Incobotulinum Toxin Type A for Treatment of Ultraviolet-B-Induced Hyperpigmentation: A Prospective, Randomized, Controlled Trial

 ,
,  and
and
Abstract
:1. Introduction
2. Result
2.1. Subjects
2.2. Objective Assessment
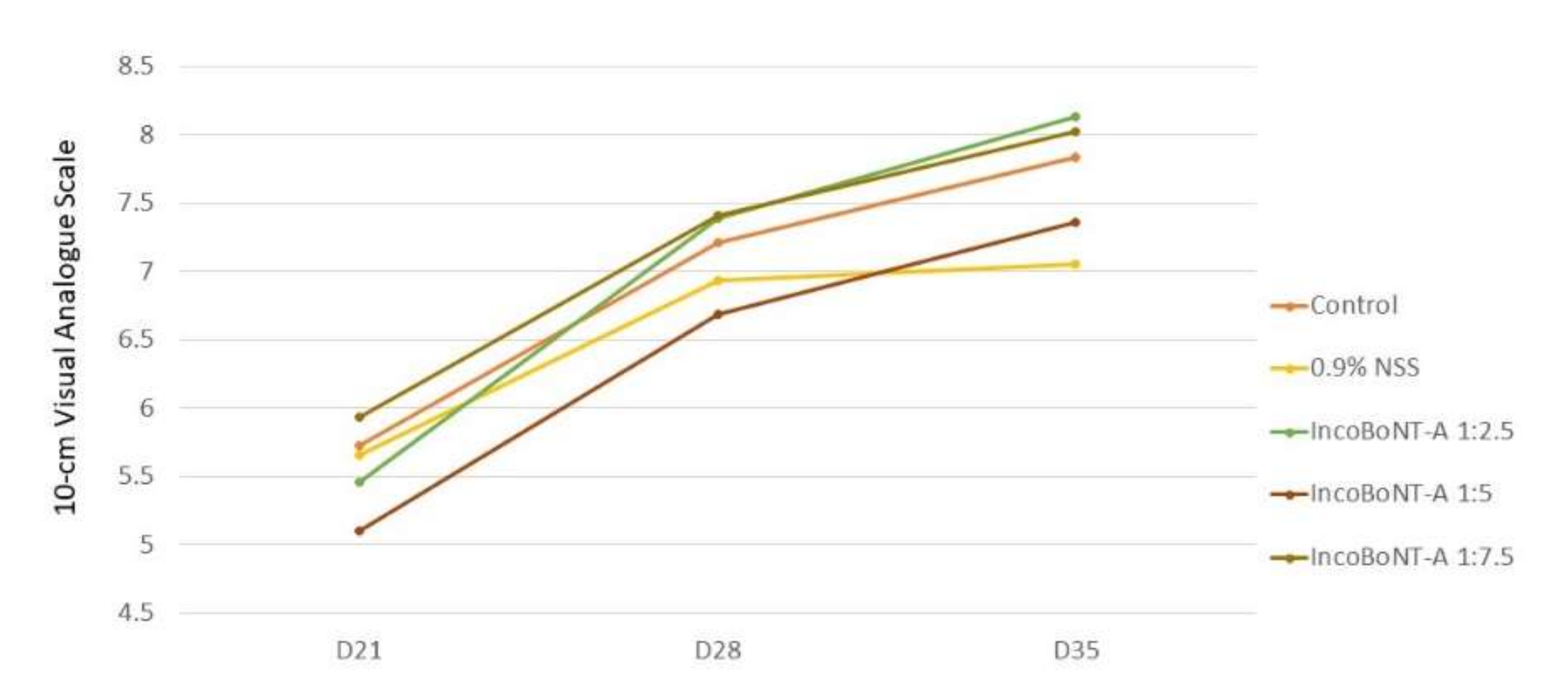
2.3. Subjective Assessment
2.4. Patient Satisfaction
2.5. Histopathologic Assessment
2.6. Side Effects
3. Discussion
4. Conclusions
5. Methods
5.1. Study Design
5.2. Subjects
5.3. Treatment
5.4. Objective Assessment
5.5. Subjective Assessment
5.6. Histopathologic Assessment
5.7. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Yamaguchi, Y.; Hearing, V.J. Physiological factors that regulate skin pigmentation. Biofactors 2009, 35, 193–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Larocca, C.; Kundu, R.; Vashi, N. Physiologic pigmentation: Molecular mechanisms and clinical diversity. Pigment. Int. 2014, 1, 44–51. [Google Scholar] [CrossRef]
- Alexis, A.F.; Sergay, A.B.; Taylor, S.C. Common dermatologic disorders in skin of color: A comparative practice survey. Cutis 2007, 80, 387–394. [Google Scholar] [PubMed]
- Kang, S.J.; Davis, S.A.; Feldman, S.R.; McMichael, A.J. Dyschromia in skin of color. J. Drugs Dermatol. 2014, 13, 401–406. [Google Scholar]
- Costin, G.E.; Hearing, V.J. Human skin pigmentation: Melanocytes modulate skin color in response to stress. FASEB J. 2007, 21, 976–994. [Google Scholar] [CrossRef]
- Gilchrest, B.A.; Park, H.Y.; Eller, M.S.; Yaar, M. Mechanisms of ultraviolet light-induced pigmentation. Photochem. Photobiol. 1996, 63, 1–10. [Google Scholar] [CrossRef]
- Jeong, S.M.; Yoon, T.J. Development of Pigmentation-Regulating Agents by Drug Repositioning. Int. J. Mol. Sci. 2021, 22, 3894. [Google Scholar] [CrossRef]
- Gillbro, J.M.; Olsson, M.J. The melanogenesis and mechanisms of skin-lightening agents-existing and new approaches. Int. J. Cosmet. Sci. 2011, 33, 210–221. [Google Scholar] [CrossRef]
- Imokawa, G. Autocrine and paracrine regulation of melanocytes in human skin and in pigmentary disorders. Pigment. Cell Res. 2004, 17, 96–110. [Google Scholar] [CrossRef]
- Carruthers, J.D.; Carruthers, J.A. Treatment of glabellar frown lines with C. botulinum-A exotoxin. J. Dermatol. Surg. Oncol. 1992, 18, 17–21. [Google Scholar] [CrossRef]
- Small, R. Botulinum toxin injection for facial wrinkles. Am. Fam. Physician 2014, 90, 168–175. [Google Scholar] [PubMed]
- Jung, J.A.; Kim, B.J.; Kim, M.S.; You, H.J.; Yoon, E.S.; Dhong, E.S.; Park, S.H.; Kim, D.W. Protective Effect of Botulinum Toxin against Ultraviolet-Induced Skin Pigmentation. Plast. Reconstr. Surg. 2019, 144, 347–356. [Google Scholar] [CrossRef]
- Vachiramon, V.; Kositkuljorn, C.; Leerunyakul, K.; Rattananukrom, T.; Jurairattanaporn, N. A Study of Botulinum Toxin A for Ultraviolet-Induced Hyperpigmentation: A Randomized Controlled Trial. Dermatol. Surg. 2021, 47, e174–e178. [Google Scholar] [CrossRef] [PubMed]
- Jurairattanaporn, N.; Palakornkitti, P.; Anuntrangsee, T.; Vachiramon, V. Study of botulinum toxin type A for the treatment of ultraviolet B-induced hyperpigmentation: A prospective, randomized, controlled trial. J. Cosmet. Dermatol. 2022. [Google Scholar] [CrossRef]
- Rappl, T.; Parvizi, D.; Friedl, H.; Wiedner, M.; May, S.; Kranzelbinder, B.; Wurzer, P.; Hellbom, B. Onset and duration of effect of incobotulinumtoxinA, onabotulinumtoxinA, and abobotulinumtoxinA in the treatment of glabellar frown lines: A randomized, double-blind study. Clin. Cosmet. Investig. Dermatol. 2013, 6, 211–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grether-Beck, S.; Marini, A.; Jaenicke, T.; Krutmann, J. Photoprotection of human skin beyond ultraviolet radiation. Photodermatol. Photoimmunol. Photomed. 2014, 30, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Balogh, T.S.; Velasco, M.V.; Pedriali, C.A.; Kaneko, T.M.; Baby, A.R. Ultraviolet radiation protection: Current available resources in photoprotection. An. Bras. Dermatol. 2011, 86, 732–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho, S.G.; Choi, W.; Brenner, M.; Miyamura, Y.; Yamaguchi, Y.; Wolber, R.; Smuda, C.; Batzer, J.; Kolbe, L.; Ito, S.; et al. Short- and long-term effects of UV radiation on the pigmentation of human skin. J. Investig. Dermatol. Symp. Proc. 2009, 14, 32–35. [Google Scholar] [CrossRef] [Green Version]
- D’Orazio, J.; Jarrett, S.; Amaro-Ortiz, A.; Scott, T. UV radiation and the skin. Int. J. Mol. Sci. 2013, 14, 12222–12248. [Google Scholar] [CrossRef] [Green Version]
- McGill, G.G.; Horstmann, M.; Widlund, H.R.; Du, J.; Motyckova, G.; Nishimura, E.K.; Lin, Y.L.; Ramaswamy, S.; Avery, W.; Ding, H.F.; et al. Bcl2 regulation by the melanocyte master regulator Mitf modulates lineage survival and melanoma cell viability. Cell 2002, 109, 707–718. [Google Scholar] [CrossRef] [Green Version]
- Rouzaud, F.; Costin, G.E.; Yamaguchi, Y.; Valencia, J.C.; Berens, W.F.; Chen, K.G.; Hoashi, T.; Bohm, M.; Abdel-Malek, Z.A.; Hearing, V.J. Regulation of constitutive and UVR-induced skin pigmentation by melanocortin 1 receptor isoforms. FASEB J. 2006, 20, 1927–1929. [Google Scholar] [CrossRef] [PubMed]
- Brenner, M.; Hearing, V.J. The protective role of melanin against UV damage in human skin. Photochem. Photobiol. 2008, 84, 539–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, T.T.; Schulman, J.; Fisher, D.E. UV and pigmentation: Molecular mechanisms and social controversies. Pigment. Cell Melanoma Res. 2008, 21, 509–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonaparte, J.P.; Ellis, D. Alterations in the Elasticity, Pliability, and Viscoelastic Properties of Facial Skin After Injection of Onabotulinum Toxin A. JAMA Facial Plast. Surg. 2015, 17, 256–263. [Google Scholar] [CrossRef] [Green Version]
- Barnes, M. Botulinum toxin--mechanisms of action and clinical use in spasticity. J. Rehabil. Med.-Suppl. 2003, 41, 56–59. [Google Scholar] [CrossRef] [Green Version]
- Irkoren, S.; Ozkan, H.S.; Ceylan, E.; Sivrioglu, N.; Tataroglu, C.; Durum, Y. The Effect of Botox on the Implant Stabilization and Capsular Formation: An Experimental Study. Ann. Plast. Surg. 2015, 75, 91–97. [Google Scholar] [CrossRef]
- Lamacz, M.; Tonon, M.C.; Louiset, E.; Cazin, L.; Strosberg, D.; Vaudry, H. Acetylcholine stimulates alpha-melanocyte-stimulating hormone release from frog pituitary melanotrophs through activation of muscarinic and nicotinic receptors. Endocrinology 1989, 125, 707–714. [Google Scholar] [CrossRef]
- Panicker, J.N.; Muthane, U.B. Botulinum toxins: Pharmacology and its current therapeutic evidence for use. Neurol. India 2003, 51, 455–460. [Google Scholar]
- Cartee, T.V.; Monheit, G.D. An overview of botulinum toxins: Past, present, and future. Clin. Plast. Surg. 2011, 38, 409–426. [Google Scholar] [CrossRef]
- Videira, I.F.; Moura, D.F.; Magina, S. Mechanisms regulating melanogenesis. An. Bras. Dermatol. 2013, 88, 76–83. [Google Scholar] [CrossRef] [Green Version]
- Schalka, S. New data on hyperpigmentation disorders. J. Eur. Acad. Dermatol. Venereol. 2017, 31 (Suppl. 5), 18–21. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day | Mean L*, Mean (±SD) | |||||
|---|---|---|---|---|---|---|
| Control | 0.9% NSS | IncoBoNT-A 1:2.5 | IncoBoNT-A 1:5 | IncoBoNT-A 1:7.5 | p-Value | |
| D0 * | 51.90 (±10.19) | 52.34 (±6.97) | 50.78 (±11.19) | 50.81 (±10.39) | 51.34 (±9.62) | 0.900 |
| D7 ** | 32.51 (±9.17) | 34.12 (±9.52) | 30.93 (±7.63) | 31.03 (±7.31) | 31.27 (±8.02) | 0379 |
| D21 | 34.13 (±7.39) | 34.23 (±7.86) | 35.35 (±7.46) | 34.84 (±7.66) | 33.34 (±6.98) | 0.858 |
| D28 | 37.49 (±8.66) | 37.06 (±8.29) | 37.86 (±9.32) | 36.65 (±9.06) | 36.28 (±7.55) | 0.923 |
| D35 | 38.09 (±8.25) | 37.47 (±6.16) | 38.16 (±6.61) | 35.48 (±8.25) | 37.40 (±6.68) | 0.612 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vachiramon, V.; Anuntrangsee, T.; Palakornkitti, P.; Jurairattanaporn, N.; Harnchoowong, S. Incobotulinum Toxin Type A for Treatment of Ultraviolet-B-Induced Hyperpigmentation: A Prospective, Randomized, Controlled Trial. Toxins 2022, 14, 417. https://doi.org/10.3390/toxins14060417
Vachiramon V, Anuntrangsee T, Palakornkitti P, Jurairattanaporn N, Harnchoowong S. Incobotulinum Toxin Type A for Treatment of Ultraviolet-B-Induced Hyperpigmentation: A Prospective, Randomized, Controlled Trial. Toxins. 2022; 14(6):417. https://doi.org/10.3390/toxins14060417
Chicago/Turabian StyleVachiramon, Vasanop, Tanaporn Anuntrangsee, Pasita Palakornkitti, Natthachat Jurairattanaporn, and Sarawin Harnchoowong. 2022. "Incobotulinum Toxin Type A for Treatment of Ultraviolet-B-Induced Hyperpigmentation: A Prospective, Randomized, Controlled Trial" Toxins 14, no. 6: 417. https://doi.org/10.3390/toxins14060417
APA StyleVachiramon, V., Anuntrangsee, T., Palakornkitti, P., Jurairattanaporn, N., & Harnchoowong, S. (2022). Incobotulinum Toxin Type A for Treatment of Ultraviolet-B-Induced Hyperpigmentation: A Prospective, Randomized, Controlled Trial. Toxins, 14(6), 417. https://doi.org/10.3390/toxins14060417