Therapeutic Approaches of Botulinum Toxin in Gynecology



Abstract
:1. Introduction
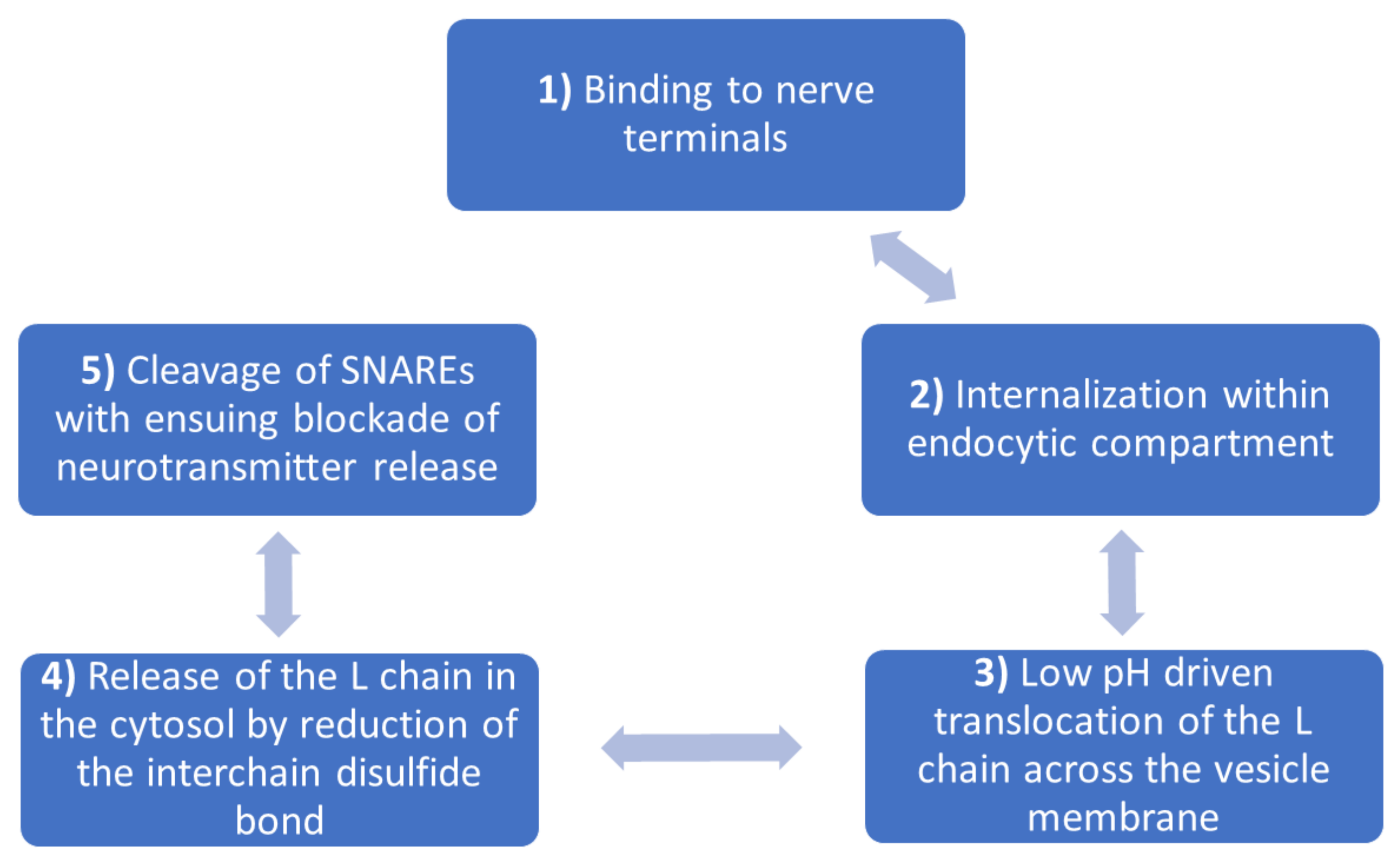
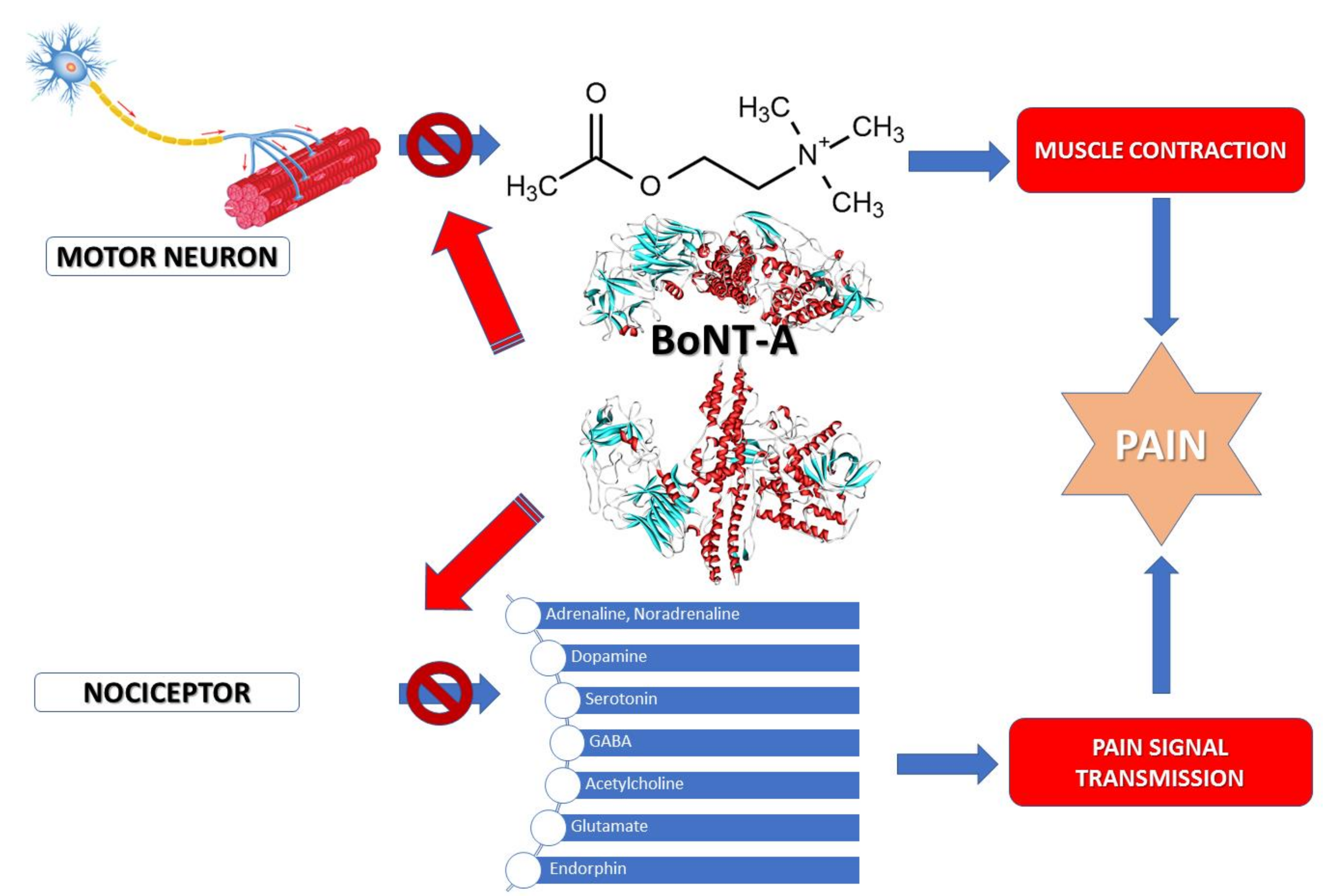
2. Botulinum Toxin
3. Review of the Literature Regarding the Gynecologic Indications for the Use of BoNT-A
3.1. Use of BoNT-A in the Treatment of Vaginism
- 1st degree:
- o
- Levator and perineal spasm relieved with reassurance
- o
- Able to tolerate vaginal exam
- 2nd degree:
- o
- the perineal spasm is maintained through the gynecology exam
- o
- Unable to relax for the pelvic exam
- 3rd degree:
- o
- Spasm of the levator muscle
- o
- Elevation of buttocks to avoid the gynecology exam
- 4th degree:
- o
- Perineal and levator spasm
- o
- Adduction of thighs, elevation of buttocks, unable to tolerate the pelvic exam.
3.2. Use of BoNT in the Treatment of Vulvodynia
3.3. Use of BoNT-A in the Treatment of Chronic Pelvic Pain
3.4. Inferior Urinary System Dysfunctions
3.4.1. Use of BoNT in the Treatment of Interstitial Cystitis (the Painful Bladder Syndrome)
3.4.2. Use of BoNT-A in Urinary Incontinence through Neurogenic Overactive Bladder and Idiopathic Overactive Bladder
4. Conclusions and Future Perspectives
Author Contributions
Conflicts of Interest
Abbreviations
| Ach | acetylcholine |
| BFLUTS | Bristol female low urinary tract symptoms |
| BoNT | botulinum toxin |
| BoNT A | botulinum toxin type A |
| BoNT B | botulinum toxin type B |
| CISC | intermittent self-catheterization |
| DC | detrusor compliance |
| EMG | electromyography |
| EQ 5D | a standardized instrument for use as a measure of health outcome |
| FSDS | female sexual distress scale |
| IIQ | Incontinence inventory questionnaire |
| IOB | idiopathic overactive bladder |
| KHQ | King’s Health Questionnaire |
| LC | Light chain |
| MCBC | maximal cystometric capacity |
| NGF | nerves growth factor |
| NOB | neurogenic overactive bladder |
| OB | overactive bladder |
| PFM | pelvic floor muscle |
| PGISC | patient global impression of symptom control |
| PVR | postvoiding residual volume |
| QoL | quality of life |
| SNARE | Soluble NSF(N-ethylmaleimide-sensitive factor) Attachment Protein) REceptor |
| SF12 | physical and mental health summary scales |
| SNAP | Synaptosomal-associated protein 25 |
| TRPV | transient receptor potential cation channels (“V” is for vanilloid type) |
| UDI | urinary distress inventory |
| VAS | visual analog scale |
| VAMP | vesicle associated membrane protein |
References
- Ahangari, A. Prevalence of chronic pelvic pain among women: An updated review. Pain Physician 2014, 17, E141–E147. [Google Scholar] [PubMed]
- Jarrell, J.F.; Vilos, G.A.; Allaire, C.; Burgess, S.; Fortin, C.; Gerwin, R.; Lapensée, L.; Lea, R.H.; Leyland, N.A.; Martyn, P.; et al. Consensus guidelines for the management of chronic pelvic pain. J. Obstet. Gynaecol. Can. 2005, 27, 781–826. [Google Scholar] [CrossRef] [PubMed]
- Akour, A.; Kasabri, V.; Afifi, F.U.; Bulatova, N. The use of medicinal herbs in gynecological and pregnancy-related disorders by Jordanian women: A review of folkloric practice vs. evidence-based pharmacology. Pharm. Biol. 2016, 54, 1901–1918. [Google Scholar] [CrossRef] [PubMed]
- Rapin, A.J.; Morgan, M.L. Chronic Pelvic Pain. In Handbook of Women’s Sexual and Reproductive Health; Issues in Women’s Health; Springer: Boston, MA, USA, 2002; pp. 217–229. Available online: https://link.springer.com/chapter/10.1007/978-1-4615-0689-8_12#citeas (accessed on 20 September 2017). [CrossRef]
- Speer, L.M.; Mushkabar, S.; Erbele, T. Chronic Pelvic Pain in Women. Am. Fam. Physician 2016, 93, 380–387. [Google Scholar] [PubMed]
- Baranowski, A.P. Chronic pelvic pain. Best Pract. Res. Clin. Gastroenterol. 2009, 23, 593–610. [Google Scholar] [CrossRef] [PubMed]
- Restani, P.; Di Lorenzo, C.; Garcia-Alvarez, A.; Badea, M.; Ceschi, A.; Egan, B.; Dima, L.; Lude, S.; Maggi, F.M.; Marculescu, A.; et al. Adverse Effects of Plant Food Supplements Self-Reported by Consumers in the PlantLIBRA Survey Involving Six European Countries. PLoS ONE 2016, 11, e0150089. [Google Scholar] [CrossRef] [PubMed]
- Said, S.Z.; Meshkinpour, A.; Carruthers, A.; Carruthers, J. Botulinum Toxin A. Am. J. Clin. Dermatol. 2003, 4, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Dima, L.; Repanovici, A.; Purcaru, D.; Rogozea, L. Informed consent and e-communication in medicine. Rev. Romana Bioet. 2014, 12, 37–46. [Google Scholar]
- Naumanna, M.; Albaneseb, A.; Heinenc, F.; Molenaersd, G.; Relja, M. Safety and efficacy of botulinum toxin type A following long-term use. Eur. J. Neurol. 2006, 13, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Nigam, P.K.; Anjana, N. Botulinum toxin. Indian J. Dermatol. 2010, 55, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Sloop, R.R.; Cole, R.A.; Escutin, R.O. Human response to botulinum toxin injection: Type B compared with type A. Neurology 1997, 49. [Google Scholar] [CrossRef]
- Pirazzini, M.; Rossetto, O.; Eleopra, R.; Montecucco, C. Botulinum Neurotoxins: Biology, Pharmacology and Toxicology. Pharmacol. Rev. 2017, 69, 200–235. [Google Scholar] [CrossRef] [PubMed]
- Rossetto, O.; Pirazzini, M.; Montecucco, C. Botulinum neurotoxins: Genetic, structural and mechanistic insights. Nat. Rev. Microbiol. 2014, 12, 535–549. [Google Scholar] [CrossRef] [PubMed]
- Hill, K.K.; Smith, T.J. Genetic diversity within Clostridium botulinum serotypes, botulinum neurotoxin gene clusters and toxin subtypes. Curr. Top. Microbiol. Immunol. 2013, 364, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Burke, G.S. Notes on Bacillus botulinus. J. Bacteriol. 1919, 4, 555–570. [Google Scholar] [PubMed]
- Gimenez, D.; Ciccarelli, A.S. Another type of Clostridium botulinum. Zentralbl. Bakteriol. 1970, 215, 221–224. [Google Scholar]
- Chai, Q.; Arndt, J.W.; Dong, M.; Tepp, W.H.; Johnson, E.A.; Chapman, E.R.; Stevens, R.C. Structural basis of cell surface receptor recognition by botulinum neurotoxin B. Nature 2006, 444, 1096–1100. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Masuyer, G.; Zhang, J.; Shen, Y.; Lundin, D.; Henriksson, L.; Miyashita, S.I.; Martínez-Carranza, M.; Dong, M.; Stenmark, P. Identification and characterization of a novel botulinum neurotoxin. Nat. Commun. 2017, 8, 14130. [Google Scholar] [CrossRef] [PubMed]
- Steegmaier, M.; Klumperman, J.; Foletti, D.L.; Yoo, J.S.; Scheller, R.H. Vesicle-associated membrane protein 4 is implicated in trans-Golgi network vesicle trafficking. Mol. Biol. Cell. 1999, 10, 1957–1972. [Google Scholar] [CrossRef] [PubMed]
- Brandhorst, D.; Zwilling, D.; Rizzoli, S.O.; Lippert, U.; Lang, T.; Jahn, R. Homotypic fusion of early endosomes: SNAREs do not determine fusion specificity. Proc. Natl. Acad. Sci. USA 2006, 103, 2701–2706. [Google Scholar] [CrossRef] [PubMed]
- Daste, F.; Galli, T.; Tareste, D. Structure and function of longin SNAREs. J. Cell. Sci. 2015, 128, 4263–4272. [Google Scholar] [CrossRef] [PubMed]
- Zornetta, I.; Azarnia Tehran, D.; Arrigoni, G.; Anniballi, F.; Bano, L.; Leka, O.; Zanotti, G.; Binz, T.; Montecucco, C. The first non Clostridial botulinum-like toxin cleaves VAMP within the juxtamembrane domain. Sci. Rep. 2016, 6, 30257. [Google Scholar] [CrossRef] [PubMed]
- Tanizawa, Y.; Fujisawa, T.; Mochizuki, T.; Kaminuma, E.; Suzuki, Y.; Nakamura, Y.; Tohno, M. Draft Genome Sequence of Weissella oryzae SG25T, Isolated from Fermented Rice Grains. Genome Announc. 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Lebreton, F.; Mansfield, M.J.; Miyashita, S.I.; Zhang, J.; Schwartzman, J.A.; Tao, L.; Masuyer, G.; Martínez-Carranza, M.; Stenmark, P. Identification of a Botulinum Neurotoxin-like Toxin in a Commensal Strain of Enterococcus faecium. Cell Host Microbe. 2018, 23, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Kukreja, R.; Singh, B.R. The botulinum toxin as a therapeutic agent: Molecular and pharmacological insights. Res. Rep. Biochem. 2015, 5, 173–183. [Google Scholar] [CrossRef]
- Azarnia Tehran, D.; Pirazzini, M.; Leka, O.; Mattarei, A.; Lista, F.; Binz, T.; Rossetto, O.; Montecucco, C. Hsp90 is involved in the entry of clostridial neurotoxins into the cytosol of nerve terminals. Cell. Microbiol. 2017, 19. [Google Scholar] [CrossRef] [PubMed]
- Montal, M. Botulinum neurotoxin: A marvel of protein design. Annu. Rev. Biochem. 2010, 79, 591–617. [Google Scholar] [CrossRef] [PubMed]
- Matac, I.; Lackovic, Z. Botulinum toxin A, brain and pain. Prog. Neurobiol. 2014, 119–120, 39–59. [Google Scholar] [CrossRef] [PubMed]
- Gallagher, J.; Ackerman, A. Botulinum toxin: From Molecule to Medicine. In Botulinum Toxin Cosmetic and Clinical Applications; Wiley Online Library: Chichester, UK, 2017; pp. 37–51. Available online: https://onlinelibrary.wiley.com/doi/10.1002/9781118661833.ch3 (accessed on 7 April 2018).
- Pickett, A.; Perrow, K. Towards new uses of botulinum toxin as a novel therapeutic tool. Toxins 2011, 3, 63–81. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.L. The life history of a botulinum toxin molecule. Toxicon 2013, 68, 40–59. [Google Scholar] [CrossRef] [PubMed]
- Montecucco, C. How do tetanus and botulinum toxins bind to neuronal membranes? Trends Biochem. Sci. 1986, 11, 314–317. [Google Scholar] [CrossRef]
- Rummel, A. Double receptor anchorage of botulinum neurotoxins accounts for their exquisite neurospecificity. Curr. Top. Microbiol. Immunol. 2013, 364, 61–90. [Google Scholar] [CrossRef] [PubMed]
- Pirazzini, M.; Rossetto, O.; Bolognese, P.; Shone, C.C.; Montecucco, C. Double anchorage to the membrane and intact inter-chain disulfide bond are required for the low pH induced entry of tetanus and botulinum neurotoxins into neurons. Cell. Microbiol. 2011, 13, 1731–1743. [Google Scholar] [CrossRef] [PubMed]
- Colasante, C.; Rossetto, O.; Morbiato, L.; Pirazzini, M.; Molgó, J.; Montecucco, C. Botulinum neurotoxin type A is internalized and translocated from small synaptic vesicles at the neuromuscular junction. Mol. Neurobiol. 2013, 48, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.L.; Coffield, J.A.; Bakry, N. Inhibition of vacuolar adenosine triphosphatase antagonizes the effects of clostridial neurotoxins but not phospholipase A2 neurotoxins. J. Pharmacol. Exp. Ther. 1994, 269, 256–262. [Google Scholar] [PubMed]
- Williamson, L.C.; Neale, E.A. Bafilomycin A1 inhibits the action of tetanus toxin in spinal cord neurons in cell culture. J. Neurochem. 1994, 63, 2342–2345. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Suresh, S.; Liu, H.; Tepp, W.H.; Johnson, E.A.; Edwardson, J.M.; Chapman, E.R. Receptor binding enables botulinum neurotoxin B to sense low pH for translocation channel assembly. Cell Host Microbe 2011, 10, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Fischer, A.; Montal, M. Crucial role of the disulfide bridge between botulinum neurotoxin light and heavy chains in protease translocation across membranes. J. Biol. Chem. 2007, 282, 29604–29611. [Google Scholar] [CrossRef] [PubMed]
- Zanetti, G.; Azarnia Teheran, D.; Pirazzini, M.; Binz, T.; Shone, C.C.; Fillo, S.; Lista, F.; Rossetto, O.; Montecucco, C. Inhibition of botulinum neurotoxins interchain disulfide bond reduction prevents the peripheral neuroparalysis of botulism. Biochem. Pharmacol. 2015, 98, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Pirazzini, M.; Azarnia Teheran, D.; Zanetti, G.; Megighian, A.; Scorzeto, M.; Fillo, S.; Shone, C.C.; Binz, T.; Rossetto, O.; Lista, F.; et al. Thioredoxin and its reductase are present on synaptic vesicles, and their inhibition prevents the paralysis induced by botulinum neurotoxins. Cell Rep. 2014, 8, 1870–1878. [Google Scholar] [CrossRef] [PubMed]
- Meyer, Y.; Buchanan, B.B.; Vignols, F.; Reichheld, J.P. Thioredoxins and glutaredoxins: Unifying elements in redox biology. Annu. Rev. Genet. 2009, 43, 335–367. [Google Scholar] [CrossRef] [PubMed]
- Hanschmann, E.M.; Godoy, J.R.; Berndt, C.; Hudemann, C.; Lillig, C.H. Thioredoxins, glutaredoxins, and peroxiredoxins—Molecular mechanisms and health significance: From cofactors to antioxidants to redox signaling. Antioxid. Redox Signal. 2013, 19, 1539–1605. [Google Scholar] [CrossRef] [PubMed]
- Berndt, C.; Lillig, C.H.; Holmgren, A. Thioredoxins and glutaredoxins as facilitators of protein folding. Biochim. Biophys. Acta 2008, 1783, 641–650. [Google Scholar] [CrossRef] [PubMed]
- Montecucco, C.; Rasotto, M.B. On botulinum neurotoxin variability. Mbio 2015, 6, E02131-14. [Google Scholar] [CrossRef] [PubMed]
- Pirazzini, M.; Leka, O.; Zanetti, G.; Rossetto, O.; Montecucco, C. On the translocation of botulinum and tetanus neurotoxins across the membrane of acidic intracellular compartments. Biochim. Bioph. Acta Biomembr. 2016, 1858, 467–474. [Google Scholar] [CrossRef] [PubMed]
- Sim, W.S. Application of Botulinum Toxin in Pain Management. Korean J. Pain 2011, 24, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Rummel, A.; Eichner, T.; Weil, T.; Karnath, T.; Gutcaits, A.; Mahrhold, S.; Sandhoff, K.; Proia, R.L.; Acharya, K.R.; Bi galke, H.; et al. Identification of the receptor binding site of botulinum neurotoxins B and G proves the double-receptor concept. Proc. Natl. Acad. Sci. USA 2007, 104, 359–364. [Google Scholar] [CrossRef] [PubMed]
- Nishiki, T.; Tokuyama, Y.; Kamata, Y.; Nemoto, Y.; Yoshida, A.; Sato, K.; Sekiguchi, M.; Takahashi, M.; Kozaki, S. The high-affinity binding of Clostridium botulinum type B neurotoxin to synaptotagmin II associated with gangliosides GT1b/GD1a. FEBS Lett. 1996, 378, 253–257. [Google Scholar] [CrossRef]
- Dressler, D.; Saberi, F.A. Botulinum toxin: Mechanism of action. Eur. Neurol. 2005, 53, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Bahat, P.Y.; Çetin, B.A.; Turan, G. Vaginismus treatment with libido increase and practice. Int. J. Reprod. Contracept. Obstet. Gynecol. 2017, 6, 3167–3169. [Google Scholar] [CrossRef]
- Lamont, J.A. Vaginismus. Am. J. Obstet. Gynecol. 1978, 131, 633–636. [Google Scholar] [CrossRef]
- Ghazizadeh, S.; Nikzad, M. Botulinum Toxin in the Treatment of Refractory Vaginismus. Obstet. Gynecol. 2004, 104, 922–925. [Google Scholar] [CrossRef] [PubMed]
- Shafik, A.; El-Sibai, O. Vaginismus: Results of treatment with botulin toxin. J. Obstet. Gynaecol. 2000, 20, 300–302. [Google Scholar] [CrossRef] [PubMed]
- Bertolasi, L.; Frasson, E.; Cappelletti, J.Y.; Vicentini, S.; Bordignon, M.; Graziottin, A. Botulinum Neurotoxin Type A Injections for Vaginismus Secondary to Vulvar Vestibulitis Syndrome. Obstet. Gynecol. 2009, 114, 1008–1016. [Google Scholar] [CrossRef] [PubMed]
- Pacik, P.T. Botox Treatment for Vaginismus. Plast. Reconstr. Surg. 2009, 124, 455e–456e. [Google Scholar] [CrossRef] [PubMed]
- Pacik, P.T. Understanding and treating vaginismus: A multimodal approach. Int. Urogynecol. J. 2014, 25, 1613–1620. [Google Scholar] [CrossRef] [PubMed]
- Pacik, P.T.; Geletta, S. Vaginismus Treatment: Clinical Trials Follow Up 241 Patients. Sex. Med. 2017, 5, e114–e123. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.; Chung, W.S.; Shim, B.S. Botulinum toxin A for the management of vulvodynia. Int. J. Impot. Res. 2007, 19, 84–87. [Google Scholar] [CrossRef] [PubMed]
- Dollery, C. Therapeutic Drugs, 2nd ed.; Churchill Livingstone: New York, NY, USA, 1999. [Google Scholar]
- Goldstein, A.T.; Marinoff, S.C.; Haefner, H.K. Vulvodynia: Strategies for treatment. Clin. Obstet. Gynecol. 2005, 48, 769–785. [Google Scholar] [CrossRef] [PubMed]
- Petersen, C.D.; Lundvall, L.; Kristensen, E.; Giraldi, A. Botulinum Toxin Type A- A Novel Treatment for Provoked Vestibulodynia? Results from a Randomized, Placebo Controlled, Double Blinded Study. J. Sex. Med. 2008, 87, 893–901. [Google Scholar] [CrossRef] [PubMed]
- Zolnoun, D.; Hartmann, K.; Lamvu, G.; As-Sanie, S.; Maixner, W.; Steege, J. A conceptual model for the pathophysiology of vulvar vestibulitis syndrome. Obstet. Gynecol. Surv. 2006, 61, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Friedrich, E.G., Jr. Vulvar vestibulitis syndrome. J. Reprod. Med. 1987, 32, 110–114. [Google Scholar] [PubMed]
- Pelletier., F.; Parratte, B.; Penz, S.; Moreno, J.P.; Aubin, F.; Humbert, P. Efficacy of high doses of botulinum toxin A for treating provoked vestibulodynia. Br. J. Dermatol. 2011, 164, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.; Kim, Y.; Shim, B.; Yoon, H.; Park, Y.; Shim, B.; Jeong, W.; Lee, D. A retrospective study of the management of vulvodynia. Korean J. Urol. 2013, 54, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.A.; Wiffen, P.J.; Derry, S.; McQuay, H.J. Gabapentin for chronic neuropathic pain and fibromyalgia in adults. Cochrane Database Syst. Rev. 2011, 3, CD007938. [Google Scholar]
- Falsetta, M.L.; Foster, D.C.; Bonham, A.D.; Phipps, R.P. A review of the available clinical therapiers for vulvodynia management and new data implicating pro-inflammatory mediators in pain elicitation. BJOG 2017, 124, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Mathias, S.; Kupperman, M.; Liberman, R.F.; Lipschutz, R.C.; Steege, J.F. Chronic pelvic pain: Prevalence, health related quality and economic correlates. Obstet. Gynecol. 1996, 87, 321–327. [Google Scholar] [CrossRef]
- Srinivasa, A.K.; Kaye, J.D.; Moldwin, R. Myofascial dysfunction associated with chronic pelvic floor pain: Management strategies. Curr. Pain Headache Rep. 2007, 11, 359–364. [Google Scholar] [CrossRef]
- Qeramaa, E.; Fuglsang-Frederiksena, A.; Jensen, T.S. The role of botulinum toxin in management of pain: An evidencebased review. Curr. Opin. Anaesthesiol. 2010, 23, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Adelowo, A.; Hacker, M.R.; Shapiro, A.; Merport Modest, A.; Elkadry, E. Botulinum Toxin Type A (BOTOX) for Refractory Myofascial Pelvic Pain. Female Pelvic. Med. Reconstr. Surg. 2013, 19, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Abbott, J.A.; Jarvis, S.K.; Lyons, S.D.; Thomson, A.; Vancaille, T.G. Botulinum Toxin Type A for Chronic Pain and Pelvic Floor Spasm in Women. A Randomized Controlled Trial. Obstet. Gynecol. 2006, 108, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Klimek, L.; Bergmann, C.K.; Biedermann, T.; Bousquet, J.; Hellings, P.; Jung, K.; Merk, H.; Olze, H.; Schlenter, W.; Stock, P.; et al. Visual analogue scales (VAS): Measuring instruments for the documentation of symptoms and therapy monitoring in cases of allergic rhinitis in everyday health care. Allergo. J. Int. 2017, 26, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Gajraj, N.M. Botulinum Toxin a Injection of the Obturator Internus Muscle for Chronic Perineal Pain. J. Pain. 2005, 6, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Jarvis, S.K.; Abbott, J.A.; Lenart, M.B.; Steensma, A.; Vancaillie, T.G. Pilot study of botulinum toxin type A in the treatment of chronic pelvic pain associated with spasm of the levator ani muscles. Aust. N. Z. J. Obstet. Gynaecol. 2004, 44, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Morrissey, D.; El-Khawand, D.; Ginzburg, N.; Wehbe, S.; O’Hare, P.; Whitmore, K. Botulinum Toxin a Injections into Pelvic Floor Muscles under Electromyographic Guidance for Women with Refractory High-Tone Pelvic Floor Dysfunction: A 6-Month Prospective Pilot Study. Female Pelvic. Med. Reconstr. Surg. 2015, 21, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Charioni, G.; Nardo, A.; Vantini, I.; Romito, A.; Whitehead, W.E. Biofeedback Is Superior to Electrogalvanic Stimulation and Massage for Treatment of Levator Ani Syndrome. Gastroenterol 2010, 138, 1321–1329. [Google Scholar] [CrossRef] [PubMed]
- Rao, S.C.C.; Paulson, J.; Mata, M.; Zimmerman, B. Clinical trial: Effects of botulinum toxin on levator ani syndrome—A double-blind, placebo-controlled study. Aliment. Pharmacol. Ther. 2009, 29, 985–991. [Google Scholar] [CrossRef] [PubMed]
- Jhang, J.F.; Kuo, H.C. Novel treatment of chronic bladder pain syndrome and other pelvic pain disorders by onabotulinumtoxinA injection. Toxins 2015, 7, 2232–2250. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Cheng, J.; Dai, J.; Zhang, D. Botulinum toxin decreases hyperalgesia and inhibits P2X3 receptor over-expression in sensory neurons induced by ventral root transection in rats. Pain Med. 2011, 12, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Montenegro, M.L.; Mateus-Vasconcelos, E.C.; Rosa e Silva, J.C.; Nogueira, A.A.; Dos Reis, F.J.; Poli Neto, O.B. Importance of pelvic muscle tenderness evaluation in women with chronic pelvic pain. Pain 2010, 11, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Tu, F.F.; As-Sanie, S.; Steege, J.F. Prevalence of pelvic musculoskeletal disorders in a female chronic pelvic pain clinic. J. Reprod. Med. 2006, 51, 185–189. [Google Scholar] [CrossRef] [PubMed]
- Arezzo, J.C. Possible mechanisms for the effects of botulinum toxin on pain. Clin. J. Pain. 2002, 18, S125–S132. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, S.G.; McMahon, S.B. ATP as a peripheral mediator of pain. J. Auton. Nerv. Syst. 2000, 81, 187–194. [Google Scholar] [CrossRef]
- Kaya, S.; Hermans, L.; Willems, T.; Roussel, N.; Meeus, M. Central sensitization in urogynecological chronic pelvic pain: A systematic literature review. Pain Phys. 2013, 16, 291–308. [Google Scholar]
- Aoki, K.R. Evidence for antinociceptive activity of botulinum toxin type A in pain management. Headache 2003, 43, S9–S15. [Google Scholar] [CrossRef] [PubMed]
- Foran, P.G.; Mohammed, N.; Lisk, G.O.; Nagwaney, S.; Lawrence, G.W.; Johnson, E.; Smith, L.; Aoki, K.R.; Dolly, J.O. Evaluation of the therapeutic usefulness of botulinum neurotoxin B, C1, E, and F compared with the long lasting type A. Basis for distinct durations of inhibition of exocytosis in central neurons. J. Biol. Chem. 2003, 278, 1363–1371. [Google Scholar] [CrossRef] [PubMed]
- Deepali, S.; Arunkalaivanan, A.S. New developments Botulinum toxin type A: Applications in urogynaecology. Obstet. Gynecol. 2006, 8, 177–180. [Google Scholar] [CrossRef]
- Apostolidis, A.; Dasgupta, P.; Denys, P.; Elneil, S.; Fowler, C.J.; Giannantoni, A.; Karsenty, G.; Schulte-Baukloh, H.; Schurch, B.; Wyndaele, J.J. Recommendations on the Use of Botulinum Toxin in the Treatment of Lower Urinary Tract Disorders and Pelvic Floor Dysfunctions: A European Consensus Report. Eur. Urol. 2009, 55, 100–120. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.P.; Radziszewski, P.; Borkowski, A.; Somogyi, G.T.; Boone, T.B.; Chancellor, M.B. Botulinum toxin a has antinociceptive effects in treating interstitial cystitis. Urology 2004, 64, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Pinto, R.A.; Silva, A.; Lopes, T.; Silva, J.F.; Silva, C.M.; Cruz, F.R.; O Dinis, P. Intratrigonal injection of botulinum toxin in patients with bladder pain syndrome- results at 9- months follow-up. J. Urol. 2009, 181, 20. [Google Scholar] [CrossRef]
- Giannantoni, A.; Costantini, E.; Di Stasi, S.M.; Mearini, E.; Santaniello, F.; Vianello, A.; Porena, M. Intravesical passive delivery of botulinum a toxin in patients affected by painful bladder syndrome: A pilot study. Eur. Urol. Suppl. 2007, 6, 246. [Google Scholar] [CrossRef]
- Giannantoni, A.; Porena, M.; Costantini, E.; Zucchi, A.; Mearini, L.; Mearini, E. Botulinum a Toxin Intravesical Injection in Patients with Painful Bladder Syndrome: 1-Year Followup. J. Urol. 2008, 179, 1031–1034. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.C. Preliminary Results of Suburothelial Injection of Botulinum a Toxin in the Treatment of Chronic Interstitial Cystitis. Urol. Int. 2005, 75, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Carl, S.; Grosse, J.; Laschke, S. Treatment of Interstitial Cystitis with Botulinum toxin type A. Eur. Urol. Suppl. 2007, 6, 248. [Google Scholar] [CrossRef]
- Ramsay, A.; Small, D.; Conn, G. Intravesical Botulinum Toxin type A in Interstitial Cystitis. Eur. Urol. Suppl. 2007, 6, 248. [Google Scholar] [CrossRef]
- Pinto, R.; Lopes, T.; Silva, J.; Silva, C.; Dinis, P.; Cruz, F. Persistent Therapeutic Effect of Repeated Injections of Onabotulinum Toxin A in Refractory Bladder Pain Syndrome/Interstitial Cystitis. J. Urol. 2013, 189, 548–553. [Google Scholar] [CrossRef] [PubMed]
- Apostolidis, A.; Dasgupta, P.; Fowler, C.J. Proposed mechanism for the efficacy of injected botulinum toxin in the treatment of human detrusor overactivity. Eur. Urol. 2006, 49, 644–650. [Google Scholar] [CrossRef] [PubMed]
- Andersson, K.E.; Wein, A.J. Pharmacology of the lower urinary tract: Basis for current and future treatments of urinary incontinence. Pharmacol. Rev. 2004, 56, 581–631. [Google Scholar] [CrossRef] [PubMed]
- Karsenty, G.; Denys, P.; Amarenco, G.; De Seze, M.; Gamé, X.; Haab, F.; Kerdraon, J.; Perrouin-Verbe, B.; Ruffion, A.; Saussine, C.; et al. Botulinum toxin A (Botox®) intradetrusor injections in adults with neurogenic detrusor overactivity/neurogenic overactive bladder: A systematic literature review. Eur. Urol. 2008, 53, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, P.F.; Chiu, H.C.; Chen, K.C.; Chang, C.H.; Chou, E.C. Botulinum toxin A for the Treatment of Overactive Bladder. Toxins 2016, 8, 59. [Google Scholar] [CrossRef] [PubMed]
- Atiemo, H.; Wynes, J.; Chuo, J.; Nipkow, L.; Sklar, G.N.; Chai, T.C. Effect of Botulinum toxin on detrusor overactivity induced by intravesical adenosine triphosphate and capsaicin in a rat model. Urology 2005, 65, 622–626. [Google Scholar] [CrossRef] [PubMed]
- Brady, C.M.; Apostolidis, A.N.; Harper, M.; Yiangou, Y.; Beckett, A.; Jacques, T.S.; Freeman, A.; Scaravilli, F.; Fowler, C.J.; Anand, P. Parallel changes in bladder suburothelial vanilloid receptor TRPV1 (VR1) and pan-neuronal marker PGP9.5 immunoreactivity in patients with neurogenic detrusor overactivity (NDO) following intravesical resiniferatoxin treatment. BJU Int. 2004, 93, 770–776. [Google Scholar] [CrossRef] [PubMed]
- Brady, C.; Apostolidis, A.; Yiangou, Y.; Baecker, P.A.; Ford, A.P.; Freeman, A.; Jacques, T.S.; Fowler, C.J.; Anand, P. P2X3-immunoreactive nerve fibres in neurogenic detrusor overactivity and the effect of intravesical resiniferatoxin (RTX). Eur. Urol. 2004, 46, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Apostolidis, A.; Popat, R.; Yiangou, Y.; Cockayne, D.; Ford, A.P.; Davis, J.B.; Dasgupta, P.; Fowler, C.J.; Anand, P. Decreased sensory receptors P2X3 and TRPV1 in suburothelial nerve fibers following intradetrusor injections of Botulinum toxin for human detrusor overactivity. J. Urol. 2005, 174, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Smet, P.J.; Moore, K.H.; Jonavicius, J. Distribution and colocalization of calcitonin gene-related peptide, tachykinins, and vasoactive intestinal peptide in normal and idiopathic unstable human urinary bladder. Lab. Investig. 1997, 77, 37–49. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.C.; Yoshimura, N.; Huang, C.C.; Chiang, P.H.; Chancellor, M.B. Intravesical Botulinum toxin A administration produces analgesia against acetic acid induced bladder pain responses in rats. J. Urol. 2004, 172, 1529–1532. [Google Scholar] [CrossRef] [PubMed]
- Lavin, S.T.; Southwell, B.R.; Murphy, R.; Jenkinson, K.M.; Furness, J.B. Activation of neurokinin 1 receptors on interstitial cells of Cajal of the guinea-pig small intestine by substance P. Histochem. Cell Biol. 1998, 110, 263–271. [Google Scholar] [CrossRef]
- Hannestad, Y.S.; Rortveit, G.; Sandvik, H.; Hunskaar, S. A community-based epidemiological survey of female urinary incontinence: The Norwegian EPINCONT study. Epidemiology of Incontinence in the County of NordTrondelag. J. Clin. Epidemiol. 2000, 53, 1150–1157. [Google Scholar] [CrossRef]
- Cvach, K.; Dwyer, P. Overactive bladder in women: Achieving effective management. Online Med. Today 2015, 16, 41–51. [Google Scholar]
- Le Normand, P.D.; Ghout, I.; Costa, P.; Chartier-Kastler, E.; Grise, P.; Hermieu, J.F.; Amarenco, G.; Karsenty, G.; Saussine, C.; Barbot, F. Efficacy and Safety of Low Doses of OnabotulinumtoxinA for the Treatment of Refractory Idiopathic Overactive Bladder: A Multicentre, Double-Blind, Randomised, Placebo-Controlled Dose-Ranging Study. Eur. Urol. 2012, 61, 520–529. [Google Scholar] [CrossRef]
- Popat, R.; Apostolidis, A.; Kalsi, V.; Gonzales, G.; Fowler, C.J. A comparison between the response of patient with idiopathic detrusor overactivity and neurogenic detrusor overactivity to the first intradetrusor injection of botulinum- A toxin. J. Urol. 2005, 174, 984–989. [Google Scholar] [CrossRef] [PubMed]
- Schmid, D.M.; Sauermann, P.; Werner, M.; Perucchini, D.; Sulser, T.; Schurch, B. Experiences including 5 year results of 180 cases treated with Botulinum-A Toxin Injections into the Detrusor muscle for Overactive Bladder refractory to Anticholinergics. Eur. Urol. Suppl. 2007, 6, 246. [Google Scholar] [CrossRef]
- Brubaker, L.; Richter, H.E.; Visco, A.; Mahajan, S.; Nygaard, I.; Braun, T.M.; Barber, M.D.; Menefee, S.; Schaffer, J.; Weber, A.M.; et al. Refractory Idiopathic Urge Urinary Incontinence and Botulinum A Injection. J. Urol. 2008, 180, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Khanlow, S.; Kesslerlow, T.M.; Apostolidis, A.; Kalsi, V.; Panicker, J.; Roosen, A.; Gonzales, G.; Haslam, C.; Elneil, S. What a Patient with Refractory Idiopathic Detrusor Overactivity Should Know about Botulinum Neurotoxin Type A Injection. J. Urol. 2009, 181, 1773–1778. [Google Scholar] [CrossRef]
- Dowson, C.; Watkins, J.; Khan, M.S.; Dasgupta, P.; Sahai, A. Repeated Botulinum Toxin Type A Injections for Refractory Overactive Bladder: Medium-Term Outcomes, Safety Profile, and Discontinuation Rates. Eur. Urol. 2011, 61, 834–839. [Google Scholar] [CrossRef] [PubMed]
- Moga, M.A.; Banciu, S.; Dimienescu, O.; Bigiu, N.F.; Scarneciu, I. Botulinum-A Toxin’s efficacy in the treatment of idiopathic overactive bladder. J. Pak. Med. Assoc. 2015, 65, 76–80. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
 |  |  |  |  |  |  |
| Neuromuscular Disorders | Ophthalmic Disorders | Chronic Pain | Cosmetic and Dermatological Applications | Pelvic floor Disorders | Gastrointestinal Disorders | Spasticity |
| Idiopathic/secondary focal dystonia | Misalignment | Tension headache | Wrinkles | Anismus | Achalasia | Stoke induced spasticity |
| Hemifacial Spasm/post-facial nerve palsy synkinesis | Paralytic strabismus | Cervicogenic headache | Face rejuvenation | Vaginismus | Bruxism | Cephalic tetanus |
| Tremor (essential, writing, palatal or cerebellar) | Therapeutic ptosis for corneal protection | Migraine | Hypersecretory disorders (hyperhidrosis, sialorrhea) | Detrusor sphincter dyssynergia | Temporomandibular joint dysfunction | Multiple sclerosis |
| Tic disorders | Restrictive or myogenic strabismus | Lower back ache | Glabellar frown | Chronic anal fissures | Palatal myoclonus | Traumatic brain injury |
| Myokymia | Upper eyelid retraction | Tennis elbow | Vertical platysma bands | Perineal muscles spasm | Esophageal diverticulosis | Cerebral palsy |
| Neuromyotonia | Duane’s syndrome | Myofascial pain | Browlift | Vulvodynia | Laryngeal disorders | Spinal cord injury |
| Origin | BoNT Serotype | Target Substrate | Bont Subtype | Substrate Localization | |
|---|---|---|---|---|---|
| C. Botulinum group I | A | SNAP-25 | A1; A2; A3; A4; A5; A6; A7; A8; A9; A10; A(B); Ab; Af; Af84 | Presynaptic plasma membrane | |
| B | VAMP | B1; B2; B3; B5(Be); B6; B7; Bf | Synaptic vesicle | ||
| F | VAMP1, VAMP2 | F1; F2; F3; F4; F5 | Synaptic vesicle | ||
| X | VAMP4, VAMP5, Ykt6 | - | Synaptic vesicle | ||
| C. Botulinum group II | B | VAMP | B4 | Synaptic vesicle | |
| E | SNAP 25 | E1; E2; E3; E6; E7; E8; E9; E10 | Presynaptic plasma membrane | ||
| F | VAMP1, VAMP2 | F6 | Synaptic vesicle | ||
| C. Botulinum group III | C | SNAP 25, Syntaxin 1A, Syntaxin 1b | C; CD; | Presynaptic plasma membrane | |
| D | VAMP1, VAMP2 | D; DC | Synaptic vesicle | ||
| C. Botulinum group IV (C. argentinese) | G | VAMP1, VAMP2 | G | Synaptic vesicle | |
| Other organisms producing BoNTs | C. Butyricum | E | SNAP 25 | E4; E5 | Presynaptic plasma membrane |
| C. Baratii | F | VAMP1, VAMP2 | F4 | Synaptic vesicle | |
| Enterococcus faecium strain | En | VAMP2, SNAP25 | - | Synaptic vesicle | |
| Weissella oryzae SG25T | Wo | VAMP2 | - | Synaptic vesicle | |
| Author | Study Design | Number of Cases | Treatment Regimen | Outcome Measures | Follow-Up | Results |
|---|---|---|---|---|---|---|
| Ghazizadeh [54] | Retrospective study | 24 | Dilution: 500 U of BoNT-A diluted with 1.5 mL of normal saline solution. Dose: 150–200 U injected first; the dose gradually increased the total dose of 400 U * Dysport, Ipsen Ltd., Maidenhead, UK |
| 12.37 months |
|
| Shafik [55] | Case-control study | 13 | BoNT group: A single injection; dose and dilution: 25 U diluted in 1 mL saline solution Control group: saline solution |
| 3.3 months |
|
| Bertolasi [56] | Prospective study | 39 | Repeated cycles at 4 weeks of botulinum neurotoxin injected into levator ani. * Dysport, Ipsen Ltd., Maidenhead, UK |
| 105 (±50 SD) weeks |
|
| Pacik [57] | Retrospective study | 20 | Dose: 100 to 150 U of BoNT-A; Dilution: 100 U of BoNT-A diluted in 2 mL of saline; * Allergan, Inc., Irvine, CA, USA. |
| Time of follow up not reported |
|
| Pacik [59] | Clinical trial | 241 | Dose: 100 U of BoNT-A; Dilution: 2 mL of saline; * onabotulinumtoxinA; Allergan, Irvine, CA, USA |
| 1 month, 3 months, 6 months, 1 year |
|
| Author | Study Design | Number of Cases | Treatment Regimen | Outcome Measures | Follow-Up | Results |
|---|---|---|---|---|---|---|
| Yoon [60] | Retrospective study | 7 | Dilution: 20 U of the BoNT diluted in saline solution; Dose: 20 U of BoNT-A * Botox, Allegran, Inc., Irvine, CA, USA |
| 4–24 months |
|
| Petersen [63] | Randomized, double blinded, placebo-controlled study | 32 cases 32 placebo | Dilution: 100 U of BoNT-A diluted in 2.5 mL saline solution; Dose: 20 U of the BoNT diluted or 0.5 mL of saline (placebo) * Botox, Allergan |
| 3, 6, 9, and 12 months |
|
| Pelletier [66] | Retrospective study | 20 | Dilution: 1 mL: 50 U BoNT-A diluted in 1 mL saline; Dose: 50 UIBoNT diluted * Botox; Allergan, Courbevoie, France |
| 3, 6 months |
|
| Jeon [67] | Retrospective study | 73 | Dose: 40 to 100 U BoNT-A (11 patients) 300 to 600 mg Gabapentin (62 patients) * Botox, Allegran Inc., Irvine, CA, USA |
| 6 to 24 months |
|
| Author | Study Design | Number of Cases | Treatment Regimen | Outcome Measures | Follow-Up | Results |
|---|---|---|---|---|---|---|
| Adelowo [73] | Retrospective cohort study | 31 | Dose: 100–300 U BoNT-A * Botox, Allergan Inc. Irvine, CA, USA |
| <6 weeks post-injection (visit 1) and ≥6 weeks post injection (visit 2). |
|
| Abott [74] | Double-blinded, randomized, placebo-controlled trial. | 60 | Cases: 80 U BoNT-A (20 units/mL) Placebo: 4 mL of saline solution * Botox, Allergan Westport, Ireland |
| 0, 1, 2, 3, 4, 5 and 6 months |
|
| Jarvis [77] | Prospective study | 12 | Dose: 40 U BoNT; Dilutions: 10 U/mL; 20 U/mL; and 100 U/mL. * Allergan (Gordon, New South Wales, Australia). |
| 2, 4, 8 and 12 weeks post-treatment |
|
| Morrissey [78] | Prospective pilot open-label study | 21 | Dose: up to 300 U BoNT-A Administration: using needle electromyography guidance, from a transperineal approach, to localize spastic pelvic floor muscles * Botox; Allergan, Irvine, CA, USA |
| 6 months (4, 8, 12, and 24 weeks after injections) |
|
| Rao [80] | Randomized, placebo-controlled study | 12 | Cases: 100 U of BoNT-A intra sphincterian (anal) at 3 months intervals; Placebo: saline solution * Botox; Allergan Pharmaceuticals, Los Angeles, CA, USA) |
| NR |
|
| Author | Study Design | Number of Cases | Treatment Regimen | Outcome Measures | Follow-Up | Results |
|---|---|---|---|---|---|---|
| Pinto [93] | Prospective study | 17 | Dose: 100 U of Botulin toxin Administration: bladder trigone only, under cystoscopy guidance * Botox (Allergan, Inc., Irvine, CA, USA) |
| 9 months |
|
| Giannantoni [94] | Prospective Study | 7 | Dose: 200 U BoNT-A, diluted in 100 mL saline, without any form of anesthesia. Administration: intravesical instillation, retained in the bladder for 40 mi * Botox (Allergan, Inc., Irvine, CA, USA) |
| 3 months |
|
| Giannantoni [95] | Prospective study | 15 | Dose: 200 U BoNT-A diluted in 20 mL saline; * Botox (Allergan, Inc., Irvine, CA, USA) |
| 12 months |
|
| Kuo [96] | Prospective study | 10 | Dose: In 5 patients, 100 U of BoNT-A; additional 100 U BoNT-A into the trigone in the other 5 patients. Administration: suburothelial into 20 sites * Botox, Allergan Inc. Irvine, CA, USA |
| 3 months |
|
| Carl [97] | Two center pilot study | 29 | Dose:500 U BoNT-A diluted in 3 mL saline Administration: injected through a rigid cystoscope into 20–25 sites submucosally in the trigone and bladder floor. * Dysport® (Ipsen Pharma, Ettlingen, Germany |
| 6 months |
|
| Ramsay [98] | Prospective study | 11 | Dose: 200–300 U-BoNT-A; Administration: BoNT was injected in 20–30 different sites (10 U per site) into the suburothelium of the bladder * source of toxin not reported |
| 14 weeks |
|
| Pinto [99] | Prospective study | 16 | Dose: 100 U BoNT-A Administration: 4 consecutive injections of BoNT-A injected intratrigonal under cystoscopic guidance * Botox (Allergan, Inc., Irvine, CA, USA) |
| 12 months |
|
| Author | STUDY DESIGN | Number of Cases | Treatment Regimen | Outcome Measures | Follow-Up | Results |
|---|---|---|---|---|---|---|
| Le Normand [113] | Prospective, randomized, double-blind, placebo-controlled comparative study | 99 | Dose: 50 U, 100 U or 150 U BoNT-A Administration: intradetrusor injection * Botox (Allergan, Inc., Irvine, CA, USA) |
| day 8; 1, 3, 5, and 6 months |
|
| Popat [114] | Prospective, open label study | 75 | Dose: 300 U (NOB) or 200 U (IOB) of BoNT Administration: injected into the bladder * Botox (Allergan, Inc., Irvine, CA, USA) |
| 1 month and 4 months |
|
| Schmid [115] | Prospective study | 180 (45 men, 135 women) | Dose: 100 U of BTX-A into the detrusor at 30 different sites. Reinjection: 52/180 of patients were reinjected after the effect had diminished (time interval between two treatments was mean 11 months) * Botox (Allergan, Inc., Irvine, CA, USA) |
| After 4, 12 and 36 weeks |
|
| Brubaker [116] | Randomized, double-blind, placebo controlled, review | 43 | Dose: 200 U BoNT dissolved in 6 mL saline Placebo: 3 mL saline. * Botox (Allergan, Inc., Irvine, CA, USA) |
| 12 months |
|
| Khanlow [117] | Prospective, open label study | 81 | Dose: 200 U BoNT-A Administration: intradetrusor injections at 20 sites per injection * Botox (Allergan, Inc., Irvine, CA, USA) |
| NR |
|
| Dowson [118] | Prospective study | 100 | Dose: 200 U BoNT-A Administration: into suburothelium or detrusor muscle under cystoscopic guidance * Onabotulinumtoxin A; Allergan Ltd., Marlow, Buckinghamshire, UK |
| To five BoNT-A injections. |
|
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moga, M.A.; Dimienescu, O.G.; Bălan, A.; Scârneciu, I.; Barabaș, B.; Pleș, L. Therapeutic Approaches of Botulinum Toxin in Gynecology. Toxins 2018, 10, 169. https://doi.org/10.3390/toxins10040169
Moga MA, Dimienescu OG, Bălan A, Scârneciu I, Barabaș B, Pleș L. Therapeutic Approaches of Botulinum Toxin in Gynecology. Toxins. 2018; 10(4):169. https://doi.org/10.3390/toxins10040169
Chicago/Turabian StyleMoga, Marius Alexandru, Oana Gabriela Dimienescu, Andreea Bălan, Ioan Scârneciu, Barna Barabaș, and Liana Pleș. 2018. "Therapeutic Approaches of Botulinum Toxin in Gynecology" Toxins 10, no. 4: 169. https://doi.org/10.3390/toxins10040169
APA StyleMoga, M. A., Dimienescu, O. G., Bălan, A., Scârneciu, I., Barabaș, B., & Pleș, L. (2018). Therapeutic Approaches of Botulinum Toxin in Gynecology. Toxins, 10(4), 169. https://doi.org/10.3390/toxins10040169