Treatment of Vestibulodynia with Submucosal Injections of IncobotulinumtoxinA into Targeted Painful Points: An Open-Label Exploratory Study


 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Results
2.1. Sample Description
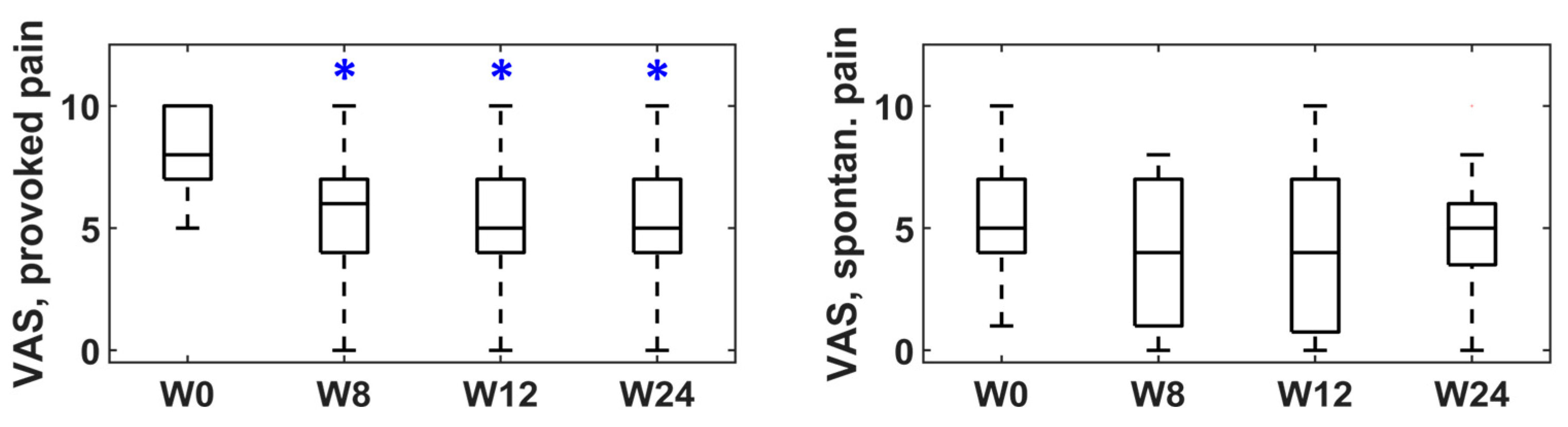
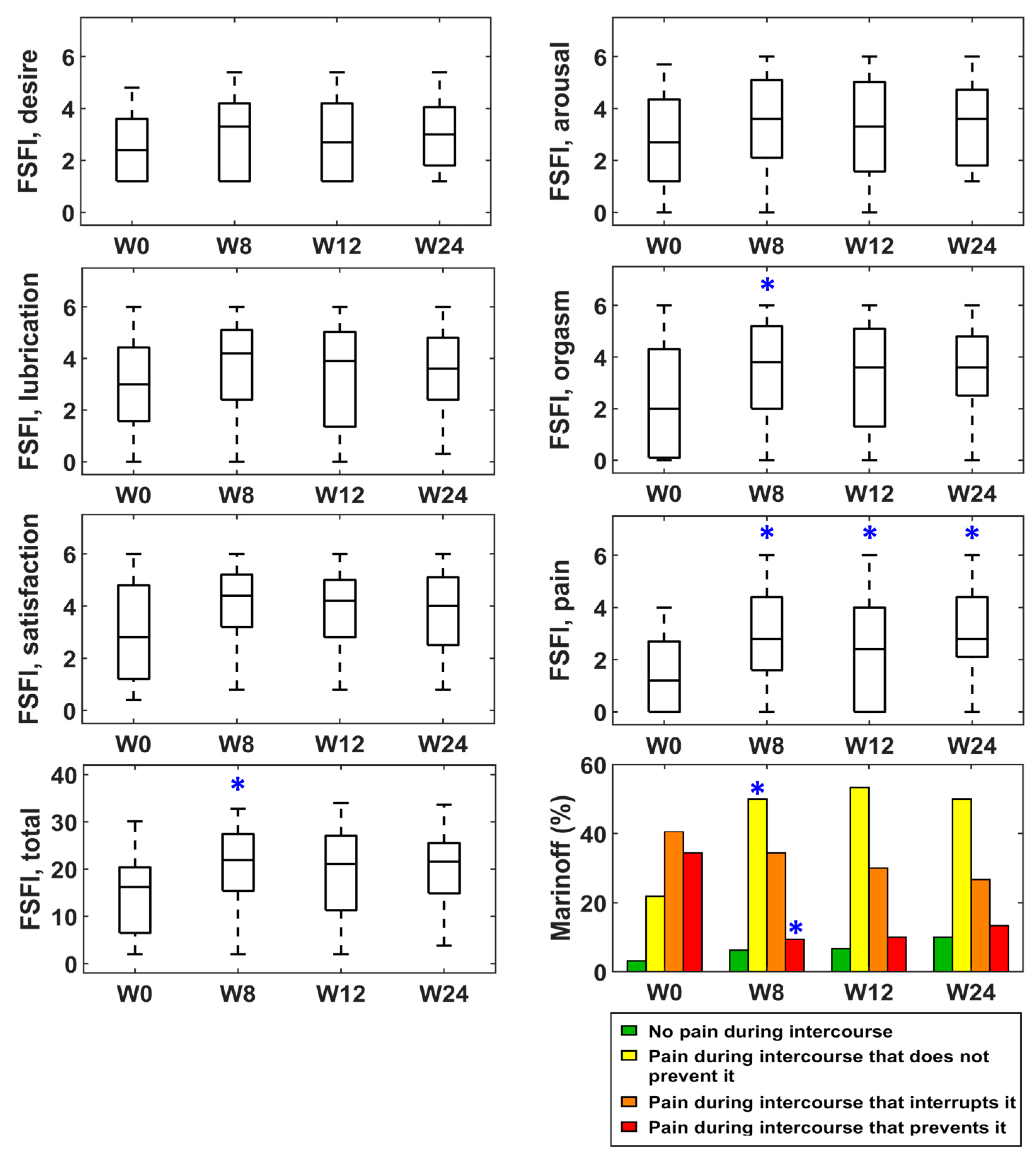
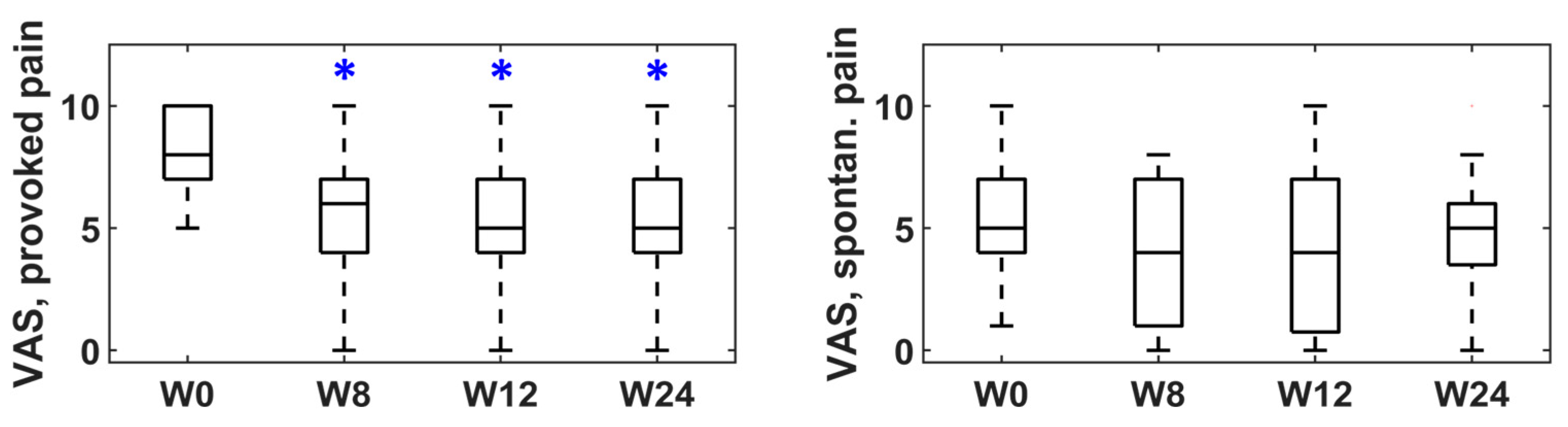
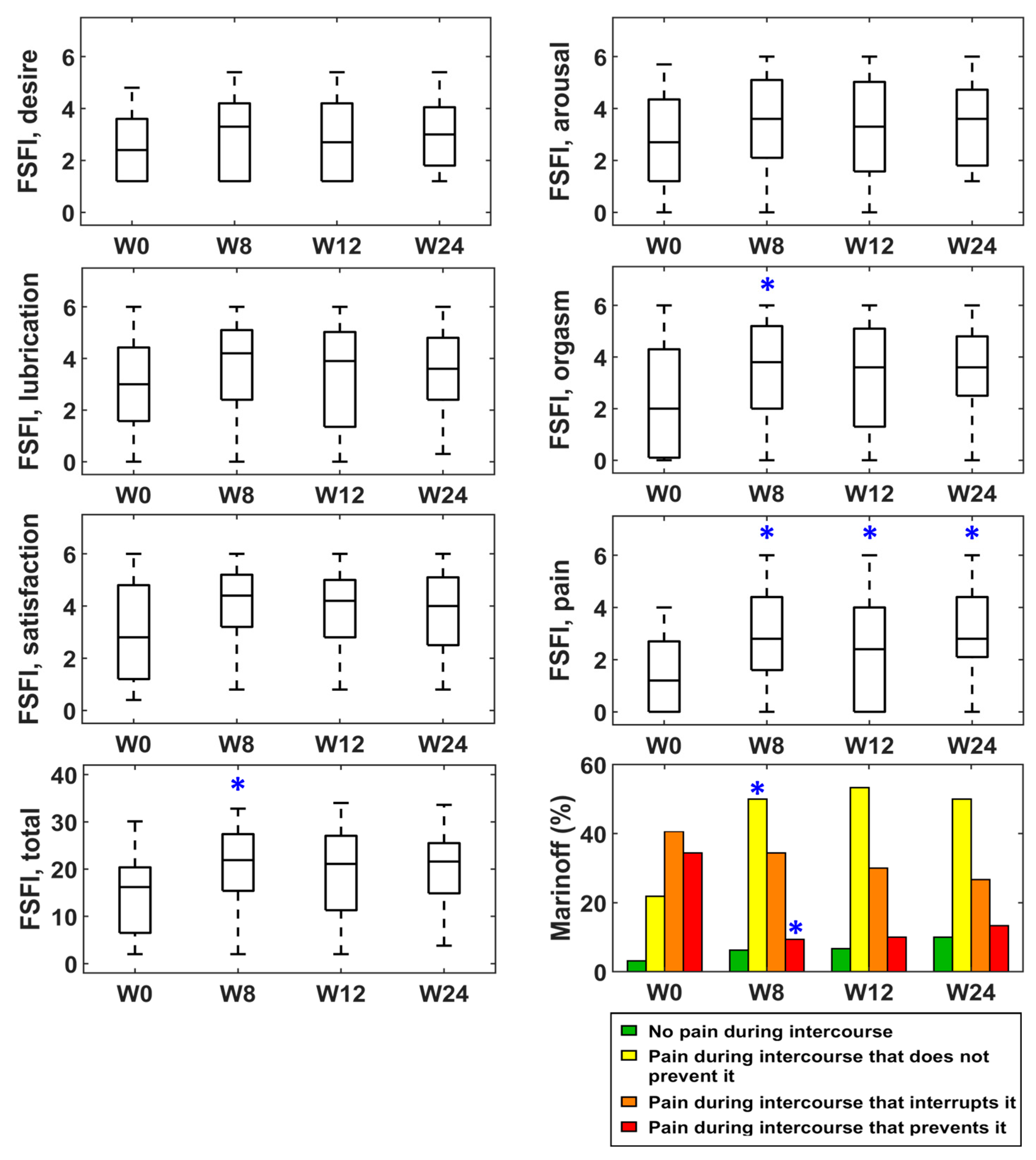
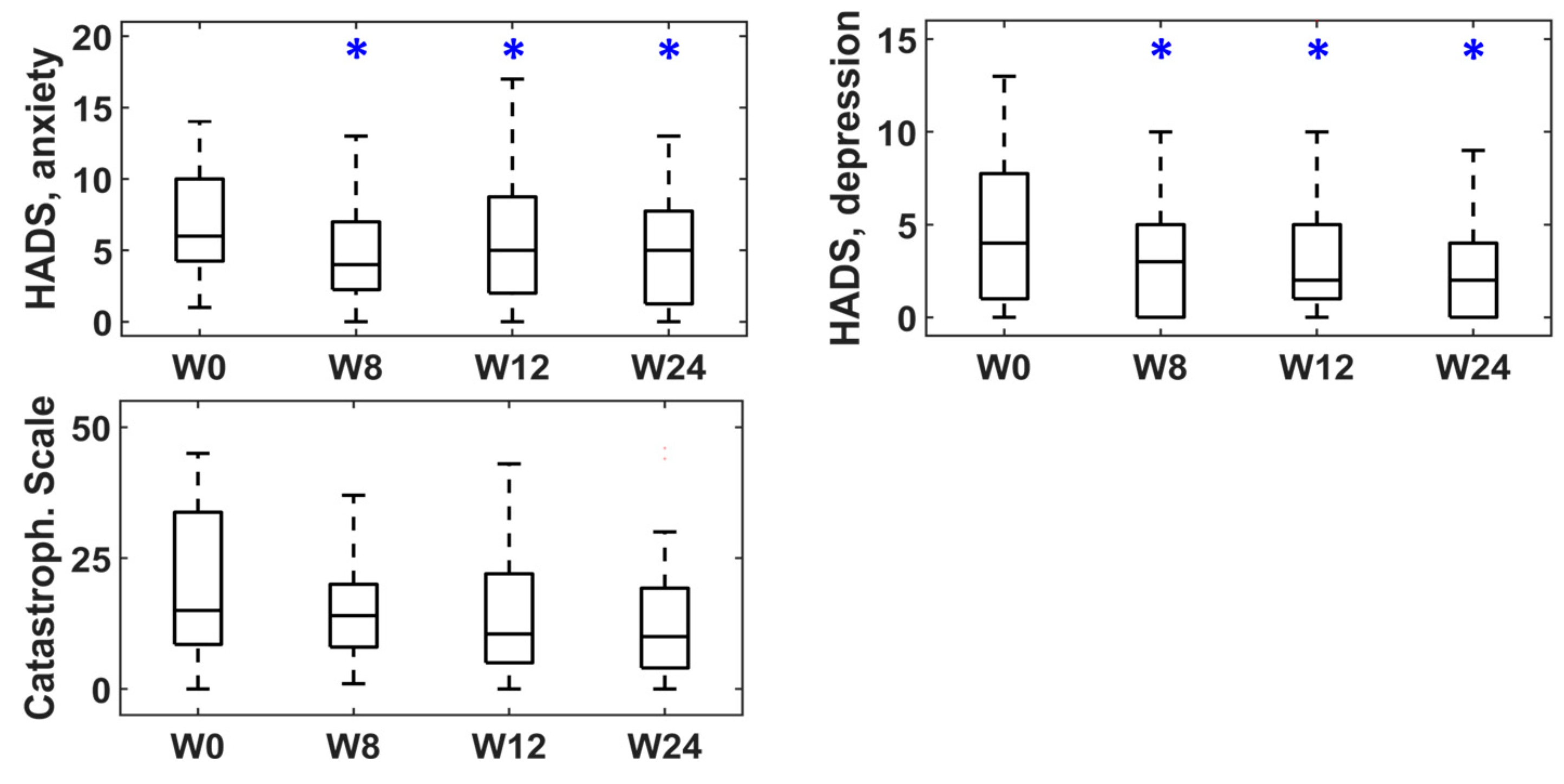
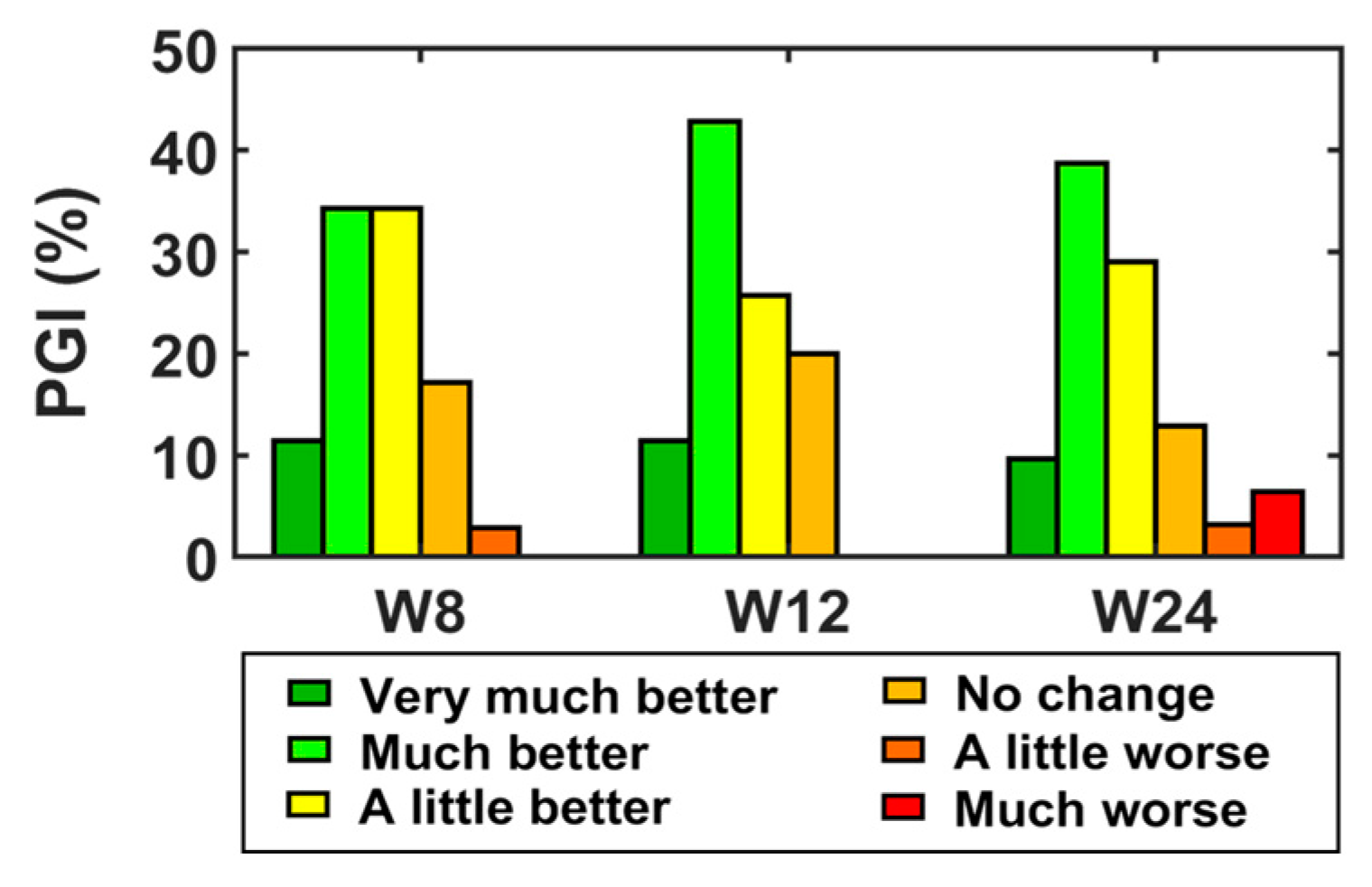
2.2. Evolution According to Clinical Questionnaires
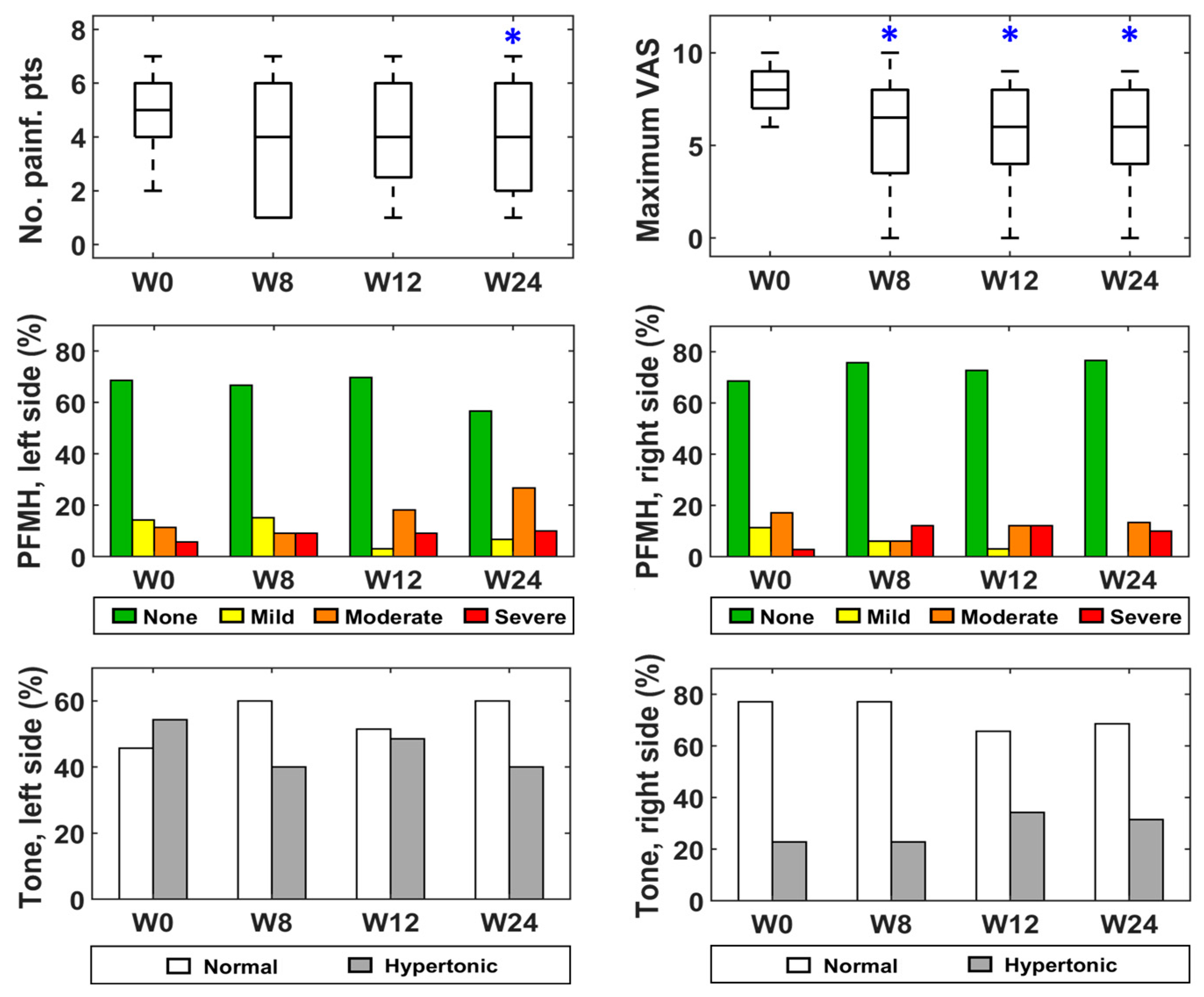
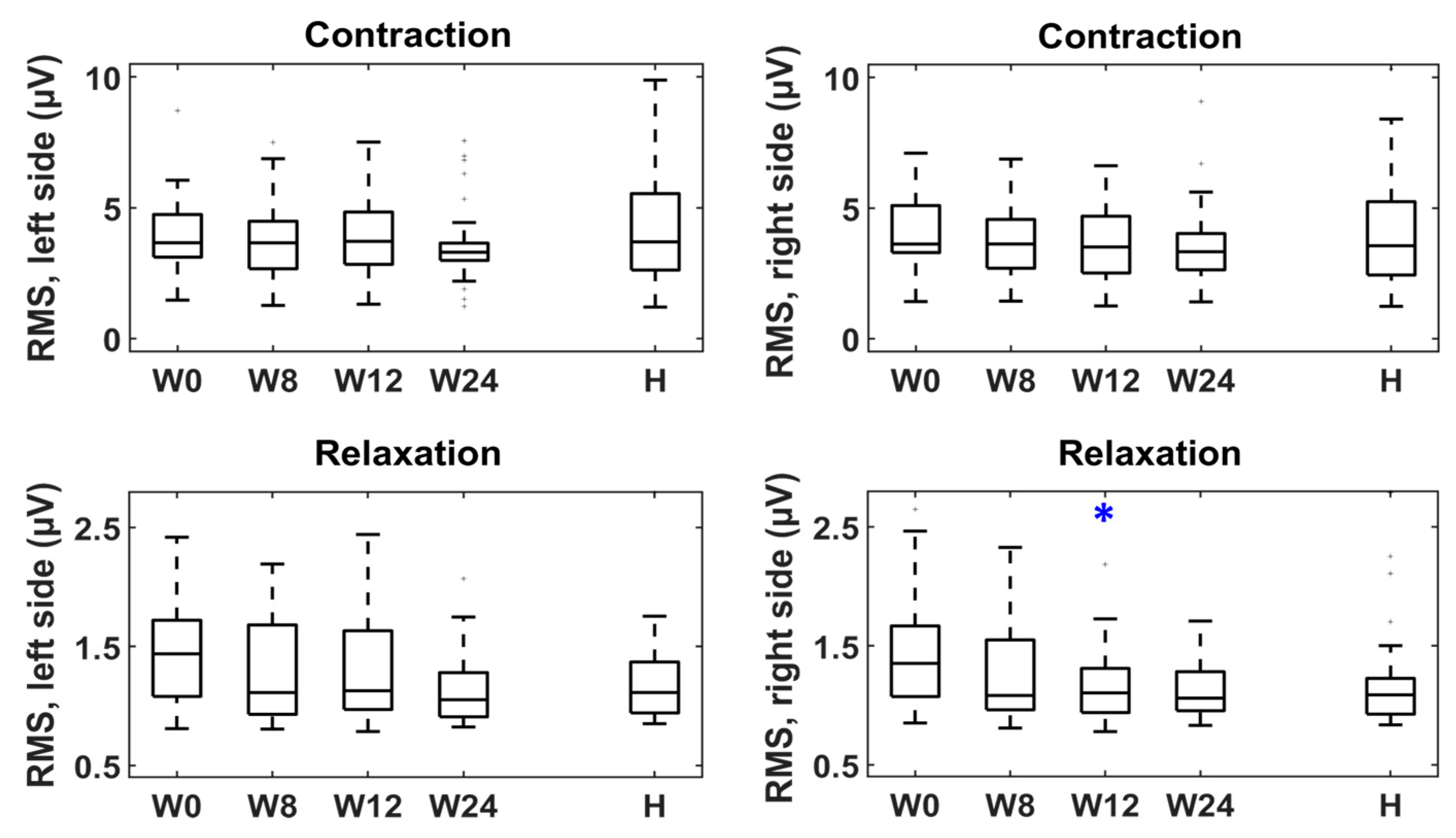
2.3. Evolution According to a Physical Examination and sEMG
2.4. Adverse Events
2.5. Analysis of Risk Factors
2.6. Sensitivity Analysis: Exclusion of the Patients Previously Treated with BoNT/A Injections into the Vestibule
3. Discussion
3.1. Patients’ Evolution after Treatment: Clinical Questionnaires
3.2. Patients’ Evolution after Treatment: Physical and Electrophysiological Exams
3.3. Patients’ Evolution after Treatment: Adverse Events
3.4. Response to BoNT/A: Definition of Clinically Significant Improvement
3.5. Response to BoNT/A: Risk and Protective Factors
3.6. Strengths and Limitations
4. Conclusions
5. Materials and Methods
5.1. Study Overview
5.2. Medical History
5.3. Monitoring Clinical Status
5.4. Monitoring Pelvic Physical Status
5.5. Monitoring Pelvic Floor Muscle Electrical Activity
5.6. BoNT/A Administration
5.7. Data Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bornstein, J.; Preti, M.; Simon, J.A.; As-Sanie, S.; Stockdale, C.; Stein, A.; Parish, S.J.; Radici, G.; Vieira-Baptista, P.; Pukall, C.; et al. Descriptors of Vulvodynia: A Multisocietal Definition Consensus (International Society for the Study of Vulvovaginal Disease, the International Society for the Study of Women Sexual Health, and the International Pelvic Pain Society). J. Low. Genit. Tract. Dis. 2019, 23, 161–163. [Google Scholar] [CrossRef] [PubMed]
- Henzell, H.; Berzins, K.; Langford, J.P. Provoked vestibulodynia: Current perspectives. Int. J. Women’s Health 2017, 9, 631. [Google Scholar] [CrossRef] [Green Version]
- Torres-Cueco, R.; Nohales-Alfonso, F. Vulvodynia—It Is Time to Accept a New Understanding from a Neurobiological Perspective. Int. J. Environ. Res. Public. Health 2021, 18, 6639. [Google Scholar] [CrossRef]
- Bergeron, S.; Reed, B.D.; Wesselmann, U.; Bohm-Starke, N. Vulvodynia. Nat. Rev. Dis. Primers 2020, 6, 36. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Shi, L.; Xiong, X.; Wu, E.; Veasley, C.; Dade, C. Economic burden and quality of life of vulvodynia in the United States. Curr. Med. Res. Opin. 2012, 28, 601–608. [Google Scholar] [CrossRef]
- Connor, J.J.; Haviland, M.; Brady, S.S.; Robinson, B.B.E.; Harlow, B.L. Psychosocial Factors Influence Sexual Satisfaction among Women with Vulvodynia. J. Sex. Marital. Ther. 2020, 46, 589–598. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.T.; Pukall, C.F.; Brown, C.; Bergeron, S.; Stein, A.; Kellogg-Spadt, S. Vulvodynia: Assessment and Treatment. Int. Consult. Sex. Med. Rep. 2016, 13, 572–590. [Google Scholar] [CrossRef]
- McLean, L.; Brooks, K. What Does Electromyography Tell Us About Dyspareunia? Sex. Med. Rev. 2017, 5, 282–294. [Google Scholar] [CrossRef]
- Sadownik, L.A.; Yong, P.J.; Smith, K.B. Systematic Review of Treatment Outcome Measures for Vulvodynia. J. Low. Genit. Tract. Dis. 2018, 22, 251–259. [Google Scholar] [CrossRef]
- De Andres, J.; Sanchis-Lopez, N.; Asensio-Samper, J.M.; Fabregat-Cid, G.; Villanueva-Perez, V.L.; Dolz, V.M.; Minguez, A.; De Andres, J. Vulvodynia—An Evidence-Based Literature Review and Proposed Treatment Algorithm. Pain Pract. 2016, 16, 204–236. [Google Scholar] [CrossRef]
- Vasileva, P.; Strashilov, S.A.; Yordanov, A.D. Aetiology, diagnosis, and clinical management of vulvodynia. Menopause Rev./Przegląd Menopauzalny 2020, 19, 44–48. [Google Scholar] [CrossRef] [PubMed]
- Sinha, D.; Karri, K.; Arunkalaivanan, A.S. Applications of Botulinum toxin in urogynaecology. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 133, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R. Therapeutic use of botulinum toxin in pain treatment. Neuronal Signal 2018, 2, 20180058. [Google Scholar] [CrossRef] [Green Version]
- Yi, K.-H.; Lee, J.-H.; Lee, D.K.; Hu, H.-W.; Seo, K.K.; Kim, H.-J. Anatomical locations of the motor endplates of sartorius muscle for botulinum toxin injections in treatment of muscle spasticity. Surg. Radiol. Anat. 2021, 43, 2025–2030. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.; Hu, H.; Lee, J.; An, M.H.; Lee, H.; Choi, Y.; Kim, H. Sihler’s staining technique: How to and guidance for botulinum neurotoxin injection in human muscles. Clin. Anat. 2023. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Chen, Y.-T.; Liu, Y.; Magat, E.; Gutierrez-Verduzco, M.; Francisco, G.E.; Zhou, P.; Li, S.; Zhang, Y. Improving Botulinum Toxin Efficiency in Treating Post-Stroke Spasticity Using 3D Innervation Zone Imaging. Int. J. Neural. Syst. 2021, 31, 2150007. [Google Scholar] [CrossRef] [PubMed]
- Meister, M.R.; Brubaker, A.; Sutcliffe, S.; Lowder, J.L. Effectiveness of Botulinum Toxin for Treatment of Symptomatic Pelvic Floor Myofascial Pain in Women: A Systematic Review and Meta-analysis. Female Pelvic. Med. Reconstr. Surg. 2021, 27, e152–e160. [Google Scholar] [CrossRef] [PubMed]
- Tarazona-Motes, M.; Albaladejo-Belmonte, M.; Nohales-Alfonso, F.J.; De-Arriba, M.; Garcia-Casado, J.; Alberola-Rubio, J. Treatment of Dyspareunia with Botulinum Neurotoxin Type A: Clinical Improvement and Influence of Patients’ Characteristics. Int. J. Environ. Res. Public. Health 2021, 18, 8783. [Google Scholar] [CrossRef] [PubMed]
- Dykstra, D.D.; Presthus, J. Botulinum toxin type A for the treatment of provoked vestibulodynia: An open-label, pilot study. J. Reprod. Med. 2006, 51, 467–470. [Google Scholar]
- Yoon, H.; Chung, W.S.; Shim, B.S. Botulinum toxin A for the management of vulvodynia. Int. J. Impot. Res. 2007, 19, 84–87. [Google Scholar] [CrossRef]
- Gunter, J.; Brewer, A.; Tawfik, O. Botulinum toxin a for vulvodynia: A case report. J. Pain 2004, 5, 238–240. [Google Scholar] [CrossRef]
- Brown, C.S.; I Glazer, H.; Vogt, V.; Menkes, D.; Bachmann, G. Subjective and objective outcomes of botulinum toxin type A treatment in vestibulodynia: Pilot data. J. Reprod. Med. 2006, 51, 635–641. [Google Scholar]
- Petersen, C.D.; Giraldi, A.; Lundvall, L.; Kristensen, E. Botulinum Toxin Type A—A Novel Treatment for Provoked Vestibulodynia? Results from a Randomized, Placebo Controlled, Double Blinded Study. J. Sex Med. 2009, 6, 2523–2537. [Google Scholar] [CrossRef]
- Diomande, I.; Gabriel, N.; Kashiwagi, M.; Ghisu, G.-P.; Welter, J.; Fink, D.; Fehr, M.K.; Betschart, C. Subcutaneous botulinum toxin type A injections for provoked vestibulodynia: A randomized placebo-controlled trial and exploratory subanalysis. Arch. Gynecol. Obstet. 2019, 299, 993–1000. [Google Scholar] [CrossRef]
- Haraldson, P.; Mühlrad, H.; Heddini, U.; Nilsson, K.; Bohm-Starke, N. Botulinum Toxin A as a Treatment for Provoked Vestibulodynia: A Randomized Controlled Trial. Obstet. Gynecol. 2020, 136, 524–532. [Google Scholar] [CrossRef]
- Pelletier, F.; Girardin, M.; Humbert, P.; Puyraveau, M.; Aubin, F.; Parratte, B. Long-term assessment of effectiveness and quality of life of OnabotulinumtoxinA injections in provoked vestibulodynia. J. Eur. Acad. Dermatol. Venereol. 2016, 30, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, F.; Parratte, B.; Penz, S.; Moreno, J.; Aubin, F.; Humbert, P. Efficacy of high doses of botulinum toxin A for treating provoked vestibulodynia. Br. J. Dermatol. 2011, 164, 617–622. [Google Scholar] [CrossRef]
- Ghizzani, A.; Carta, S.; Casoni, A.; Ferrata, P.; Luisi, S.; Fortina, M. Differentiating overlapping symptoms of vulvodynia and pudendal neuralgia. Br. J. Pain 2019, 13, 54–58. [Google Scholar] [CrossRef]
- Zhang, Z.; Zolnoun, D.A.; Francisco, E.M.B.; Holden, J.K.B.; Dennis, R.G.; Tommerdahl, M. Altered central sensitization in subgroups of women with vulvodynia. Clin. J. Pain 2011, 27, 755–763. [Google Scholar] [CrossRef] [PubMed]
- Shallcross, R.; Dickson, J.; Nunns, D.; MacKenzie, C.; Kiemle, G. Women’s Subjective Experiences of Living with Vulvodynia: A Systematic Review and Meta-Ethnography. Arch. Sex Behav. 2018, 47, 577–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gentilcore-Saulnier, E.; McLean, L.; Goldfinger, C.; Pukall, C.F.; Chamberlain, S. Pelvic floor muscle assessment outcomes in women with and without provoked vestibulodynia and the impact of a physical therapy program. J. Sex Med. 2010, 7, 1003–1022. [Google Scholar] [CrossRef] [PubMed]
- Zachariou, A.; Filiponi, M.; Kaltsas, A.; Dimitriadis, F.; Mamoulakis, C.; Karagiannis, A.; Tsounapi, P.; Takenaka, A.; Sofikitis, N. The strength of the pelvic floor muscles contributes to a better female sexual function. J. Sex Med. 2022, 19, S29. [Google Scholar] [CrossRef]
- Juhász, M.; Hosking, A.-M.; Mesinkovska, N.A. Botulinum Toxins in Medical and Cosmetic Dermatology. EMJ Dermatol. 2021. [Google Scholar] [CrossRef]
- Frevert, J. Xeomin®: An innovative new botulinum toxin type A-Frevert-2009-European Journal of Neurology. Eur. J. Neurol. 2009, 16, 11–13. [Google Scholar] [CrossRef] [PubMed]
- LaRowe, L.R.; Ditre, J.W. Pain, nicotine, and tobacco smoking: Current state of the science. Pain 2020, 161, 1688–1693. [Google Scholar] [CrossRef]
- Palacios, S.; González, S.P.; Fernández-Abellán, M.; Manubens, M.; García-Alfaro, P.; Argudo Prieto, C.; Baquedando Mainar, L.; Abu-Amshah, J.C.; Cancelo Hidalgo, M.J.; Castelo-Branco i Flores, C.; et al. Impact of Vulvovaginal Atrophy of Menopause In Spanish Women: Prevalence And Symptoms According To The EVES Study. Sex Med. 2019, 7, 207–216. [Google Scholar] [CrossRef] [Green Version]
- Klifto, K.M.; Lee Dellon, A. Persistent Genital Arousal Disorder: Review of Pertinent Peripheral Nerves. Sex Med. Rev. 2020, 8, 265–273. [Google Scholar] [CrossRef]
- Pukall, C.F.; Mitchell, L.S.; Goldstein, A.T. Non-Medical, Medical, and Surgical Approaches for the Treatment of Provoked Vestibulodynia. Curr. Sex Health Rep. 2016, 8, 240–248. [Google Scholar] [CrossRef]
- Levesque, A.; Riant, T.; Ploteau, S.; Rigaud, J.; Labat, J.J.; Convergences PP Network. Clinical Criteria of Central Sensitization in Chronic Pelvic and Perineal Pain (Convergences PP Criteria): Elaboration of a Clinical Evaluation Tool Based on Formal Expert Consensus. Pain Med. 2018, 19, 2009–2015. [Google Scholar] [CrossRef] [Green Version]
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R., Jr. The Female Sexual Function Index (FSFI): A Multidimensional Self-Report Instrument for the Assessment of Female Sexual Function. J. Sex Marital. Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef]
- De Seta, F.; Stabile, G.; Antoci, G.; Zito, G.; Nappi, R.E. Provoked Vestibulodynia and Topical Treatment: A New Option. Healthcare 2022, 10, 830. [Google Scholar] [CrossRef] [PubMed]
- Bjelland, I.; Dahl, A.A.; Haug, T.T.; Neckelmann, D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J. Psychosom. Res. 2002, 52, 69–77. [Google Scholar] [CrossRef]
- Sewell, M.; Churilov, L.; Mooney, S.; Ma, T.; Maher, P.; Grover, S.R. Chronic pelvic pain-pain catastrophizing, pelvic pain and quality of life. Scand. J. Pain 2018, 18, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Srikrishna, S.; Robinson, D.; Cardozo, L. Validation of the Patient Global Impression of Improvement (PGI-I) for urogenital prolapse. Int. Urogynecol. J. 2010, 21, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Labat, J.-J.; Riant, T.; Robert, R.; Amarenco, G.; Lefaucheur, J.-P.; Rigaud, J. Diagnostic criteria for pudendal neuralgia by pudendal nerve entrapment (Nantes criteria). Neurourol. Urodyn. 2008, 27, 306–310. [Google Scholar] [CrossRef]
- Bhide, A.A.; Puccini, F.; Bray, R.; Khullar, V.; Digesu, G.A. The pelvic floor muscle hyperalgesia (PFMH) scoring system: A new classification tool to assess women with chronic pelvic pain: Multicentre pilot study of validity and reliability. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 193, 111–113. [Google Scholar] [CrossRef]
- Gerbershagen, H.J.; Rothaug, J.; Kalkman, C.J.; Meissner, W. Determination of moderate-to-severe postoperative pain on the numeric rating scale: A cut-off point analysis applying four different methods. Br. J. Anaesth. 2011, 107, 619–626. [Google Scholar] [CrossRef] [Green Version]
- Albaladejo-Belmonte, M.; Nohales-Alfonso, F.J.; Tarazona-Motes, M.; De-Arriba, M.; Alberola-Rubio, J.; Garcia-Casado, J. Effect of BoNT/A in the Surface Electromyographic Characteristics of the Pelvic Floor Muscles for the Treatment of Chronic Pelvic Pain. Sensors 2021, 21, 4668. [Google Scholar] [CrossRef]
- Albaladejo-Belmonte, M.; Tarazona-Motes, M.; Nohales-Alfonso, F.J.; De-Arriba, M.; Alberola-Rubio, J.; Garcia-Casado, J. Characterization of Pelvic Floor Activity in Healthy Subjects and with Chronic Pelvic Pain: Diagnostic Potential of Surface Electromyography. Sensors 2021, 21, 2225. [Google Scholar] [CrossRef]
- Simon, J.; Parish, S.; Bernick, B.; Graham, S.; Mirkin, S. 020 Bioidentical Combined Estradiol and Progesterone Capsules Improved Vaginal Dryness in Women with Vasomotor Symptoms. J. Sex Med. 2019, 16, S9–S10. [Google Scholar] [CrossRef]
- Van der Vaart, L.R.; Vollebregt, A.; Milani, A.L.; Lagro-Janssen, A.L.; Duijnhoven, R.G.; Roovers, J.P.; Van der Vaart, C.H. Pessary or surgery for a symptomatic pelvic organ prolapse: The PEOPLE study, a multicentre prospective cohort study. BJOG 2021, 129, 820–829. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Fattah, M.; Cao, G.; Mostafa, A. Long-term outcomes for transobturator tension-free vaginal tapes in women with urodynamic mixed urinary incontinence. Neurourol. Urodyn. 2017, 36, 902–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Sample Size | Placebo-Controlled | Randomized | Open Label | Dose/Side | Repeated Injections | Clinical Dimensions Monitored |
|---|---|---|---|---|---|---|---|
| Petersen et al., 2009 [23] | 64 | Yes | Yes | No | 20 units | No | Day-to-day pain Sexual function Quality of life |
| Pelletier et al., 2016 [26] | 19 | No | No | Yes | 50 units | No | Day-to-day pain Sexual function Quality of life |
| Diomande et al., 2019 [24] | 31 | Yes | Yes | No | 50 or 100 units | Yes (6 months later) | Vulvar sensitivity Sexual function |
| Haraldson et al., 2020 [25] | 88 | Yes | Yes | No | 20 units | No | PFM strength Sexual function |
| Background | Characteristic | Mean ± SD | No. of Patients | % | |
|---|---|---|---|---|---|
| General | Age (years) | 41.9 ± 14.1 | |||
| Body mass index (kg/m2) | 22.4 ± 2.7 | ||||
| Academic background | Reading and writing | 0/35 | 0.0 | ||
| Primary | 1/35 | 2.9 | |||
| Secondary | 6/35 | 17.1 | |||
| Undergraduate | 10/35 | 28.6 | |||
| Graduate | 18/35 | 51.4 | |||
| Postgraduate | 0/35 | 0.0 | |||
| Work activity | Unemployed | 2/35 | 5.7 | ||
| Pensioner | 2/35 | 5.7 | |||
| Work incapacity | 1/35 | 2.9 | |||
| Active worker | 21/35 | 60.0 | |||
| Student | 6/35 | 17.1 | |||
| Off work | 1/35 | 2.9 | |||
| Housewife | 2/35 | 5.7 | |||
| Smoke | 8/35 | 22.9 | |||
| History of abuse | 3/35 | 8.6 | |||
| Obstetric | Pregnancies | 16/35 | 45.7 | ||
| Vaginal deliveries | 9/16 | 56.3 | |||
| Episiotomy | 7/9 | 77.8 | |||
| Perineal tears | 5/9 | 55.6 | |||
| Cesarean sections | 6/16 | 37.5 | |||
| Gynecological | Vulvovaginal trauma | 7/35 | 20.0 | ||
| Vulvovaginal infections/inflammations | 6/35 | 17.1 | |||
| Menopause (hormonal deficiencies) | 12/35 | 34.3 | |||
| Comorbidities | Cervical pain | 15/35 | 42.9 | ||
| Lumbar pain | 13/35 | 37.1 | |||
| Headaches | 11/35 | 31.5 | |||
| Temporomandibular joint pain | 13/35 | 37.1 | |||
| Allergies/intolerances | 12/35 | 34.3 | |||
| Vestibulodynia description | Inciting factor | Provoked | 21/35 | 60.0 | |
| Spontaneous | 0/35 | 0.0 | |||
| Mixed | 14/35 | 40.0 | |||
| Location | Generalized | 27/35 | 77.1 | ||
| Localized | 8/35 | 22.9 | |||
| Temporal pattern (provoked pain) | Punctual, short duration | 26/35 | 74.3 | ||
| Intermit., few days | 0/35 | 0.0 | |||
| Constant, few days | 6/35 | 17.1 | |||
| Intermit., long time | 1/35 | 2.9 | |||
| Constant, long time | 1/35 | 2.9 | |||
| Temporal pattern (spontaneous pain) | Punctual, short duration | 27/35 | 77.1 | ||
| Intermit., few days | 1/35 | 2.9 | |||
| Constant, few days | 1/35 | 2.9 | |||
| Intermit., long time | 5/35 | 14.3 | |||
| Constant, long time | 7/35 | 20.0 | |||
| Years since pain onset | 6.9 ± 6.3 | ||||
| Other symptoms | Myofascial pelvic pain | 17/35 | 48.6 | ||
| Adverse Event | Onset | Duration | Severity |
|---|---|---|---|
| Stress urinary incontinence | 2 weeks after treatment | 7 weeks | Mild |
| Difficulties in achieving climax | 4 weeks after treatment | 6 weeks | Mild |
| Factor | OR | 95% CI | p-Value |
|---|---|---|---|
| Smoking | 7.12 | [1.10–46.20] | 0.03 |
| Associated painful syndromes (sensitization questionnaire) | 6.88 | [1.08–43.61] | 0.03 |
| Vestibular pain at the 3 o’clock position | 0.15 | [0.02–0.97] | 0.04 |
| Maximum VAS score (cotton swab test) | 0.41 | [0.17–0.96] | 0.03 |
| FSFI score (orgasm domain) | 2.18 | [1.00–4.78] | 0.04 |
| Previous Visit | Week 0 | Week 8 | Week 12 | Week 24 | |
|---|---|---|---|---|---|
| Eligibility criteria | X | ||||
| Patient’s informed consent | X | ||||
| Medical history | X | ||||
Physical examination
| |||||
| X | X | X | X | X | |
| X | X | X | X | X | |
| X | X | X | X | X | |
| X | X | X | X | X | |
| X | X | X | X | ||
Clinical questionnaires
| |||||
| X | X | X | X | ||
| X | X | X | X | ||
| X | X | X | X | ||
| X | X | X | X | ||
| X | X | X | |||
| sEMG recording | X | X | X | X | |
| Administration of BoNT/A | X | ||||
| Adverse events | X | X | X | X | |
| Intercurrent medication | X | X | X | X | |
| Morbidity | X | X | X | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villa-Muñoz, P.; Albaladejo-Belmonte, M.; Nohales-Alfonso, F.J.; Alberola-Rubio, J.; Garcia-Casado, J. Treatment of Vestibulodynia with Submucosal Injections of IncobotulinumtoxinA into Targeted Painful Points: An Open-Label Exploratory Study. Toxins 2023, 15, 476. https://doi.org/10.3390/toxins15080476
Villa-Muñoz P, Albaladejo-Belmonte M, Nohales-Alfonso FJ, Alberola-Rubio J, Garcia-Casado J. Treatment of Vestibulodynia with Submucosal Injections of IncobotulinumtoxinA into Targeted Painful Points: An Open-Label Exploratory Study. Toxins. 2023; 15(8):476. https://doi.org/10.3390/toxins15080476
Chicago/Turabian StyleVilla-Muñoz, Paula, Monica Albaladejo-Belmonte, Francisco J. Nohales-Alfonso, Jose Alberola-Rubio, and Javier Garcia-Casado. 2023. "Treatment of Vestibulodynia with Submucosal Injections of IncobotulinumtoxinA into Targeted Painful Points: An Open-Label Exploratory Study" Toxins 15, no. 8: 476. https://doi.org/10.3390/toxins15080476