Khat, a Cultural Chewing Drug: A Toxicokinetic and Toxicodynamic Summary

 ,
,  ,
,  and
and
Abstract
:1. Introduction
2. Results and Discussion
2.1. Khat Phytochemistry
2.2. Khat Legality
2.3. Khat Toxicokinetics
2.4. Khat Toxicodynamic
2.5. Addiction
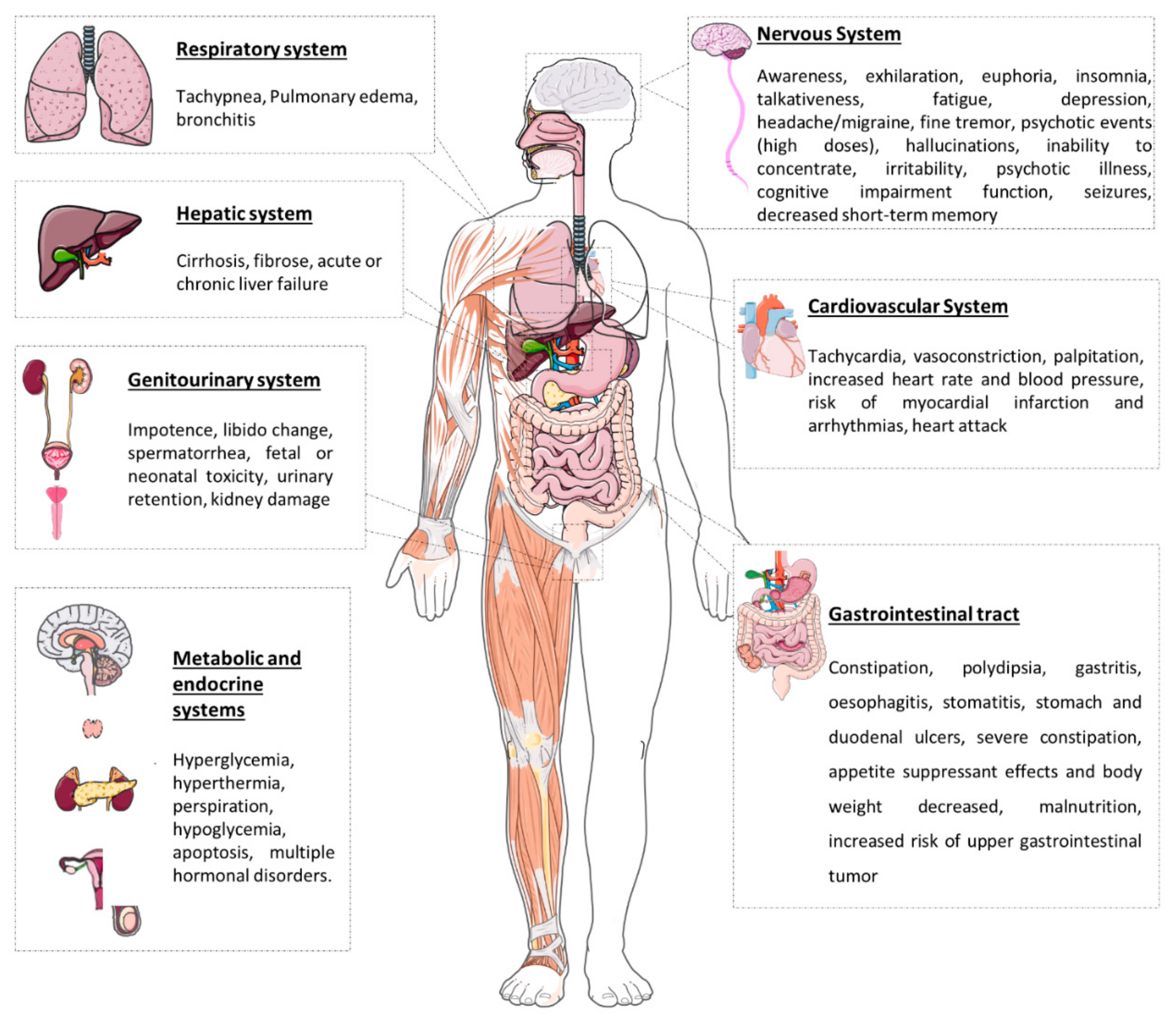
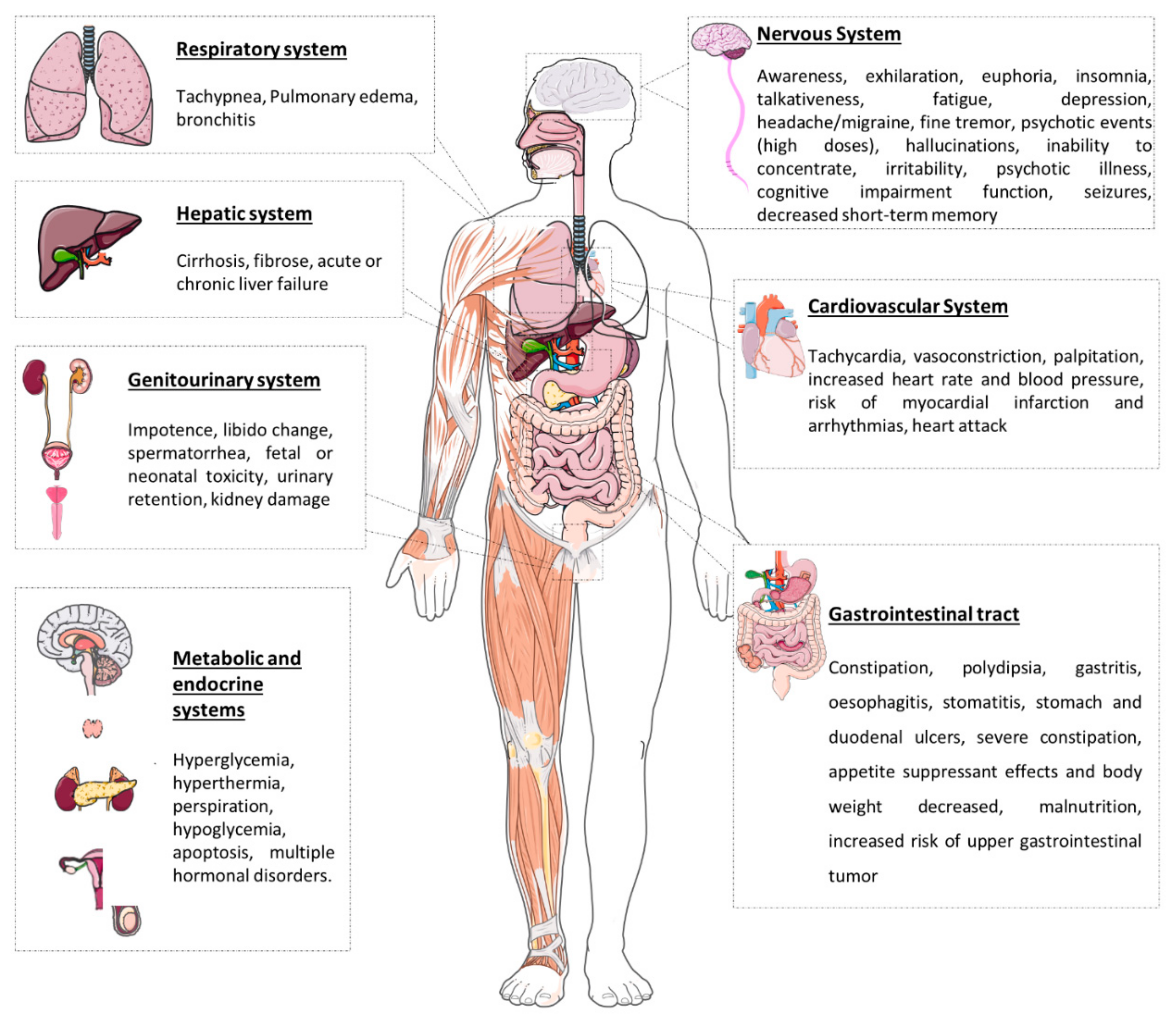
2.6. Effects after Chewing Khat Leaves
2.6.1. In Vitro Studies
2.6.2. Human Studies
2.7. Khat Interactions
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abebe, W. Khat: A Substance of Growing Abuse with Adverse Drug Interaction Risks. J. Natl. Med Assoc. 2018, 110, 624–634. [Google Scholar] [CrossRef] [PubMed]
- Balint, E.E.; Falkay, G.; Balint, G.A. Khat—A controversial plant. Wien Klin Wochenschr 2009, 121, 604–614. [Google Scholar] [CrossRef]
- Valente, M.J.; de Pinho, P.G.; Bastos, M.D.L.; Carvalho, F.; Carvalho, M. Khat and synthetic cathinones: A review. Arch. Toxicol. 2014, 88, 15–45. [Google Scholar] [CrossRef] [PubMed]
- Al-Hebshi, N.N.; Skaug, N. Khat (Catha edulis)—An updated review. Addict. Biol. 2005, 10, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Al-Motarreb, A.; Baker, K.; Broadley, K.J. Khat: Pharmacological and medical aspects and its social use in Yemen. Phytother. Res. 2002, 16, 403–413. [Google Scholar] [CrossRef]
- Al-Habori, M. The potential adverse effects of habitual use of Catha edulis(khat). Expert Opin. Drug Saf. 2005, 4, 1145–1154. [Google Scholar] [CrossRef] [PubMed]
- Cochrane, L.; O’Regan, D. Legal harvest and illegal trade: Trends, challenges, and options in khat production in Ethiopia. Int. J. Drug Policy 2016, 30, 27–34. [Google Scholar] [CrossRef]
- Szendrei, K. The chemistry of khat. Bull. Narc. 1980, 32, 5–35. [Google Scholar]
- Kalix, P. Cathinone, a natural amphetamine. Pharmacol. Toxicol. 1992, 70, 77–86. [Google Scholar] [CrossRef]
- Brenneisen, R.; Geisshüsler, S. Psychotropic drugs.III. Analytical and chemical aspects of Catha edulis Forsk. Pharm. Acta Helv. 1985, 60, 290–301. [Google Scholar]
- Kelly, J.P. Cathinone derivatives: A review of their chemistry, pharmacology and toxicology. Drug Test. Anal. 2011, 3, 439–453. [Google Scholar] [CrossRef] [PubMed]
- Kalix, P.; Braenden, O. Pharmacological aspects of the chewing of khat leaves. Pharmacol. Rev. 1985, 37, 149–164. [Google Scholar] [PubMed]
- Geisshüsler, S.; Brenneisen, R. The content of psychoactive phenylpropyl and phenylpentenyl khatamines in Catha edulis Forsk. of different origin. J. Ethnopharmacol. 1987, 19, 269–277. [Google Scholar] [CrossRef]
- Kalix, P. Pharmacological properties of the stimulant khat. Pharmacol. Ther. 1990, 48, 397–416. [Google Scholar] [CrossRef]
- Feyissa, A.M.; Kelly, J.P. A review of the neuropharmacological properties of khat. Prog. Neuropsychopharmacol. Biol. Psychiatry 2008, 32, 1147–1166. [Google Scholar] [CrossRef] [PubMed]
- Feng, L.-Y.; Battulga, A.; Han, E.; Chung, H.; Li, J.-H. New psychoactive substances of natural origin: A brief review. J. Food Drug Anal. 2017, 25, 461–471. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.B. Khat (Catha edulis Forsk)—And now there are three. Brain Res. Bull. 2019, 145, 92–96. [Google Scholar] [CrossRef]
- Sawair, F.A.; Al-Mutwakel, A.; Al-Eryani, K.; Al-Surhy, A.; Maruyama, S.; Cheng, J.; Al-Sharabi, A.; Saku, T. High relative frequency of oral squamous cell carcinoma in Yemen: Qat and tobacco chewing as its aetiological background. Int. J. Environ. Health Res. 2007, 17, 185–195. [Google Scholar] [CrossRef]
- Toennes, S.W.; Harder, S.; Schramm, M.; Niess, C.; Kauert, G.F. Pharmacokinetics of cathinone, cathine and norephedrine after the chewing of khat leaves. Br. J. Clin. Pharmacol. 2003, 56, 125–130. [Google Scholar] [CrossRef] [Green Version]
- Toennes, S.W.; Kauert, G.F. Excretion and detection of cathinone, cathine, and phenylpropanolamine in urine after kath chewing. Clin. Chem. 2002, 48, 1715–1719. [Google Scholar] [CrossRef] [Green Version]
- Widler, P.; Mathys, K.; Brenneisen, R.; Kalix, P.; Fisch, H.-U. Pharmacodynamics and pharmacokinetics of khat: A controlled study. Clin. Pharmacol. Ther. 1994, 55, 556–562. [Google Scholar] [CrossRef]
- Halket, J.M.; Karasu, Z.; Murray-Lyon, I.M. Plasma cathinone levels following chewing khat leaves (Catha edulis Forsk). J. Ethnopharmacol. 1995, 49, 111–113. [Google Scholar] [CrossRef]
- Brenneisen, R.; Fisch, H.U.; Koelbing, U.; Geisshusler, S.; Kalix, P. Amphetamine-like effects in humans of the khat alkaloid cathinone. Br. J. Clin. Pharmacol. 1990, 30, 825–828. [Google Scholar] [CrossRef] [Green Version]
- Brenneisen, R.; Geisshüsler, S.; Schorno, X. Metabolism of cathinone to (−)-norephedrine and (−)-norpseudoephedrine. J. Pharm. Pharmacol. 1986, 38, 298–300. [Google Scholar] [CrossRef] [PubMed]
- Mathys, K.; Brenneisen, R. Determination of (S)-(−)-cathinone and its metabolites (R,S)-(−)-norephedrine and (R,R)-(−)-norpseudoephedrine in urine by high-performance liquid chromatography with photodiode-array detection. J. Chromatogr. 1992, 593, 79–85. [Google Scholar] [CrossRef]
- Engidawork, E. Pharmacological and Toxicological Effects of Catha edulisF. (Khat). Phytotherapy Res. 2017, 31, 1019–1028. [Google Scholar] [CrossRef] [PubMed]
- Odenwald, M.; al’Absi, M. Khat use and related addiction, mental health and physical disorders: The need to address a growing risk. East Mediterr. Health J. 2017, 23, 236–244. [Google Scholar] [CrossRef]
- Cox, G.; Rampes, H. Adverse effects of khat: A review. Adv. Psychiatr. Treat. 2003, 9, 456–463. [Google Scholar] [CrossRef]
- Heal, D.J.; Smith, S.L.; Gosden, J.; Nutt, D.J. Amphetamine, Past and present—A pharmacological and clinical perspective. J. Psychopharmacol. 2013, 27, 479–496. [Google Scholar] [CrossRef] [Green Version]
- Mladěnka, P.; Applová, L.; Patočka, J.; Costa, V.M.; Remiao, F.; Pourová, J.; Mladěnka, A.; Karlíčková, J.; Jahodář, L.; Vopršalová, M.; et al. Comprehensive review of cardiovascular toxicity of drugs and related agents. Med Res Rev 2018, 38, 1332–1403. [Google Scholar] [CrossRef]
- Nencinp, P.; Amiconi, G.; Befani, O.; Abdullahi, M.; Anania, M. Possible involvement of amine oxidase inhibition in the sympathetic activation induced by khat (catha edulis) chewing in humans. J. Ethnopharmacol. 1984, 11, 79–86. [Google Scholar] [CrossRef]
- Osorio-Olivares, M.; Rezende, M.C.; Sepúlveda-Boza, S.; Cassels, B.K.; Fierro, A. MAO inhibition by arylisopropylamines: The effect of oxygen substituents at the beta-position. Bioorg. Med. Chem. 2004, 12, 4055–4066. [Google Scholar] [CrossRef]
- Basker, G. A review on hazards of khat chewing. Int. J. Pharm. Pharm. Sci. 2013, 5, 74–77. [Google Scholar]
- Nielen, R.J.; A Van Der Heijden, F.M.M.; Tuinier, S.; A Verhoeven, W.M. Khat and mushrooms associated with psychosis. World J. Biol. Psychiatry 2004, 5, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Patel, N.B. Mechanism of action of cathinone: The active ingredient of khat (Catha edulis). East Afr. Med J. 2009, 77, 329–332. [Google Scholar] [CrossRef] [Green Version]
- Al-Meshal, I.A.; Qureshi, S.; Ageel, A.M.; Tariq, M. The toxicity of Catha edulis (khat) in mice. J. Subst. Abus. 1991, 3, 107–115. [Google Scholar] [CrossRef]
- Ahmed, M.B.; el-Qirbi, A.B. Biochemical effects of Catha edulis, cathine and cathinone on adrenocortical functions. J. Ethnopharmacol. 1993, 39, 213–216. [Google Scholar] [CrossRef]
- Islam, M.W.; Al-Shabanah, O.A.; Al-Harbi, M.M.; Al-Gharably, N.A. Evaluation of teratogenic potential of khat (Catha edulis forsk.) In rats. Drug Chem. Toxicol. 1994, 17, 51–68. [Google Scholar] [CrossRef]
- Al-Motarreb, A.L.; Broadley, K.J. Coronary and aortic vasoconstriction by cathinone, the active constituent of khat. Auton. Autacoid Pharmacol. 2003, 23, 319–326. [Google Scholar] [CrossRef]
- Banjaw, M.Y.; Miczek, K.; Schmidt, W.J. Repeated Catha edulis oral administration enhances the baseline aggressive behavior in isolated rats. J. Neural. Transm. 2006, 113, 543–556. [Google Scholar] [CrossRef]
- Abdulwaheb, M.; Makonnen, E.; Debella, A.; Abebe, D. Effect of Catha edulis foresk (khat) extracts on male rat sexual behavior. J. Ethnopharmacol. 2007, 110, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Al-Ahdal, M.N.; McGarry, T.J.; Hannan, M.A. Cytotoxicity of Khat (Catha edulis) extract on cultured mammalian cells: Effects on macromolecule biosynthesis. Mutat. Res. 1988, 204, 317–322. [Google Scholar] [CrossRef]
- Nyongesa, A.W.; Patel, N.B.; Onyango, D.W.; Wango, E.O.; Odongo, H.O. In vitro study of the effects of khat (Catha edulis Forsk) extract on isolated mouse interstitial cells. J. Ethnopharmacol. 2007, 110, 401–405. [Google Scholar] [CrossRef]
- Dimba, E.A.; Gjertsen, B.T.; Bredholt, T.; Fossan, K.O.; Costea, D.E.; Francis, G.W.; Johannessen, A.C.; Vintermyr, O.K. Khat (Catha edulis)-induced apoptosis is inhibited by antagonists of caspase-1 and -8 in human leukaemia cells. Br. J. Cancer 2004, 91, 1726–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bredholt, T.; Dimba, E.A.; Hagland, H.R.; Wergeland, L.; Skavland, J.; O Fossan, K.; Tronstad, K.J.; Johannessen, A.C.; Vintermyr, O.K.; Gjertsen, B.T. Camptothecin and khat (Catha edulis Forsk.) induced distinct cell death phenotypes involving modulation of c-FLIPL, Mcl-1, procaspase-8 and mitochondrial function in acute myeloid leukemia cell lines. Mol. Cancer 2009, 8, 101. [Google Scholar] [CrossRef] [Green Version]
- Abou-Elhamd, A.S.; Kalamegam, G.; Ahmed, F.; Assidi, M.; Alrefaei, A.F.; Pushparaj, P.N.; Abu-Elmagd, M. Unraveling the Catha edulis Extract Effects on the Cellular and Molecular Signaling in SKOV3 Cells. Front. Pharmacol. 2021, 12, 666885. [Google Scholar] [CrossRef]
- Abebe, M.; Kindie, S.; Adane, K. Adverse Health Effects of Khat: A Review. Fam. Med. Med. Sci. Res. 2015, 4, 154. [Google Scholar]
- Tesfaye, F.; Byass, P.; Wall, S.; Berhane, Y.; Bonita, R. Association of Smoking and Khat (Catha edulis Forsk) Use With High Blood Pressure Among Adults in Addis Ababa, Ethiopia, 2006. Prev. Chronic Dis. 2008, 5, A89. [Google Scholar]
- Al-Motarreb, A.; Briancon, S.; Al-Jaber, N.; Al-Adhi, B.; Al-Jailani, F.; Salek, M.S.; Broadley, K. Khat chewing is a risk factor for acute myocardial infarction: A case-control study. Br. J. Clin. Pharmacol. 2005, 59, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Alkadi, H.; A Noman, M.; Al-Thobhani, A.K.; Al-Mekhlafi, F.S.; Raja’A, Y. Clinical and experimental evaluation of the effect of Khat-induced myocardial infarction. Saudi Med. J. 2002, 23, 1195–1198. [Google Scholar]
- Ahmed, A.M. Effect of Khat on the Heart and Blood Vessels. Heart Views 2004, 5, 54–57. [Google Scholar]
- Hill, C.M.; Gibson, A. The oral and dental effects of q’at chewing. Oral. Surg. Oral. Med. Oral. Pathol. 1987, 63, 433–436. [Google Scholar] [CrossRef]
- Goldenberg, D.; Lee, J.; Koch, W.M.; Kim, M.M.; Trink, B.; Sidransky, D.; Moon, C.-S. Habitual Risk Factors for Head and Neck Cancer. Otolaryngol. Neck Surg. 2004, 131, 986–993. [Google Scholar] [CrossRef]
- Heymann, T.D.; Bhupulan, A.; Zureikat, N.E.K.; Bomanji, J.; Drinkwater, C.; Giles, P.; Murray-Lyon, I.M. Khat chewing delays gastric emptying of a semi-solid meal. Aliment. Pharmacol. Ther. 2007, 9, 81–83. [Google Scholar] [CrossRef]
- Tucci, S.A. Phytochemicals in the Control of Human Appetite and Body Weight. Pharmaceuticals 2010, 3, 748–763. [Google Scholar] [CrossRef]
- Chapman, M.H.; Kajihara, M.; Borges, G.; O’Beirne, J.; Patch, D.; Dhillon, A.P.; Crozier, A.; Morgan, M.Y. Severe, Acute Liver Injury and Khat Leaves. N. Engl. J. Med. 2010, 362, 1642–1644. [Google Scholar] [CrossRef]
- Stuyt, R.J.L.; Willems, S.M.; Wagtmans, M.J.; Van Hoek, B. Chewing khat and chronic liver disease. Liver Int. 2011, 31, 434–436. [Google Scholar] [CrossRef] [PubMed]
- Mwenda, J.; M’Arimi, M.M.; Kyama, M.; Langat, D. Effects of khat (Catha edulis) consumption on reproductive functions: A review. East Afr. Med J. 2005, 80, 318–323. [Google Scholar] [CrossRef] [Green Version]
- Dhadphale, M.; Mengech, A.; Chege, S.W. Miraa (Catha edulis) as a cause of psychosis. East Afr. Med. J. 1981, 58, 130–135. [Google Scholar] [PubMed]
- Critchlow, S.; Seifert, R. Khat-induced Paranoid Psychosis. Br. J. Psychiatry 2018, 150, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Jager, A.D.; Sireling, L. Natural history of Khat psychosis. Aust. N. Z. J. Psychiatry 1994, 28, 331–332. [Google Scholar] [CrossRef]
- Alem, A.; Shibre, T. Khat induced psychosis and its medico-legal implication: A case report. Ethiop. Med. J. 1997, 35, 137–139. [Google Scholar] [PubMed]
- Abdulkarim, K. Cephradine Bioequivalence and Its Interaction with Khat and Food (Al-Sayadeyah) in Yemen. Ph.D. Thesis, University of Khartoum, Khartoum, Sudan, 2004. [Google Scholar]
- Attef, O.A.; Ali, A.A.; Ali, H.M. Effect of Khat chewing on the bioavailability of ampicillin and amoxycillin. J. Antimicrob. Chemother 1997, 39, 523–525. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bamashmus, M.; Othrob, N.Y.; Mousa, A.; Al-Tay, W. Effect of Khat (Qat) consumption on pain during and after local anesthesia for patients undergoing cataract surgery. Med Sci. Monit. 2010, 16, SR29–SR33. [Google Scholar]
- Bamgbade, O.A. The perioperative implications of khat use. Eur. J. Anaesthesiol. 2008, 25, 170–172. [Google Scholar] [CrossRef]
- Farah, F.; Attef, O.; Ali, A.-A. The Influence of Khat on the In-vitro and In-vivo availability of Tetracycline-HCl. Res. J. Pharm. Dos. Technol. 2015, 7, 1–6. [Google Scholar]
- Bedada, W.; de Andrés, F.; Engidawork, E.; Pohanka, A.; Beck, O.; Bertilsson, L.; Llerena, A.; Aklillu, E. The Psychostimulant Khat (Catha edulis) Inhibits CYP2D6 Enzyme Activity in Humans. J. Clin. Psychopharmacol. 2015, 35, 694–699. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subjects | Oral Cathinone Dose (per Kilogram of Body Weight) | Maximum Plasma Concentration | Terminal Elimination Half-Life | Ref. |
|---|---|---|---|---|
| Six male volunteers (25–35 years) | 0.8 mg (54–71 g of fresh khat leaves) | 127 ± 53 ng/mL after 2.1 ± 0.5 h | 4.3 ± 1.7 h | [21] |
| Five volunteers (two females and three males) (21–30 years) | 0.8–1 mg (60 g of fresh khat leaves) | 83 ± 42 ng/mL after 1.5–3.5 h | - | [22] |
| Four volunteers (two male and two female) (26–57 years) | 0.6 mg (26–59 g of fresh khat leaves) | 58.9 ± 18.8 ng/mL after 2.31 ± 0.65 h | 1.5 ± 0.8 h | [19] |
| Six male volunteers (28–36 years) | 0.5 mg | 1 h | - | [23] |
| In Vitro Model | Concentration ofKhat Extract | Results |
| KB cells [42] | 0–80 ng/mL | LD50 of 40 ng/mL DNA synthesis inhibition by 50% at 200 ng/mL |
| 1BR.3 and XP2Bi [42] | Biphasic survival (LD50 of 20 ng/mL for 25% of the cell population and 75 ng/mL for the more resistant subpopulation) DNA synthesis inhibition by 50% at 45 ng/mL in 1BR.3 cells, and 60 ng/mL in XP2Bi cells | |
| Mouse interstitial cells [43] | 0.06, 0.6, 6, 30 and 60 mg/mL | The highest concentrations (30 mg/mL and 60 mg/mL): significantly inhibited testosterone production and decreased the cell viability The lowest concentrations (0.06, 0.6, and 6 mg/mL): significantly stimulated testosterone production and had no effect on interstitial viability |
| HL-60, Jurkat, NB4 cell lines, and primary peripheral leukocytes [44] | Organic khat extract induced apoptotic cell death, regulated by the activation of cellular caspase −1, −3, and −8 | |
| MOLM-13, MOLM-14, NB4 and MV-4-11 cell lines [45] | 200 μg/mL | Organic khat extract activated a distinct cell death involving mitochondrial damage and morphological features of autophagy |
| SKOV3 [46] | 0.01, 0.03, 0.1, 0.3, 1, 3, and 10 mg/mL | Khat induces reduced cell size, cell membrane damage, and apoptosis The highest concentrations (1, 3, and 10 mg/mL) affected cell metabolic activity, cell cycle, and cellular proliferation |
| In silico [46] | Khat constituents (cathine, cathinone, and catheduline): bound to family A of G-protein-coupled receptors and altered several signalling pathways (CREB, Wnt, FGF, IL-6, and ERK/MAPK) |
| Drug Classes | Drug | Results |
|---|---|---|
| Anaesthetics | benoxinate (0.4%) [65] | Consumption of khat (12 h prior surgery): Reduces pain tolerance and comfort of patients during local anesthesia and surgery |
| sevoflurane (2%) plus nitrous oxide (65%) [66] | Consumption of khat (4 h prior surgery): Recovery from anesthesia was delayed | |
| Antibiotics | ampicillin (500 mg); amoxicillin (500 mg) [64] cephradine (500 mg) [63] tetracycline (500 mg) [67] | The astringent activity of tannins present in khat on GI surface can prevent/reduce absorption of oral drugs The bioavailability of both drugs was significantly reduced by khat Reductions in maximum plasma concentration, slower time for reaching peak concentration, and decrease in absorption rate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, B.; Soares, J.; Rocha-Pereira, C.; Mladěnka, P.; Remião, F.; on behalf of The OEMONOM Researchers. Khat, a Cultural Chewing Drug: A Toxicokinetic and Toxicodynamic Summary. Toxins 2022, 14, 71. https://doi.org/10.3390/toxins14020071
Silva B, Soares J, Rocha-Pereira C, Mladěnka P, Remião F, on behalf of The OEMONOM Researchers. Khat, a Cultural Chewing Drug: A Toxicokinetic and Toxicodynamic Summary. Toxins. 2022; 14(2):71. https://doi.org/10.3390/toxins14020071
Chicago/Turabian StyleSilva, Bárbara, Jorge Soares, Carolina Rocha-Pereira, Přemysl Mladěnka, Fernando Remião, and on behalf of The OEMONOM Researchers. 2022. "Khat, a Cultural Chewing Drug: A Toxicokinetic and Toxicodynamic Summary" Toxins 14, no. 2: 71. https://doi.org/10.3390/toxins14020071
APA StyleSilva, B., Soares, J., Rocha-Pereira, C., Mladěnka, P., Remião, F., & on behalf of The OEMONOM Researchers. (2022). Khat, a Cultural Chewing Drug: A Toxicokinetic and Toxicodynamic Summary. Toxins, 14(2), 71. https://doi.org/10.3390/toxins14020071