
New Era of Electroceuticals: Clinically Driven Smart Implantable Electronic Devices Moving towards Precision Therapy



Abstract
:1. Introduction
2. Needs for Next-Generation Electroceuticals: Intelligent Biomedical Implants
3. Smart Implants Development Challenges
4. Electroceuticals—Intelligent Environments
4.1. Pacemaker
4.2. Neural Stimulations and Electrode Arrays
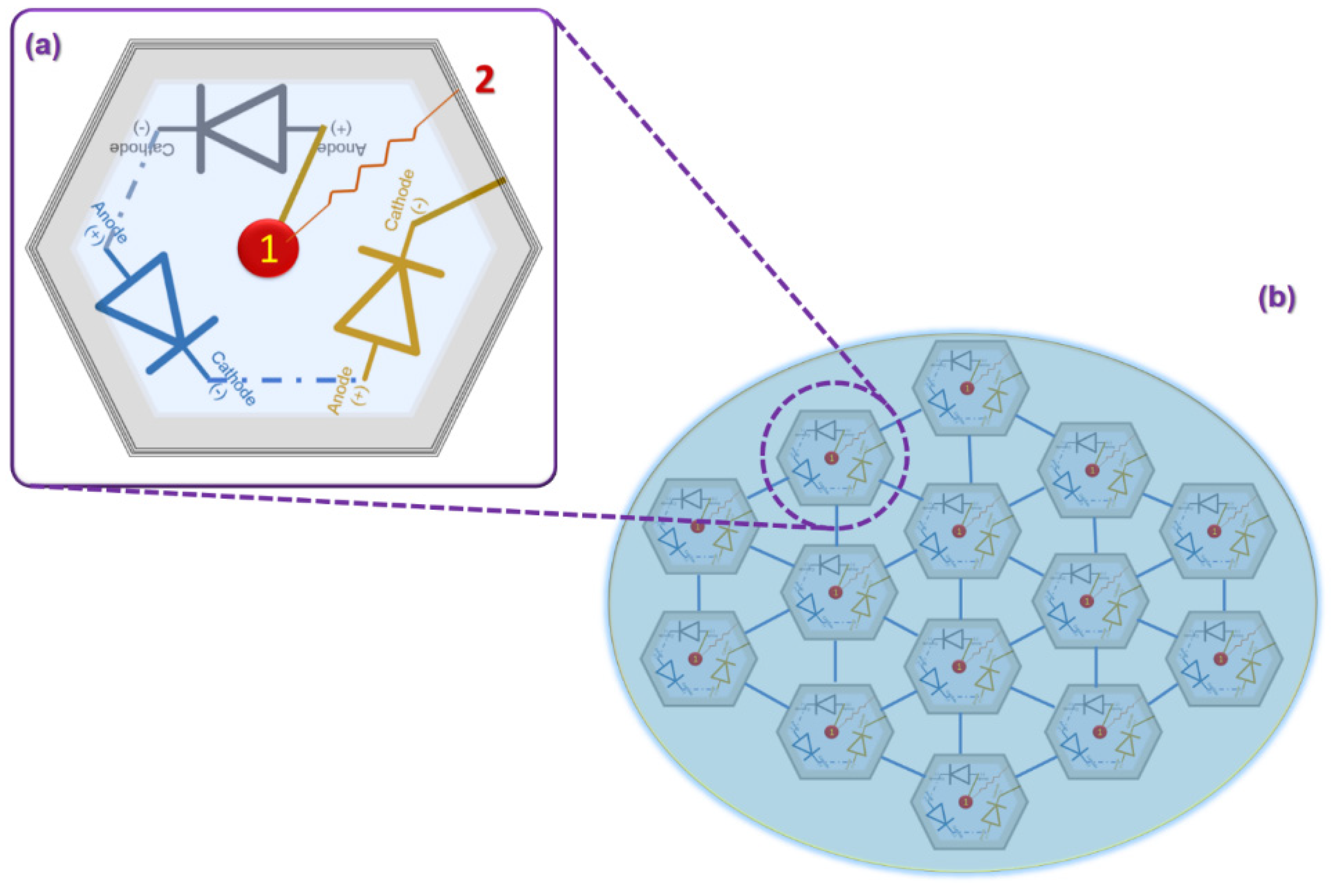
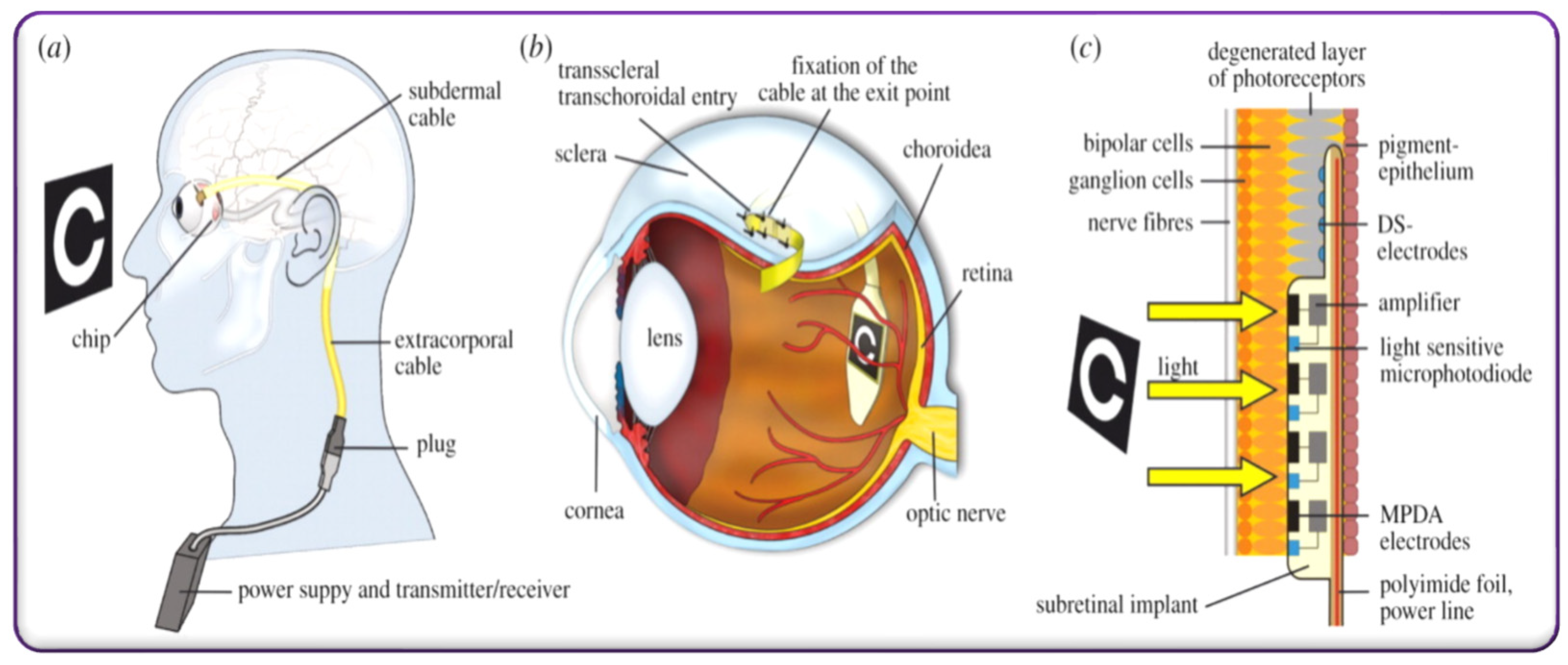
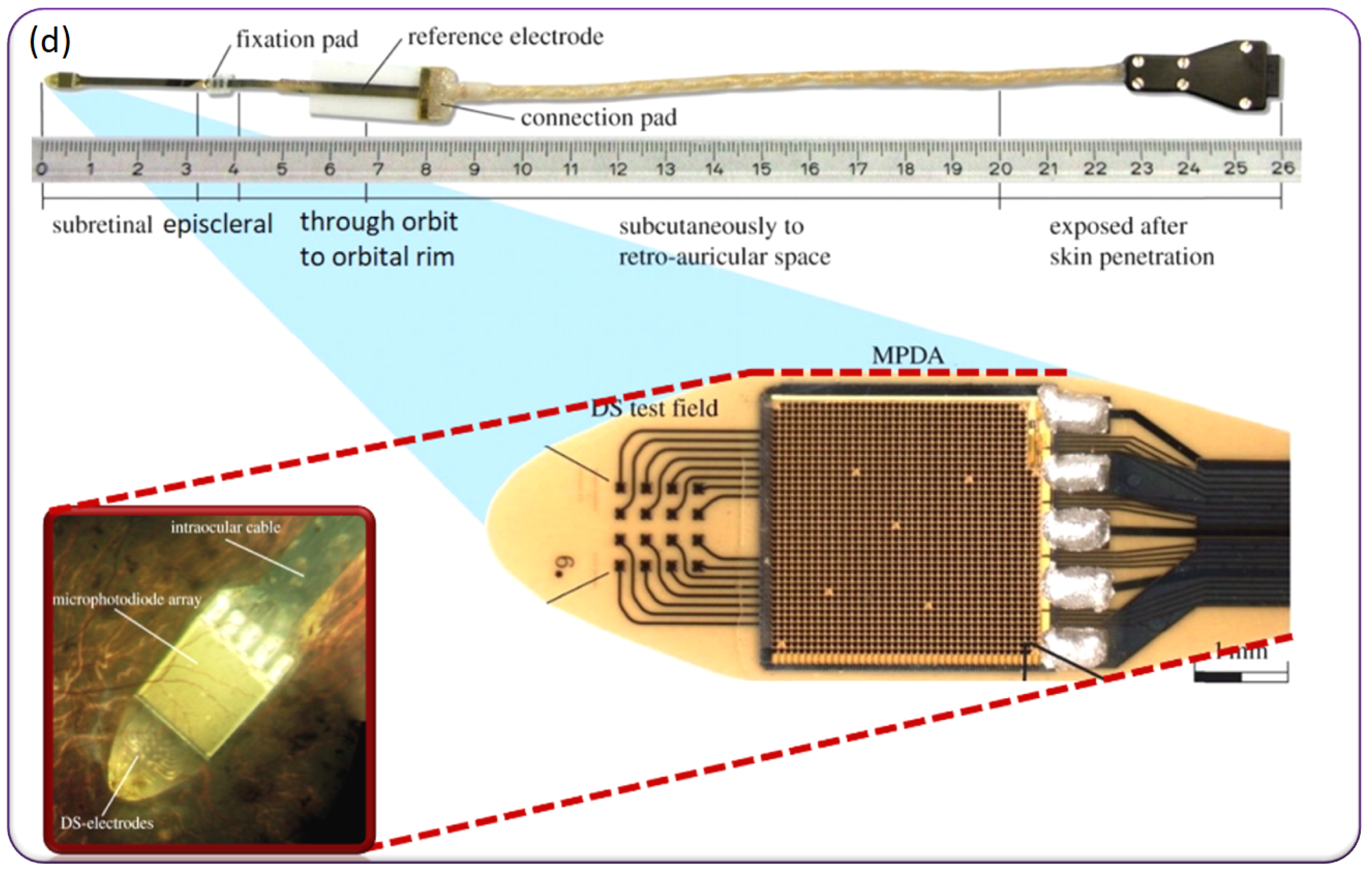
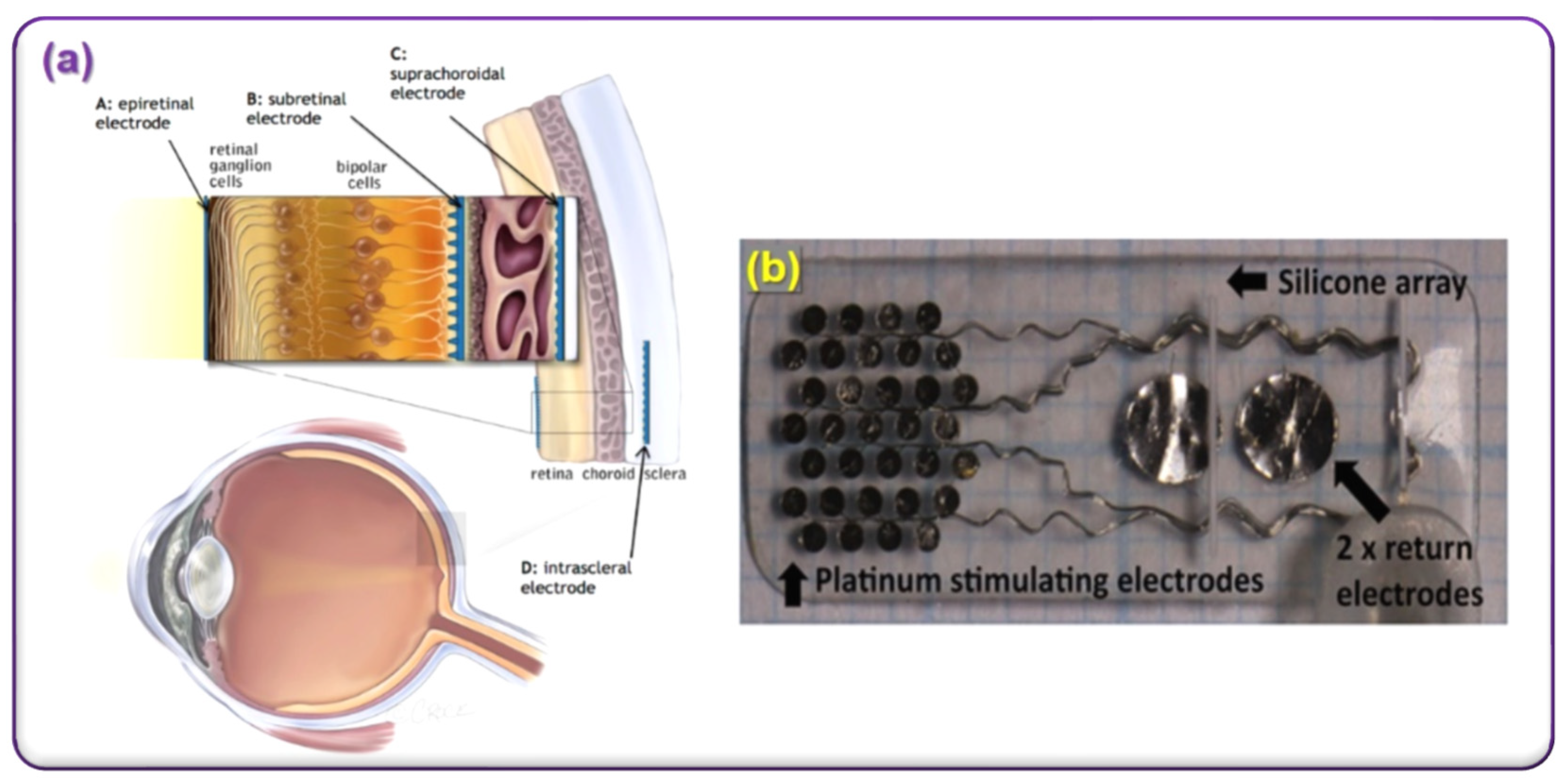
4.3. Artificial Retina
4.4. Vagus Nerve Stimulation
5. Safe Packaging against Electromagnetic Interference
6. Conclusions
Funding
Conflicts of Interest
References
- Avula, M.N.; Grainger, D.W. Addressing Medical Device Challenges with Drug-Device Combinations. In Drug-Device Combinations for Chronic Diseases; Lyu, S., Siegel, R.A., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2015. [Google Scholar]
- Sumant, U.; Rupali, S. Biomedical Warming and Thawing Devices Market; Global Market Insights: Selbyville, DE, USA, 2021; p. 140. [Google Scholar]
- Biomedical Warming and Thawing Devices Market Size, Statistics Report, 2027. In Medical Device Manufacturing in India–A Sunrise; Department of Industrial Policy and Promotion, Department of Pharmaceuticals; World Health Organization Country Office for India: Delhi, India, 2017; p. 45.
- Shmulewitz, A.; Langer, R.; Patton, J. Convergence in biomedical technology. Nat. Biotechnol. 2006, 24, 277. [Google Scholar] [CrossRef] [PubMed]
- Graudejus, O.; Yu, Z.; Jones, J.; Morrison, B., III; Wagner, S. Characterization of an elastically stretchable microelectrode array and its application to neural field potential recordings. J. Electrochem. Soc. 2009, 156, P85. [Google Scholar] [CrossRef]
- Prox, J.; Seicol, B.; Qi, H.; Argall, A.; Araya, N.; Behnke, N.; Guo, L. Toward living neuroprosthetics: Developing a biological brain pacemaker as a living neuromodulatory implant for improving parkinsonian symptoms. J. Neural Eng. 2021, 18, 046081. [Google Scholar] [CrossRef] [PubMed]
- Gabriels, J.; Chang, D.; Maytin, M.; Tadros, T.; John, R.M.; Sobieszczyk, P.; Eisenhauer, A.; Epstein, L.M. Percutaneous management of superior vena cava syndrome in patients with cardiovascular implantable electronic devices. Heart Rhythm. 2021, 18, 392–398. [Google Scholar] [CrossRef]
- Zheng, Q.; Tang, Q.; Wang, Z.L.; Li, Z. Self-powered cardiovascular electronic devices and systems. Nat. Rev. Cardiol. 2021, 18, 7–21. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, D. Retinal prostheses: Progress toward the next generation implants. Front. Neurosci. 2015, 9, 290. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.W.; Seo, J.M.; Ha, S.; Kim, E.T.; Chung, H.; Kim, S.J. Development of microelectrode arrays for artificial retinal implants using liquid crystal polymers. Investig. Ophthalmol. Vis. Sci. 2009, 50, 5859–5866. [Google Scholar] [CrossRef] [PubMed]
- Zhou, D.D.; Greenberg, R.J. Microsensors and microbiosensors for retinal implants. Front. Biosci. 2005, 10, 166–179. [Google Scholar] [CrossRef] [Green Version]
- Ben-Menachem, E. Vagus-nerve stimulation for the treatment of epilepsy. Lancet Neurol. 2002, 1, 477–482. [Google Scholar] [CrossRef]
- Kavakbasi, E.; Gross, J.; Wollbrink, A.; Fellmeth, R.; Baune, B.T. Acute effect of vagus nerve stimulation (VNS) on brain function. J. Psychiatr. Res. 2021, 141, 136–139. [Google Scholar] [CrossRef]
- Pruitt, D.T.; Danaphongse, T.T.; Lutchman, M.; Patel, N.; Reddy, P.; Wang, V.; Parashar, A.; Rennaker, R.L.; Kilgard, M.P.; Hays, S.A. Optimizing dosing of vagus nerve stimulation for stroke recovery. Transl. Stroke Res. 2021, 12, 65–71. [Google Scholar] [CrossRef]
- Cingolani, E.; Goldhaber, J.I.; Marbán, E. Next-generation pacemakers: From small devices to biological pacemakers. Nat. Rev. Cardiol. 2018, 15, 139–150. [Google Scholar] [CrossRef]
- Ritaccio, A.L.; Brunner, P.; Schalk, G. Electrical stimulation mapping of the brain: Basic principles and emerging alternatives. J. Clin. Neurophysiol. Off. Publ. Am. Electroencephalogr. Soc. 2018, 35, 86. [Google Scholar] [CrossRef] [PubMed]
- Englot, D.J.; Yang, L.; Hamid, H.; Danielson, N.; Bai, X.; Marfeo, A.; Yu, L.; Gordon, A.; Purcaro, M.J.; Motelow, J.E.; et al. Impaired consciousness in temporal lobe seizures: Role of cortical slow activity. Brain 2010, 133, 3764–3777. [Google Scholar] [CrossRef] [Green Version]
- Grunwald, T.; Boutros, N.N.; Pezer, N.; von Oertzen, J.; Fernández, G.; Schaller, C.; Elger, C.E. Neuronal substrates of sensory gating within the human brain. Biol. Psychiatry 2003, 53, 511–519. [Google Scholar] [CrossRef]
- Mathieson, K.; Loudin, J.; Goetz, G.; Huie, P.; Wang, L.; Kamins, T.I.; Galambos, L.; Smith, R.; Harris, J.S.; Sher, A.; et al. Photovoltaic retinal prosthesis with high pixel density. Nat. Photonics 2012, 6, 391–397. [Google Scholar] [CrossRef] [PubMed]
- Suaning, G.J.; Lovell, N.H. CMOS neurostimulation ASIC with 100 channels, scaleable output, and bidirectional radio-frequency telemetry. IEEE Trans. Biomed. Eng. 2001, 48, 248–260. [Google Scholar] [CrossRef]
- Liu, W.; Vichienchom, K.; Clements, M.; DeMarco, S.C.; Hughes, C.; McGucken, E.; Humayun, M.S.; De Juan, E.; Weiland, J.D.; Greenberg, R. A neuro-stimulus chip with telemetry unit for retinal prosthetic device. IEEE J. Solid-State Circ. 2000, 35, 1487–1497. [Google Scholar] [CrossRef]
- Akin, T.; Najafi, K.; Bradley, R.M. A wireless implantable multichannel digital neural recording system for a micromachined sieve electrode. IEEE J. Solid-State Circ. 1998, 33, 109–118. [Google Scholar] [CrossRef] [Green Version]
- Huang, Q.; Oberle, M. A 0.5-mW passive telemetry IC for biomedical applications. IEEE J. Solid-State Circ. 1998, 33, 937–946. [Google Scholar] [CrossRef]
- Lindsey, D.P.; McKee, E.L.; Hull, M.L.; Howell, S.M. A new technique for transmission of signals from implantable transducers. IEEE Trans. Biomed. Eng. 1998, 45, 614–619. [Google Scholar] [CrossRef]
- Ghovanloo, M.; Najafi, K. A high data transfer rate frequency shift keying demodulator chip for the wireless biomedical implants. In Proceedings of the 2002 45th Midwest Symposium on Circuits and Systems, Tulsa, OK, USA, 4–7 August 2002; Volume 3, p. 3. [Google Scholar]
- Parramon, J.; Doguet, P.; Marin, D.; Verleyssen, M.; Munoz, R.; Leija, L.; alderrama, E. ASIC-based batteryless implantable telemetry microsystem for recording purposes. In Proceedings of the 19th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Magnificent Milestones and Emerging Opportunities in Medical Engineering, Chicago, IL, USA, 30 October–2 November 1997; Volume 5, pp. 2225–2228. [Google Scholar]
- Gudnason, G.; Bruun, E.; Haugland, M. A chip for an implantable neural stimulator. Analog. Integr. Circ. Signal Processing 2000, 22, 81–89. [Google Scholar] [CrossRef]
- Smith, B.; Tang, Z.; Johnson, M.W.; Pourmehdi, S.; Gazdik, M.M.; Buckett, J.R.; Peckham, P.H. An externally powered, multichannel, implantable stimulator-telemeter for control of paralyzed muscle. IEEE Trans. Biomed. Eng. 1998, 45, 463–475. [Google Scholar] [CrossRef] [PubMed]
- Trigui, A.; Mehri, S.; Ammari, A.; Slama, J.B.H.; Sawan, M. Prosthetic power supplies. Wiley Encycl. Electr. Electron. Eng. 1999, 1–12. [Google Scholar] [CrossRef]
- Zikria, J.F.; Machnicki, S.; Rhim, E.; Bhatti, T.; Graham, R.E. MRI of patients with cardiac pacemakers: A review of the medical literature. Am. J. Roentgenol. 2011, 196, 390–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- International IEC standards: Medical Electrical Equipment; General Requirements for Safety; Electromagnetic Compatibility Requirements and Tests. IEC-60601-1-2. Available online: https://www.sis.se/api/document/preview/566963/ (accessed on 15 January 2022).
- Driessen, S.; Napp, A.; Schmiedchen, K.; Kraus, T.; Stunder, D. Electromagnetic interference in cardiac electronic implants caused by novel electrical appliances emitting electromagnetic fields in the intermediate frequency range: A systematic review. Ep Eur. 2019, 21, 219–229. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Environmental Health Criteria Monograph no. 232-Static Fields; WHO: Geneva, Switzerland, 2006; Available online: http://www.who.int/peh-emf/publications/EHC_232_Static_Fields_full_document.pdf (accessed on 12 December 2016).
- A Practical Guide to IEC 60601. Available online: https://www.rigelmedical.com/gb/downloads/Rigel-Medical-A-Practical-guide-to-IEC-60601-1.pdf (accessed on 12 November 2020).
- Kim, J.; Kim, H.; Kim, D.; Park, H.J.; Ban, K.; Ahn, S.; Park, S.M. A wireless power transfer based implantable ECG monitoring device. Energies 2020, 13, 905. [Google Scholar] [CrossRef] [Green Version]
- Hannan, M.A.; Mutashar, S.; Samad, S.A.; Hussain, A. Energy harvesting for the implantable biomedical devices: Issues and challenges. Biomed. Eng. Online 2014, 13, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skrivervik, A.K. Implantable antennas: The challenge of efficiency. In Proceedings of the 2013 7th European Conference on Antennas and Propagation, Gothenburg, Sweden, 8–12 April 2013; pp. 3627–3631. [Google Scholar]
- Turok, D.K.; Gero, A.; Simmons, R.G.; Kaiser, J.E.; Stoddard, G.J.; Sexsmith, C.D.; Gawron, L.M.; Sanders, J.N. Levonorgestrel vs. copper intrauterine devices for emergency contraception. N. Engl. J. Med. 2021, 384, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Jang, S.G.; Lim, H.G.; Kim, H.H.; Park, S.M. Acoustic Power Transfer Using Self-Focused Transducers for Miniaturized Implantable Neurostimulators. IEEE Access 2021, 9, 153850–153862. [Google Scholar] [CrossRef]
- Nathan, M. Microbattery technologies for miniaturized implantable medical devices. Curr. Pharm. Biotechnol. 2010, 11, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Dinis, H.; Mendes, P.M. A comprehensive review of powering methods used in state-of-the-art miniaturized implantable electronic devices. Biosens. Bioelectron. 2021, 172, 112781. [Google Scholar] [CrossRef]
- Akinin, A.; Ford, J.M.; Wu, J.; Kim, C.; Thacker, H.D.; Mercier, P.P.; Cauwenberghs, G. An Optically Addressed Nanowire-Based Retinal Prosthesis with Wireless Stimulation Waveform Control and Charge Telemetering. IEEE J. Solid-State Circ. 2021, 56, 3263–3273. [Google Scholar] [CrossRef]
- Ghafari, B. Practical Limits and Challenges for Powering of Wireless Systems in Implantable and Lab on a Chip Biomedical Devices and Review of the Low Power Design Techniques. In Proceedings of the 2021 IEEE International IOT, Electronics and Mechatronics Conference, Toronto, ON, Canada, 21–24 April 2021; pp. 1–9. [Google Scholar]
- Dai, Y.; Hu, H.; Wang, M.; Xu, J.; Wang, S. Stretchable transistors and functional circuits for human-integrated electronics. Nat. Electron. 2021, 4, 17–29. [Google Scholar] [CrossRef]
- Xu, Q.; Lv, Y.; Dong, C.; Sreeprased, T.S.; Tian, A.; Zhang, H.; Tang, Y.; Yu, Z.; Li, N. Three-dimensional micro/nanoscale architectures: Fabrication and applications. Nanoscale 2015, 7, 10883–10895. [Google Scholar] [CrossRef]
- Someya, T.; Amagai, M. Toward a new generation of smart skins. Nat. Biotechnol. 2019, 37, 382–388. [Google Scholar] [CrossRef]
- Magisetty, R.; Prajapati, D.; Ambekar, R.; Shukla, A.; Kandasubramanian, B. β-Phase Cu-phthalocyanine/acrylonitrile butadiene styrene terpolymer nanocomposite film technology for organoelectronic applications. J. Phys. Chem. C 2019, 123, 28081–28092. [Google Scholar] [CrossRef]
- Liu, Z.; Li, H.; Shi, B.; Fan, Y.; Wang, Z.L.; Li, Z. Wearable and implantable triboelectric nanogenerators. Adv. Funct. Mater. 2019, 29, 1808820. [Google Scholar] [CrossRef]
- Wang, L.; Jiang, K.; Shen, G. Wearable, Implantable, and Interventional Medical Devices Based on Smart Electronic Skins. Adv. Mater. Technol. 2021, 6, 100107. [Google Scholar] [CrossRef]
- Lee, J.; Park, E.; Kang, W.; Kim, Y.; Lee, K.S.; Park, S.M. An efficient noninvasive neuromodulation modality for overactive bladder using time interfering current method. IEEE Trans. Biomed. Eng. 2020, 68, 214–224. [Google Scholar] [CrossRef]
- Kang, W.; Lee, J.; Kim, Y.R.; Chung, W.R.; Na, D.L.; Shon, Y.M.; Park, S.M. Analyzing the advantages of subcutaneous over transcutaneous electrical stimulation for activating brainwaves. Sci. Rep. 2020, 10, 1–14. [Google Scholar] [CrossRef]
- Kadish, A.; Mehra, M. Heart failure devices: Implantable cardioverter-defibrillators and biventricular pacing therapy. Circulation 2005, 111, 3327–3335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Germano, J.J.; Reynolds, M.; Essebag, V.; Josephson, M.E. Frequency and causes of implantable cardioverter-defibrillator therapies: Is device therapy proarrhythmic? Am. J. Cardiol. 2006, 97, 1255–1261. [Google Scholar] [CrossRef]
- Ashraf, M.; Masoumi, N. A thermal energy harvesting power supply with an internal startup circuit for pacemakers. IEEE Trans. Very Large Scale Integr. Syst. 2015, 24, 26–37. [Google Scholar] [CrossRef]
- Haeberlin, A.; Zurbuchen, A.; Walpen, S.; Schaerer, J.; Niederhauser, T.; Huber, C.; Tanner, H.; Servatius, H.; Seiler, J.; Haeberlin, H.; et al. The first batteryless, solar-powered cardiac pacemaker. Heart Rhythm. 2015, 12, 1317–1323. [Google Scholar] [CrossRef] [Green Version]
- Rufer, L.; Colin, M.; Basrour, S. Application driven design, fabrication and characterization of piezoelectric energy scavenger for cardiac pacemakers. In Proceedings of the 2013 joint IEEE International Symposium on Applications of Ferroelectric and Workshop on Piezoresponse Force Microscopy, Prague, Czech Republic, 21–25 July 2013; pp. 340–343. [Google Scholar]
- Ryu, H.; Park, H.M.; Kim, M.K.; Kim, B.; Myoung, H.S.; Kim, T.Y.; Yoon, H.J.; Kwak, S.S.; Kim, J.; Hwang, T.H.; et al. Self-rechargeable cardiac pacemaker system with triboelectric nanogenerators. Nat. Commun. 2021, 12, 1–9. [Google Scholar] [CrossRef]
- Azimi, S.; Golabchi, A.; Nekookar, A.; Rabbani, S.; Amiri, M.H.; Asadi, K.; Abolhasani, M.M. Self-powered cardiac pacemaker by piezoelectric polymer nanogenerator implant. Nano Energy 2021, 83, 105781. [Google Scholar] [CrossRef]
- Kim, D.; Jeong, D.; Kim, J.; Kim, H.; Kim, J.; Park, S.M.; Ahn, S. Design and implementation of a wireless charging-based cardiac monitoring system focused on temperature reduction and robust power transfer efficiency. Energies 2020, 13, 1008. [Google Scholar] [CrossRef] [Green Version]
- Abiri, P.; Duarte-Vogel, S.; Chou, T.C.; Abiri, A.; Gudapati, V.; Yousefi, A.; Roustaei, M.; Chang, C.C.; Cui, Q.; Hsu, J.J.; et al. In Vivo Intravascular Pacing Using a Wireless Microscale Stimulator. Ann. Biomed. Eng. 2021, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Khalili, H.F.; Kirchner, J.; Bartunik, M.; Werner, S.; Ebel, N.; Schubert, D.W.; Weyand, M.; Fischer, G. Transcutaneous Energy Transfer System for Cardiac-Assist Devices by Use of Inhomogeneous Biocompatible Core Material. IEEE Trans. Magn. 2021, 57, 5200412. [Google Scholar] [CrossRef]
- Mohanarangam, K.; Palagani, Y.; Cho, K.H.; Choi, J.R. Inductive Power Transfer Link at 13.56 MHz for Leadless Cardiac Pacemakers. Energies 2021, 14, 5436. [Google Scholar] [CrossRef]
- Liu, Y.; Zhou, H.; Zhou, W.; Meng, S.; Qi, C.; Liu, Z.; Kong, T. Biocompatible, high-performance, wet-adhesive, stretchable all-hydrogel supercapacitor implant based on PANI@ rGO/mxenes electrode and hydrogel electrolyte. Adv. Energy Mater. 2021, 11, 2101329. [Google Scholar] [CrossRef]
- Al-Dulimi, Z.; Wallis, M.; Tan, D.K.; Maniruzzaman, M.; Nokhodchi, A. 3D printing technology as innovative solutions for biomedical applications. Drug Discov. Today 2020, 26, 360–383. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Zhang, Y.; Itoh, T.; Maeda, R. Flexible implantable microtemperature sensor fabricated on polymer capillary by programmable UV lithography with multilayer alignment for biomedical applications. J. Microelectromechanical Syst. 2013, 23, 21–29. [Google Scholar] [CrossRef]
- Koydemir, H.C.; Ozcan, A. Wearable and implantable sensors for biomedical applications. Annu. Rev. Anal. Chem. 2018, 11, 127–146. [Google Scholar] [CrossRef] [PubMed]
- Hoare, D.; Bussooa, A.; Neale, S.; Mirzai, N.; Mercer, J. The future of cardiovascular stents: Bioresorbable and integrated biosensor technology. Adv. Sci. 2019, 6, 1900856. [Google Scholar] [CrossRef] [Green Version]
- Talha, M. A history of development in brain chips in present and future. Int. J. Psychosoc. Rehabil. 2020, 24, 7244–7250. [Google Scholar]
- Lee, Y.; Lee, T.W. Organic synapses for neuromorphic electronics: From brain-inspired computing to sensorimotor nervetronics. Acc. Chem. Res. 2019, 52, 964–974. [Google Scholar] [CrossRef]
- Lee, H.; Mun, J.S.; San Lee, J.; Chung, Y.; Jung, W.R.; Kang, J.S.; Park, S.M.; Kang, W.; Kim, S.H.; Seo, D.W.; et al. Long-term Non-Anesthetic Preclinical Study Available Extra-Cranial Brain Activator (ECBA) System for the Future Minimally-Invasive Human Neuro-Modulation. In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society, Montreal, QC, Canada, 20–24 July 2020; pp. 5184–5187. [Google Scholar]
- Alivisatos, A.P.; Andrews, A.M.; Boyden, E.S.; Chun, M.; Church, G.M.; Deisseroth, K.; Donoghue, J.P.; Fraser, S.E.; Lippincott-Schwartz, J.; Looger, L.L.; et al. Nanotools for neuroscience and brain activity mapping. ACS Nano 2013, 7, 1850–1866. [Google Scholar] [CrossRef]
- Lee, A.H.; Lee, J.; Jang, J.; Nurmikko, A.; Song, Y.K. Wireless Addressable Cortical Microstimulators Powered by Near-Infrared Harvesting. ACS Sens. 2021, 6, 2728–2737. [Google Scholar] [CrossRef]
- Lyu, L.; Ye, D.; Shi, C.J.R. A 340 nW/Channel 110 dB PSRR Neural Recording Analog Front-End Using Replica-Biasing LNA, Level-Shifter Assisted PGA, and Averaged LFP Servo Loop in 65 nm CMOS. IEEE Trans. Biomed. Circ. Syst. 2020, 14, 811–824. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; San Lee, J.; Chung, Y.; Chung, W.R.; Kim, S.J.; Kang, J.S.; Park, S.M.; Kang, W.; Seo, D.W.; Na, D.L.; et al. Development of wirelessly-powered, extracranial brain activator (ECBA) in a large animal model for the future non-invasive human neuromodulation. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Marcellis, A.; Stanchieri, G.D.P.; Faccio, M.; Palange, E.; Constandinou, T.G. A 300 mbps 37 pJ/bit pulsed optical biotelemetry. IEEE Trans. Biomed. Circ. Syst. 2020, 14, 441–451. [Google Scholar]
- Lee, J.; and Park, S.M. Parameterization of physical properties of layered body structure into equivalent circuit model. BMC Biomed. Eng. 2021, 3, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Dong, N.; Berlinguer-Palmini, R.; Soltan, A.; Ponon, N.; O’Neil, A.; Travelyan, A.; Maaskant, P.; Degenaar, P.; Sun, X. Opto-electro-thermal optimization of photonic probes for optogenetic neural stimulation. J. Biophotonics 2018, 11, e201700358. [Google Scholar] [CrossRef] [PubMed]
- Rand, D.; Jakešová, M.; Lubin, G.; Vėbraitė, I.; David-Pur, M.; Đerek, V.; Cramer, T.; Sariciftci, N.S.; Hanein, Y.; Głowacki, E.D. Direct electrical neurostimulation with organic pigment photocapacitors. Adv. Mater. 2018, 30, 1707292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, W.; Shin, J.; Fu, R.; Kandela, I.; Lu, D.; Ni, X.; Park, Y.; Liu, Z.; Hang, T.; Wu, D.; et al. Bioresorbable photonic devices for the spectroscopic characterization of physiological status and neural activity. Nat. Biomed. Eng. 2019, 3, 644–654. [Google Scholar] [CrossRef]
- Warden, M.R.; Cardin, J.A.; Deisseroth, K. Optical neural interfaces. Annu. Rev. Biomed. Eng. 2014, 16, 103–129. [Google Scholar] [CrossRef] [Green Version]
- Hotamisligil, G.S. Inflammation and metabolic disorders. Nature 2006, 444, 860–867. [Google Scholar] [CrossRef]
- Lo, E.H.; Dalkara, T.; Moskowitz, M.A. Mechanisms, challenges and opportunities in stroke. Nat. Rev. Neurosci. 2003, 4, 399–414. [Google Scholar] [CrossRef]
- DeBerardinis, R.J.; Chandel, N.S. Fundamentals of cancer metabolism. Sci. Adv. 2016, 2, e1600200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tai, L.C.; Gao, W.; Chao, M.; Bariya, M.; Ngo, Q.P.; Shahpar, Z.; Nyein, H.Y.; Park, H.; Sun, J.; Jung, Y.; et al. Methylxanthine drug monitoring with wearable sweat sensors. Adv. Mater. 2018, 30, 1707442. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Lee, I.K.; Taylor, K.; Richters, K.; Baek, D.H.; Ryu, J.H.; Cho, S.J.; Jung, Y.H.; Park, D.W.; Novello, J.; et al. Single-neuronal cell culture and monitoring platform using a fully transparent microfluidic DEP device. Sci. Rep. 2018, 8, 13194. [Google Scholar] [CrossRef] [PubMed]
- Bettinger, C.J. Recent advances in materials and flexible electronics for peripheral nerve interfaces. Bioelectron. Med. 2018, 4, 6. [Google Scholar] [CrossRef] [Green Version]
- Buzsáki, G. Neural syntax: Cell assemblies, synapsembles, and readers. Neuron 2010, 68, 362–385. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Ge, C.; Wang, F.; Guo, Z.; Hong, W.; Jiang, C.; Ji, B.; Wang, M.; Li, C.; Sun, B.; et al. Dense Packed Drivable Optrode Array for Precise Optical Stimulation and Neural Recording in Multiple-Brain Regions. ACS Sens. 2021, 6, 4126–4135. [Google Scholar] [CrossRef]
- Fiáth, R.; Raducanu, B.C.; Musa, S.; Andrei, A.; Lopez, C.M.; van Hoof, C.; Ruther, P.; Aarts, A.; Horváth, D.; Ulbert, I. A silicon-based neural probe with densely-packed low-impedance titanium nitride microelectrodes for ultrahigh-resolution in vivo recordings. Biosens. Bioelectron. 2018, 106, 86–92. [Google Scholar] [CrossRef] [Green Version]
- Raducanu, B.C.; Yazicioglu, R.F.; Lopez, C.M.; Ballini, M.; Putzeys, J.; Wang, S.; Andrei, A.; Rochus, V.; Welkenhuysen, M.; Helleputte, N.V.; et al. Time multiplexed active neural probe with 1356 parallel recording sites. Sensors 2017, 17, 2388. [Google Scholar] [CrossRef] [Green Version]
- Jun, J.J.; Steinmetz, N.A.; Siegle, J.H.; Denman, D.J.; Bauza, M.; Barbarits, B.; Lee, A.K.; Anastassiou, C.A.; Andrei, A.; Aydın, Ç.; et al. Fully integrated silicon probes for high-density recording of neural activity. Nature 2017, 551, 232–236. [Google Scholar] [CrossRef] [Green Version]
- Frey, U.; Sedivy, J.; Heer, F.; Pedron, R.; Ballini, M.; Mueller, J.; Bakkum, D.; Hafizovic, S.; Faraci, F.D.; Greve, F.; et al. Switch-matrix-based high-density microelectrode array in CMOS technology. IEEE J. Solid-State Circ. 2010, 45, 467–482. [Google Scholar] [CrossRef]
- Eversmann, B.; Jenkner, M.; Hofmann, F.; Paulus, C.; Brederlow, R.; Holzapfl, B.; Fromherz, P.; Merz, M.; Brenner, M.; Schreiter, M.; et al. A 128 × 128 CMOS biosensor array for extracellular recording of neural activity. IEEE J. Solid-State Circ. 2003, 38, 2306–2317. [Google Scholar] [CrossRef]
- Nieus, T.; D’Andrea, V.; Amin, H.; Di Marco, S.; Safaai, H.; Maccione, A.; Berdondini, L.; Panzeri, S. State-dependent representation of stimulus-evoked activity in high-density recordings of neural cultures. Sci. Rep. 2018, 8, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Poirier-Quinot, M.; Ginefri, J.C.; Girard, O.; Robert, P.; Darrasse, L. Performance of a miniature high-temperature superconducting (HTS) surface coil for in vivo microimaging of the mouse in a standard 1.5 T clinical whole-body scanner. Magn. Reson. Med. Off. J. Int. Soc. Magn. Reson. Med. 2008, 60, 917–927. [Google Scholar] [CrossRef]
- Serfaty, S.; Haziza, N.; Darrasse, L.; Kan, S. Multi-turn split-conductor transmission-line resonators. Magn. Reson. Med. 1997, 38, 687–689. [Google Scholar] [CrossRef]
- Couty, M.; Woytasik, M.; Ginefri, J.C.; Rubin, A.; Martincic, E.; Poirier-Quinot, M.; Darrasse, L.; Boumezbeur, F.; Lethimonnier, F.; Tatoulian, M.; et al. Fabrication and packaging of flexible polymeric microantennae for in vivo magnetic resonance imaging. Polymers 2012, 4, 656–673. [Google Scholar] [CrossRef] [Green Version]
- Masilamany, G.; Joubert, P.Y.; Serfaty, S.; Roucaries, B.; Griesmar, P. Wireless implementation of high sensitivity radiofrequency probes for the dielectric characterization of biological tissues. In Proceedings of the 2014 IEEE International Symposium on Medical Measurements and Applications, Lisboa, Portugal, 11–12 June 2014; pp. 1–6. [Google Scholar]
- Lee, A.H.; Lee, J.; Laiwalla, F.; Leung, V.; Huang, J.; Nurmikko, A.; Song, Y.K. A scalable and low stress post-CMOS processing technique for implantable microsensors. Micromachines 2020, 11, 925. [Google Scholar] [CrossRef]
- Maghami, M.H.; Sodagar, A.M.; Lashay, A.; Riazi-Esfahani, H.; Riazi-Esfahani, M. Visual prostheses: The enabling technology to give sight to the blind. J. Ophthalmic Vis. Res. 2014, 9, 494. [Google Scholar]
- Petoe, M.A.; Titchener, S.A.; Kolic, M.; Kentler, W.G.; Abbott, C.J.; Nayagam, D.A.; Baglin, E.K.; Kvansakul, J.; Barnes, N.; Walker, J.G.; et al. A Second-Generation (44-Channel) Suprachoroidal Retinal Prosthesis: Interim Clinical Trial Results. Transl. Vis. Sci. Technol. 2021, 10, 12. [Google Scholar]
- Brelén, M.E.; Duret, F.; Gérard, B.; Delbeke, J.; Veraart, C. Creating a meaningful visual perception in blind volunteers by optic nerve stimulation. J. Neural Eng. 2005, 2, S22. [Google Scholar] [CrossRef] [PubMed]
- Damle, S.; Carleton, M.; Kapogianis, T.; Arya, S.; Cavichini-Corderio, M.; Freeman, W.R.; Lo, Y.H.; Oesch, N.W. Minimizing iridium oxide electrodes for high visual acuity subretinal stimulation. Eneuro 2021, 8, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Fujikado, T.; Kamei, M.; Sakaguchi, H.; Kanda, H.; Morimoto, T.; Ikuno, Y.; Nishida, K.; Kishima, H.; Maruo, T.; Konoma, K.; et al. Testing of semichronically implanted retinal prosthesis by suprachoroidal-transretinal stimulation in patients with retinitis pigmentosa. Investig. Ophthalmol. Vis. Sci. 2011, 52, 4726–4733. [Google Scholar] [CrossRef]
- Dobelle, W.H. Artificial vision for the blind by connecting a television camera to the visual cortex. ASAIO J. 2000, 46, 3–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, S.K.; Ellersick, W.F.; Krishnan, A.; Doyle, P.; Shire, D.B.; Wyatt, J.L.; Rizzo, J.F. Redundant safety features in a high-channel-count retinal neurostimulator. In Proceedings of the 2014 IEEE Biomedical Circuits and Systems Conference Proceedings, Lausanne, Switzerland, 22–24 October 2014; pp. 216–219. [Google Scholar]
- Kelly, S.K.; Shire, D.B.; Chen, J.; Gingerich, M.D.; Cogan, S.F.; Drohan, W.A.; Ellersick, W.; Krishnan, A.; Behan, S.; Wyatt, J.L.; et al. Developments on the Boston 256-channel retinal implant. In Proceedings of the 2013 IEEE International Conference on Multimedia and Expo Workshops, San Jose, CA, USA, 15–19 July 2013; pp. 1–6. [Google Scholar]
- Kelly, S.K.; Shire, D.B.; Chen, J.; Doyle, P.; Gingerich, M.D.; Cogan, S.F.; Drohan, W.A.; Behan, S.; Theogarajan, L.; Wyatt, J.L.; et al. A hermetic wireless subretinal neurostimulator for vision prostheses. IEEE Trans. Biomed. Eng. 2011, 58, 3197–3205. [Google Scholar] [CrossRef] [Green Version]
- Chow, A.Y.; Chow, V.Y. Subretinal electrical stimulation of the rabbit retina. Neurosci. Lett. 1997, 225, 13–16. [Google Scholar] [CrossRef]
- Zrenner, E. Will retinal implants restore vision? Science 2002, 295, 1022–1025. [Google Scholar] [CrossRef] [Green Version]
- Zrenner, E. Fighting blindness with microelectronics. Sci. Transl. Med. 2013, 5, 210ps16. [Google Scholar] [CrossRef]
- Akinin, A.; Ford, J.M.; Wu, J.; Kim, C.; Thacker, H.D.; Mercier, P.P.; Cauwenberghs, G. 18.1 An Optically-Addressed Nanowire-Based Retinal Prosthesis with 73% RF-to-Stimulation Power Efficiency and 20nC-to-3μ C Wireless Charge Telemetering. In Proceedings of the 2021 IEEE International Solid-State Circuits Conference, San Francisco, CA, USA, 13–22 February 2021; Volume 64, pp. 276–278. [Google Scholar]
- Jung, S.W.; Shin, J.Y.; Pi, K.; Goo, Y.S.; Cho, D.I. Neuron Stimulation Device Integrated with Silicon Nanowire-Based Photodetection Circuit on a Flexible Substrate. Sensors 2016, 16, 2035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krylyuk, S.; Davydov, A.V.; Levin, I. Tapering control of Si nanowires grown from SiCl4 at reduced pressure. ACS Nano 2011, 5, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Lorach, H.; Goetz, G.; Smith, R.; Lei, X.; Mandel, Y.; Kamins, T.; Mathieson, K.; Huie, P.; Harris, J.; Sher, A.; et al. Photovoltaic restoration of sight with high visual acuity. Nat. Med. 2015, 21, 476–482. [Google Scholar] [CrossRef] [Green Version]
- Zrenner, E.; Bartz-Schmidt, K.U.; Benav, H.; Besch, D.; Bruckmann, A.; Gabel, V.P.; Gekeler, F.; Greppmaier, U.; Harscher, A.; Kibbel, S.; et al. Subretinal electronic chips allow blind patients to read letters and combine them to words. Proc. R. Soc. B Biol. Sci. 2011, 278, 1489–1497. [Google Scholar] [CrossRef]
- Ayton, L.N.; Blamey, P.J.; Guymer, R.H.; Luu, C.D.; Nayagam, D.A.; Sinclair, N.C.; Shivdasani, M.N.; Yeoh, J.; McCombe, M.F.; Briggs, R.J.; et al. First-in-human trial of a novel suprachoroidal retinal prosthesis. PLoS ONE 2014, 9, e115239. [Google Scholar] [CrossRef] [Green Version]
- Zeng, Q.; Wu, T. Enhanced electrochemical performance of neural electrodes based on PEDOT: PSS hydrogel. J. Appl. Polym. Sci. 2021, 139, 51804. [Google Scholar] [CrossRef]
- Ptito, M.; Bleau, M.; Djerourou, I.; Paré, S.; Schneider, F.C.; Chebat, D.R. Brain-machine interfaces to assist the blind. Front. Hum. Neurosci. 2021, 15, 1–19. [Google Scholar] [CrossRef] [PubMed]
- George, M.S.; Nahas, Z.; Bohning, D.E.; Lomarev, M.; Denslow, S.; Osenbach, R.; Ballenger, J.C. Vagus nerve stimulation: A new form of therapeutic brain stimulation. CNS Spectr. 2000, 5, 43–52. [Google Scholar] [CrossRef]
- Zabara, J. Inhibition of experimental seizures in canines by repetitive vagal stimulation. Epilepsia 1992, 33, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Sackeim, H.A.; Rush, A.J.; George, M.S.; Marangell, L.B.; Husain, M.M.; Nahas, Z.; Johnson, C.R.; Seidman, S.; Giller, C.; Haines, S.; et al. Vagus nerve stimulation (VNS™) for treatment-resistant depression: Efficacy, side effects, and predictors of outcome. Neuropsychopharmacology 2001, 25, 713–728. [Google Scholar] [CrossRef] [Green Version]
- Groves, D.A.; Brown, V.J. Vagal nerve stimulation: A review of its applications and potential mechanisms that mediate its clinical effects. Neurosci. Biobehav. Rev. 2005, 29, 493–500. [Google Scholar] [CrossRef]
- Englot, D.J.; Chang, E.F.; Auguste, K.I. Efficacy of Vagus Nerve Epilepsy Stimulation by Patient for Age, Epilepsy Duration, and Seizure Type. Epilepsy Issue Neurosurg. Clin. E-Book 2011, 22, 443. [Google Scholar] [CrossRef]
- Schwedt, T.J.; Vargas, B. Neurostimulation for treatment of migraine and cluster headache. Pain Med. 2015, 16, 1827–1834. [Google Scholar] [CrossRef] [Green Version]
- Dawson, J.; Engineer, N.D.; Prudente, C.N.; Pierce, D.; Francisco, G.; Yozbatiran, N.; Tarver, W.B.; Casavant, R.; Kline, D.K.; Cramer, S.C.; et al. Vagus nerve stimulation paired with upper-limb rehabilitation after stroke: One-year follow-up. Neurorehabilit. Neural Repair 2020, 34, 609–615. [Google Scholar] [CrossRef]
- Penry, J.K.; Dean, J.C. Prevention of intractable partial seizures by intermittent vagal stimulation in humans: Preliminary results. Epilepsia 1990, 31, S40–S43. [Google Scholar] [CrossRef]
- Uthman, B.M.; Wilder, B.J.; Penry, J.K.; Dean, C.; Ramsay, R.E.; Reid, S.A.; Hammond, E.J.; Tarver, W.B.; Wernicke, J.F. Treatment of epilepsy by stimulation of the vagus nerve. Neurology 1993, 43, 1338. [Google Scholar] [CrossRef]
- Cristancho, M.A.; Cristancho, P.; Altinay, M.; O’Reardon, J.P. Vagus nerve stimulation (VNS). In Psychiatric Neurotherapeutics; Humana Press: New York, NY, USA, 2016; pp. 99–116. [Google Scholar]
- Jodoin, V.D.; Richer, F.; Miron, J.P.; Fournier-Gosselin, M.P.; Lespérance, P. Long-term sustained cognitive benefits of vagus nerve stimulation in refractory depression. J. ECT 2018, 34, 283–290. [Google Scholar] [CrossRef]
- Wang, D.W.; Yin, Y.M.; Yao, Y.M. Vagal modulation of the inflammatory response in sepsis. Int. Rev. Immunol. 2016, 35, 415–433. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.Z.; Fu-Shan, X.; Sun, C.; Liao, X.; Liu, J.H. Vagal nerve stimulation: A potentially useful adjuvant to treatment of sepsis. J. Anesth. Perioper. Med. 2018, 5, 161. [Google Scholar] [CrossRef] [Green Version]
- De Ferrari, G.M.; Crijns, H.J.; Borggrefe, M.; Milasinovic, G.; Smid, J.; Zabel, M.; Gavazzi, A.; Sanzo, A.; Dennert, R.; Kuschyk, J.; et al. Chronic vagus nerve stimulation: A new and promising therapeutic approach for chronic heart failure. Eur. Heart J. 2011, 32, 847–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steinberg, B.E.; Silverman, H.A.; Robbiati, S.; Gunasekaran, M.K.; Tsaava, T.; Battinelli, E.; Stiegler, A.; Bouton, C.E.; Chavan, S.S.; Tracey, K.J.; et al. Cytokine-specific neurograms in the sensory vagus nerve. Bioelectron. Med. 2016, 3, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Birnbaum, H.G.; White, A.G.; Schiller, M.; Waldman, T.; Cleveland, J.M.; Roland, C.L. Societal costs of prescription opioid abuse, dependence, and misuse in the United States. Pain Med. 2011, 12, 657–667. [Google Scholar] [CrossRef] [Green Version]
- Koopman, F.A.; Chavan, S.S.; Miljko, S.; Grazio, S.; Sokolovic, S.; Schuurman, P.R.; Mehta, A.D.; Levine, Y.A.; Faltys, M.; Zitnik, R.; et al. Vagus nerve stimulation inhibits cytokine production and attenuates disease severity in rheumatoid arthritis. Proc. Natl. Acad. Sci. USA 2016, 113, 8284–8289. [Google Scholar] [CrossRef] [Green Version]
- GammaCore (nVNS). Non-Drug Relief for Migraine & Cluster Headache Pain. Available online: www.gammacore.com (accessed on 1 August 2018).
- Yap, J.Y.; Keatch, C.; Lambert, E.; Woods, W.; Stoddart, P.R.; Kameneva, T. Critical review of transcutaneous vagus nerve stimulation: Challenges for translation to clinical practice. Front. Neurosci. 2020, 14, 284. [Google Scholar] [CrossRef]
- Cao, Y.; Pan, S.; Yan, M.; Sun, C.; Huang, J.; Zhong, C.; Wang, L.; Yi, L. Flexible and stretchable polymer optical fibers for chronic brain and vagus nerve optogenetic stimulations in free-behaving animals. BMC Biol. 2021, 19, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Chen, P.; Wang, Q.; Wan, X.; Yang, M.; Liu, C.; Xu, C.; Hu, B.; Feng, J.; Luo, Z. Wireless electrical stimulation of the vagus nerves by ultrasound-responsive programmable hydrogel nanogenerators for anti-inflammatory therapy in sepsis. Nano Energy 2021, 89, 106327. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhou, L.; Gao, X.; Liu, C.; Chen, H.; Zheng, H.; Gui, J.; Sun, C.; Yu, L.; Guo, S. Performance-enhanced flexible piezoelectric nanogenerator via layer-by-layer assembly for self-powered vagal neuromodulation. Nano Energy 2021, 89, 106319. [Google Scholar] [CrossRef]
- Dubey, S.; Chiao, J.C. Implantable Radio Frequency Powered Gastric Electrical Stimulator. IEEE J. Electromagn. RF Microw. Med. Biol. 2021, 1–8. [Google Scholar] [CrossRef]
- Wu, Y.; Jiang, D.; Neshatvar, N.; Demosthenous, A. A Power Efficient Time-to-Current Stimulator for Vagal-Cardiac Connection after Heart Transplantation. In Proceedings of the 2021 IEEE International Symposium on Circuits and Systems, Daegu, Korea, 22–28 May 2021; pp. 1–4. [Google Scholar]
- Dabiri, B.; Zeiner, K.; Nativel, A.; Kaniusas, E. Multifunctional auricular vagus nerve stimulator for closed-loop application. In Proceedings of the 2021 34th SBC/SBMicro/IEEE/ACM Symposium on Integrated Circuits and Systems Design, Campinas, Brazil, 23–27 August 2021; pp. 1–5. [Google Scholar]
- Devi, S.; Guha, K.; Laskar, N.M.; Nath, S.; Baishnab, K.L.; Iannacci, J.; Krishnaswamy, N. Modelling and analysis of a modified preamplifier for seizure detection. Microsyst. Technol. 2021, 27, 1–14. [Google Scholar] [CrossRef]
- Magisetty, R.; Shukla, A.; Kandasubramanian, B. Magnetodielectric microwave radiation absorbent materials and their polymer composites. J. Electron. Mater. 2018, 47, 6335–6365. [Google Scholar] [CrossRef]
- Magisetty, R.; Shukla, A.; Kandasubramanian, B. Terpolymer (ABS) cermet (Ni-NiFe2O4) hybrid nanocomposite engineered 3D-carbon fabric mat as a X-band electromagnetic interference shielding material. Mater. Lett. 2019, 238, 214–217. [Google Scholar] [CrossRef]
- Magisetty, R.; Raj, A.B.; Datar, S.; Shukla, A.; Kandasubramanian, B. Nanocomposite engineered carbon fabric-mat as a passive metamaterial for stealth application. J. Alloy Compd. 2020, 848, 155771. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Retinal Prosthesis Devices | Implantable VNS Devices and External VNS Devices | Cardiac Pacemaker Devices | Deep Brain Stimulation Devices |
|---|---|---|---|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Magisetty, R.; Park, S.-M. New Era of Electroceuticals: Clinically Driven Smart Implantable Electronic Devices Moving towards Precision Therapy. Micromachines 2022, 13, 161. https://doi.org/10.3390/mi13020161
Magisetty R, Park S-M. New Era of Electroceuticals: Clinically Driven Smart Implantable Electronic Devices Moving towards Precision Therapy. Micromachines. 2022; 13(2):161. https://doi.org/10.3390/mi13020161
Chicago/Turabian StyleMagisetty, RaviPrakash, and Sung-Min Park. 2022. "New Era of Electroceuticals: Clinically Driven Smart Implantable Electronic Devices Moving towards Precision Therapy" Micromachines 13, no. 2: 161. https://doi.org/10.3390/mi13020161
APA StyleMagisetty, R., & Park, S.-M. (2022). New Era of Electroceuticals: Clinically Driven Smart Implantable Electronic Devices Moving towards Precision Therapy. Micromachines, 13(2), 161. https://doi.org/10.3390/mi13020161