
Deoxynivalenol Exposure Assessment for Pregnant Women in Bangladesh

Abstract
:1. Introduction
2. Results
2.1. Validation Parameters for Biomarker Analysis

{kind=link}
| Spike Level (ng/mL) | DON | DOM-1 | ||
|---|---|---|---|---|
| Recovery (%) | RSD (%) | Recovery (%) | RSD (%) | |
| 0.5 (n = 3) | 102 | 12.2 | 88 | 8.5 |
| 1.0 (n = 3) | 90 | 8.4 | 92 | 4.8 |
| 2.0 (n = 3) | 94 | 10.4 | 78 | 4.2 |
| Spike Level (ng/mL) | DON | DOM-1 | ||||
|---|---|---|---|---|---|---|
| Mean ± SD (ng/mL) | Recovery (%) | RSD (%) | Mean ± SD (ng/mL) | Recovery (%) | RSD (%) | |
| Intra-day (1.0) n = 6 | 0.92 ± 0.12 | 92 | 13.0 | 0.82 ± 0.06 | 82 | 7.3 |
| Inter-day (1.0) n = 6 | 0.88 ± 0.08 | 88 | 9.1 | 0.80 ± 0.08 | 80 | 10.0 |
2.2. Demographic Characteristics of the Participants
| Characteristics | Rural | Suburban | Total |
|---|---|---|---|
| n | 31 | 22 | 54 |
| Age (years) | |||
| Mean ± SD | 25 ± 5 | 26 ± 5 | 25 ± 5 |
| Range | 18–36 | 18–36 | 18–36 |
| Occupation (n, %) | |||
| Housewives | 29 (91) | 16 (73) | 45 (83) |
| Office workers | 3 (9) | 6 (27) | 9 (17) |
| BMI (kg/m2) | |||
| Mean ± SD | 21.2 ± 2.3 * | 18.6 ± 3.2 | 20.1 ± 3.0 |
| Range | 14.3–28.2 | 12.0–24.4 | 12.0–28.2 |
| Creatinine (mg/L) | |||
| Mean ± SD | 652 ± 509 | 710 ± 472 | 676 ± 490 |
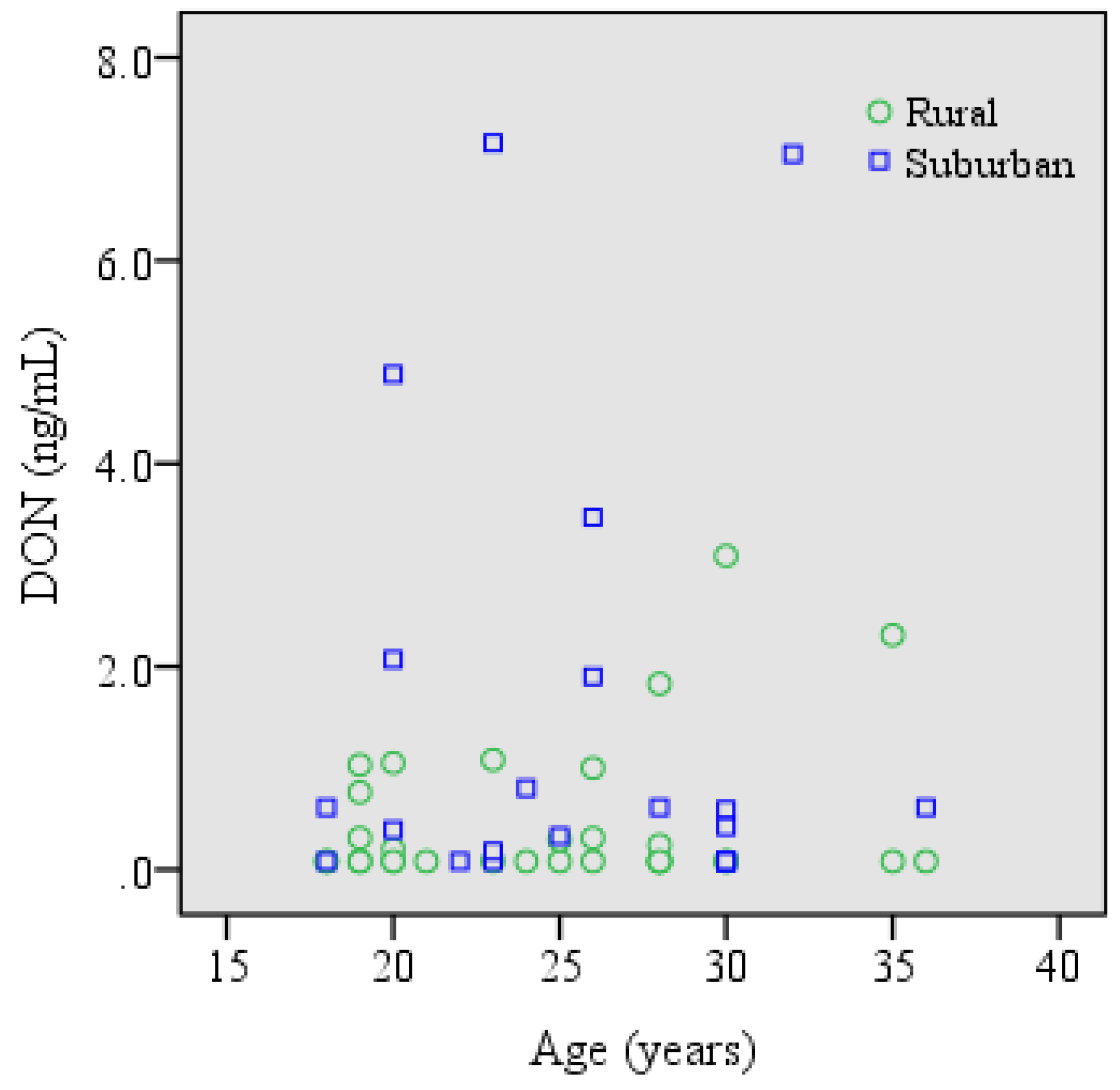
2.3. Urinary Level of DON in the Cohorts
| Cohort | n | Positive Samples n (%) | Mean ± SD (ng/mL) | Median (Range) (ng/mL) | 75th Percentile (ng/mL) | Mean ± SD (ng/mg Creatinine) |
|---|---|---|---|---|---|---|
| Rural | 32 | 13 (41) | 0.47 ± 0.73 | nd (nd–3.09) | 0.65 | 1.14 ± 2.47 |
| Suburban | 22 | 15 (68) | 1.44 ± 2.20 * | 0.51 (nd–7.16) | 1.94 | 3.60 ± 6.63 |
| Total | 54 | 28 (52) | 0.86 ± 1.57 | 0.19 (nd–7.16) | 0.85 | 2.14 ± 4.74 |

2.4. Estimation of DON Intake
| Cohort | n | Mean ± SD ng/kg b.w. | Median ng/kg b.w. | Range ng/kg b.w. | Exceeding TDI n (%) |
|---|---|---|---|---|---|
| Rural | 32 | 26.8 ± 39.0 | 5.0 | 3.1–154.0 | - |
| Suburban | 22 | 89.9 ± 133.2 * | 31.1 | 4.7–460.8 | - |
| Total | 54 | 52.5 ± 94.4 | 11.2 | 3.1–460.8 | - |
2.5. Correlation between Urinary DON and Food Intake
| Foodstuff | Correlation (r) | p-Value |
|---|---|---|
| Rice | −0.174 | 0.395 |
| Wheat/maize | 0.067 | 0.746 |
| Lentil soup | 0.182 | 0.374 |
| Chicken meat | 0.151 | 0.462 |
3. Discussion
4. Experimental Section
4.1. Standards and Reagents
4.2. Participants and Sample Collection
4.3. Enzymatic Hydrolysis
4.4. Sample Preparation
4.5. LC-MS/MS Analysis
4.6. Creatinine Analysis
4.7. Exposure Assessment
4.8. Food Consumption Data
4.9. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- WHO. WHO food additives series 47. In Proceedings of the 56th Meeting of the Joint FAO/WHO Expert Committee on Food Additives (JECFA), Geneva, Switzerland, 6–15 February 2001.
- European Food Safety Authority (EFSA). Deoxynivalenol in food and feed. EFSA J. 2013, 11, 3379. [Google Scholar] [CrossRef]
- Rotter, B.A.; Prelusky, D.B.; Pestka, J.J. Toxicology of deoxynivalenol (vomitoxin). J. Toxicol. Environ. Health 1996, 48, 1–34. [Google Scholar] [CrossRef] [PubMed]
- Pestka, J.J.; Smolinski, A.T. Deoxynivalenol: Toxicology and potential effects on humans. J. Toxicol. Environ. Health B Crit. Rev. 2005, 8, 39–69. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh, A.; Braber, S.; Akbari, P.; Garssen, J.; Fink-Gremmels, J. Deoxynivalenol impairs weight gain and affects markers of gut health after low-dose, short-term exposure of growing pigs. Toxins 2015, 7, 2071–2095. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Wu, Q.; Kuča, K.; Dohnal, V.; Tian, Z. Deoxynivalenol: Signaling pathways and human exposure risk assessment—An update. Arch. Toxicol. 2014, 88, 1915–1928. [Google Scholar] [CrossRef] [PubMed]
- Pestka, J.J. Deoxynivalenol: Mechanisms of action, human exposure, and toxicological relevance. Arch. Toxicol. 2010, 84, 663–679. [Google Scholar] [CrossRef] [PubMed]
- Maresca, M. From the gut to the brain: Journey and pathophysiological effects of the food-associated trichothecene mycotoxin deoxynivalenol. Toxins 2013, 5, 784–820. [Google Scholar] [CrossRef] [PubMed]
- Goyarts, T.; Dänicke, S.; Brussow, K.P.; Valenta, H.; Ueberschär, K.H.; Tiemann, U. On the transfer of the Fusarium toxins deoxynivalenol (DON) and zearalenone (ZON) from sows to their fetuses during days 35–70 of gestation. Toxicol. Lett. 2007, 171, 38–49. [Google Scholar] [CrossRef] [PubMed]
- Tiemann, U.; Brussow, K.P.; Dänicke, S.; Vanselow, J. Feeding of pregnant sows with mycotoxin-contaminated diets and their non-effect on foetal and maternal hepatic transcription of genes of the insulin-like growth factor system. Food Addit. Contam. Part A 2008, 25, 1365–1373. [Google Scholar] [CrossRef] [PubMed]
- Jakovac-Strajn, B.; Vengust, A.; Pestevsek, U. Effects of a deoxynivalenol contaminated diet on the reproductive performance and immunoglobulin concentrations in pigs. Vet. Rec. 2009, 165, 713–718. [Google Scholar] [PubMed]
- Nielsen, J.K.S.; Vikström, A.C.; Turner, P.C.; Knudsen, L.E. Deoxynivalenol transport across the human placental barrier. Food Chem. Toxicol. 2011, 49, 2046–2052. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; Flannery, B.; Isitt, C.; Ali, M.; Pestka, J. The role of biomarkers in evaluating human health concerns from fungal contaminants in food. Nutr. Res. Rev. 2012, 25, 162–179. [Google Scholar] [CrossRef] [PubMed]
- Warth, B.; Sulyok, M.; Berthiller, F.; Schuhmacher, R.; Krska, R. New insights into the human metabolism of the Fusarium mycotoxins deoxynivalenol and zearalenone. Toxicol. Lett. 2013, 220, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; White, K.L.; Burley, V.J.; Hopton, R.P.; Rajendram, A.; Fisher, J.; Cade, J.E.; Wild, C.P. A comparison of deoxynivalenol intake and urinary deoxynivalenol in UK adults. Biomarkers 2010, 15, 553–562. [Google Scholar] [CrossRef] [PubMed]
- Solfrizzo, M.; Gambacorta, L.; Warth, B.; White, K.; Srey, C.; Sulyok, M.; Krska, R.; Gong, Y.Y. Comparison of single and multi-analyte methods based on LC-MS/MS for mycotoxin biomarker determination in human urine. World Mycotoxin J. 2013, 6, 355–366. [Google Scholar] [CrossRef]
- Gratz, S.W.; Richardson, A.J.; Duncan, G.; Holtrop, G. Annual variation of dietary deoxynivalenol exposure during years of different Fusarium prevalence: A pilot biomonitoring study. Food Addit. Contam. Part A 2014, 31, 1579–1585. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; Hopton, R.P.; Lecluse, Y.; White, K.L.; Fisher, J.; Lebailly, P. Determinants of urinary deoxynivalenol and de-epoxy deoxynivalenol in male farmers from Normandy, France. J. Agric. Food Chem. 2010, 58, 5206–5212. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; Ji, B.T.; Shu, X.O.; Zheng, W.; Chow, W.H.; Gao, Y.T.; Hardie, L.J. A biomarker survey of urinary deoxynivalenol in China: The Shanghai Women’s Health Study. Food Addit. Contam. Part A 2011, 28, 1220–1223. [Google Scholar] [CrossRef] [PubMed]
- Turner, P.C.; Hopton, R.P.; White, K.L.; Fisher, J.; Cade, J.E.; Wild, C.P. Assessment of deoxynivalenol metabolite profiles in UK adults. Food Chem. Toxicol. 2011, 49, 132–135. [Google Scholar] [CrossRef] [PubMed]
- Hepworth, S.J.; Hardie, L.J.; Fraser, L.K.; Burley, V.J.; Mijal, R.S.; Wild, C.P.; Azad, R.; Mckinney, P.A.; Turner, P.C. Deoxynivalenol exposure assessment in a cohort of pregnant women from Bradford, UK. Food Addit. Contam. Part A 2012, 29, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Piekkola, S.; Turner, P.C.; Abdel-Hamid, M.; Ezzat, S.; El-Daly, M.; El-Kafrawy, S.; Savchenko, E.; Poussa, T.; Woo, J.C.S.; Mykkänen, H.; El-Nezami, H. Characterisation of aflatoxin and deoxynivalenol exposure among pregnant Egyptian women. Food Addit. Contam. Part A 2012, 29, 962–971. [Google Scholar] [CrossRef] [PubMed]
- Šarkanj, B.; Warth, B.; Uhlig, S.; Abia, W.A.; Sulyok, M.; Klapec, T.; Krska, R.; Banjari, I. Urinary analysis reveals high deoxynivalenol exposure in pregnant women from Croatia. Food Chem. Toxicol. 2013, 62, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Warth, B.; Petchkongkaew, A.; Sulyok, M.; Krska, R. Utilising an LCMS/ MS-based multi-biomarker approach to assess mycotoxin exposure in the Bangkok metropolitan area and surrounding provinces. Food Addit. Contam. Part A 2014, 12, 2040–2046. [Google Scholar] [CrossRef] [PubMed]
- Warth, B.; Sulyok, M.; Fruhmann, P.; Berthiller, F.; Schuhmacher, R.; Hametner, C.; Adam, G.; Fröhlich, J.; Krska, R. Assessment of human deoxynivalenol exposure using an LC-MS/MS based biomarker method. Toxicol. Lett. 2012, 211, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Wallin, S.; Hardie, L.J.; Kotova, N.; Warensjö Lemming, E.; Nälsén, C.; Ridefelt, P.; Turner, P.C.; White, K.L.M.; Olsen, M. Biomonitoring study of deoxynivalenol exposure and association with typical cereal consumption in Swedish adults. World Mycotoxin J. 2013, 6, 439–448. [Google Scholar] [CrossRef]
- Solfrizzo, M.; Gambacorta, L.; Visconti, A. Assessment of multi-mycotoxin exposure in southern Italy by urinary multi-biomarker determination. Toxins 2014, 6, 523–538. [Google Scholar] [CrossRef] [PubMed]
- Huybrechts, B.; Debongnie, P.; Uhlig, S.; Callebaut, A. Fast and sensitive LC-MS/MS method measuring human mycotoxin exposure using biomarkers in urine. Arch. Toxicol. 2014. [Google Scholar] [CrossRef] [PubMed]
- Gerding, J.; Cramer, B.; Humpf, H.U. Determination of mycotoxin exposure in Germany using an LC-MS/MS multibiomarker approach. Mol. Nutr. Food Res. 2014, 58, 2358–2368. [Google Scholar] [CrossRef] [PubMed]
- Gerding, J.; Ali, N.; Schwartzbord, J.; Cramer, B.; Brown, D.L.; Degen, G.H.; Humpf, H.U. A comparative study of the human urinary mycotoxin excretion patterns in Bangladesh, Germany and Haiti using a rapid and sensitive LC-MS/MS approach. Mycotoxin Res. 2015, 31, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Ezekiel, C.; Warth, B.; Ogara, I.M.; Abia, W.; Ezekiel, V.C.; Sulyok, M.; Turner, P.C.; Krska, R.; Tayo, G. Exposure to mycotoxins in rural residents in northern Nigeria: A pilot, multi-urinary biomarker study. Environ. Int. 2014, 66, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Shephard, G.S.; Burger, H.M.; Gambacorta, L.; Gong, Y.Y.; Krska, R.; Rheeder, J.P.; Solfrizzo, M.; Srey, C.; Sulyok, M.; Visconti, A.; et al. Multiple mycotoxin exposure determined by urinary biomarkers in rural subsistence farmers in the former Transkei, South Africa. Food Chem. Toxicol. 2013, 62, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Degen, G.H. Tools for investigating workplace related risks from mycotoxin exposure. World Mycotoxin J. 2011, 4, 315–327. [Google Scholar] [CrossRef]
- Dawlatana, M.; Coker, R.D.; Nagler, M.J.; Wild, C.P.; Hassan, M.S.; Blunden, G. The occurrence of mycotoxins in key commodities in Bangladesh: Surveillance results from 1993 to 1995. J. Nat. Toxins 2002, 11, 379–386. [Google Scholar] [PubMed]
- Wallin, S.; Gambacorta, L.; Kotova, N.; Warensjo Lemming, E.; Nalsen, C.; Solfrizzo, M.; Olsen, M. Biomonitoring of of concurrent mycotoxin exposure among adults in Sweden through urinary multi-biomarker analysis. Food Chem. Toxicol. 2015, 83, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Heyndrickx, E.; Sioen, I.; Huybrechts, B.; Callebaut, A.; De Henauw, S.; de Saeger, S. Human biomonitoring of multiple mycotoxins in the Belgian population: Results of the BIOMYCO study. Environ. Int. 2015, 84, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Murphy, P.; Cunnick, J.; Hendrich, S. Synthesis and characterization of deoxynivalenol glucuronide: Its comparative immunotoxicity with deoxynivalenol. Food Chem. Toxicol. 2007, 45, 1846–1855. [Google Scholar] [CrossRef] [PubMed]
- Doohan, F.M.; Brennan, J.; Cooke, B.M. Influence of climatic factors on Fusarium species pathogenic to cereals. Eur. J. Plant Pathol. 2003, 109, 755–768. [Google Scholar] [CrossRef]
- Ali, N.; Blaszkewicz, M.; Mohanto, N.C.; Rahman, M.; Alim, A.; Hossain, K.; Degen, G.H. First results on analysis of citrinin biomarkers in urines from two cohorts in Bangladesh. Mycotoxin Res. 2015, 31, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Blaszkewicz, M.; Liesenhoff-Henze, K. Creatinine in Urine. In The MAK Collection for Occupational Health and Safety; Part IV, Biomonitoring Methods, Vol 12; Wiley-VCH Verlag: Weinheim, Germany, 2010; pp. 169–184. [Google Scholar] [CrossRef]
- Mikhail, M.S.; Anyaegbunam, A. Lower urinary tract dysfunction in pregnancy: A review. Obstet. Gynecol. Surv. 1995, 50, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Carrasco, Y.; Mañes, J.; Berrada, H.; Font, G. Preliminary estimation of deoxynivalenol excretion through a 24 h pilot study. Toxins 2015, 7, 705–718. [Google Scholar] [CrossRef] [PubMed]
- Hornung, R.W.; Reed, L.D. Estimation of average concentration in the presence of nondetectable values. Appl. Occup. Environ. Hyg. 1990, 5, 46–51. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ali, N.; Blaszkewicz, M.; Al Nahid, A.; Rahman, M.; Degen, G.H. Deoxynivalenol Exposure Assessment for Pregnant Women in Bangladesh. Toxins 2015, 7, 3845-3857. https://doi.org/10.3390/toxins7103845
Ali N, Blaszkewicz M, Al Nahid A, Rahman M, Degen GH. Deoxynivalenol Exposure Assessment for Pregnant Women in Bangladesh. Toxins. 2015; 7(10):3845-3857. https://doi.org/10.3390/toxins7103845
Chicago/Turabian StyleAli, Nurshad, Meinolf Blaszkewicz, Abdullah Al Nahid, Mustafizur Rahman, and Gisela H. Degen. 2015. "Deoxynivalenol Exposure Assessment for Pregnant Women in Bangladesh" Toxins 7, no. 10: 3845-3857. https://doi.org/10.3390/toxins7103845
APA StyleAli, N., Blaszkewicz, M., Al Nahid, A., Rahman, M., & Degen, G. H. (2015). Deoxynivalenol Exposure Assessment for Pregnant Women in Bangladesh. Toxins, 7(10), 3845-3857. https://doi.org/10.3390/toxins7103845