1. Introduction
Cervical dystonia (CD) is the most common form of focal dystonia characterized by sustained, involuntary or intermittent muscle contractions and/or twitching resulting in abnormal postures and/or positioning of the head and/or neck [
1]. Botulinum neurotoxin (BoNT) is recommended as the first line treatment for CD [
2,
3], with statistically significant improvement in clinical studies in 70–90% of patients [
4,
5]. In everyday practice many patients experience an improvement; nevertheless, it is suboptimal in a majority of them [
6,
7]. This may be caused by several factors including inaccurate diagnosis, primary or secondary resistance to treatment and invalid drug storage. Nevertheless, it seems that appropriate pattern classification, a physician’s experience, BoNT-A dose and precision of injections are the most important factors contributing to successful treatment of CD [
8,
9].
Initially, CD was classified into four types, related to: turning the head (torticollis), tilting the head to one side (laterocollis), backwards (retrocollis), or forwards (anterocollis) [
10]. The Col-Cap concept, introduced by Reichel et al. [
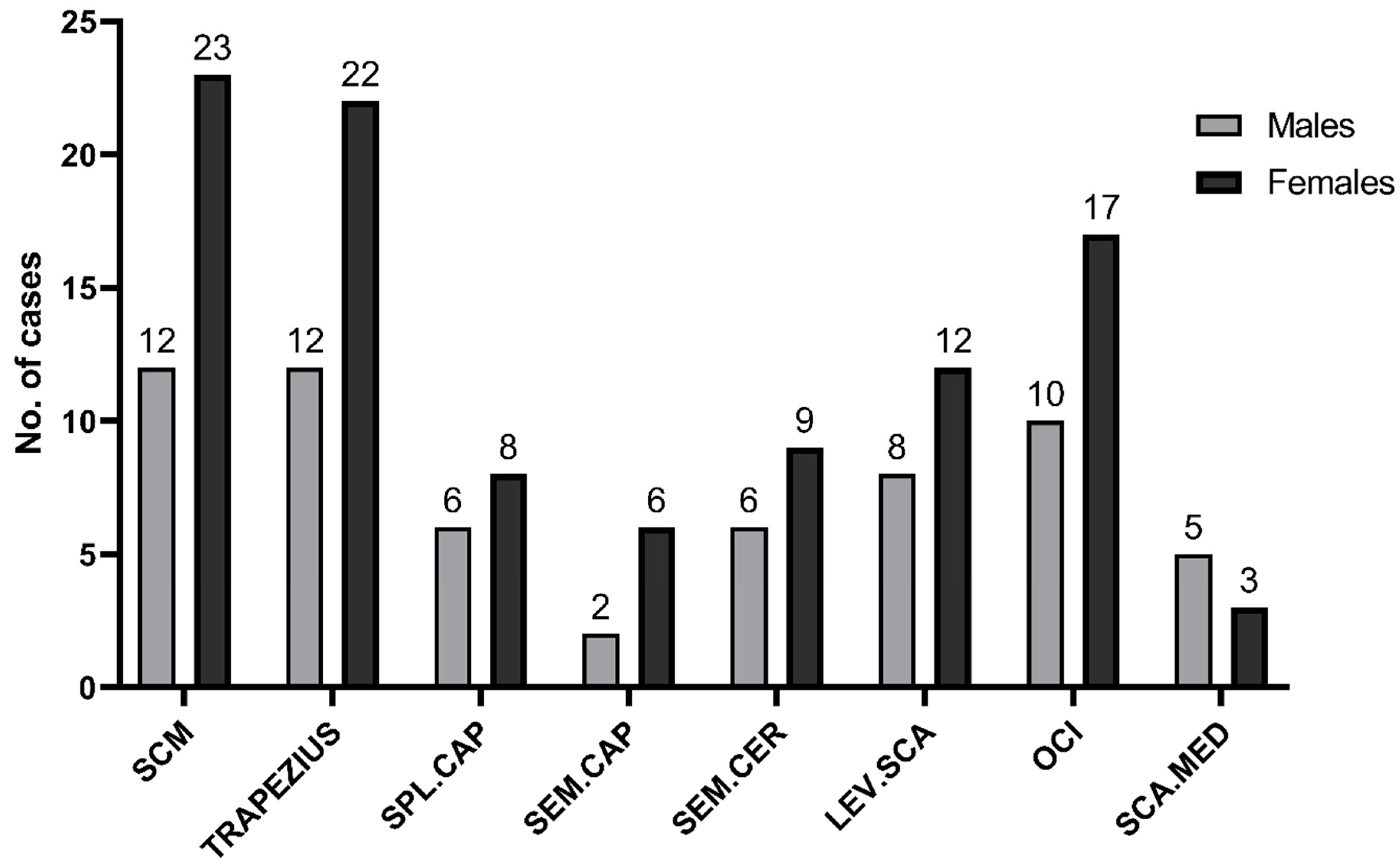
11] in consonance with anatomic and imaging studies, identified 10 main types of CD. According to this concept, deeply located muscles like obliquus capitis inferior (OCI), semispinalis cervicis or longus colli are involved. Jost et al. [
12] confirmed that during the last several decades some new muscles, which were previously never, or hardly ever, considered, have been added. Based on this study the most common injected muscles besides splenius capitis, sternocleidomastoid (scm) and trapezius were the levator scapulae, semispinalis capitis and OCI. It seems to be that deep lying muscles are difficult to be located and precisely injected without any visualization. Muscles can be injected using anatomical landmarks, under electromyography (EMG), computed tomography (CT) or ultrasound (US) guidance, but it remains controversial whether EMG and/or US are helpful in clinical practice. There are studies that support the role of EMG indicating that injections performed using only anatomic landmarks are unreliable (83% reached sternocleidomastoid, but only 47% the levator scapulae muscle) [
13]. The other study evaluating the accuracy of anatomy-guided injections also showed that even targeting first-layer muscles can be difficult (splenius capitis 67.9%, scm 86.7%, trapezius 75%, levator scapulae 78.3% of accuracy) [
14].
Ultrasound-guided injection provides real-time visualization of muscles and adjacent anatomical structures, which eventually may result in more precise injections and potentially a lower number of side effects [
15]. Nevertheless, thus far there is a lack of research elucidating the real effectiveness of US-guided treatment.
Most of the studies have been performed in small groups of patients or were focused on injections into deep cervical muscles only [
16,
17,
18,
19,
20,
21]. There is only one recently published study directly comparing the results of US-guided and non-guided BoNT-A injections in two groups of patients [
22]. Nevertheless, there are no randomized, controlled studies proving the higher effectiveness of US-guided versus blinded injections. In order to address this hypothesis, the aim of our study was to evaluate the efficacy of US-guided BoNT-A injections in comparison with using anatomic landmarks.
3. Discussion
The novel approach to BoNT-A treatment of CD include the identification of dystonia pattern according to the Col-Cap concept [
23]. According to this concept, in many forms of CD deeply located muscles, which are difficult to identify without imaging, like OCI or semispinalis cervicis, are involved. On the other hand, superficial muscles (like trapezius, scm, splenius capitis) also may be easily missed without any visualization [
13,
14]. In studies comparing the blinded (AL) and EMG guided/verified [
13] or US verified injections [
14], even in the hands of an experienced physician there was a substantial rate of missed muscles.
Ultrasonography is a convenient, non-invasive method that enables the visualization of muscles and surrounding structures, including nerve bundles and large vessels, in real time. It is hypothesized that using US increases the accuracy of injections of both superficial and deep cervical muscles. Available data on using US in the treatment of CD is scarce. Bhidayasiri et al. [
16] presented a case series of three patients about whom they conclude the lack of deeply located muscles imaging led to BoNT-A treatment failure. There is only one study comparing directly US-guided and non-guided injections in two different groups of patients which found no difference [
22]. An expert-statement published in 2015 [
24] suggested that US-guided injections should be used especially in cases with specific anatomic conditions, such as pronounced or inaccessible neck muscles, obesity or muscle atrophy, during adverse events following BoNT-A treatment, complex dystonic patterns with involvement of deep cervical muscles, or in secondary non-responders. Nevertheless, evidence is still lacking for proving the real effectiveness of US-guided vs. AL injections in CD treatment. In our study, the response to treatment measured by clinical scales was significant in both US-guided and AL injections, but a greater decrease in scales was associated with US use. The consistency of the results obtained by unblinded and blinded raters proved this hypothesis. Despite the effectiveness of both, the comparison of the two approaches (AL vs. US) showed the superiority of US-guided injections (
Table 3). All injections and US assessments were performed by one and the same experienced (15 years) and certified neurologist, which is why it cannot be excluded that the results in group AL were influenced by the principal investigator’s knowledge of anatomy and experience in the use of ultrasound.
Hong et al. [
15] revealed that use of US during injections decreases the incidence of dysphagia (0% vs. 34.7%), but no exact conclusions have been made due to the small number of participants (
n = 5). Similarly, in our study, swallowing problems were less frequent in the US-guided group, but the difference did not reach significance. In our opinion, a low number of patients may have been relevant. On the other hand, a retrospective study on a group of 75 CD patients revealed that US guidance is not able to prevent dysphagia [
25].
In summary, US can be helpful in improving the results of BoNT-A injections in CD.
There are, however, several limitations of our study. First of all, we have not employed a randomized trial protocol, nor a case-control study. The study was only partially blinded. The assessments based on TWSTRS and Tsui scores were not blind, with the only blind assessment being the CGI assessment. To study the exact effect of US use on a patient’s clinical improvement, we decided to subtract the results of measurements over time (value
after − value
before) and create a Δvalue which showed a greater decrease in scales, but more studies are needed to evaluate whether it has clinically relevant effect. On the other hand, we compared the results of AL and US in the same patients, which seems to be a more reliable method, taking into account the high variability of CD patterns. Our approach does not provide information about the possible influence of other variables (e.g., sex, age, disease duration, BoNT-A preparation and doses) on treatment efficacy. However, comparing the results in one patient allowed us to exclude the influence of many factors (e.g., dose or dystonia pattern, co-morbidities like depression or anxiety) which could influence the overall effect [
5,
26,
27].
To the best of our knowledge, this is one of the most complex studies performed to date, showing that US-guided injections might be helpful in improving the results of BoNT-A injections in cervical dystonia. We definitely need more larger and controlled studies to prove the concept.
5. Materials and Methods
5.1. Study Design and Patients
Thirty-five consecutive patients (12 males, 23 females, mean age 52.49 ± 10.05) with clinical diagnosis of idiopathic CD were recruited from the outpatient clinic from the group who participate in the routine therapeutic program for cervical dystonia. They were the patients who fulfilled the following inclusion criteria: ≥18 years of age, previous effective treatment with BoNT-A, the recurrence of symptoms and at least 12 weeks interval after the last injection. The study was prospective and each patient underwent two sessions: the first one in which injections were administered according to anatomic landmarks (AL group) and, after no less than 12 weeks, the second one was performed under US guidance (US group). The second session was only performed on condition that the patient had returned to the clinical condition from before the first session (the same number of points in the scales). Patients were evaluated by the same physician (the so-called Study Physician) with 15 years of experience who performed a clinical examination and classified dystonic posture on the basis of the Col-Cap concept [
23,
28].
The choice of muscles, type of BoNT-A, total dose and each muscle dose remained the same as before and during both sessions. Each session was digitally video recorded according to the same protocol.
In US-guided injection, we used a Hitachi Arietta 50 device with a linear probe (6–13 MHz) and out-of-plane approach.
The landmarks used for injections and muscle injection sites with US use are presented in the
Supplementary Materials.
All patients signed informed consent before enrollment into the study. The study was approved by the local bioethics committee (Nr of consent K.B.-2/17).
5.2. Assessments
All patients were evaluated before each session and 4 weeks after the injection. The efficacy assessments included Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS, including total scores, severity, disability and pain subscale scores); Tsui-modified score; Craniocervical Dystonia Questionnaire (CDQ-24); and Clinical Global Impression–Improvement (CGI-I) score (calculated on a scale from 1-very much improved to 7-very much worse). CGI-I was assessed by patients, injector and two independent blinded raters to whom standardized video recordings were sent. The patients were filmed in frontal position (with open and closed eyes, and with shoulder stabilization), from the side, and while walking. Both raters were experienced neurologists with at least five years of experience in BoNT-A treatment of CD. Safety assessments included incidence of adverse events: dysphagia, muscle pain and head drop as obligatory questions and others spontaneously reported by patients.
5.3. Statistical Analysis
Statistical analysis was performed using GraphPad Prism 9 and Statistica 13 software. Continuous variables were presented using mean and standard deviation, while numerical and non-continuous variables as number of cases (n) and percentage, median and interquartile range. Distribution of the variables was assessed using the Shapiro–Wilk test. To compare differences between groups, the Student’s t-test in Welch’s modification or the Mann–Whitney U test were used. The correlation was performed using the Spearman correlation coefficient. A correlation coefficient ranging from 0.00 to 0.19 was considered as very weak, 0.20 to 0.39 as weak, 0.40 to 0.59 as moderate, 0.60 to 0.79 as strong and 0.80 to 1.0 as very strong. A p value below 0.05 was deemed significant.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}