynn, N.E.; Chiu, D.K.-C.; Sheu, L.Y.; et al. Neutrophil-activating therapy for the treatment of cancer. Cancer Cell 2023, 41, 356–372.e10. [Google Scholar] [CrossRef] [PubMed]
- Huuhtanen, J.; Adnan-Awad, S.; Theodoropoulos, J.; Forstén, S.; Warfvinge, R.; Dufva, O.; Bouhlal, J.; Dhapola, P.; Duàn, H.; Laajala, E.; et al. Single-cell analysis of immune recognition in chronic myeloid leukemia patients following tyrosine kinase inhibitor discontinuation. Leukemia 2024, 38, 109–125. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, Z.; Kwong, S.Q.; Lui, E.L.H.; Friedman, S.L.; Li, F.R.; Lam, R.W.C.; Zhang, G.C.; Zhang, H.; Ye, T. Inhibition of PDGF, TGF-β, and Abl signaling and reduction of liver fibrosis by the small molecule Bcr-Abl tyrosine kinase antagonist Nilotinib. J. Hepatol. 2011, 55, 612–625. [Google Scholar] [CrossRef] [PubMed]
- Mustjoki, S.; Ekblom, M.; Arstila, T.P.; Dybedal, I.; Epling-Burnette, P.K.; Guilhot, F.; Hjorth-Hansen, H.; Höglund, M.; Kovanen, P.; Laurinolli, T.; et al. Clonal expansion of T/NK-cells during tyrosine kinase inhibitor dasatinib therapy. Leukemia 2009, 23, 1398–1405. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).