Botulinum Toxin Injections for Psychiatric Disorders: A Systematic Review of the Clinical Trial Landscape

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Quality Assessment
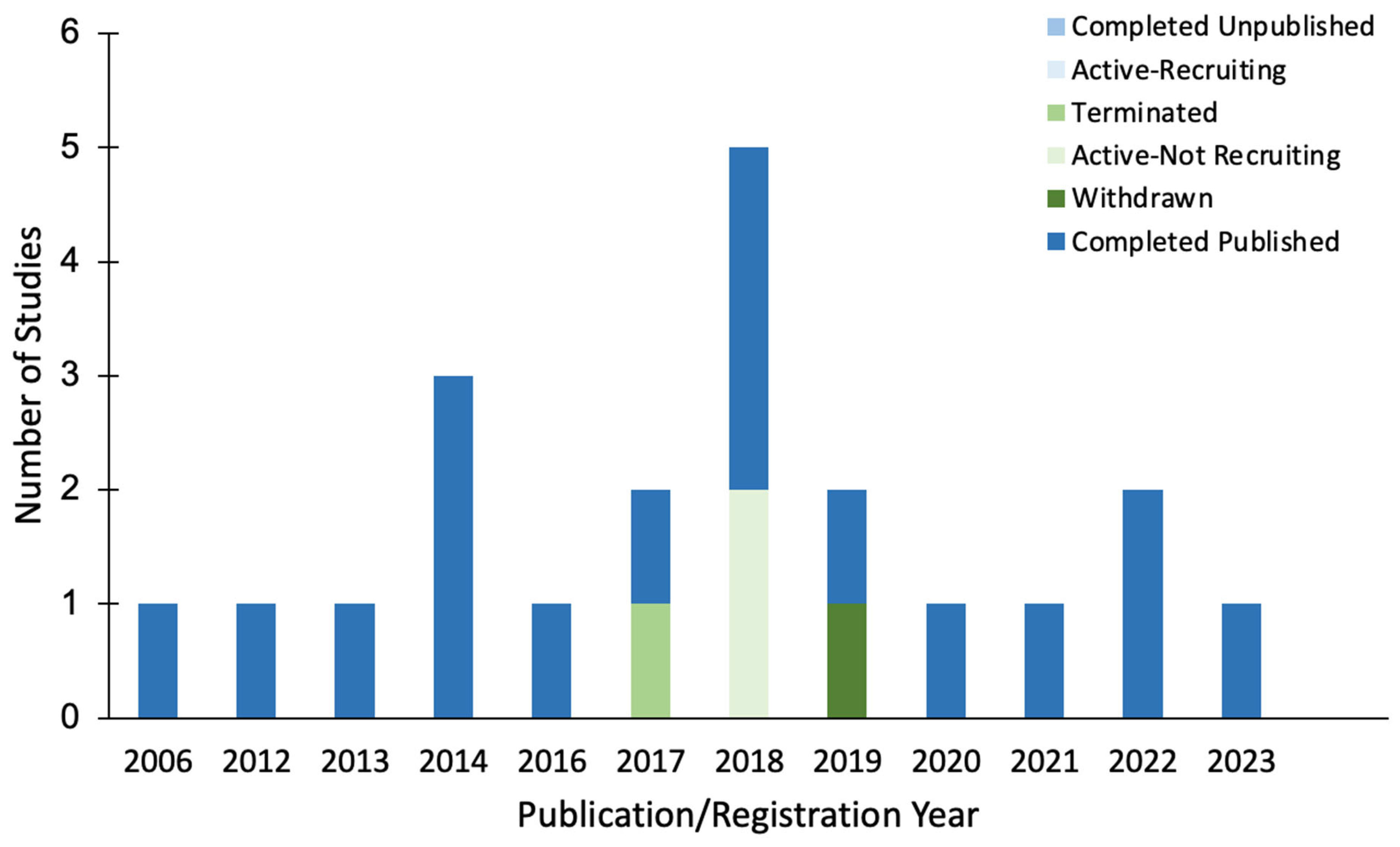
2.2. Studies by Start Date and Completion Status
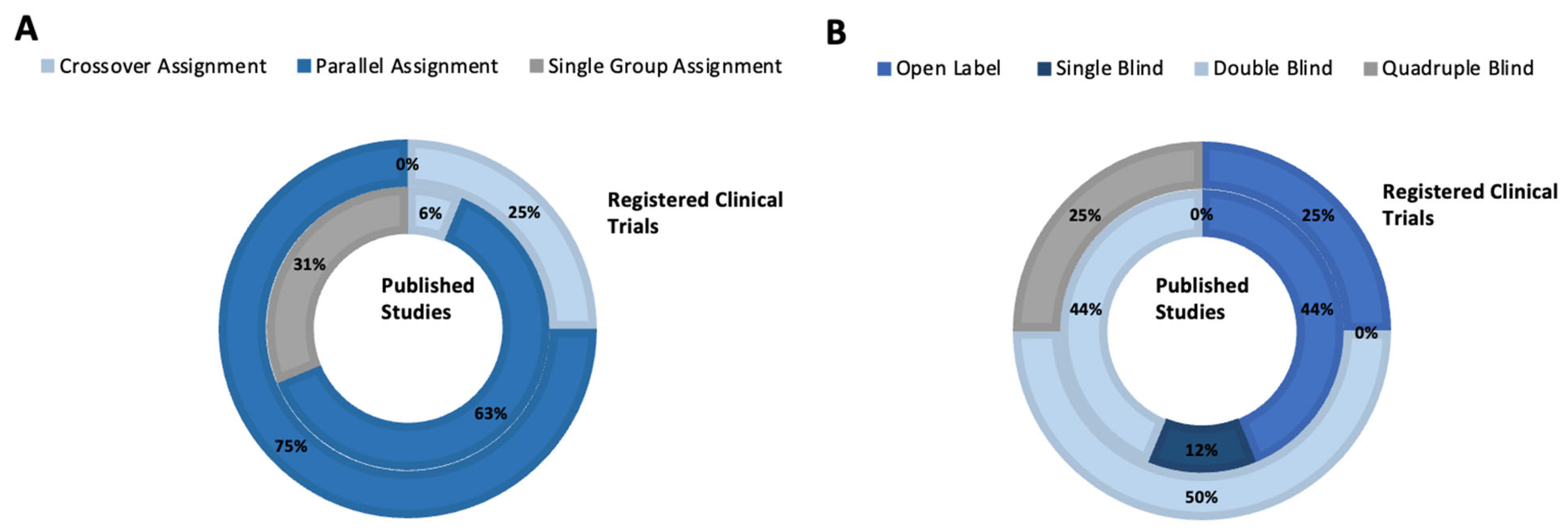
2.3. Studies by Phase and Design
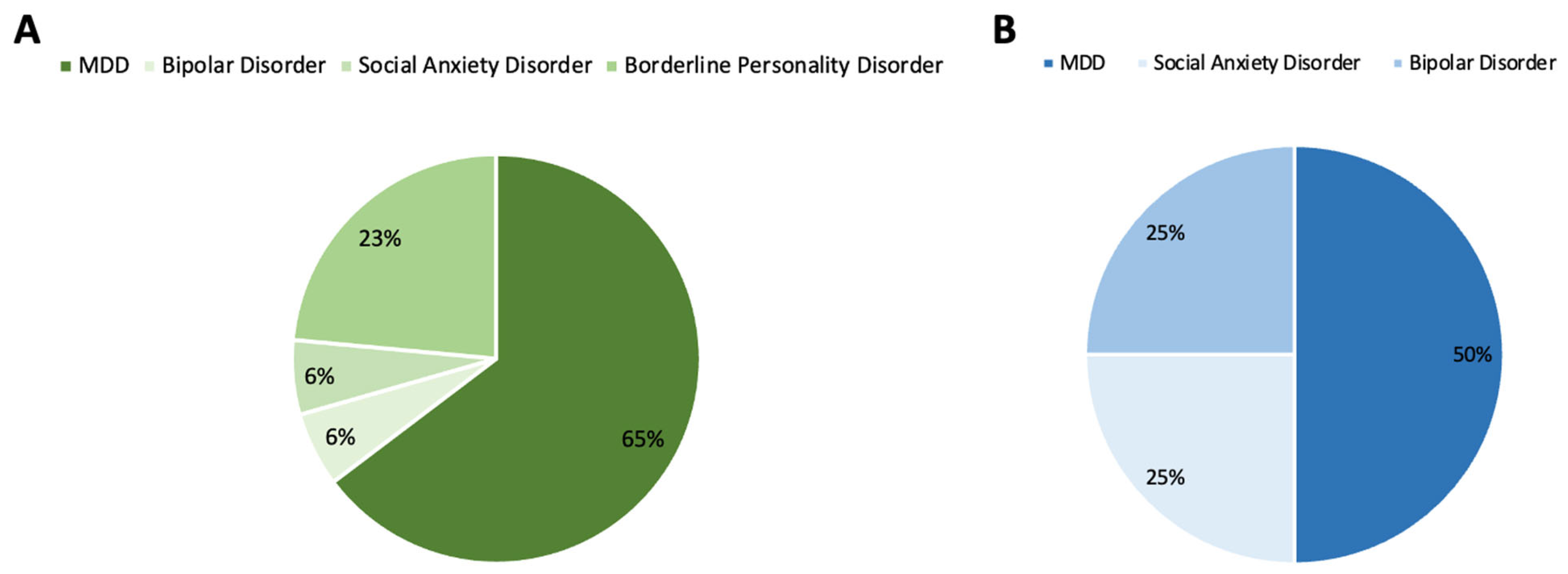
2.4. Studies by Clinical Indication
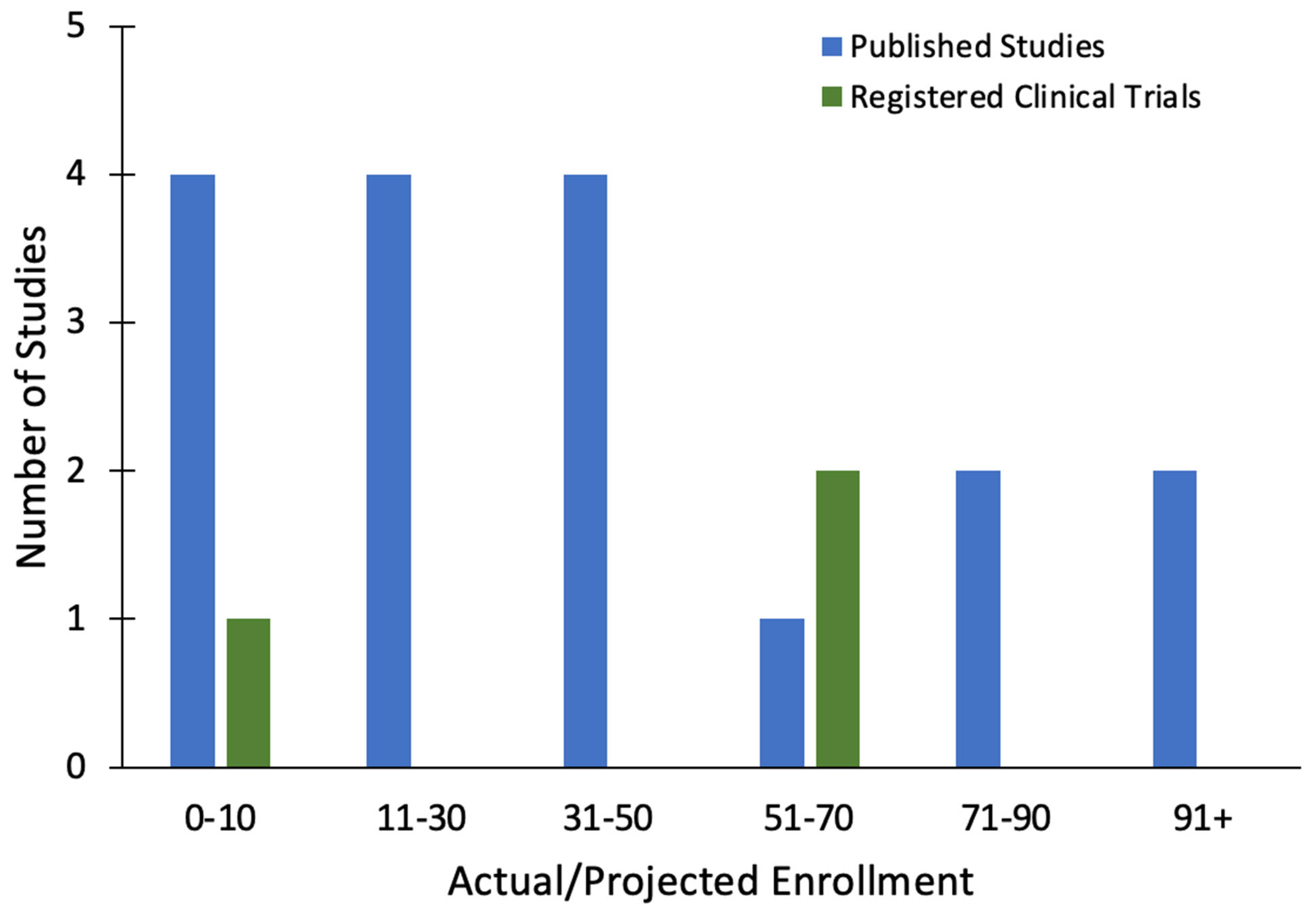
2.5. Studies by Enrolled Participants
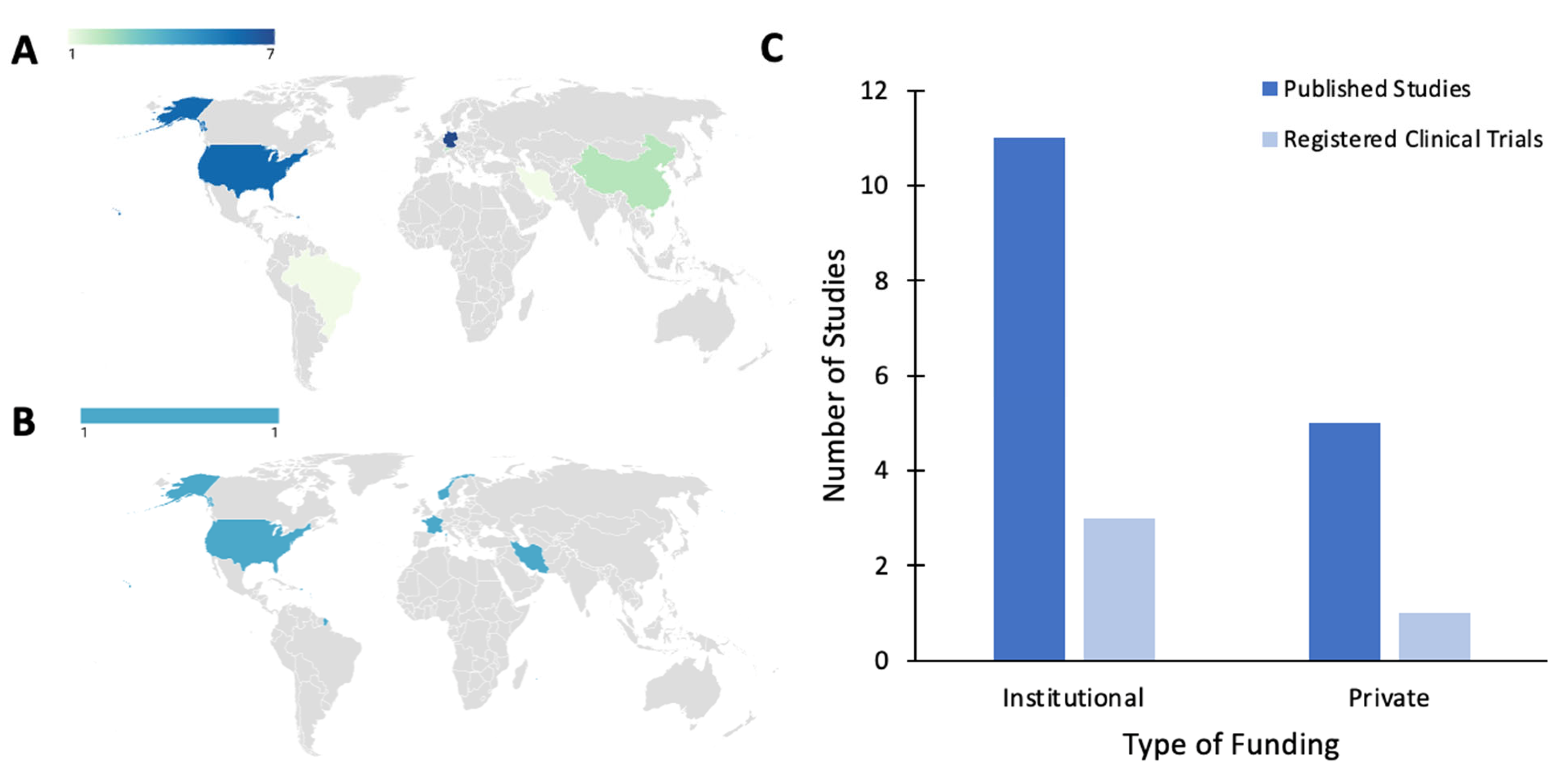
2.6. Studies by Country of Origin and Funding Source
2.7. Studies by BONT-A Treatment Parameters
2.8. Studies by Outcome Measures
2.9. Studies by Treatment Efficacy
3. Discussion
Limitations
4. Conclusions
5. Materials and Methods
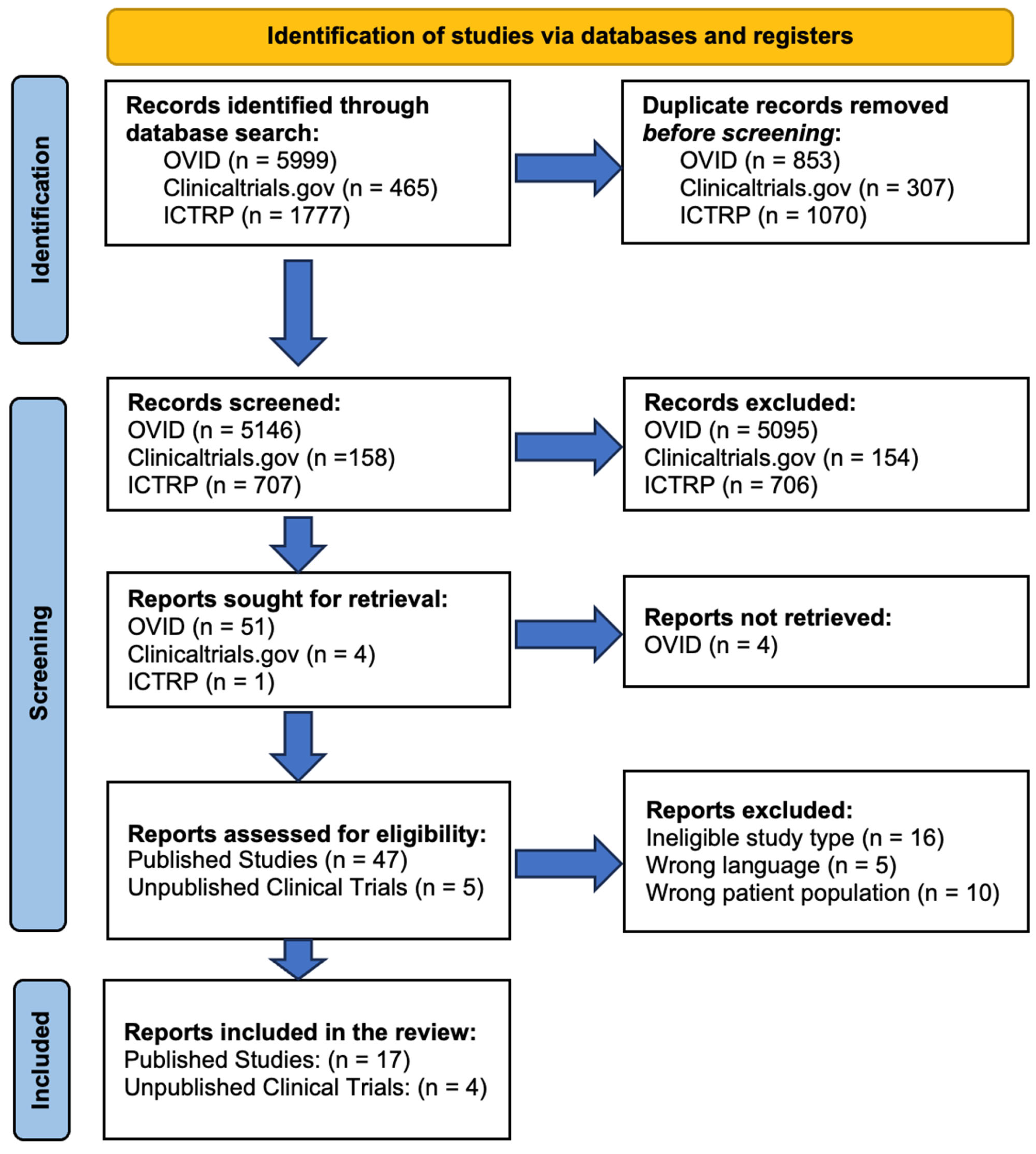
5.1. Search Strategy
5.2. Screening Process and Inclusion Criteria
5.3. Retrieval of Published Results
5.4. Variable Extraction and Synthesis
5.5. Quality Assessment
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders; DSM-5-TR; American Psychiatric Association Publishing: Washington, DC, USA, 2022; ISBN 978-0-89042-575-6. [Google Scholar]
- Escobar, J.I.; Dìaz-Martínez, A.; Gara, M. Idiopathic Physical Symptoms: A Common Manifestation of Psychiatric Disorders in Primary Care. CNS Spectr. 2006, 11, 201–210. [Google Scholar] [CrossRef]
- Trivedi, M.H. The Link between Depression and Physical Symptoms. Prim. Care Companion J. Clin. Psychiatry 2004, 6, 12–16. [Google Scholar]
- Ekman, P.; Rosenberg, E.L. What the Face Reveals: Basic and Applied Studies of Spontaneous Expression Using the Facial Action Coding System (FACS); Oxford University Press: Oxford, UK, 2005; ISBN 978-0-19-517964-4. [Google Scholar]
- Darwin, C. The Expression of the Emotions in Man and Animals; John Murray: London, UK, 1872. [Google Scholar]
- Tourangeau, R.; Ellsworth, P.C. The Role of Facial Response in the Experience of Emotion. J. Personal. Soc. Psychol. 1979, 37, 1519–1531. [Google Scholar] [CrossRef] [PubMed]
- Demchenko, I.; Desai, N.; Iwasa, S.N.; Gholamali Nezhad, F.; Zariffa, J.; Kennedy, S.H.; Rule, N.O.; Cohn, J.F.; Popovic, M.R.; Mulsant, B.H.; et al. Manipulating Facial Musculature with Functional Electrical Stimulation as an Intervention for Major Depressive Disorder: A Focused Search of Literature for a Proposal. J. Neuroeng. Rehabil. 2023, 20, 64. [Google Scholar] [CrossRef]
- Wollmer, M.A.; Magid, M.; Kruger, T.H.C.; Finzi, E. Treatment of Depression with Botulinum Toxin. Toxins 2022, 14, 383. [Google Scholar] [CrossRef] [PubMed]
- Montecucco, C.; Molgó, J. Botulinal Neurotoxins: Revival of an Old Killer. Curr. Opin. Pharmacol. 2005, 5, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.B.; Bowler, P.J. Botulinum Toxin Cosmetic Therapy Correlates with a More Positive Mood. J. Cosmet. Dermatol. 2009, 8, 24–26. [Google Scholar] [CrossRef]
- Lewis, M.B. The Interactions between Botulinum-Toxin-Based Facial Treatments and Embodied Emotions. Sci. Rep. 2018, 8, 14720. [Google Scholar] [CrossRef]
- Davis, J.I.; Senghas, A.; Brandt, F.; Ochsner, K.N. The Effects of BOTOX Injections on Emotional Experience. Emotion 2010, 10, 433–440. [Google Scholar] [CrossRef]
- Kim, M.J.; Neta, M.; Davis, F.C.; Ruberry, E.J.; Dinescu, D.; Heatherton, T.F.; Stotland, M.A.; Whalen, P.J. Botulinum Toxin-Induced Facial Muscle Paralysis Affects Amygdala Responses to the Perception of Emotional Expressions: Preliminary Findings from an A-B-A Design. Biol. Mood Anxiety Disord. 2014, 4, 11. [Google Scholar] [CrossRef]
- Hennenlotter, A.; Dresel, C.; Castrop, F.; Ceballos-Baumann, A.O.; Wohlschläger, A.M.; Haslinger, B. The Link between Facial Feedback and Neural Activity within Central Circuitries of Emotion—New Insights from Botulinum Toxin–Induced Denervation of Frown Muscles. Cereb. Cortex 2009, 19, 537–542. [Google Scholar] [CrossRef]
- Kruger, T.H.C.; Schulze, J.; Bechinie, A.; Neumann, I.; Jung, S.; Sperling, C.; Engel, J.; Müller, A.; Kneer, J.; Kahl, K.G.; et al. Neuronal Effects of Glabellar Botulinum Toxin Injections Using a Valenced Inhibition Task in Borderline Personality Disorder. Sci. Rep. 2022, 12, 14197. [Google Scholar] [CrossRef] [PubMed]
- Finzi, E.; Wasserman, E. Treatment of Depression with Botulinum Toxin A: A Case Series. Dermatol. Surg. 2006, 32, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Magid, M.; Finzi, E.; Kruger, T.; Robertson, H.; Keeling, B.; Jung, S.; Reichenberg, J.; Rosenthal, N.; Wollmer, M. Treating Depression with Botulinum Toxin: A Pooled Analysis of Randomized Controlled Trials. Pharmacopsychiatry 2015, 48, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Schulze, J.; Neumann, I.; Magid, M.; Finzi, E.; Sinke, C.; Wollmer, M.A.; Krüger, T.H.C. Botulinum Toxin for the Management of Depression: An Updated Review of the Evidence and Meta-Analysis. J. Psychiatr. Res. 2021, 135, 332–340. [Google Scholar] [CrossRef] [PubMed]
- Arnone, D.; Galadari, H.; Rodgers, C.J.; Östlundh, L.; Aziz, K.A.; Stip, E.; Young, A.H. Efficacy of onabotulinumtoxinA in the Treatment of Unipolar Major Depression: Systematic Review, Meta-Analysis and Meta-Regression Analyses of Double-Blind Randomised Controlled Trials. J. Psychopharmacol. 2021, 35, 910–918. [Google Scholar] [CrossRef] [PubMed]
- Qian, H.; Shao, F.; Lenahan, C.; Shao, A.; Li, Y. Efficacy and Safety of Botulinum Toxin vs. Placebo in Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Psychiatry 2020, 11, 603087. [Google Scholar] [CrossRef] [PubMed]
- Crowley, J.S.; Silverstein, M.L.; Reghunathan, M.; Gosman, A.A. Glabellar Botulinum Toxin Injection Improves Depression Scores: A Systematic Review and Meta-Analysis. Plast. Reconstr. Surg. 2022, 150, 211e–220e. [Google Scholar] [CrossRef] [PubMed]
- Van Aert, R.C.M.; Wicherts, J.M.; Van Assen, M.A.L.M. Publication Bias Examined in Meta-Analyses from Psychology and Medicine: A Meta-Meta-Analysis. PLoS ONE 2019, 14, e0215052. [Google Scholar] [CrossRef]
- Mitelman, S.A. Transdiagnostic Neuroimaging in Psychiatry: A Review. Psychiatry Res. 2019, 277, 23–38. [Google Scholar] [CrossRef]
- Wollmer, M.A.; Kalak, N.; Jung, S.; De Boer, C.; Magid, M.; Reichenberg, J.S.; Brand, S.; Holsboer-Trachsler, E.; Kruger, T.H.C. Agitation Predicts Response of Depression to Botulinum Toxin Treatment in a Randomized Controlled Trial. Front. Psychiatry 2014, 5, 36. [Google Scholar] [CrossRef]
- Li, Y.; Zhu, T.; Shen, T.; Wu, W.; Cao, J.; Sun, J.; Liu, J.; Zhou, X.; Jiang, C.; Tang, Z.; et al. Botulinum Toxin A (BoNT/A) for the Treatment of Depression: A Randomized, Double-Blind, Placebo, Controlled Trial in China. J. Affect. Disord. 2022, 318, 48–53. [Google Scholar] [CrossRef]
- Wollmer, M.A.; Neumann, I.; Jung, S.; Bechinie, A.; Herrmann, J.; Müller, A.; Wohlmuth, P.; Fournier-Kaiser, L.; Sperling, C.; Peters, L.; et al. Clinical Effects of Glabellar Botulinum Toxin Injections on Borderline Personality Disorder: A Randomized Controlled Trial. J. Psychopharmacol. 2022, 36, 159–169. [Google Scholar] [CrossRef]
- Wollmer, M.A.; De Boer, C.; Kalak, N.; Beck, J.; Götz, T.; Schmidt, T.; Hodzic, M.; Bayer, U.; Kollmann, T.; Kollewe, K.; et al. Facing Depression with Botulinum Toxin: A Randomized Controlled Trial. J. Psychiatr. Res. 2012, 46, 574–581. [Google Scholar] [CrossRef]
- Brin, M.F.; Durgam, S.; Lum, A.; James, L.; Liu, J.; Thase, M.E.; Szegedi, A. OnabotulinumtoxinA for the Treatment of Major Depressive Disorder: A Phase 2 Randomized, Double-Blind, Placebo-Controlled Trial in Adult Females. Int. Clin. Psychopharmacol. 2020, 35, 19–28. [Google Scholar] [CrossRef]
- Finzi, E.; Rosenthal, N.E. Treatment of Depression with onabotulinumtoxinA: A Randomized, Double-Blind, Placebo Controlled Trial. J. Psychiatr. Res. 2014, 52, 1–6. [Google Scholar] [CrossRef]
- Magid, M.; Reichenberg, J.S.; Poth, P.E.; Robertson, H.T.; LaViolette, A.K.; Kruger, T.H.C.; Wollmer, M.A. Treatment of Major Depressive Disorder Using Botulinum Toxin A: A 24-Week Randomized, Double-Blind, Placebo-Controlled Study. J. Clin. Psychiatry 2014, 75, 837–844. [Google Scholar] [CrossRef]
- Schulze, J.; Sinke, C.; Neumann, I.; Wollmer, M.A.; Kruger, T.H.C. Effects of Glabellar Botulinum Toxin Injections on Resting-State Functional Connectivity in Borderline Personality Disorder. Eur. Arch. Psychiatry Clin. Neurosci. 2024, 274, 97–107. [Google Scholar] [CrossRef]
- Zamanian, A.; Ghanbari Jolfaei, A.; Mehran, G.; Azizian, Z. Efficacy of Botox versus Placebo for Treatment of Patients with Major Depression. Iran. J. Public Health 2017, 46, 982–984. [Google Scholar]
- Zhang, Q.; Wu, W.; Fan, Y.; Li, Y.; Liu, J.; Xu, Y.; Jiang, C.; Tang, Z.; Cao, C.; Liu, T.; et al. The Safety and Efficacy of Botulinum Toxin A on the Treatment of Depression. Brain Behav. 2021, 11, e2333. [Google Scholar] [CrossRef]
- Finzi, E.; Kels, L.; Axelowitz, J.; Shaver, B.; Eberlein, C.; Krueger, T.H.; Wollmer, M.A. Botulinum Toxin Therapy of Bipolar Depression: A Case Series. J. Psychiatr. Res. 2018, 104, 55–57. [Google Scholar] [CrossRef]
- Finzi, E.; Rosenthal, N.E. Botulinum Toxin Therapy of Social Anxiety Disorder: A Case Series. J. Clin. Psychopharmacol. 2019, 39, 410–412. [Google Scholar] [CrossRef]
- Kruger, T.H.C.; Magid, M.; Wollmer, M.A. Can Botulinum Toxin Help Patients with Borderline Personality Disorder? Am. J. Psychiatry 2016, 173, 940–941. [Google Scholar] [CrossRef]
- Chugh, S.; Chhabria, A.; Jung, S.; Kruger, T.H.C.; Wollmer, M.A. Botulinum Toxin as a Treatment for Depression in a Real-World Setting. J. Psychiatr. Pract. 2018, 24, 15–20. [Google Scholar] [CrossRef]
- Hexsel, D.; Brum, C.; Siega, C.; Schilling-Souza, J.; Forno, T.D.; Heckmann, M.; Rodrigues, T.C. Evaluation of Self-Esteem and Depression Symptoms in Depressed and Nondepressed Subjects Treated with OnabotulinumtoxinA for Glabellar Lines. Dermatol. Surg. 2013, 39, 1088–1096. [Google Scholar] [CrossRef]
- Samizadeh, S.; De Boulle, K. Botulinum Neurotoxin Formulations: Overcoming the Confusion. Clin. Cosmet. Investig. Dermatol. 2018, 11, 273–287. [Google Scholar] [CrossRef]
- Stark, S.; Stark, C.; Wong, B.; Brin, M.F. Modulation of Amygdala Activity for Emotional Faces Due to Botulinum Toxin Type A Injections That Prevent Frowning. Sci. Rep. 2023, 13, 3333. [Google Scholar] [CrossRef]
- Gothard, K.M. The Amygdalo-Motor Pathways and the Control of Facial Expressions. Front. Neurosci. 2014, 8, 72097. [Google Scholar] [CrossRef]
- Finzi, E. Botulinum Toxin Treatment for Depression: A New Paradigm for Psychiatry. Toxins 2023, 15, 336. [Google Scholar] [CrossRef]
- Wyczesany, M.; Ferdek, M.A.; Grzybowski, S.J. Cortical Functional Connectivity Is Associated with the Valence of Affective States. Brain Cogn. 2014, 90, 109–115. [Google Scholar] [CrossRef]
- Güntekin, B.; Femir, B.; Gölbaşı, B.T.; Tülay, E.; Başar, E. Affective Pictures Processing Is Reflected by an Increased Long-Distance EEG Connectivity. Cogn. Neurodyn. 2017, 11, 355–367. [Google Scholar] [CrossRef]
- Takehara, H.; Ishihara, S.; Iwaki, T. Comparison between Facilitating and Suppressing Facial Emotional Expressions Using Frontal EEG Asymmetry. Front. Behav. Neurosci. 2020, 14, 554147. [Google Scholar] [CrossRef]
- Moon, S.-E.; Chen, C.-J.; Hsieh, C.-J.; Wang, J.-L.; Lee, J.-S. Emotional EEG Classification Using Connectivity Features and Convolutional Neural Networks. Neural Netw. 2020, 132, 96–107. [Google Scholar] [CrossRef]
- Zhao, X.; Chen, J.; Liu, Y.; Chen, T.; Wang, S.; Zeng, X.; Liu, G. Electrophysiological Evidence for Inhibition Hypothesis of Micro-Expressions Based on Tensor Component Analysis and Physarum Network Algorithm. Neurosci. Lett. 2022, 790, 136897. [Google Scholar] [CrossRef]
- Dimberg, U.; Söderkvist, S. The Voluntary Facial Action Technique: A Method to Test the Facial Feedback Hypothesis. J. Nonverbal. Behav. 2011, 35, 17–33. [Google Scholar] [CrossRef]
- Caputo, G.B.; Bortolomasi, M.; Ferrucci, R.; Giacopuzzi, M.; Priori, A.; Zago, S. Visual Perception during Mirror-Gazing at One’s Own Face in Patients with Depression. Sci. World J. 2014, 2014, 946851. [Google Scholar] [CrossRef]
- Coles, N.A.; March, D.S.; Marmolejo-Ramos, F.; Larsen, J.T.; Arinze, N.C.; Ndukaihe, I.L.G.; Willis, M.L.; Foroni, F.; Reggev, N.; Mokady, A.; et al. A Multi-Lab Test of the Facial Feedback Hypothesis by the Many Smiles Collaboration. Nat. Hum. Behav. 2022, 6, 1731–1742. [Google Scholar] [CrossRef]
- Fu, G.; Yu, Y.; Ye, J.; Zheng, Y.; Li, W.; Cui, N.; Wang, Q. A Method for Diagnosing Depression: Facial Expression Mimicry Is Evaluated by Facial Expression Recognition. J. Affect. Disord. 2023, 323, 809–818. [Google Scholar] [CrossRef]
- Havas, D.A.; Glenberg, A.M.; Gutowski, K.A.; Lucarelli, M.J.; Davidson, R.J. Cosmetic Use of Botulinum Toxin-A Affects Processing of Emotional Language. Psychol. Sci. 2010, 21, 895–900. [Google Scholar] [CrossRef]
- Li, Y.; Liu, T.; Luo, W. Botulinum Neurotoxin Therapy for Depression: Therapeutic Mechanisms and Future Perspective. Front. Psychiatry 2021, 12, 584416. [Google Scholar] [CrossRef]
- Demchenko, I.; Tassone, V.K.; Kennedy, S.H.; Dunlop, K.; Bhat, V. Intrinsic Connectivity Networks of Glutamate-Mediated Antidepressant Response: A Neuroimaging Review. Front. Psychiatry 2022, 13, 864902. [Google Scholar] [CrossRef]
- Li, B.-J.; Friston, K.; Mody, M.; Wang, H.-N.; Lu, H.-B.; Hu, D.-W. A Brain Network Model for Depression: From Symptom Understanding to Disease Intervention. CNS Neurosci. Ther. 2018, 24, 1004–1019. [Google Scholar] [CrossRef]
- Tang, E.; Ravaud, P.; Riveros, C.; Perrodeau, E.; Dechartres, A. Comparison of Serious Adverse Events Posted at ClinicalTrials.Gov and Published in Corresponding Journal Articles. BMC Med. 2015, 13, 189. [Google Scholar] [CrossRef]
- Ross, J.S.; Madigan, D.; Hill, K.P.; Egilman, D.S.; Wang, Y.; Krumholz, H.M. Pooled Analysis of Rofecoxib Placebo-Controlled Clinical Trial Data: Lessons for Postmarket Pharmaceutical Safety Surveillance. Arch. Intern. Med. 2009, 169, 1976–1985. [Google Scholar] [CrossRef]
- Viergever, R.F.; Karam, G.; Reis, A.; Ghersi, D. The Quality of Registration of Clinical Trials: Still a Problem. PLoS ONE 2014, 9, e84727. [Google Scholar] [CrossRef]
- Coles, N.A.; Larsen, J.T.; Kuribayashi, J.; Kuelz, A. Does Blocking Facial Feedback Via Botulinum Toxin Injections Decrease Depression? A Critical Review and Meta-Analysis. Emot. Rev. 2019, 11, 294–309. [Google Scholar] [CrossRef]
- Rudorfer, M.V. Botulinum Toxin: Does It Have a Place in the Management of Depression? CNS Drugs 2018, 32, 97–100. [Google Scholar] [CrossRef]
- Solomon, S. Botulinum Toxin for the Treatment of Chronic Migraine: The Placebo Effect. Headache 2011, 51, 980–984. [Google Scholar] [CrossRef]
- Ahmed, S.; Subramaniam, S.; Sidhu, K.; Khattab, S.; Singh, D.; Babineau, J.; Kumbhare, D.A. Effect of Local Anesthetic Versus Botulinum Toxin-A Injections for Myofascial Pain Disorders: A Systematic Review and Meta-Analysis. Clin. J. Pain 2019, 35, 353–367. [Google Scholar] [CrossRef]
- Mathew, N.T.; Frishberg, B.M.; Gawel, M.; Dimitrova, R.; Gibson, J.; Turkel, C.; BOTOX CDH Study Group. Botulinum Toxin Type A (BOTOX®) for the Prophylactic Treatment of Chronic Daily Headache: A Randomized, Double-Blind, Placebo-Controlled Trial. Headache 2005, 45, 293–307. [Google Scholar] [CrossRef]
- Brin, M.F.; Boodhoo, T.I.; Pogoda, J.M.; James, L.M.; Demos, G.; Terashima, Y.; Gu, J.; Eadie, N.; Bowen, B.L. Safety and Tolerability of onabotulinumtoxinA in the Treatment of Facial Lines: A Meta-Analysis of Individual Patient Data from Global Clinical Registration Studies in 1678 Participants. J. Am. Acad. Dermatol. 2009, 61, 961–970.e11. [Google Scholar] [CrossRef] [PubMed]
- Pantelyat, A. NCT03069911—Trial of OnabotulinumtoxinA for Depression in Parkinson Disease. Available online: https://clinicaltrials.gov/study/NCT03069911 (accessed on 2 February 2024).
- Flynn, T.C. Botox in Men: Botox in Men. Dermatol. Ther. 2007, 20, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Keaney, T.C.; Alster, T.S. Botulinum Toxin in Men: Review of Relevant Anatomy and Clinical Trial Data. Dermatol. Surg. 2013, 39, 1434–1443. [Google Scholar] [CrossRef] [PubMed]
- Charles, E.; Ranoux, D. NCT03484754—Infiltrations of OnaBotulinum Toxin A in Resistant Depression: Comparison of Two Facial Injection Sites. (OnaDEP). Available online: https://clinicaltrials.gov/study/NCT03484754?cond=NCT03484754&rank=1 (accessed on 16 May 2023).
- Alam, M.; Barrett, K.C.; Hodapp, R.M.; Arndt, K.A. Botulinum Toxin and the Facial Feedback Hypothesis: Can Looking Better Make You Feel Happier? J. Am. Acad. Dermatol. 2008, 58, 1061–1072. [Google Scholar] [CrossRef] [PubMed]
- Strawbridge, R.; Young, A.H.; Cleare, A.J. Biomarkers for Depression: Recent Insights, Current Challenges and Future Prospects. Neuropsychiatr. Dis. Treat. 2017, 13, 1245–1262. [Google Scholar] [CrossRef]
- Hacimusalar, Y.; Esel, E. Suggested Biomarkers for Major Depressive Disorder. Arch. Neuropsychiatr. 2018, 55, 280. [Google Scholar] [CrossRef] [PubMed]
- Kennis, M.; Gerritsen, L.; Van Dalen, M.; Williams, A.; Cuijpers, P.; Bockting, C. Prospective Biomarkers of Major Depressive Disorder: A Systematic Review and Meta-Analysis. Mol. Psychiatry 2020, 25, 321–338. [Google Scholar] [CrossRef]
- Kan, R.L.D.; Padberg, F.; Giron, C.G.; Lin, T.T.Z.; Zhang, B.B.B.; Brunoni, A.R.; Kranz, G.S. Effects of Repetitive Transcranial Magnetic Stimulation of the Left Dorsolateral Prefrontal Cortex on Symptom Domains in Neuropsychiatric Disorders: A Systematic Review and Cross-Diagnostic Meta-Analysis. Lancet Psychiatry 2023, 10, 252–259. [Google Scholar] [CrossRef]
- Rabin, J.S.; Giacobbe, P.; Nestor, S.M. A Transdiagnostic Approach to Transcranial Magnetic Stimulation. Lancet Psychiatry 2023, 10, 236–237. [Google Scholar] [CrossRef]
- Becker, B. Ketamine as a Potential Transdiagnostic Treatment for Anhedonia? Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2022, 7, 241–242. [Google Scholar] [CrossRef]
- Hartland, H.; Mahdavi, K.; Jelen, L.A.; Strawbridge, R.; Young, A.H.; Alexander, L. A Transdiagnostic Systematic Review and Meta-Analysis of Ketamine’s Anxiolytic Effects. J. Psychopharmacol. 2023, 37, 764–774. [Google Scholar] [CrossRef] [PubMed]
- Pansieri, C.; Pandolfini, C.; Bonati, M. Clinical Trial Registries: More International, Converging Efforts Are Needed. Trials 2017, 18, 86. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic Reviews of Effectiveness. In JBI Manual for Evidence Synthesis; JBI: Adelaide, Australia, 2020; ISBN 978-0-648-84880-6. [Google Scholar]
- Barker, T.H.; Stone, J.C.; Sears, K.; Klugar, M.; Tufanaru, C.; Leonardi-Bee, J.; Aromataris, E.; Munn, Z. The Revised JBI Critical Appraisal Tool for the Assessment of Risk of Bias for Randomized Controlled Trials. JBI Evid. Synth. 2023, 21, 494–506. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Sample Size | Allocation | Intervention Model | Masking | Drug | Site of Injection | Min Dose, U | Max Dose, U | Outcome Measures |
|---|---|---|---|---|---|---|---|---|---|---|
| Major Depressive Disorder | ||||||||||
| Finzi & Wasserman (2006) [16] | Case series | 10 | Non-randomized | Single group | Open label | n.s. | Glabellar area | 29 | 29 | BDI |
| Wollmer et al. (2012) [27] | RCT | 30 | Randomized | Parallel | Double | Onabotulinum toxin A (Allergan Inc., Irvine, CA, USA) | Glabellar area | 29 | 39 | HAM-D, BDI, CGI |
| Hexsel et al. (2013) [38] | Open label | 50 | Non-randomized | Parallel | Open label | Onabotulinum toxin A (Allergan Inc., Irvine, CA, USA) | Glabellar area | 20 | 20 | BDI, RSE |
| Finzi & Rosenthal (2014) [29] | RCT | 85 | Randomized | Parallel | Double | Onabotulinum toxin A (Allergan Inc., Irvine, CA, USA) | Glabellar area | 29 | 40 | MADRS, treatment response and remission rates, BDI, CGI |
| Magid et al. (2014) [30] | RCT | 30 | Randomized | Crossover | Double | Onabotulinum toxin A (Allergan Inc., USA) | Glabellar area | 29 | 39 | HAM-D, BDI, PHQ-9 |
| Wollmer et al. (2014) [24] | RCT | 30 | Randomized | Parallel | Double | Onabotulinum toxin A (Allergan Inc., Irvine, CA, USA) | Glabellar area | 20 | 50 | HAM-D, BDI |
| Zamanian et al. (2017) [32] | RCT | 28 | Randomized | Parallel | Double | n.s. | Glabellar area | n.s. | n.s. | BDI |
| Chugh et al. (2018) [37] | Open label | 42 | Non-randomized | Single group | Open label | Onabotulinum toxin A (Allergan Inc., Irvine, CA, USA) | Glabellar area | 29 | 39 | HAM-D, MADRS, BDI |
| Brin et al. (2020) [28] | RCT | 255 | Randomized | Parallel | Double | Onabotulinum toxin A (Allergan Inc., Irvine, CA, USA) | Glabellar area | 30 | 50 | MADRS |
| Zhang et al. (2021) [33] | RCT | 76 | Randomized | Parallel | Double | BONT-A (trade name: Hengli, Cat. No. S10970037, Lanzhou, China) | Glabellar area | 100 | 100 | HAM-D, HAMA, SDS, SAS |
| Li et al. (2022) [25] | RCT | 120 | Randomized | Parallel | Double | BONT-A (trade name: Hengli, Cat. No. S10970037, Lanzhou, China) | Glabellar area | 100 | 100 | HAM-D |
| Borderline Personality Disorder | ||||||||||
| Kruger et al. (2016) [36] | Case series | 45 | Non-randomized | Single group | Open label | n.s. | Glabellar area | 29 | 29 | ZAN-BPD, BSL-23 |
| Wollmer et al. (2022) [26] | RCT | 54 | Randomized | Parallel | Single group | Incobotulinum toxin A (Bocouture®, Merz Pharmaceuticals GmbH, Frankfurt, Germany), dissolved in 0.9% NaCl solution (100 U/2.5 mL) | Glabellar area | 34 | 34 | ZAN-BPD |
| Kruger et al. (2022) [15] | RCT | 45 | Randomized | Parallel | Single group | Incobotulinum toxin A (Bocouture®, Merz Pharmaceuticals GmbH, Frankfurt, Germany), dissolved in 0.9% NaCl solution (100 U/2.5 mL) | Glabellar area | 34 | 34 | ZAN-BPD, BSL-23 |
| Schulze et al. (2023) [31] | RCT | 45 | Randomized | n.s. | Open label | Incobotulinum toxin A (Bocouture®, Merz Pharmaceuticals GmbH, Frankfurt, Germany), dissolved in 0.9% NaCl solution (100 U/2.5 mL) | Glabellar area | 34 | 34 | ZAN-BPD, BSL-23 |
| Social Anxiety Disorder | ||||||||||
| Finzi & Rosenthal (2019) [35] | Case series | 6 | Non-randomized | Single group | Open label | n.s. | Glabellar area | 29 | 29 | LSAS |
| Bipolar Disorder | ||||||||||
| Finzi et al. (2018) [34] | Case series | 6 | Non-randomized | Single group | Open label | n.s. | Glabellar area | 29 | 46 | BDI, MADRS, QIDS-SR-16 |
| Study | Study Design | Sample Size | Outcome | Pre-Treatment Mean Score (Active Arm) | Post-Treatment Mean Score (Active Arm) | Results |
|---|---|---|---|---|---|---|
| Major Depressive Disorder | ||||||
| Finzi & Wasserman (2006) [16] | Case series | 10 | BDI-II | 30.7 | 8.1 |
|
| Wollmer et al. (2012) [27] | RCT | 30 | HAM-D | 21.4 | 11.33 |
|
| Hexsel et al. (2013) [38] | Open label | 50 | BDI | 27.4 | 12.5 |
|
| Finzi & Rosenthal (2014) [29] | RCT | 85 | MADRS | 31.6 | 16.9 |
|
| Magid et al. (2014) [30] | RCT | 30 | HAM-D | 27.9 (BONT-A at week 0) vs. 23.7 (BONT-A at week 12) | 15.2 (BONT-A at week 0) vs. 15.3 (BONT-A at week 12) |
|
| Wollmer et al. (2014) [24] | RCT | 30 | HAMD | 1.07 | 0.67 |
|
| Zamanian et al. (2017) [32] | RCT | 28 | BDI | 30.86 | 19 |
|
| Chugh et al. (2018) [37] | Open label | 42 | HAMD | 32.8 | 23.9 |
|
| Brin et al. (2020) [28] | RCT | 255 | MADRS | 32 | 17.2 |
|
| Zhang et al. (2021) [33] | RCT | 76 | HAMD | 14.04 | 4.89 |
|
| Li et al. (2022) [25] | RCT | 120 | HAMD | 12.82 | 5.78 |
|
| Borderline Personality Disorder | ||||||
| Kruger et al. (2016) [36] | Case series | 45 | ZAN-BPD | 17.67 | 4.67 |
|
| Wollmer et al. (2022) [26] | RCT | 54 | ZAN-BPD | 15.41 | n.s. |
|
| Kruger et al. (2022) [15] | RCT | 45 | ZAN-BPD | 16.04 | 10.35 |
|
| Schulze et al. (2023) [31] | RCT | 45 | ZAN-BPD | 16.04 | 10.35 |
|
| Social Anxiety Disorder | ||||||
| Finzi & Rosenthal (2019) [35] | Case series | 6 | BDI | n.s. | n.s. |
|
| Bipolar Disorder | ||||||
| Finzi et al. (2018) [34] | Case series | 6 | BDI, QIDS-SR-16, MADRS | n.s. | n.s. |
|
| Clinical Trial | Phase | Study Design | Sample Size | Allocation | Intervention Model | Masking | Drug | Site of Injection | Min Dose, U | Max Dose, U | Clinical Indication | Primary Outcomes | Secondary Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| NCT03833063 | I | RCT | 0 | Randomized | Crossover | Quadruple | n.s. | Glabellar area | n.s. | n.s. | MDD | Response (MADRS) | Remission (MADRS); GDS; QOL-AD; safety/tolerability |
| NCT03484754 | n.s. | RCT | 58 | Randomized | Parallel | Open label | Onabotulinum toxin A (Allergan Inc., Irvine, CA, USA) | Glabellar area (corrugator, procerus) vs. crow’s feet area (orbicularis oculi) | 10 | 10 | MDD | MADRS (proportion of patients with improvements in depressive symptoms) | N/A |
| NCT03078270 | n.s. | RCT | 4 | Randomized | Parallel | Double | Clostridium botulinum type A neurotoxin complex; 0.5 mg Albumin Human; 0.9 mg NaCl | n.s. | 40 | 50 | Social anxiety disorder | LSAS | BDI |
| IRCT20160523028008N7 | II–III | RCT | 70 | Randomized | Parallel | Double | n.s. | Glabellar area | 48 | 64 | Bipolar disorder | HAM-D | N/A |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Demchenko, I.; Swiderski, A.; Liu, H.; Jung, H.; Lou, W.; Bhat, V. Botulinum Toxin Injections for Psychiatric Disorders: A Systematic Review of the Clinical Trial Landscape. Toxins 2024, 16, 191. https://doi.org/10.3390/toxins16040191
Demchenko I, Swiderski A, Liu H, Jung H, Lou W, Bhat V. Botulinum Toxin Injections for Psychiatric Disorders: A Systematic Review of the Clinical Trial Landscape. Toxins. 2024; 16(4):191. https://doi.org/10.3390/toxins16040191
Chicago/Turabian StyleDemchenko, Ilya, Alyssa Swiderski, Helen Liu, Hyejung Jung, Wendy Lou, and Venkat Bhat. 2024. "Botulinum Toxin Injections for Psychiatric Disorders: A Systematic Review of the Clinical Trial Landscape" Toxins 16, no. 4: 191. https://doi.org/10.3390/toxins16040191
APA StyleDemchenko, I., Swiderski, A., Liu, H., Jung, H., Lou, W., & Bhat, V. (2024). Botulinum Toxin Injections for Psychiatric Disorders: A Systematic Review of the Clinical Trial Landscape. Toxins, 16(4), 191. https://doi.org/10.3390/toxins16040191