Reply to Comment on Ultrasound Guidance for Botulinum Neurotoxin Chemodenervation Procedures. Toxins 2018, 10, 18—Quintessential Use of Ultrasound Guidance for Botulinum Toxin Injections



{kind=link}
{kind=link}
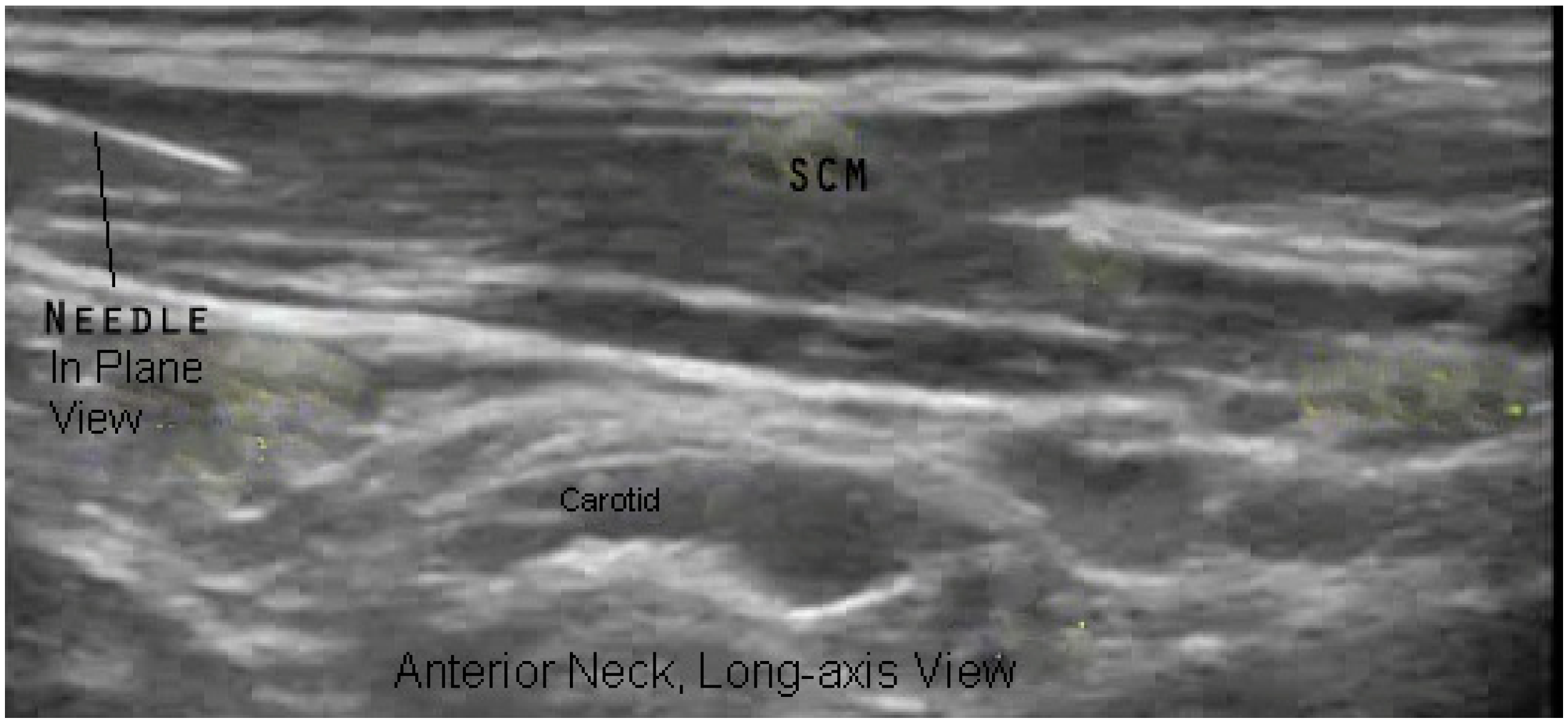
- The IP technique requires insertion of the needle distant to the target such that the needle would traverse un-targeted structures.
- There is no safe path to the target using an IP technique.
- An OP approach provides direct access to the muscle, such as the flexor carpi radialis, while the IP technique would require the needle to penetrate or traverse additional undesired muscles or pass near to or through other structures such as vessels or nerves.
Conflicts of Interest
References
- Childers, M.K. Targeting the neuromuscular junction in skeletal muscles. Am. J. Phys. Med. Rehabil. 2004, 83, S38–S44. [Google Scholar] [CrossRef] [PubMed]
- Amirali, A.; Mu, L.; Gracies, J.M.; Simpson, D.M. Anatomical localization of motor endplate bands in the human biceps brachii. J. Clin. Neuromusc. Dis. 2007, 9, 306–312. [Google Scholar] [CrossRef] [PubMed]
- Saitou, K.; Masuda, T.; Michikami, D.; Michikami, D.; Kojima, R.; Okada, M. Innervation zones of the upper and lower limb muscles estimated by using multichannel surface EMG. J. Hum. Ergol. 2000, 29, 35–52. [Google Scholar]
- Van Campenhout, A.; Molenaers, G. Localization of the motor endplate zone in human skeletal muscles of the lower limb: Anatomical guidelines for injection with botulinum toxin. Dev. Med. Child Neurol. 2011, 53, 108–119. [Google Scholar] [CrossRef] [PubMed]
- Gracies, J.M.; Lugassy, M.; Weisz, D.J.; Vecchio, M.; Flanagan, S.; Simpson, D.M. Botulinum toxin dilution and endplate targeting in spasticity: A double-blind controlled study. Arch. Phys. Med. Rehabil. 2009, 90, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.; Finnoff, J.T. Diagnostic and interventional musculoskeletal ultrasound: Part 2. Clinical applications. PM R 2009, 1, 162–177. [Google Scholar] [CrossRef] [PubMed]
- Kaymak, B.; Kara, M.; Yağiz On, A.; Soylu, A.R.; Özçakar, L. Innervation zone targeted botulinum toxin injections. Eur. J. Phys. Rehabil. Med. 2018, 54, 100–109. [Google Scholar] [PubMed]
- Kara, M.; Kaymak, B.; Ulaşli, A.M.; Tok, F.; Öztürk, G.T.; Chang, K.V.; Hsiao, M.Y.; Hung, C.Y.; Yağiz On, A.; Özçakar, L. Sonographic guide for botulinum toxin injections of the upper limb: Euro-musculus/USPRM spasticity approach. Eur. J. Phys. Rehabil. Med. 2018, 54, 469–485. [Google Scholar] [CrossRef] [PubMed]
- Kaymak, B.; Kara, M.; Tok, F.; Ulasli, A.M.; Öztürk, G.T.; Chang, K.V.; Hsiao, M.Y.; Hung, C.Y.; Yağiz On, A.; Özçakar, L. Sonographic guide for botulinum toxin injections of the lower limb: Euro-musculus/USPRM spasticity approach. Eur. J. Phys. Rehabil. Med. 2018, 54, 486–498. [Google Scholar] [CrossRef] [PubMed]
- Kaymak, B.; Kara, M.; Gürçay, E.; Özçakar, L. Sonographic guide for botulinum toxin injections of the neck muscles in cervical dystonia. Phys. Med. Rehabil. Clin. N. Am. 2018, 29, 105–123. [Google Scholar] [CrossRef] [PubMed]
- Alter, K.E. Neurotoxin Storage, Reconstitution, Handling, and Dilution. In Botulinum Neurotoxin Injection Manual; Demos Medical Publishing: New York, NY, USA, 2015; pp. 19–28. [Google Scholar]


© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alter, K.E.; Karp, B.I. Reply to Comment on Ultrasound Guidance for Botulinum Neurotoxin Chemodenervation Procedures. Toxins 2018, 10, 18—Quintessential Use of Ultrasound Guidance for Botulinum Toxin Injections. Toxins 2018, 10, 400. https://doi.org/10.3390/toxins10100400
Alter KE, Karp BI. Reply to Comment on Ultrasound Guidance for Botulinum Neurotoxin Chemodenervation Procedures. Toxins 2018, 10, 18—Quintessential Use of Ultrasound Guidance for Botulinum Toxin Injections. Toxins. 2018; 10(10):400. https://doi.org/10.3390/toxins10100400
Chicago/Turabian StyleAlter, Katharine E., and Barbara I. Karp. 2018. "Reply to Comment on Ultrasound Guidance for Botulinum Neurotoxin Chemodenervation Procedures. Toxins 2018, 10, 18—Quintessential Use of Ultrasound Guidance for Botulinum Toxin Injections" Toxins 10, no. 10: 400. https://doi.org/10.3390/toxins10100400
APA StyleAlter, K. E., & Karp, B. I. (2018). Reply to Comment on Ultrasound Guidance for Botulinum Neurotoxin Chemodenervation Procedures. Toxins 2018, 10, 18—Quintessential Use of Ultrasound Guidance for Botulinum Toxin Injections. Toxins, 10(10), 400. https://doi.org/10.3390/toxins10100400