Rapid, Sensitive, and Accurate Point-of-Care Detection of Lethal Amatoxins in Urine

 , , ,
, , , 
Abstract
:
1. Introduction
2. Results and Discussion
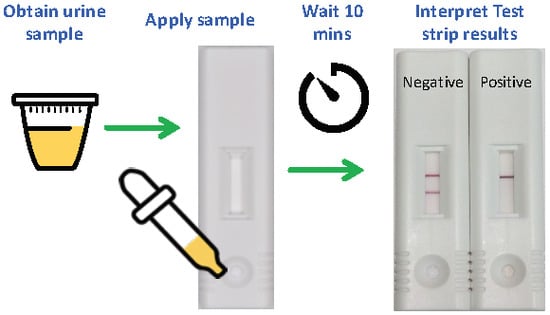
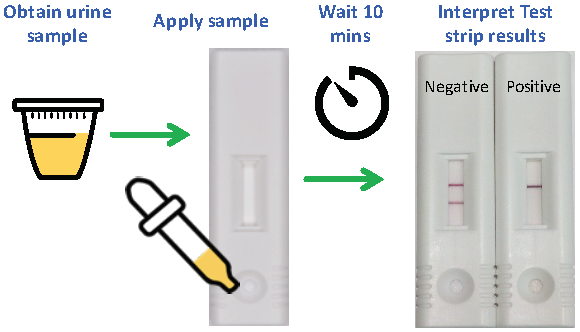
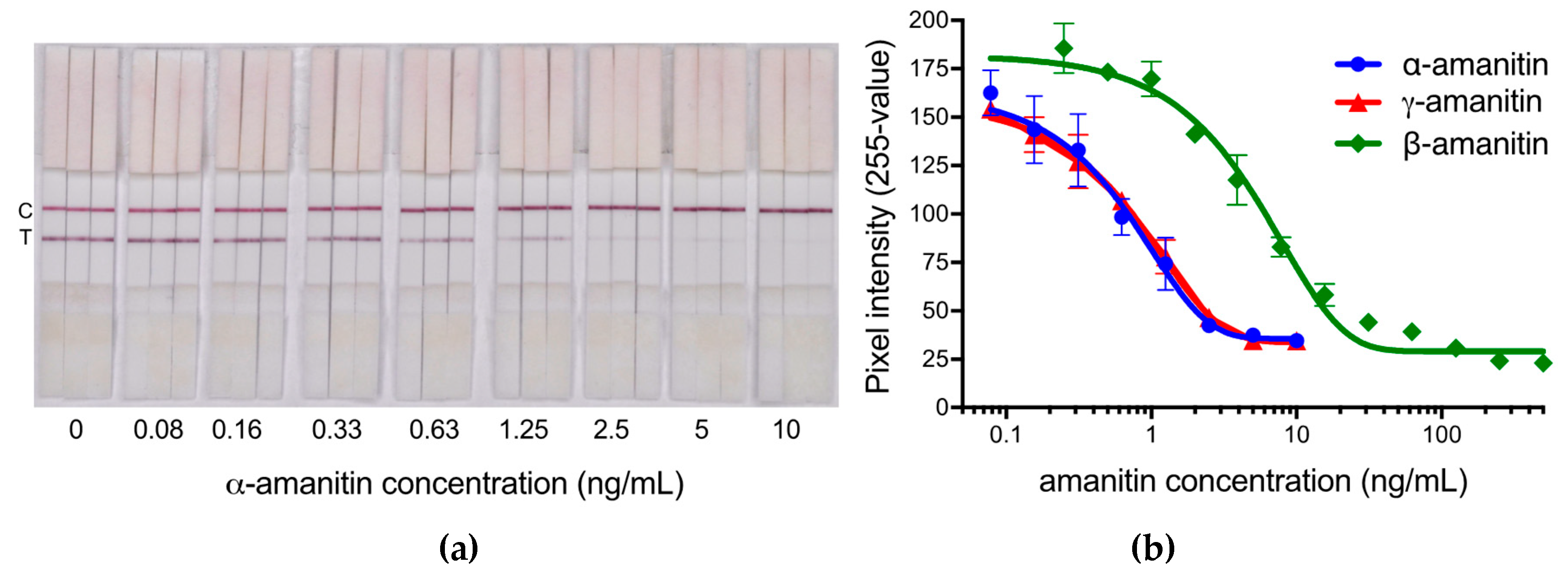
2.1. Analytical Sensitivity of the LFIA and Interpretation of Results
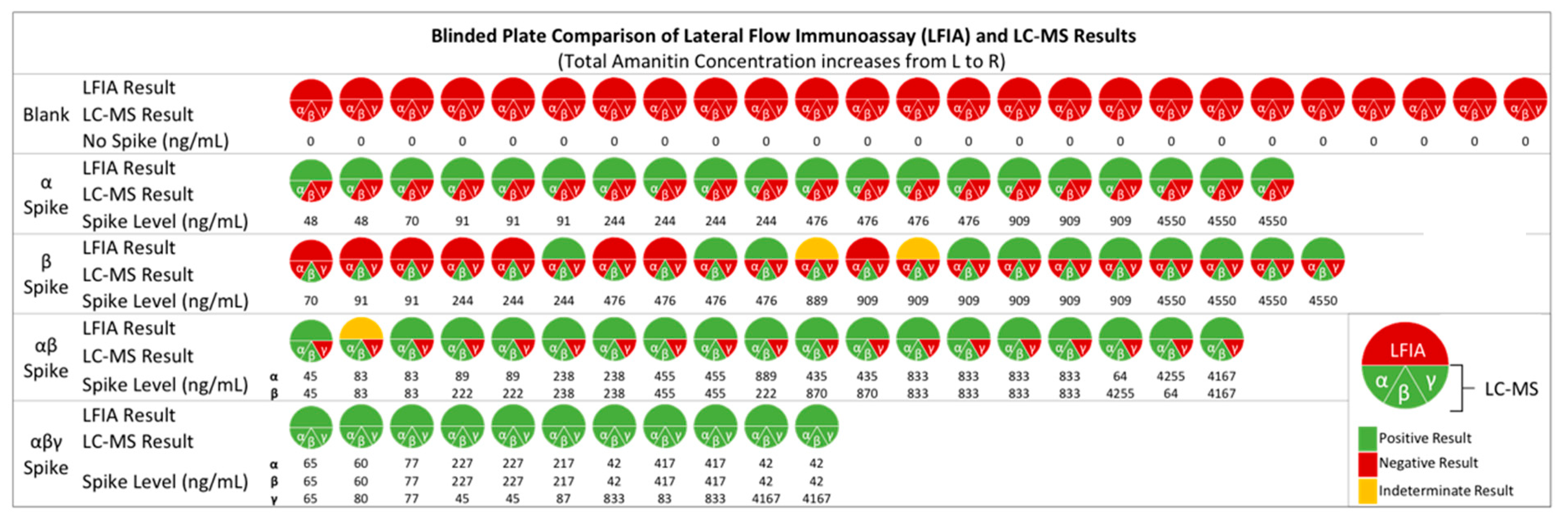
2.2. Detection of Amatoxins in Blind Fortified Human Urine Samples
2.3. Detection of Amatoxins in Dog Urine Samples
3. Materials and Methods
3.1. Materials and Approvals
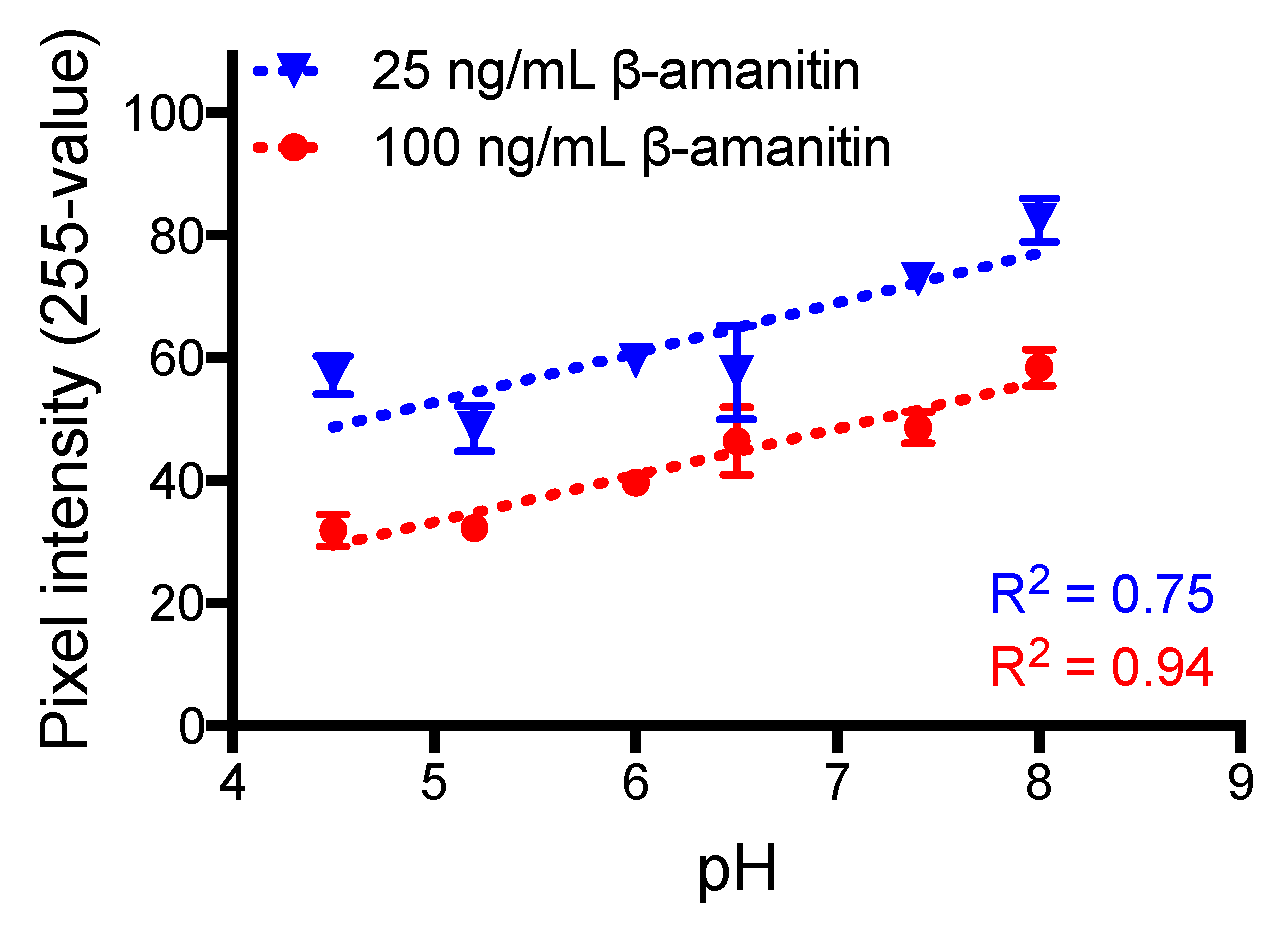
3.2. Analytical Sensitivity of the LFIA
3.3. Amatoxin-Fortified Human Urine Analysis
| False positive (FP) = | LFIA positive, although the amatoxin concentration was below the cut-off value |
| False negative (FN) = | LFIA negative, although the amatoxin concentration was above the cut-off value |
| Diagnostic sensitivity = | TP/(TP + FN) |
| Diagnostic specificity = | TN/(TN+ FP) |
| Single-study diagnostic efficiency = | (TP + TN)/(TP |
3.4. Collected Dog Urine Analysis for Amatoxins
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Disclaimer
References
- Brandenburg, W.E.; Ward, K.J. Mushroom poisoning epidemiology in the United States. Mycologia 2018, 110, 637–641. [Google Scholar] [CrossRef] [PubMed]
- Walton, J.D. The Cyclic Peptide Toxins of Amanita and Other Poisonous Mushrooms, 1st ed.; Springer Science & Business Media: New York, NY, USA, 2018. [Google Scholar]
- Kaya, E.; Karahan, S.; Bayram, R.; Yaykasli, K.O.; Colakoglu, S.; Saritas, A. Amatoxin and phallotoxin concentration in Amanita phalloides spores and tissues. Toxicol. Ind. Health 2015, 31, 1172–1177. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, I.; Ermis, F.; Akata, I.; Kaya, E. A case study: What doses of Amanita phalloides and amatoxins are lethal to humans? Wilderness Environ. Med. 2015, 26, 491–496. [Google Scholar] [CrossRef] [Green Version]
- Graeme, K.A. Mycetism: A review of the recent literature. J. Med. Toxicol. 2014, 10, 173–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, D.R. Mushrooms: Poisons and Panaceas: A Handbook for Naturalists, Mycologists, and Physicians; W. H. Freeman and Company: New York, NY, USA, 1995; p. 422. [Google Scholar]
- Li, Y.; Mu, M.Y.; Yuan, L.; Zeng, B.M.; Lin, S.D. Challenges in the early diagnosis of patients with acute liver failure induced by amatoxin poisoning two case reports. Medicine 2018, 97, e11288. [Google Scholar] [CrossRef] [PubMed]
- Costantino, D. Mushroom poisoning in Italy. Int. J. Artif Organs 1978, 1, 257–259. [Google Scholar] [CrossRef]
- Diaz, J.H. Amatoxin-containing mushroom poisonings: Species, toxidromes, treatments, and outcomes. Wilderness Environ. Med. 2018, 29, 111–118. [Google Scholar] [CrossRef] [Green Version]
- Koksal, O.; Armagan, E.; Inal, T.; Ayyildiz, T.; Oner, N. A 4 year retrospective analysis of our patients with mushroom poisoning. Hong Kong J. Emerg. Med. 2013, 20, 105–110. [Google Scholar] [CrossRef]
- Ward, J.; Kapadia, K.; Brush, E.; Salhanick, S.D. Amatoxin poisoning: Case reports and review of current therapies. J. Emerg. Med. 2013, 44, 116–121. [Google Scholar] [CrossRef]
- Jaeger, A.; Jehl, F.; Flesch, F.; Sauder, P.; Kopferschmitt, J. Kinetics of amatoxins in human poisoning—Therapeutic implications. J. Toxicol. Clin. Toxicol. 1993, 31, 63–80. [Google Scholar] [CrossRef]
- Butera, R.; Locatelli, C.; Coccini, T.; Manzo, L. Diagnostic accuracy of urinary amanitin in suspected mushroom poisoning: A pilot study. J. Toxicol. Clin. Toxicol. 2004, 42, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Niu, Y.M.; Zhang, Y.T.; Li, H.J.; Yin, Y.; Zhang, Y.Z.; Ma, P.B.; Zhou, J.; Huang, L.; Zhang, H.S.; et al. Toxicity and toxicokinetics of Amanita exitialis in beagle dogs. Toxicon 2018, 143, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Morel, S.; Fons, F.; Rapior, S.; Dubois, V.; Vitou, M.; Portet, K.; Dore, J.-C.; Poucheret, P. Decision-making for the detection of amatoxin poisoning: A comparative study of standard analytical methods. Cryptogam. Mycol. 2016, 37, 217–239. [Google Scholar] [CrossRef]
- Broussard, C.N.; Aggarwal, A.; Lacey, S.R.; Post, A.B.; Gramlich, T.; Henderson, J.M.; Younossi, Z.M. Mushroom poisoning—From diarrhea to liver transplantation. Am. J. Gastroenterol. 2001, 96, 3195–3198. [Google Scholar] [PubMed]
- Abbott, N.L.; Hill, K.L.; Garrett, A.; Carter, M.D.; Hamelin, E.I.; Johnson, R.C. Detection of alpha-, beta, and gamma-amanitin in urine by LC-MS/MS using 15N10-alpha-amanitin as the internal standard. Toxicon 2018, 152, 71–77. [Google Scholar] [CrossRef]
- Zhang, S.; Zhao, Y.F.; Li, H.J.; Zhou, S.; Chen, D.W.; Zhang, Y.Z.; Yao, Q.M.; Sun, C.Y. A simple and high-throughput analysis of amatoxins and phallotoxins in human plasma, serum and urine using UPLC-MS/MS combined with prime HLB elution platform. Toxins 2016, 8, 128. [Google Scholar] [CrossRef] [Green Version]
- Leite, M.; Freitas, A.; Azul, A.M.; Barbosa, J.; Costa, S.; Ramos, F. Development, optimization and application of an analytical methodology by ultra performance liquid chromatography-tandem mass spectrometry for determination of amanitins in urine and liver samples. Anal. Chim. Acta 2013, 799, 77–87. [Google Scholar] [CrossRef]
- Filigenzi, M.S.; Poppenga, R.H.; Tiwary, A.K.; Puschner, B. Determination of alpha-amanitin in serum and liver by multistage linear ion trap mass spectrometry. J. Agric. Food Chem. 2007, 55, 2784–2790. [Google Scholar] [CrossRef]
- Maurer, H.H.; Schmitt, C.J.; Weber, A.A.; Kraemer, T. Validated electrospray liquid chromatographic-mass spectrometric assay for the determination of the mushroom toxins alpha- and beta-amanitin in urine after immunoaffinity extraction. J. Chromatogr. B 2000, 748, 125–135. [Google Scholar] [CrossRef]
- Gicquel, T.; Lepage, S.; Fradin, M.; Tribut, O.; Duretz, B.; Morel, I. Amatoxins (alpha- and beta-amanitin) and phallotoxin (phalloidin) analyses in urines using high-resolution accurate mass LC-MS technology. J. Anal. Toxicol. 2014, 38, 335–340. [Google Scholar] [CrossRef] [Green Version]
- Defendenti, C.; Bonacina, E.; Mauroni, M.; Gelosa, L. Validation of a high performance liquid chromatographic method for alpha amanitin determination in urine. Forensic Sci. Int. 1998, 92, 59–68. [Google Scholar] [CrossRef]
- Abuknesha, R.A.; Maragkou, A. A highly sensitive and specific enzyme immunoassay for detection of beta-amanitin in biological fluids. Anal. Bioanal. Chem 2004, 379, 853–860. [Google Scholar] [CrossRef] [PubMed]
- Bühlmann Laboratories, A.G. Amanitin ELISA Product Insert; Catalog# ek-am1; Bühlmann Laboratories AG: Schönenbuch, Switzerland, 2013. [Google Scholar]
- Bever, C.S.; Adams, C.A.; Hnasko, R.M.; Cheng, L.W.; Stanker, L.H. Development and application of a lateral flow immunoassay for the rapid and sensitive detection of lethal amatoxins from mushrooms. Toxins 2020. under review. [Google Scholar]
- Enjalbert, F.; Gallion, C.; Jehl, F.; Monteil, H.; Faulstich, H. Amatoxins and phallotoxins in Amanita species-high-performance liquid-chromatographic determination. Mycologia 1993, 85, 579–584. [Google Scholar] [CrossRef]
- Yilmaz, I.; Kaya, E.; Sinirlioglu, Z.A.; Bayram, R.; Surmen, M.G.; Colakoglu, S. Clinical importance of toxin concentration in Amanita verna mushroom. Toxicon 2014, 87, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Staack, R.F.; Maurer, H.H. New Bühlmann ELISA for determination of amanitins in urine—Are there false positive results due to interferences with urine matrix, drugs or their metabolites? Toxichem. Krimtech. 2000, 68, 68–71. [Google Scholar]
- Cope, R.B. Mushroom poisoning in dogs. Vet. Med. 2007, 102, 95–100. [Google Scholar]
- Puschner, B.; Wegenast, C. Mushroom poisoning cases in dogs and cats: Diagnosis and treatment of hepatotoxic, neurotoxic, gastroenterotoxic, nephrotoxic, and muscarinic mushrooms. Vet. Clin. North Am. Small Anim. Pract. 2018, 48, 1053–1067. [Google Scholar] [CrossRef]
- Bever, C.S.; Barnych, B.; Hnasko, R.; Cheng, L.W.; Stanker, L.H. A new conjugation method used for the development of an immunoassay for the detection of amanitin, a deadly mushroom toxin. Toxins 2018, 10, 265. [Google Scholar] [CrossRef] [Green Version]
- Bever, C.S.; Hnasko, R.M.; Cheng, L.W.; Stanker, L.H. A rapid extraction method combined with a monoclonal antibody-based immunoassay for the detection of amatoxins. Toxins 2019, 11, 724. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnostic Parameter | Fortified Human Urine a | Intoxicated Dog Urine b |
|---|---|---|
| # of samples | n = 96 c | n = 38 |
| True positive (TP) | 60 | 8 |
| True negative (TN) | 28 | 22 |
| False positive (FP) | 0 | 0 |
| False negative (FN) | 5 | 8 |
| Sensitivity | 92.3% | 50% |
| Specificity | 100% | 100% |
| Efficiency | 94.6% | 78.9% |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bever, C.S.; Swanson, K.D.; Hamelin, E.I.; Filigenzi, M.; Poppenga, R.H.; Kaae, J.; Cheng, L.W.; Stanker, L.H. Rapid, Sensitive, and Accurate Point-of-Care Detection of Lethal Amatoxins in Urine. Toxins 2020, 12, 123. https://doi.org/10.3390/toxins12020123
Bever CS, Swanson KD, Hamelin EI, Filigenzi M, Poppenga RH, Kaae J, Cheng LW, Stanker LH. Rapid, Sensitive, and Accurate Point-of-Care Detection of Lethal Amatoxins in Urine. Toxins. 2020; 12(2):123. https://doi.org/10.3390/toxins12020123
Chicago/Turabian StyleBever, Candace S., Kenneth D. Swanson, Elizabeth I. Hamelin, Michael Filigenzi, Robert H. Poppenga, Jennifer Kaae, Luisa W. Cheng, and Larry H. Stanker. 2020. "Rapid, Sensitive, and Accurate Point-of-Care Detection of Lethal Amatoxins in Urine" Toxins 12, no. 2: 123. https://doi.org/10.3390/toxins12020123
APA StyleBever, C. S., Swanson, K. D., Hamelin, E. I., Filigenzi, M., Poppenga, R. H., Kaae, J., Cheng, L. W., & Stanker, L. H. (2020). Rapid, Sensitive, and Accurate Point-of-Care Detection of Lethal Amatoxins in Urine. Toxins, 12(2), 123. https://doi.org/10.3390/toxins12020123