Botulinum Toxin Injection for Medically Refractory Neurogenic Bladder in Children: A Systematic Review


Abstract
:1. Introduction
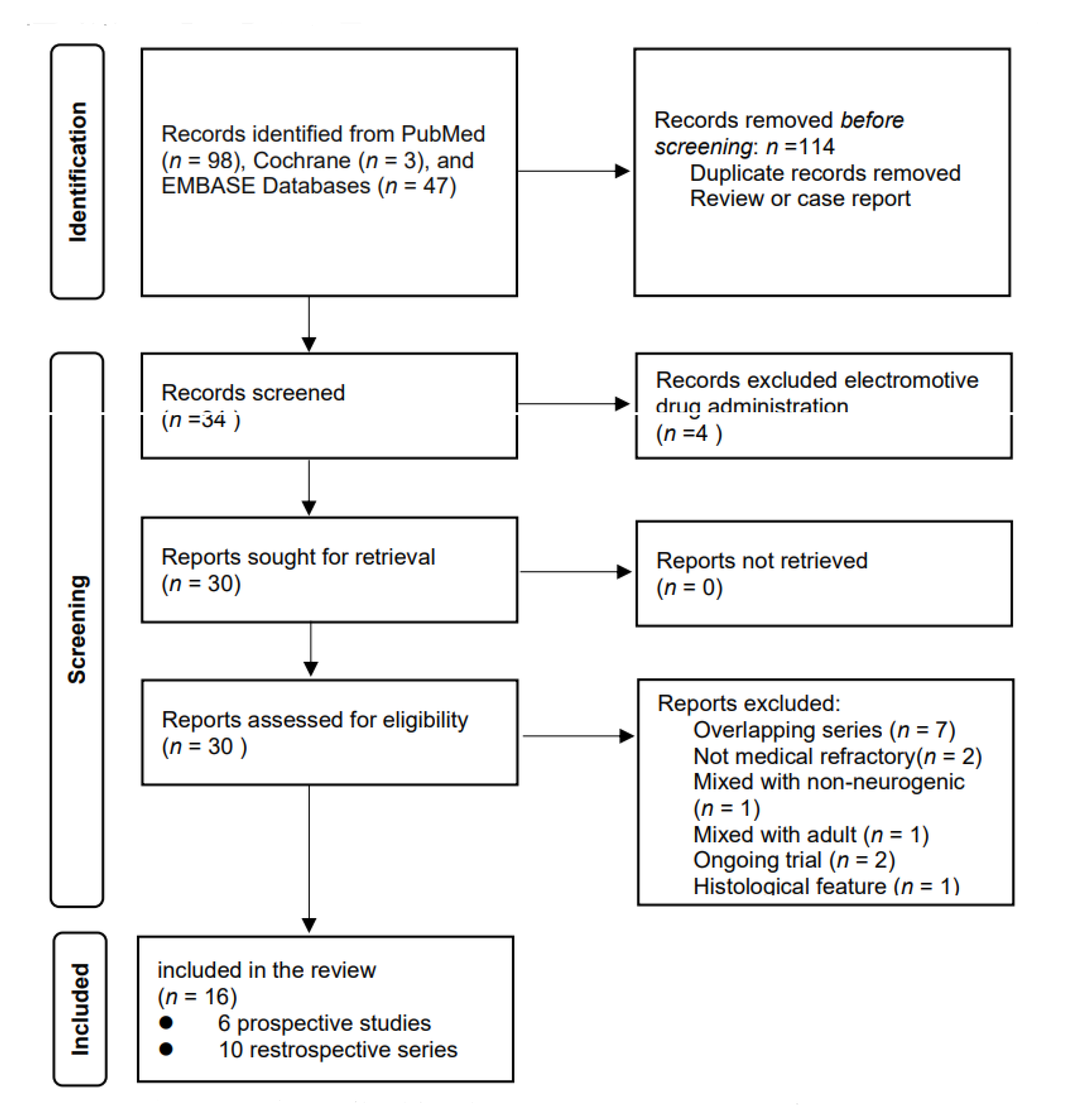
2. Materials and Methods
3. Results
3.1. Clinical Parameters
3.2. Urodynamic Parameters
3.3. Safety and Side Effects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Dik, P.; Klijn, A.J.; van Gool, J.D.; de Jong-de Vos van Steenwijk, C.C.E.; de Jong, T.P.V.M. Early start to therapy preserves kidney function in spina bifida patients. Eur. Urol. 2006, 49, 908–913. [Google Scholar] [CrossRef]
- Kasabian, N.G.; Bauer, S.B.; Dyro, F.M.; Colodny, A.H.; Mandell, J.; Retik, A.B. The prophylactic value of clean intermittent catheterization and anticholinergic medication in newborns and infants with myelodysplasia at risk of developing urinary tract deterioration. Am. J. Dis. Child. 1992, 146, 840–843. [Google Scholar] [CrossRef]
- Nitti, V.W. Botulinum toxin for the treatment of idiopathic and neurogenic overactive bladder: State of the art. Rev. Urol. 2006, 8, 198–208. [Google Scholar]
- Lee, B.; Featherstone, N.; Nagappan, P.; McCarthy, L.; O’Toole, S. British Association of Paediatric Urologists consensus statement on the management of the neuropathic bladder. J. Pediatr. Urol. 2016, 12, 76–87. [Google Scholar] [CrossRef]
- Figueroa, V.; Romao, R.; Salle, J.L.P.; Koyle, M.A.; Braga, L.H.P.; Bägli, D.J.; Lorenzo, A.J. Single-center experience with botulinum toxin endoscopic detrusor injection for the treatment of congenital neuropathic bladder in children: Effect of dose adjustment, multiple injections, and avoidance of reconstructive procedures. J. Pediatr. Urol. 2014, 10, 368–373. [Google Scholar] [CrossRef]
- Riccabona, M.; Koen, M.; Schindler, M.; Goedele, B.; Pycha, A.; Lusuardi, L.; Bauer, S.B. Botulinum-A toxin injection into the detrusor: A safe alternative in the treatment of children with myelomeningocele with detrusor hyperreflexia. J. Urol. 2004, 171, 845–848. [Google Scholar] [CrossRef]
- Akbar, M.; Abel, R.; Seyler, T.M.; Bedke, J.; Haferkamp, A.; Gerner, H.J.; Möhring, K. Repeated botulinum-A toxin injections in the treatment of myelodysplastic children and patients with spinal cord injuries with neurogenic bladder dysfunction. BJU Int. 2007, 100, 639–645. [Google Scholar] [CrossRef]
- Schulte-Baukloh, H.; Michael, T.; Schobert, J.; Stolze, T.; Knispel, H.H. Efficacy of botulinum-A toxin in children with detrusor hyperreflexia due to myelomeningocele: Preliminary results. Urology 2002, 59, 325–327. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Kajbafzadeh, A.M.; Moosavi, S.; Tajik, P.; Arshadi, H.; Payabvash, S.; Salmasi, A.H.; Akbari, H.R.; Nejat, F. Intravesical injection of botulinum toxin type A: Management of neuropathic bladder and bowel dysfunction in children with myelomeningocele. Urology 2006, 68, 1091–1096. [Google Scholar] [CrossRef]
- Altaweel, W.; Jednack, R.; Bilodeau, C.; Corcos, J. Repeated intradetrusor botulinum toxin type A in children with neurogenic bladder due to myelomeningocele. J. Urol. 2006, 175, 1102–1105. [Google Scholar] [CrossRef]
- Safari, S.; Jamali, S.; Habibollahi, P.; Arshadi, H.; Nejat, F.; Kajbafzadeh, A.M. Intravesical injections of botulinum toxin type A for management of neuropathic bladder: A comparison of two methods. Urology 2010, 76, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.V.; Sampang, R.; Smith, G.H.H. Study of botulinum toxin A in neurogenic bladder due to spina bifida in children. ANZ J. Surg. 2010, 80, 250–253. [Google Scholar] [CrossRef] [PubMed]
- Nué, R.L.; Harper, L.; Sèze, M.D.; Bouteiller, C.; Goossens, D.; Dobremez, E. Evolution of the management of acquired neurogenic bladder in children using intradetrusor botulinum toxin type A injections: 5-year experience and perspectives. J. Pediatr. Urol. 2012, 8, 497–503. [Google Scholar] [CrossRef]
- Horst, M.; Weber, D.M.; Bodmer, C.; Gobet, R. Repeated Botulinum-A toxin injection in the treatment of neuropathic bladder dysfunction and poor bladder compliance in children with myelomeningocele. Neurourol. Urodyn. 2011, 30, 1546–1549. [Google Scholar] [CrossRef] [PubMed]
- Kroll, P.; Jankowski, A.; Soltysiak, J.; Murias, M.; Skrzypczak, M.; Zachwieja, J. Botulinum toxin-A injections in children with neurogenic bladder. Nephro Urol Mon. 2011, 3, 125–128. [Google Scholar]
- Marte, A. Onabotulinumtoxin A for Treating Overactive/Poor Compliant Bladders in Children and Adolescents with Neurogenic Bladder Secondary to Myelomeningocele. Toxins 2013, 5, 16–24. [Google Scholar] [CrossRef]
- Kim, S.W.; Choi, J.H.; Lee, Y.S.; Han, S.W.; Im, Y.J. Preoperative urodynamic factors predicting outcome of botulinum toxin-A intradetrusor injection in children with neurogenic detrusor overactivity. Urology 2014, 84, 1480–1484. [Google Scholar] [CrossRef]
- Khan, M.K.; Brink, B.A.V.; DeFoor, W.R.; Minevich, E.; Jackson, E.; Noh, P.; Reddy, P.P. Botulinum toxin injection in the pediatric population with medically refractory neuropathic bladder. J. Pediatr. Urol. 2016, 12, 104.e1–104.e6. [Google Scholar] [CrossRef]
- Sekerci, C.A.; Tanidir, Y.; Garayev, A.; Akbal, C.; Tarcan, T.; Simsek, F. Clinical and Urodynamic Results of Repeated IntradetrusorOnabotulinum Toxin A Injections in Refractory Neurogenic Detrusor Overactivity: Up to 5 Injections in a Cohort of Children With Myelodysplasia. Urology 2018, 111, 168–175. [Google Scholar] [CrossRef]
- Hascoet, J.; Peyronnet, B.; Forin, V.; Baron, M.; Capon, G.; Prudhomme, T.; Allenet, C.; Tournier, S.; Maurin, C.; Cornu, J.N.; et al. Intra-Detrusor Injections of Botulinum Toxin Type a in Children with Spina Bifida: A Multicenter Study. Urology 2018, 116, 161–167. [Google Scholar] [CrossRef] [PubMed]
- Naqvi, S.; Clothier, J.; Wright, A.; Garriboli, M. Urodynamic Outcomes in Children after Single and Multiple Injections for Overactive and Low Compliance Neurogenic Bladder Treated with Abobotulinum Toxin A. J. Urol. 2020, 203, 413–419. [Google Scholar] [CrossRef]
- Neel, K.F.; Soliman, S.; Salem, M.; Seida, M.; Al-Hazmi, H.; Khatab, A. Botulinum-A toxin: Solo treatment for neuropathic noncompliant bladder. J. Urol. 2007, 178, 2593–2597. [Google Scholar] [CrossRef]
- Veenboer, P.W.; Bosch, J.L.H.R.; van Asbeck, F.W.A.; de Kort, L.M.O. Upper and lowerurinary tract outcomes in adult myelomeningocele patients: A systematic review. PLoS ONE 2012, 7, e48399. [Google Scholar] [CrossRef] [Green Version]
- Schurch, B.; Stöhrer, M.; Kramer, G.; Schmid, D.M.; Gaul, G.; Hauri, D. Botulinum-Atoxin for treating detrusor hyperreflexia in spinal cord injured patients: A new alternative to anticholinergic drugs? Preliminary results. J. Urol. 2000, 164, 692–697. [Google Scholar] [CrossRef]
- Alloussi, S.; Mürtz, G.; Braun, R.; Gerhardt, U.; Heinrich, M.; Hellmis, E.; Horn, W.; Marschall-Kehrel, D.; Niklas, K.; Raabe, M. Efficacy, tolerability and safety of propiverine hydrochloride in comparison to oxybutynin in children with urge incontinence due to overactive bladder: Results of a multicentre observational cohort study. BJU Int. 2010, 106, 550–556. [Google Scholar] [CrossRef]
- Uçar, M.; Akgül, A.K.; Parlak, A.; Yücel, C.; Kılıç, N.; Balkan, E. Non-invasive evaluation of botulinum-A toxin treatment efficacy in children with refractory overactive bladder. Int. Urol. Nephrol. 2018, 50, 1367–1373. [Google Scholar] [CrossRef]
- Frevert, J. Pharmaceutical, biological, and clinical propertiesof botulinum neurotoxin type A products. Drugs R D 2015, 15, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Scheepe, J.R.; Blok, B.F.M.; Hoen, L.A. Applicability of botulinum toxin type A in paediatric neurogenic bladder management. Curr. Opin. Urol. 2017, 27, 14–19. [Google Scholar] [CrossRef]
- Mangera, A.; Apostolidis, A.; Andersson, K.E.; Dasgupta, P.; Giannantoni, A.; Roehrborn, C.; Novara, G.; Chapple, C. An updated systematic review and statistical comparison of standardised mean outcomes for the use of botulinum toxin in the management of lower urinary tract disorders. Eur. Urol. 2014, 65, 981–990. [Google Scholar] [CrossRef]
- Schulte-Baukloh, H.; Herholz, J.; Bigalke, H.; Miller, K.; Knispel, H.H. Results of a BoNT/A antibody study in children and adolescents after onabotulinumtoxin A (Botox®) detrusor injection. Urol. Int. 2011, 87, 434–438. [Google Scholar] [CrossRef] [PubMed]
- Haferkamp, A.; Schurch, B.; Reitz, A.; Krengel, U.; Grosse, J.; Kramer, G.; Schumacher, S.; Bastian, P.J.; Büttner, R.; Müller, S.C. Lack of ultrastructural detrusor changes following endoscopic injection of botulinum toxin type a in overactive neurogenic bladder. Eur. Urol. 2004, 46, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Giannantoni, A.; Di Stasi, S.M.; Chancellor, M.B.; Costantini, E.; Porena, M. New frontiers in intravesical ltherapies and drug delivery. Eur. Urol. 2006, 50, 1183–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajbafzadeh, A.M.; Montaser-Kouhsari, L.; Ahmadi, H.; Sotoudeh, M. Intravesical electromotive botulinum toxin type A administration: Part I—experimental study. Urology 2011, 77, 1460–1464. [Google Scholar] [CrossRef] [PubMed]
- Kajbafzadeh, A.M.; Ahmadi, H.; Montaser-Kouhsari, L.; Sharifi-Rad, L.; Nejat, F.; Bazargan-Hejazi, S. Intravesical electromotive botulinum toxin type A administration—Part II: Clinical application. Urology 2011, 77, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Koh, C.; Melling, C.V.; Jennings, C.; Lewis, M.; Goyal, A. Efficacy of electromotive drug administration in delivering botulinum toxin a in children with neuropathic detrusor overactivity-outcomes of a pilot study. J. Pediatr. Urol. 2019, 15, 552.e1–552.e8. [Google Scholar] [CrossRef] [PubMed]
- Chang, H.I.; Yeh, M.K. Clinical development of liposome-based drugs: Formulation, characterization, and therapeutic efficacy. Int. J. Nanomed. 2012, 7, 49–60. [Google Scholar]
- Rajaganapathy, B.R.; Chancellor, M.B.; Nirmal, J.; Dang, L.; Tyagi, P. Bladder uptake of liposomes after intravesical administration occurs by endocytosis. PLoS ONE 2015, 10, e0122766. [Google Scholar] [CrossRef] [Green Version]
- Chuang, Y.C.; Kaufmann, J.H.; Chancellor, D.D.; Chancellor, M.B.; Kuo, H.C. Bladder instillation of liposome encapsulated onabotulinumtoxin A improves overactive bladder symptoms: A prospective, multicenter, double-blind, randomized trial. J. Urol. 2014, 192, 1743–1749. [Google Scholar] [CrossRef]

{kind=link}
| First Author | Type of Study | Number of Patients (n, M/F) | Mean Age (Year) | Neurologic Diseases (n) | Previous Treatment Modalities | Treatment Modality | Treatment Duration | Follow Up Period | Clinical Parameters | Urodynamic Parameters | Adverse Event (n) | Primary and Special Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Heinrich Schulte-Baukloh [8] | Retrospective chart analysis | 10, 6/4 | 11.2 | MMC 8 Intraspinal astrocytoma 1 SCI 1 | anticholinergic medications and CIC | 12 IU/kg, diluted in 15 to 20 mL normal saline, injected into 30 to 50 sites | repeated injection (at least three injections; 4 had received five or more injections) | 1, 3, and 6 months | NR | Reflex volume, Pdetmax, maximun bladder capacity, bladder compliance | NR | After the first versus the fifth injection reflex volume increased by 81% versus 88%, maximal detrusor pressure decreased by 7% versus 39% maximal cystometric bladder capacity increased by 88% versus 72% |
| Abdol-Mohammad Kajbafzadeh [10] | Single-center, prospective, unrandomized study | 26, 20/6 | 6.9 | MMC | anticholinergic medications and CIC | 10 IU/kg, diluted in 20 mL of normal saline, injected intravesically into at least 40 sites | single injection | 4 months | Incontinence, VUR, urinary tract infection, fecal continence | Pdetmax, maximun bladder capacity | no major treatment related event | 73% complete dry, 88% total improvement in urine incontinence; significant improvements in mean maximal detrusor pressure and average maximal bladder capacity |
| W. Altaweel [11] | Prospective study | 20, 8/12 | 13 | MMC | anticholinergic medications and CIC | 5 IU/kg (maximum 300 IU) diluted 10 times in normal saline, injected to give 10 IU per site | repeated injection (reassess approximately 3 months after each treatment, repeat injection if incontinent) | 3 months after each treatment (total mean follow-up 17.2 months) | Incontinence, hydronephrosis | Pdetmax, bladder compliance | no treatment related event | 65% continent; significant improvements in mean bladder capacity, maximum detrusor pressure and compliance |
| Saeed Safari [12] | Prospective, single center, double-blind, randomized control trial | Group A (30, 13/17) Group B (30, 14/16) | Group A (6.58) Group B (6.71) | MMC | anticholinergic medications and CIC | Group A (10 U/kg, diluted in 20 mL of normal saline, injected into 40 points of bladder); Group B (8 U/kg, injected in the same way as in group A and the remaining (2 U/kg) was injected by 4 additional injections in external urethral sphincter) | single injection | 3 and 6 months | Incontinence episodes, Constipation, Vesicoureteral reflux grade | Detrusor-sphincter dyssinergia, maximum detrusor pressure, post-voiding residual volumn, bladder capacity | NR | BTX-A injections in both sphincter and detrusor seems to have extra benefits in voiding |
| Aniruddh V Deshpande [13] | Prospective, non-randomized study | 7, 6/1 | 16 | Spinal bifida | CIC and oxybutynin (dose range 5 mg b.d.–5 mg q.i.d.) | 10 IU/kg, (maximum 300 IU) diluted as 10 units per mL in saline, injected into the detrusor at approximately 20 to 30 sites | single injection | 1, 3–6 and 9 months | Incontinence, satisfaction score | Bladder capacity, bladder compliance | UTI 1 | significant improvements in bladder compliance and incontinence |
| R Le Nué [14] | Retrospective chart analysis | 8, 3/5 | 12.4 | SCI 6 Stroke 2 | maximal oral anticholinergic treatment, CIC | 12 IU/kg (maximal 300 IU), diluting to a concentration of 100 IU/10 mL before 2008 and then 100 IU/5 mL of 0.9% saline, injected into 10 to 30 sites | repeated injection (2–6 injections, repeat injections depended on the initial urodynamic status) | 6 months after each treatment (total mean follow-up 47 months) | continence score | Pdetmax, bladder compliance, maximun bladder capacity, safe capacity | NR | Improvements in the mentioned parameters |
| Maya Horst [15] | Retrospective chart analysis | 11, 1/10 | 6.7 | MMC | anticholinergic medications | 10 IU/kg (maximal 300 IU), diluting to a concentration of 100 IU/10 mL of 0.9% saline, each injection contained 0.3–0.5 mL | repeated injection (1–4 injections, reinjection was performed if the urodynamic follow up study showed compliance and pressure returned to baseline values) | 3 and 12 months after each injection | VUR | Changes in bladder compliance, maximal bladder capacity, maximal detrusor pressure | NR | detrusor pressure decreased by 17% and bladder capacity increased by 33%; similar effect on capacity and detrusor pressure could be achieved with repeated injection |
| Pawel Kroll [16] | prospective, non-placebo-controlled study | 65, 34/31 | 6.7 | MMC 61 Sacral agenesis 3 Cerebral palsy 1 | CIC and oral oxybutynine | 50 IU/kg (maximal 500 IU), diluted in 10 mL normal saline, injected each with 0.5 mL of the solution | single injection | 6 and 12 months | continence | Maximun catheterized volume, maximun volume of leak point pressure | NR | Improvements in the mentioned parameters |
| Antonio Marte [17] | Retrospective chart analysis | 47, 25/22 | 10.7 | MMC | anticholinergic medications and CIC | 200 IU, diluted in 20 mL of 0.9% saline solution, not exceeding the dosage of 12 IU/kg, injected for a total of 20 injections | repeated injection (1–3 injections, for the recurrence of symptoms) | 6, 12 and 24 weeks after each injection (total mean followup 5.7 years) | Incontinence, VUR | Mean leak point volume, mean leak point pressure, specific capacity at 20 cm H2O, bladder capacity | slight hematuria 38, UTI 2, gastric pain 2, facial flushing 2, mild hyposthenia of the lower limbs 5 | significant 66.45% average increase of leak point volume, significant 118.57% average increase of specific bladder capacity at 20 cm H2O |
| V. Figueroa [5] | Prospective study | 17 | 10.7 | spina bifida/spinal dysraphism | anticholinergic medications | 10 IU/kg (maximal 200 IU), diluted in normal saline to a concentration of 10 units/cc | repeated injection (average of 2.5 injections/patient; range, 1–6) | 3, 6 months after each injection (total mean follow-up 4 years) | Incontinence | Mean bladder capacity, detrusor compliance, bladder volume, bladder compliance | NR | The optimal response occurs with a maximum administration of BTX-A up to 300 units. |
| Sang Woon Kim [18] | Retrospective chart analysis | 37, 22/15 | 7.49 | Spina bifida 29 Syrinx 1 Cerebral palsy 4 Guillain-Barre syndrome 1 Spinal cord hemangioma 1 Post meningitis sequelae 1 | high-dose anticholinergic medications | 10 IU/kg (maximal 200 IU), diluting to a concentration of 100 IU/5 mL of 0.9% saline, injected into 20 to 40 sites | single injection | 1, 3, 6 months | Patient Global Impression of Improvement (PGI-I) | detrusor-sphincter dyssynergia, maximum cystometric capacity, estimated bladder capacity, Residual urine volume, maximal detrusor pressure, reflex detrusor volume, bladder compliance, open bladder neck | UTI 1 | preoperative bladder compliance and open bladder neck were important predictors |
| M. K. Khan [19] | Retrospective chart analysis | 22, 16/6 | 10 | Myelomeningocele 10 Anorectal malformation 3 Spinal cord trauma 3 Tethered cord syndrome 2 Caudal regression syndrome 2 Sacrococcygeal teratoma 1 Transverse myelitis 1 | anticholinergic medications | 10 IU/kg (maximal 300 IU), diluted in normal saline to a concentration of 10 units/cc | repeated injection (Four patients have received two or more injections for the recurrence of symptoms) | 3, 6 months after each injection (total mean follow-up 11 months, range 3–38) | Incontinence, hydronephrosis | Cystometric bladder capacity, mean maximum detrusor pressure | NR | patients with anticholinergics intolerance seen to have be more effective after BTX-A injection than those with anticholinergic refractory |
| Cagri Akin Sekerci [20] | Retrospective chart analysis | 19, 4/15 | 10.3 | myelodysplasia | anticholinergic medications | 10 IU/kg (maximal 200 IU), diluted in normal saline to a concentration of 10 units/cc, injected to give 10 IU per site | repeated injection (1–5 injections, repeated only after the relapse of incontinence accompanying deterioration in urodynamic findings) | every 3 months after each injection | Incontinence, VUR, hydronephrosis | Maximum cystometric capacity, Maximum detrusor pressure, Compliance | hematuria 2 | significant improvements in the mentinal parameters after repeat injection |
| Juliette Hascoet [21] | Retrospective chart analysis | 53, 28/25 | 8.5 | Spina bifida | anticholinergic medications | 100–500 U | repeated injection (1–8 injections) | mean follow up of 3.7 years | Incontinence | Resolution of detrusor overactivity, normal bladder compliance, maximum cystometric capacity, maximum detrusor pressure | 3 UTI episodes out of 141 injections (2.1%) | 66% clinical success rate, 34% urodynamic success rate |
| Shehryer Naqvi [22] | Retrospective chart analysis | 30, 15/15 | 7.4 | MMC 18, Lipomeningocoele 4, Transverse myelitis 1, Sacral agenesis 3 | anticholinergic medications and CIC | 40 IU/kg, (maximal 1200 IU) diluted in 20 mL sodium chloride solution | repeated injection (Median number of injections was 3 (range 2 to 5) | median 2 months (range 0–29) | incontinence, VUR | Bladder compliance, cystometric capacity, maximum neurogenic detrusor overactivity | abdominal pain 1, UTI 1 | significantly improved cystometric capacity and maximum neurogenic detrusor overactivity, no significant difference in urodynamic parameters between first and last injections |
| Khalid Fouda Neel [23] | Prospective, single center, randomized trial | Group 1: 12 9/3 Group 2: 11 6/7 | Group 1: 6.1, Group 2: 5.1 | MMC | oxybutynin and CIC | 12 IU/kg (maximal 300 IU) Group 1: continued to receive anticholinergics; Group 2: dicontinued to receive anticholinergics | single injection | 12 months | incontinence | Maximum cystometric capacity, maximum detrusor pressure | NR | Oxybutynin did not have augmentative effect after BTX-A injection |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, S.-Y.; Chang, S.-J.; Yang, S.S.-D.; Hsu, C.-K. Botulinum Toxin Injection for Medically Refractory Neurogenic Bladder in Children: A Systematic Review. Toxins 2021, 13, 447. https://doi.org/10.3390/toxins13070447
Wu S-Y, Chang S-J, Yang SS-D, Hsu C-K. Botulinum Toxin Injection for Medically Refractory Neurogenic Bladder in Children: A Systematic Review. Toxins. 2021; 13(7):447. https://doi.org/10.3390/toxins13070447
Chicago/Turabian StyleWu, Shu-Yu, Shang-Jen Chang, Stephen Shei-Dei Yang, and Chun-Kai Hsu. 2021. "Botulinum Toxin Injection for Medically Refractory Neurogenic Bladder in Children: A Systematic Review" Toxins 13, no. 7: 447. https://doi.org/10.3390/toxins13070447
APA StyleWu, S. -Y., Chang, S. -J., Yang, S. S. -D., & Hsu, C. -K. (2021). Botulinum Toxin Injection for Medically Refractory Neurogenic Bladder in Children: A Systematic Review. Toxins, 13(7), 447. https://doi.org/10.3390/toxins13070447