Abstract
Dual energy (DE) technique has been used by numerous studies in order to detect breast cancer in early stages. Although mammography is the gold standard, the dual energy technique offers the advantage of the suppression of the contrast between adipose and glandular tissues and reveals pathogenesis that is not present in conventional mammography. Both dual energy subtraction and dual energy contrast enhanced techniques were used in order to study the potential of dual energy technique to assist in detection or/and visualization of calcification minerals, masses and lesions obscured by overlapping tissue. This article reviews recent developments in this field, regarding: i) simulation studies carried out for the optimizations of the dual energy technique used in order to characterize and quantify calcification minerals or/and visualize suspected findings, and ii) the subsequent experimental verifications, and finally, the adaptation of the dual energy technique in clinical practice.
Keywords:
dual energy; X-rays; minerals; crystalline compounds; crystal structure; breast imaging; mammography; cancer 1. Introduction
Breast cancer is one of the most common causes of cancer death in the United States [1], accounting for approximately 12% of globally diagnosed cancers in 2012 [2]. Diagnosis of cancer in early stage leads to more efficient treatment [3,4,5]. Furthermore, early detection through screening and adequate follow-up of women with positive findings could significantly reduce breast cancer mortality (by 15–25%) [6]. Preliminary signs of masses and microcalcifications are important indicators of breast cancer [7,8,9]. A considerable percentage of non-palpable breast cancers (30–50%) are detected only because of the appearance of microcalcifications in a mammogram [10].
Several imaging modalities, such as mammography, ultrasound, and digital tomosynthesis, have been used for breast cancer diagnosis. X-ray mammography is the gold standard method for early detection of breast carcinomas [11,12,13,14]. Masses, areas of distortion, and calcifications that cannot be detected by physical examination can be visible on mammograms [15]. Although mammography can detect the aforementioned distortions, overlapping tissue structures may obscure their detection. As calcifications are the smallest objects that can be detected, any further improvement in their detection and visualization is an important step forward. Microcalcifications exhibit higher X-ray attenuation compared to the surrounding breast tissue making them visible, while masses are difficult to be detected since the X-ray attenuation is similar to that of the healthy breast tissue [16].
Dual energy (DE) technique suppresses the contrast between adipose and glandular tissues revealing pathogenesis that is not present in screening mammography [16]. Dual energy digital mammography (DEDM) employs two sequential measurements at different kilovoltages (kV), typically with different beam filters mechanically moved into and out of the beam between exposures [17]. Since dual energy technique requires two separate irradiations, no energy discrimination is required in the detector. The added filtration selectively removes lower energy photons from the high kV beam and provides similar beam intensities at the detector, which otherwise would be much greater for the high kV beam [17,18]. By properly subtracting the low- and high- energies, the contrast between any two materials may be cancelled or reduced to enhance visualization in imaging procedures [19,20,21,22,23]. Weighted subtraction of the logarithmic transform of the low- and high-energy images is performed to obtain a subtracted image that enhances microcalcifications [20,21]. In the same sense, in dual energy contrast enhanced digital mammography (CEDM) has been evaluated for the improvement in the detection of lesions in the final (subtracted) image [22,23].
This paper reviews recent developments in this field regarding: (i) the simulation studies performed for the optimization of the dual energy technique in order to detect/visualize suspected findings (masses, lesions and calcification minerals with crystalline formation), (ii) the experimental verifications of studies as well as their results, and (iii) the application of DE in clinical practice.
2. Dual Energy Method
Dual energy digital mammography (DEDM) involves the acquisition of two images (high- and low-energy image) and then weighted subtraction is applied leading to decrease of the obscurity from tissue structure materials [17,24]. Dual kilovoltage technique employ two sequential measurements at different kilovoltages, typically, with different beam filters resulting in no need of energy discrimination in at the detector. [17,18]. The proper subtraction of the low- and high- energy images results in cancellation or reduction of the contrast between any two materials. Thus, the suspected findings (i.e., lesions, calcifications, masses) are enhanced in the final image [17,18,19,20,21,22,23].
The dual energy technique can be implemented with two filtering methods. The K-edge filtering technique is used to modify the output from the X-ray tube. The selected filter materials should have a K-shell absorption edge near the midpoint of the energy spectrum. Selective attenuation of photons just above the absorption edge creates a transmitted spectrum consisting of two relatively narrow bands. Only a single exposure is required with K-edge filtering as both energies are present simultaneously in the radiation beam [17]. When single exposure is used, an energy-resolving detector should be employed in order to distinguish and use only the appropriate energy range. The K-edge filtering technique has also been used in the dual energy imaging in order to shape the low- and high-energy spectra and obtain quasi-monochromatic spectra [25,26,27,28].
In dual energy iodine contrast imaging technique, iodine is used as a contrast agent. The balanced filter technique, that is used in iodine contrast imaging, is the second filtering method and uses three filters. Since iodine is the contrast medium, it is used as one of the three filters (filter 2). The other two filters are selected in the basis that their atomic numbers should be lower (filter 1) and higher (filter 3) than iodine, respectively. In iodine contrast imaging technique, the patient undergoes a mammogram before the contrast medium injection [16]. The subtraction of the mammogram and the image acquired, after the injection, cancels out the background and the lesions are enhanced due to the iodine uptake. However, with iodine contrast imaging technique both low- and high-energy images can be acquired after the patient is injected with the contrast medium [29,30].
Regardless the image filtering and acquisition techniques, a weighted subtraction after logarithmic transform of the low- and high-energy pixel values is performed. The final dual energy image reveals enhanced the distortions either the patient was injected or not [16,20,21,25,26].
3. Detectors Used in Dual Energy Breast Imaging
In the last decades, several researchers studied the ability of Dual Energy mammography using different detector systems. Johns and Yaffe worked firstly on a theoretical optimization considering an ideal imaging system [31] and the experimental verification followed, was accomplished with a prototype scanned projection detector [31]. Boone et al. [32] evaluated the efficacy of simulated color mammography dual energy image. A calcium index image is computed which corresponds to a dual energy basis decomposition tissue subtracted image. Then the calcium index image is colorized using simple color schemes and overlaid onto the conventional single energy image. Six detector pairs, with the following crystalline materials, were examined: Y2O2S/Gd2O2S, SrFBr/BaFBr, Y2O2S/LaOBr, Y2O2S/CaWO4, Y2O2S/YTaO4, and Y2O2S/LuTaO4 [32]. The Y2O2S/Gd2O2S as well as the SrFBr/BaFBr crystalline materials were found to be the best combinations. Brettle and Cowen [33] expanded the theoretical model of Boone et al. [32] using a commercial Computed Radiography system. Furthermore, hydrogenated amorphous silicon (aSi:H) flat panel detectors coupled with a thallium-doped cesium iodide (CsI:Tl) converter layer have extensively used in dual energy mammography studies [8,9,21,22,23,34,35,36,37]. Finally, digital X-ray imaging detectors [38,39,40] based on complementary metal oxide semiconductor (CMOS) active pixel sensors (APS) coupled to Gd2O2S:Tb phosphor screen have been recently introduced in dual energy breast imaging applications [25,26,27,28].
4. Simulation Studies
The present section summarizes the simulation studies developed in dual energy breast imaging field. The development or modification of algorithms, the study of the impact in using different input parameters, and generally the adoption of different considerations in those simulation studies are presented below. The results obtained from each study are also presented.
Lemacks et al. presented the theoretical framework they developed for the calculation of the calcification signal-to-noise ratio (SNR) in dual energy images [20]. They studied the influence of various imaging parameters (i.e., polyenergetic X-ray spectrum, scintillating material, microcalcification size, tissue composition, breast thickness) on the calcification contrast-to-noise ratio, considering a fixed entrance exposure of 1000 mR. The standard clinical practices and considerations were preserved throughout the study. The optimization of the dual energy technique resulted in the detection of 250 μm microcalcificaton mineral size in a 5 cm compressed breast composed of 50% adipose and 50% glandular tissue. The signal-to-noise analysis presented in this work, evaluated the performance of dual energy imaging, without addressing the impact of scatter radiation and detector response [20]. This was addressed in following studies [8,9,24,35].
Brandan and Ramirez applied Lemacks’ analytical model [20] to calculate the contrast-to-noise ratio in subtracted images considering exposure conditions (i.e., voltage, target and filter material and thickness) available in a Senographe 2000D unit used in clinical practice [21]. The input parameters (i.e., X-ray spectra, breast and microcalcification composition) used were obtained from different published data, compared to Lemacks et al. [20]. The results showed differences ranging from 40% to 70% in contrast-to-noise ratio values. The differences depended on the choices made for the spectra, breast tissue and calcification composition. The contrast-to-noise ratio values in the subtracted microcalcification image were found to be smaller than the Rose’s criterion when using the equipment beams. According to Rose’s criterion, the minimum signal-to-noise ratio should be close to 5 in order an object to be visible in a homogeneous background. The study of Brandan and Ramirez concluded to different results than Lemacks et al. despite the fact that the same analytical model was used [20,21].
Ducote and Molloi investigated the use of dual energy imaging to quantify breast density. Both monoenergetic beams and polyenergetic X-ray spectra were studied [41]. The impact of various beam energies, dose ratios, and pre-patient filtration on breast density was investigated for several breast thicknesses. The results, considering a breast of 4.2 cm, for the monoenergetic approach showed that a mean glandular dose of 0.183 μGy was required, while the required mean glandular dose for the polyenergetic approach was 9.85 μGy. Based on these results, the breast density can be measured with dual energy imaging with either configuration (monoenergetic or polyenergetic) with an increase in the dose when polyenergetic X-ray spectra are used. This study concluded that this technique could make use of a standard screening mammogram along with a high energy image exposure, while an added small amount of dose would be imparted to the patient [41].
Koukou et al. investigated a dual energy method for the detection of the minimum microcalcification thickness. The minimum microcalcification thickness was determined by applying Lemacks’s et al. [20] monoenergetic analytical modeling [25]. In this study, a modified radiographic X-ray unit was considered to overcome the kVp range limitation of mammographic units used in previous dual energy studies [20,21]. The optimum irradiation conditions (i.e., X-ray tube high voltage, filter material according to their K-edge and thickness) were resolved for polyenergetic spectra, so the study becomes more realistic. The contrast-to-noise ratio of the subtracted calcification images was calculated for various skin entrance doses (0.96 mGy to 3.52 mGy) and a breast thickness of 4 cm. The resulted minimum detectable microcalcification mineral thickness was 150 μm. The dual energy method modeled in this work revealed that this method could provide improved calcification detectability in breast imaging [25].
Del Lama et al. studied the dual energy features with the use of a modified PENELOPE Monte Carlo code [42]. The dual energy technique, using mammography parameters and geometry, was employed for (i) studying the visualization and measurement of microcalcification thicknesses, (ii) determination of the glandular ratios and (iii) evaluation of the effect of the algorithm correction methods. The modified Monte Carlo code followed the mathematical framework developed by Lemacks et al. (2002) [20]. It was found that the obtained scatter and noise corrected dual energy maps revealed better quality images when compared to conventional mammography images. This was attributed to the elimination of background. Furthermore, the results of this study showed that it was able to visualize microcalcifications as small as 200 μm with a contrast-to-noise ratio of 4, regardless the breast glandularity (25%, 50%, and 75%). The mean glandular dose was constrained to 2.5 mGy. The dual energy technique could also verify the breast glandular ratio for different glandularities (25%, 50%, and 75%) and breast thicknesses ranging from 2 to 6 cm. The proposed method could be used as an adjunction for standard mammography in cases where the calcification thickness and glandularity needs to be assessed [42].
Del Lama et al. modified and validated a PENELOPE code for digital mammography applications that evaluated several quantities such as scatter to primary ratio, scatter fraction, and normalized mean glandular dose [43]. The magnitude of the incident scattered radiation on the detector is quantified using the scatter to primary ratio or the scatter fraction. The simulated dual energy images were investigated for visualization of microcalcifications. In this study was adopted the mathematical formalism developed by Lemacks et al. (2002) [20]. The modified PENELOPE code was found to agree well against previous works found in literature [44,45,46,47,48,49,50,51,52,53,54], especially under mammography conditions. Based on the results, the modified code of the present study could distinguish between primary and secondary radiation. The simulated dual energy images enhanced the calcification mineral visualization over the neighboring tissues and allowed a better assessment of its dimensions. It was considered a 4 cm thick breast composed of 30% glandular tissue and 70% of adipose tissue. The minimum microcalcification that could be visualized (contrast-to-noise ratio of 4), with a mean glandular dose of 2.5 mGy, was 200 μm. The proposed simulations showed that the dual energy technique could be a complementary tool for the conventional images, regarding the visualization and estimation of glandular ratio and calcification thicknesses [43].
Table 1 summarizes the optimum parameters of the simulation studies. The low– and high-energy beam and low- and high-energy spectra combinations are indicated with keV and kVp, respectively. The anode/filter combinations used for the low energy (LE) and high energy (HE) images in the polyenergetic approaches are also presented. The majority of studies used calcium carbonate (CaCO3) crystals simulating microcalcifications [20,21,42,43]. Koukou et al. used Hydroxyapatite (Hap) to simulate microcalcifications [25]. According to previous studies, the microcalcifications that are associated with malignancy are mainly composed of Hydroxyapatite crystals [44,45]. Finally, the mean glandular doses of the studies are also presented. Only the study of Ducote and Molloi [41] resulted in mean glandular dose of μGy. However, the mean glandular dose of the polyenergetic approach was substantially increased, as expected, compared to the monoenergetic approach (approximately 53.8 times).

Table 1.
Optimized parameters and results of the simulation studies.
5. Experimental Studies
The Experimental Studies section present the experimental studies developed using the dual energy technique. Experimental evaluation of studies (see Simulation Studies section) as well as experimental procedures for detection of tumor like lesions, calcifications, and determination of breast density is the scope of the studies below. The results obtained from each study are also presented.
Marziani et al. based on the tissue cancellation algorithm published by Alvarez and Macovski [31,55] developed a prototype dual energy radiographic system [56]. A quasi-monochromatic X-ray source [57] with a phosphor-coated CCD detector [58,59] were used in order to acquire the low-and high- energy images of a test object in the energy range 17–36 keV. The test object (Figure 1a) consisted of rods filled with water and Polyethylene (PE) placed in a Polymethyl Methacrylate (PMMA) tank. Although tissue cancellation and enhancement of tumor-like lesions were achieved for some of the tissue equivalent inserts of the test object, further investigation on energy optimization of the primary beams, delivered dose and noise propagation should be done [56].
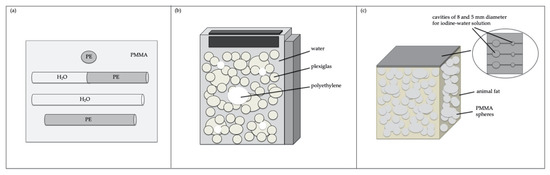
Figure 1.
Schematic representation of phantoms used in the experimental studies [22,34,56,60]; (a,b) The phantoms represent tumor-like lesions; (c) iodine concentration for dual energy contrast enhanced mammography technique.
Kappadath and Shaw investigated whether inverse-mapping functions could estimate calcification thickness and glandular ratio [24]. The glandular ratio was defined as the ratio of the glandular tissue thickness to the total tissue thickness. The dual energy technique was actually used in this study in order to invert the low- and high-energy images from log-signal functions into calcification thickness and glandular ratio. Low- and high-energy images were acquired with the dual energy digital mammography technique under narrow beam geometry (Figure 2b) in order to obtain calibration data. The inverse-mapping of the measured dual energy transmission data into aluminum thicknesses, simulating microcalcifications, and glandular ratios was accomplished by fitting the calibration data with analytical functions (linear, quadratic, cubic, and conic). The linear function could not fit the data of both aluminum thickness and glandular ratio. The quadratic, cubic and conic functions proved to be more accurate compared to linear function, with more accurate the cubic or conic function. They concluded that the effects of scatter radiation and non-uniform log-signal values would be investigated in full field images. [24].
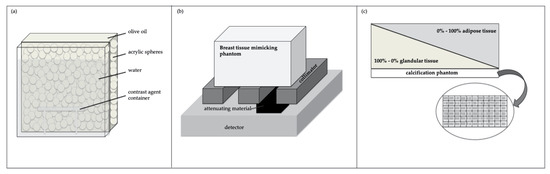
Figure 2.
Schematic representation of the experimental studies’ phantoms [8,9,24,29]; (a) iodine concentration for dual energy contrast enhanced mammography technique; (b,c) calcification for dual energy mammography technique.
Taibi et al. implemented a feasibility study of the dual energy technique using a GE Senographe 2000D digital unit (GE Medical Systems, USA) aiming to detect small and low contrast tumor-like lesions embedded in a cluttered background [34]. A three-component tissue equivalent breast phantom was constructed for this preliminary study (Figure 1b). The three-component phantom consisted of a PMMA box filled with water. PMMA and Polyethylene spheres of different diameters were placed into the 5 cm thick PMMA box. The combination of low- and high-energy images acquired by a Molybdenum anode at 28 kVp and a Rhodium anode at 49 kVp, respectively, resulted in a 2.25 mGy mean glandular dose and enhancement of an 8 mm Polyethylene sphere over the cancelled out background. The applied technique resulted successfully in removing the contrast between water and PMMA and thereby enhancing the visibility of Polyethylene details [34].
Kappadath and Shaw presented a dual energy digital mammography technique with nonlinear inverse-mapping functions for calcification thickness estimation [8]. The phantoms irradiated, under narrow-beam geometry (Figure 2b), were constructed with breast tissue equivalent materials of different glandularities (25%, 50%, 75%, and 100%) and aluminum strips (0.39, 0.78, 1.17, 1.56, and 1.95 mm) simulating calcifications. The measured aluminum thicknesses found close to the true aluminum thicknesses regardless the glandularity studied. The underestimation of the true aluminum thicknesses was attributed to the presence of scatter from the neighboring areas. Despite the fact that the aluminum contrast-to-noise ratio was decreased in the dual energy digital mammography images, the tissue structures did not reduce the visualization of the aluminum stripes any further. Thus, dual energy digital mammography could provide quantitative information for the calcification thickness [8].
Kappadath and Shaw carried out a dual energy digital mammography technique for the visualization of calcifications (Figure 2c) using a commercially available digital mammography system (Senographe 2000D, GE Medical Systems, Milwaukee, WI) [9]. As spatial non-uniformity was observed, reference images of uniform slab phantoms were acquired in order to reduce the signals in the background of the final dual energy images. The total entrance-skin exposure and mean-glandular dose from the low- and high-energy images were within the mammography screening levels. Under these considerations, calcifications with sizes ranging from 300 μm to 355 μm were clearly visible in the dual energy calcification images. When the criterion turned from visible to barely visible and local adjustments of contrast and brightness were performed, the margins of calcifications with sizes ranging from 250 μm to 280 μm were detectable. However, with the proposed method, the visibility of calcifications was limited by quantum noise [9].
Baldelli et al. studied the application of the dual energy K-edge subtraction mammography and dual energy temporal subtraction mammography techniques [22,60]. Synchrotron radiation and a clinical digital mammography system (Senographe 2000D, GE Medical Systems, Milwaukee, WI) were used for the above techniques, respectively. The three-component phantom (Figure 1c) used in this study enclosed cavities that were filled with different concentrations of iodine. The contrast-to-noise ratio (CNR) and the mean glandular dose (MGD) values were also assessed. The minimum iodine concentration that could significantly enhance the detectability of the pathology, with delivered dose within the acceptable levels of mammography, was the objective in each technique. The optimum contrast medium concentration for each technique was estimated based on the introduced figure of merit (FOM = CNR2/MGD). A CNR of 5 could be achieved in this study with 2 mGy. The two techniques were found to be comparable when a monochromatic source is used [22,60].
Saito worked on the approach of using the balanced filter method in dual energy technique [29]. A simulation study was conducted for the theoretical optimization in order to obtain the required dose for a signal-to-noise ratio of 5 in the dual energy subtracted iodine image. To this aim, the analytical model of Lemacks et al. [20] was used to calculate signal-to-noise ratio in an iodinated contrast agent subtraction image. The use of a 0.1 mm thick CsI:Tl scintillator [61,62,63] led to optimal Tungsten anode tube voltage of 45 kVp and use of Zirconium, Iodine, and Neodymium balanced filters. Preliminary phantom (Figure 2a) experiments were carried out to demonstrate the capability of dual energy contrast-enhanced mammography using the balanced filter method to obtain a clutter-free subtracted image that preferentially shows the iodinated contrast agent in a breast phantom. A mean glandular dose of 1.0 mGy was needed to achieve a signal-to-noise ratio of 5 for the detection of 1.0 mg/cm2 iodine in the obtained clutter-free image of a 5 cm thick breast composed of 50% adipose and 50% glandular tissue. The proposed dual energy method could be used not only in conventional mammography but also in tomography (i.e., tomosynthesis, computed tomography) in order to achieve three dimensional tumor enhancement [29].
Kappadath and Shaw studied the effects of three different noise reduction techniques on dual energy calcification images acquired under full-field imaging conditions using a commercially available flat-panel based digital mammography system (Senographe 2000D, GE Medical Systems, Milwaukee, WI) [35]. A boxcar smoothing filter was applied to the dual energy image, a median filter to the high energy image before its use for the computation of the dual energy image, and an adaptation of the Kalender’s [64] correlated noise reduction (KNR) technique to the dual energy image. A breast tissue equivalent slab phantom of 5 cm thick, enclosing calcium carbonate crystals of various sizes to simulate calcifications was used for the evaluation of the study. The slab phantom had continuously varying glandular tissue ratio along its length in order to evaluate the study for different glandularities. The noise reducing techniques were compared in the means of the root-mean-square signal in background regions, when no calcifications present, of the dual energy calcification images and the contrast-to-noise ratio values of the calcifications in the dual energy calcification images. The results showed that the KNR method provided the most effective reduction of image noise with simultaneous increase of the contrast-to-noise ratio value. In order for a calcification to be visible, the contrast-to-noise ratio value should be equal or exceed the value of 4. The minimum visible calcification size that ranged from 300 μm to 355 μm for standard dual energy calcification images was decreased to about 250 μm when both KNR and high energy median filter were applied. The noise reduction techniques were also verified with dual energy images of an animal tissue phantom consisting calcifications and concluded that noise reduction techniques improved significantly the calcification dual energy images [35].
Ducote and Molloi carried out a quantitative method to characterize the accuracy of measuring the breast density with dual energy mammography [65]. A Tungsten anode X-ray tube with a 50 μm Rhodium and 300 μm Copper beam filters were used for the acquisition of the low- and high-energy images, respectively. Several phantom thicknesses, densities, sizes, and shapes were measured. The four constructed phantoms were also used for breast density measurement error calculations. The effect of dose on measuring breast density was also examined. All the acquired images were undergone scatter correction. The root-mean-square error in breast density measurements were: (i) 0.44% for the examined variable thickness phantoms, (ii) 0.64% for the variable density phantoms, (iii) 2.87% for the phantoms of different areal sizes, and (iv) 4.63% for step phantoms designed to mimic the shape of a breast. Thus, the results indicated that dual energy mammography could be used for breast density measurement with an overall root-mean-square error of approximately 5% and can be implemented with only few changes compared to conventional mammography [65].
Koukou et al. presented an experimental dual energy method in order to visualize microcalcifications [26]. A modified Tungsten anode radiographic X-ray tube operating at 40 kV with 100 μm Cadmium and 70 kV with 1000 μm Copper for the low- and high-energy, respectively. The X-ray tube was combined with a high-resolution CMOS active pixel sensor (pixel pitch of 22.5 μm), coupled with a 33.91 mg/cm2 terbium-doped gadolinium oxysulfide (Gd2O2S:Tb) [66,67] scintillator screen. Custom-made homogenous and inhomogeneous breast phantoms and two different calcification phantoms (Figure 3a) were constructed with various calcification thicknesses ranging from 16 μm to 152 μm. The American College of Radiology (ACR) mammography accreditation phantom [68] was also examined in this study (Figure 4). The mean glandular dose and the contrast-to-noise ratio were calculated from the dual energy subtracted images for various entrance surface doses. A calcification thickness of 152 μm was visible in the standard dual energy image, with mean glandular doses within the acceptable levels (below 3 mGy). The minimum visible calcification thickness was reduced to 93 μm with a mean glandular dose of 1.62 mGy after post-processing on the dual energy images obtained from the inhomogeneous phantom. Due to the small pixel pitch of the sensor used the pixel binning method was allowed to be applied in the final dual energy images increasing the contrast-to-noise ratio. With pixel binning method the signal is averaged after it was read-out in squares of neighboring pixels. They concluded that the proposed dual energy method could potentially improve the visibility of calcifications in dual energy image [26].
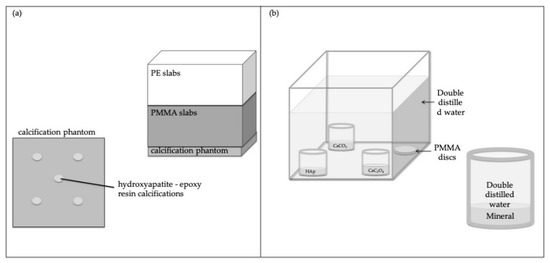
Figure 3.
Schematic representation of the used phantoms in the experimental studies [26,28]; (a,b) calcification for dual energy mammography technique.
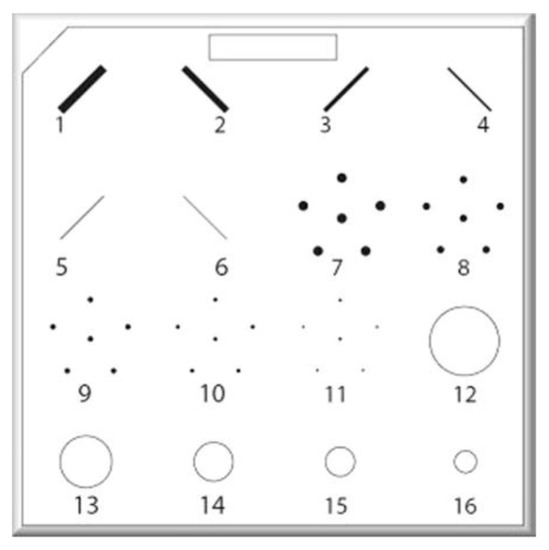
Figure 4.
American College of Radiology (ACR) accreditation phantom: fibers 1–6, calcification clusters 7–11, and masses 12–16.
Koukou et al. evaluated a dual energy method, previously developed by that group [26], on a breast cancer specimen [27]. A modified Tungsten anode radiographic X-ray tube combined with a high-resolution complementary metal-oxide semiconductor active pixel sensor [61,62,63,67] X-ray detector was used. The spectral combination used was 40 kV with 100 μm Cadmium and 70 kV with 1000 μm Copper for the low- and high-energy, respectively. The dual energy images obtained from a formalin-fixed breast cancer specimen for various entrance surface doses were compared to standard mammographic image of the specimen. The mean glandular dose values calculated in this study (1.62 to 2.39 mGy) were within the acceptable levels for mammography. Initial results demonstrated that the dual energy images were directly comparable with the mammographic image. Additionally, it was identified similar or even increased calcification information by experienced radiologists [27].
Martini et al. presented a dual energy X-ray method for the characterization of minerals associated with pathogenesis [28]. According to the literature, calcifications are divided into Type I and Type II [69,70,71,72,73,74,75]. The calcifications of Type I are composed calcium oxalate (CaC2O4) crystals [76] and are found to be associated with benign lesions or mostly non-invasive lobular carcinoma in situ [77,78]. The calcifications of Type II are composed of calcium phosphate, mainly hydroxyapatite (Hap) crystals [76,79,80,81] and in some cases of calcium carbonate (CaCO3). Hydroxyapatite is associated with malignancy including carcinomas, while calcium carbonate crystals [82,83,84,85,86] with benignancy [44,45,70,87]. An analytical model using monoenergetic and polyenergetic X-ray beams was developed to determine the Calcium/Phosphorus mass ratio (mCa/mP). The effective mCa/mP was calculated for various calcification thicknesses (100–1000 μm) and types (CaC2O4, CaCO3, HAp) in the simulation study carried out. The optimized irradiation conditions obtained from the simulation were used in the experimental evaluation of the study. The X-ray systems that were used for the experimental verification were Tungsten anode X-ray tubes combined with energy dispersive and energy integrating (imaging) detectors. For the single exposure technique was used a Tungsten anode Norland XR-46 (Norland Medical Systems Inc., Fort Atkinson, WI) combined with a Cadmium-Telluride (CdTe) X-ray energy discriminating and counting system (AMPTEK XR-100T). As for the double exposure technique, the Del Medical Eureka Tungsten anode system was used, combined with a high-resolution CMOS active pixel sensor (pixel pitch of 22.5 μm), coupled with a 33.91 mg/cm2 terbium-doped gadolinium oxysulfide (Gd2O2S:Tb) [61,62,63,67] scintillator screen. The effective mCa/mP was determined in custom-made phantoms containing calcifications of all three aforementioned mineral types (Figure 3b) and thicknesses ranging from 300 to 900 μm at 200 μm increments. The proposed method is capable of discriminating HAp and CaCO3 or Hap and CaC2O4 (i.e., malignancy (HAp), and benignancy (CaCO3 and CaC2O4)) for calcification thicknesses of 300 μm or higher, with MGD of 3.29 and 3.25 mGy for the single and double exposure technique respectively, since there was found statistically significant difference (p < 0.05) between the different types of minerals [28].
The Code of Federal Regulations suggests that the average glandular dose that should be delivered during a single craniocaudal view, when irradiating an FDA-accepted phantom simulating a standard breast, shall not exceed 3 mGy per exposure [88]. Table 2 summarizes the European Guidelines for the maximum average glandular doses to equivalent breast thicknesses. As for the mean glandular dose for standard breast, its value should not exceed 2.5 mGy [89].
Table 2.
European Guidelines for maximum average glandular doses.
Figure 1 illustrates schematic representations phantoms used in the experimental studies phantoms. The phantoms represent tumor-like lesions Figure 1a,b [34,56], iodine concentration for dual energy contrast enhanced mammography technique Figure 1c and Figure 2a [22,29,60], and calcification for dual energy mammography technique Figure 2b,c and Figure 3a,b [8,9,24,26,28].
5.1. Noise Reduction Techniques
Several studies presented above [25,35,42] used noise reduction techniques in order to enhance their findings in the final dual energy image. The noise reduction techniques that were used are the following.
5.2. Boxcar Filter
The Boxcar filter is an elementary technique for noise reduction resulting in a smoothed 2D image. The result of boxcar filtering is a smoothed dual energy image. A two-dimensional boxcar average filter with defined kernel size was applied as follows [35]:
where w is the size of the kernel used, DL and DH are the optical densities of the low- and high-energy images, and t′c is the boxcar filtered image.
5.3. Kalender’s Noise Reduction Technique (KNR)
Kalender et al. [64] working on dual energy computed tomography established a noise reduction algorithm. This noise reduction algorithm used the (anti)correlation for the components of the noise [20,35,55,90]. The dual energy glandular ratio image was filtered with a highpass filter in order to measure the correlated noise. The final KNR-filtered image was obtained after the summation of the highpass filtered dual energy glandular ratio image and the unprocessed dual energy image. The final KNR-filtered image was obtained using the following formula:
where s is the weighting factor, and gr is the dual energy glandular ratio image.
5.4. High Energy Median Filter
The application of a median filter [91] on the high energy image only was an option for smoothing the final dual energy image in some cases [35]. The formula used was the following.
where w is the size of the kernel used, and D′H is the median filtered high energy image.
6. Clinical Practice
Lewin et al. studied the potential of dual energy contrast enhanced technique in indicating breast cancers [92]. The mediolateral oblique (MLO) low- and high- energy images were acquired with a full-field digital mammography system (Senographe 2000D; GE Medical Systems, Milwaukee, Wis). The technique was implemented in 26 women requiring biopsy according to mammographic or clinical findings, where 13 of them had invasive cancers. The women were injected with 100 mL iohexol with 350 mg of iodine per milliliter. After administrating the iodinated contrast agent and applying the dual energy contrast enhanced technique, 11 tumors were strongly enhanced, 1 was enhanced to some extent, and 1 was poorly enhanced. The duct of a ductal carcinoma in situ tested was also poorly enhanced [92].
Dromain et al. worked on the estimation the accuracy of dual energy contrast enhanced digital mammography in addition to mammography versus mammography alone and versus mammography plus ultrasound [37]. In their study, 120 women with 142 suspect findings on mammography and/or ultrasound underwent dual energy contrast enhanced digital mammography. A pair of low- and high-energy images was acquired using a modified full-field digital mammography system (GE Healthcare Senographe DS (Chalfont St. Giles, UK)) (Figure 5a). The MLO and craniocaudal (CC) images were acquired at 2 minutes and 4 minutes, respectively, after the injection of 1.5 ml/kg of an iodinated contrast agent. The mammography, ultrasound and dual energy contrast enhanced digital mammography images were evaluated by one reader during 2 sessions 1 month apart. Sensitivity, specificity, and area under the receiver operating characteristic (ROC) curve were estimated. The results according to pathology and follow-up indicated 62 benign and 80 malignant lesions. The areas under the ROC curves were significantly superior for mammography plus dual energy contrast enhanced digital mammography than it was for mammography alone and for mammography plus ultrasound using Breast Imaging Reporting and Data System (BI-RADS). The sensitivity was higher for mammography plus contrast enhanced digital mammography than it was for mammography (93% versus 78%; p < 0.001) with no loss in specificity. Mammography plus contrast enhanced digital mammography detected all the 23 multifocal lesions correctly, while mammography and ultrasound detected 16 and 15 lesions, respectively [37].

Figure 5.
Commercial digital mammography systems employed for dual energy techniques in clinical practice studies: (a) Senographe DS, (b) Senographe Essential, and (c) Mammomat Inspiration [99,100,101,102].
Dromain et al. compared the dual energy contrast enhanced digital mammography as an adjunct to mammography plus ultrasonography with mammography plus ultrasonography alone in terms of diagnostic accuracy [23]. For the implementation of the study 110 women with 148 breast lesions went through two-view dual energy contrast enhance digital mammography, additionally to mammography and ultrasonography, using a specially modified digital mammography system (Senographe DS, GE Healthcare) (Figure 5a). Among the 148 breast lesions, 84 were malignant and 64 benign. For 138 lesions the reference standard was histology and for 12 lesions follow-up. Confidence of presence, probability of cancer, as well as BI-RADS scores were assessed for each finding. Sensitivity, specificity and ROC curve areas were estimated for each of the four reader and overall. The per lesion sensitivity to malignant breast lesions of all readers was improved for the dual energy contrast enhanced digital mammography as an adjunct to mammography plus ultrasonography compared to mammography plus ultrasonography alone (0.78 versus 0.71 using BI-RADS, p = 0.006). For all readers the clinical performance was improved and the average area under the ROC curve was significantly superior for contrast enhanced digital mammography as an adjunct to mammography plus ultrasonography than for mammography plus ultrasonography alone (0.87 versus 0.83, p = 0.045). In 80% of the cases, similar or improved visibility of breast lesions was indicated on contrast enhanced digital mammography as an adjunct to mammography compared to mammography plus ultrasonography [23].
Jochelson et al. explored the potential of bilateral dual energy contrast enhanced digital mammography in tumor identification and compared dual energy contrast enhanced digital mammography with conventional digital mammography and breast magnetic resonance imaging in women with newly diagnosed breast cancer [93]. Ten (10) women were injected with 1.5 mL per kilogram of body weight of iohexol in order to evaluate the feasibility of their study. The images were acquired between 2.5 and 10 min after injection. After the feasibility confirmation, 52 women with newly diagnosed cancer that had undergone breast magnetic resonance imaging, underwent dual energy contrast enhanced digital mammography. The two images in each view for dual energy contrast enhanced digital mammography were acquired with a digital mammography unit (Senographe DS; GE, Buc, France) (Figure 5a). The results showed that the tumors were enhanced regardless the timing of agent injection, which was up to 10 minutes. Magnetic resonance imaging and dual energy contrast enhanced digital mammography both depicted 50 (96%) of 52 index malignant tumors, while conventional mammography depicted 42 (81%). Dual energy contrast enhanced digital mammography visualized lesions raging from 4 mm to 67 mm in size (median: 17 mm). Magnetic resonance imaging depicted 22 out of 25 (88%) additional ipsilateral cancers and contrast enhanced digital mammography 14 of out 25 (56%). Although the sensitivity of dual energy contrast enhanced digital mammography was lower than the one of magnetic resonance imaging in detecting additional ipsilateral cancers, revealed higher specificity [93].
Cheung et al. analyzed the efficiency of dual energy contrast enhanced spectral mammography in dense breasts compared to contrast enhanced subtracted mammography and conventional mammography [94]. The dual energy contrast enhanced spectral mammography used in this work was a commercial unit developed by GE Healthcare (Senographe Essential CESM, Buc, France) (Figure 5b). Contrast enhanced spectral mammography cases of dense breasts, with histological proof, were assessed in their study. Four experienced radiologists in mammography interpretation blindly read mammography first, and then dual energy contrast enhanced spectral mammography. The diagnostic profiles, consistency and learning curve were analyzed statistically. The 100 lesions (28 benign and 72 breast malignancies) of 89 women were analyzed in this work. With the use of dual energy contrast enhanced spectral mammography cancer diagnosis was improved by 21.2% in sensitivity (71.5% to 92.7%), by 16.1% in specificity (51.8% to 67.9%) and by 19.8% in accuracy (65.9% to 85.8%) compared with conventional mammography. The interobserver diagnostic consistency was markedly higher using dual energy contrast enhanced spectral mammography than using mammography alone (0.6235 versus 0.3869 using the kappa ratio). After 75 consecutive case readings the probability of a correct prediction raised from 80% to 90% [94].
Cheung et al. assessed the potential of dual energy contrast enhanced spectral mammography to evaluate malignant microcalcifications [95]. The dual energy contrast enhanced spectral mammography used in this work was a commercial unit developed by GE Healthcare (Senographe Essential CESM, Buc, France) (Figure 5b). From 2056 dual energy contrast enhanced spectral mammography cases reviewed, 59 cases fulfilled the following criteria and analyzed: (i) suspicious malignant microcalcifications (BI-RADS 4) on mammogram, (ii) no related mass, (iii) with pathological diagnoses. The microcalcification morphology and associated enhancement were taken into consideration in order to analyze the accuracy of the diagnosis and the cancer size measurements compared to the results of pathology. Out of the 59 microcalcifications, 22 were diagnosed as cancers, 19 were atypical lesions and 18 were benign lesions. 20 cancers (76.9%), 3 atypia (11.55%) and 3 benign lesions (11.55%) revealed enhancement. The true-positive rate of intermediate- and high- concern microcalcifications was 93.75%, while of low-concern lesions it was 50%. In general, the diagnostic sensitivity of enhancement was 90.9%, with 83.78% specificity, 76.92% positive predictive value, 93.94% negative predictive value and 86.4% accuracy [95].
Knogler et al. studied the feasibility of contrast enhanced dual energy mammography by introducing Titanium filtering at 49 kVp for high energy images and using an artefact reducing image subtraction post-processing algorithm [96]. In this study, 15 patients with suspicious findings (ACR BIRADS 4 and 5) detected on digital mammograms were undergone contrast enhanced dual energy mammography with a modified prototype Siemens Mammomat Inspiration full-field digital mammography (FFDM) unit (Siemens Healthcare) (Figure 5c). Subtracted contrast enhanced dual energy mammography images were obtained from a fully automatic, locally adjusted tissue thickness-dependent subtraction factor in order to prevent the subtracted images from over-subtraction at the breast border. The mammography and contrast enhanced dual energy mammography images were evaluated by two observers according to ACR BI-RADS in two reading sessions. The results were compared with those of histopathology. From the 15 patients included in the study, 7 were found with benign findings and 8 with malignant. Strong contrast enhancement was identified by all malignant lesions. With the addition of contrast enhanced dual energy mammography the BI-RADS assessment was altered in 66.6%, leading to a general increase in the accuracy. Contrast enhanced dual energy mammography also revealed additional lesions and reduced the false-positive rate compared to mammography [96].
Knogler et al. used BI-RADS descriptors of contrast enhanced magnetic resonance imaging for the assessment of contrast enhanced dual energy mammography mass lesion images. 11 women with suspicious mass lesions on their mammograms (BI-RADS 4 or 5) were included [97]. The contrast enhanced dual energy mammography images were obtained from a modified Siemens Mammomat Inspiration unit (Siemens Healthcare) (Figure 5c). All images were blindly assessed by 2 breast radiologists in 2 sessions. The criteria used were related to morphology and contrast enhancement intensity according to the BI-RADS lexicon. Histopathology was used as the standard of reference. 5 women with benign lesions and 6 malignant were included in the study. In all malignant cases, the enhancement of both contrast enhanced magnetic resonance imaging and contrast enhanced dual energy mammography were similar. In the cases were benign lesions were examined, contrast enhanced magnetic resonance imaging revealed stronger enhancement compared to contrast enhanced dual energy mammography. Discrepancies in the BI-RADS descriptors did not influence the final BI-RADS score, which was almost equal in all cases. 1 malignant lesion was rated BI-RADS 4 with contrast enhanced dual energy mammography and BI-RADS 5 with contrast enhanced magnetic resonance imaging, and 1 benign was rated BI-RADS 2 and BIRADS 1, respectively [97].
Sung et al. evaluated the performance of contrast enhanced digital mammography for breast cancer screening [98]. In this study, 904 women undergone contrast enhanced digital mammography with a commercially available digital mammography unit (Senographe Essential; GE Medical Systems, Milwaukee, Wis) (Figure 5b) after their medical records’ review for age, risk factors, short-interval follow-up and biopsies recommended, and cancers detected. For all cases were determined the sensitivity, specificity, positive predictive value of abnormal findings at screening, positive predictive value of biopsy performed, and negative predictive value. From the 904 women, 700 (77.4%) had dense breasts, 247 (27.3%) had a family history of breast cancer in a first-degree relative age 50 years or younger, and 363 (40.2%) a personal history of breast cancer. BI-RADS 1 or 2 was scored in 832 of 904 (92.0%) women, BI-RADS 3 in 25 of 904 (2.8%) women, and BI-RADS 4 or 5 in 47 of 904 (5.2%) women. The use of contrast enhanced digital mammography resulted in the diagnosis of 15 cancers in 14 of 904 women (cancer detection rate, 15.5 of 1000). The positive predictive value of biopsy performed was 29.4% (15 of 51). At least 1-year follow up was available in 858 women. The sensitivity was 50.0% (eight of 16; 95% confidence interval: 24.7%, 75.3%) on the low energy images compared with 87.5% (14 of 16; 95% confidence interval: 61.7%, 98.4%) for the entire study (low energy and iodine images; P = 0.03). The specificity was 93.7% (789 of 842; 95% confidence interval: 91.8%, 95.2%); positive predictive value of abnormal findings at screening was 20.9% (14 of 67; 95% confidence interval: 11.9%, 32.6%), and negative predictive value was 99.7% (789 of 791; 95% confidence interval: 99.09%, 99.97%) [98].
7. Conclusions
Breast cancer is one of the leading causes of death worldwide [1,2]. The potential of diagnosing breast cancer in early stages through screening and adequate follow-up of women with positive findings could significantly reduce breast cancer mortality (by 15–25%) [6]. Furthermore, early detection could lead to more effective treatment planning and medication [3,4,5] based on the stage for each patient individually [3,4,5]. Even though X-ray mammography is the gold standard method for early detection of breast carcinomas, ultrasound and digital tomosynthesis have also been used in diagnosing breast cancer [11,12,13,14]. Suspicious findings (such as masses, areas of distortion, calcification minerals) that cannot be detected by physical examination and they can be visible on mammograms [15], are often obscured by overlapping tissue. Dual energy technique suppresses the contrast between adipose and glandular tissues leading to enhancement of pathogenesis that is not present in screening mammography [16]. Regardless the method (i.e., subtraction, contrast enhanced with iodine) used to obtain the dual energy image, the results of the studies (simulation and experimental) adopting the dual energy technique are very promising.
According to several studies, the type of calcification crystals present in a mammogram may indicate malignancy and disease state [85,86,87]. Simulation studies were conducted by following the analytical modeling developed by Lemacks et al. [20]. Both minimum microcalcification size [20,21] or thickness [25] detection [20,21,25] and visualization were explored [42,43]. To this aim, a modified Monte Carlo code was also used. Based on extensive research for the X-ray tube high voltage, filter material/thickness and entrance dose, they concluded to the optimum irradiation conditions. Lemacks et al. was able to detect calcification sizes of 250 μm [20]. Although Brandan and Ramirez used the analytical model employed by Lemacks et al. [20], they resulted in a difference in the contrast-to-noise ratio values of 40% up to 70% [21]. These differences are attributed to different considerations between the two studies. Del Lama et al. [42,43] with the use of the modified Monte Carlo code were able to visualize microcalcifications of 200 μm. Koukou et al. [25] used the analytical model of Lemacks et al. [20] investigating the possibility of detecting microcalcifications by using radiographic X-ray spectra. The results showed that a microcalcification thickness of 150 μm could be achieved [25]. Since the glandularity of breast is also a risk factor for breast cancer, Ducote and Molloi explored the potential of glandularity measurements with the use of dual energy mammography [41]. According to the results of this study, the dual energy technique is capable of measuring breast density [41]. Based on such promising results, some of the aforementioned teams evaluated their methods in future studies [25,41].
Kappadath and Shaw used the formalism of Lemacks et al. [20] in order to investigate whether the calcification thickness and glandular ratio could be estimated through analytical functions [24]. This study was extended for different calcification thicknesses and glandular ratios [8,9] and the use of different noise reduction techniques [35]. After noise reduction techniques were applied, the visibility of calcification size decreased from 300 to 355 μm to 250 μm [35]. Koukou et al. [26] were able to visualize calcifications with thickness of 152 μm. Post-processing led Koukou et al. [26] to decrease the calcification thickness that can be visualized at 93 μm. A step forward of this method was the comparison of the dual energy image to standard mammography image of a breast cancer specimen [27]. The results indicated that the dual energy images of the method were directly comparable with the mammographic image and revealed similar or even increased calcification information according to experienced radiologists [27]. The use of balanced filtering in dual energy technique was applied by Saito [29] in order to achieve a signal-to-noise ratio of 5 in the final dual energy subtracted iodine image. Although the appearance of calcifications may indicate breast cancer, the consistency of calcifications will indicate whether they are associated with malignancy or benignancy [69,70,71,72,73,74,75,76,77,78,79,80,81,87]. Martini et al. [28] worked on the differentiation of calcifications consisting of minerals found to indicate malignancy and benignancy according to literature [103,104,105]. The proposed method of Martini et al. [28] led to the differentiation of 300 μm thick calcifications or higher. The different types of minerals were found to have statistically significant difference (p < 0.05). The cancellation of the cluttered background was also investigated by Marziani et al. [56] and Taibi et al. [34], since the capability of cancelling out the background will reveal the lesions, calcifications and distortions in general. Taibi et al. [34] were able to detect tumor-like lesions embedded in clutter background. The contrast enhanced dual energy mammography was applied for the investigation of the minimum iodine concentration able to significantly enhance the detectability of the pathology [22,60]. Ducote and Molloi [65] measured the breast density with the use of dual energy mammography with an overall root-mean-square error of approximately 5%. All these studies achieved to visualize calcifications of small sizes or thicknesses discriminate whether their minerals are associated with malignancy or benignancy and measured the breast density. These studies proved that dual energy technique is capable of providing information that may help to find breast cancer in early stages or even give a hint of breast cancer.
The dual energy contrast enhanced technique was used in clinical practice. Women with breast lesions undergone dual energy contrast enhanced mammography [23,37,92,93,94,95,96,97,98]. The results of all studies indicated that dual energy contrast enhanced technique could improve the visibility of breast lesions. When the dual energy contrast enhanced technique was combined with mammography, both sensitivity and specificity were higher compared to the results obtained from standard mammography. Additionally, the false positive findings were decreased indicating that dual energy contrast enhanced mammography can lead to less recall rates.
Dual energy methods are not established in clinical practice yet. The absorbed dose in dual energy, in terms of MGD, is ranging from 2 to 3.52 mGy, where MGD must not exceed 2.5 mGy [89]. These results are higher comparing to conventional mammography. However, application of the dual energy method in clinical practice will reveal the benefits in diagnosis against the increased dose. In this approach the ability of the dual energy methods to require longer time intervals between necessary dual energy mammographs must be taken into account. Additionally, in the calcification minerals characterization method proposed by Martini et al. [28], the second irradiation, as proposed by the authors can be restricted in a small area surrounding the suspected calcification. In this approach the MGD and entrance skin dose are comparable to conventional mammography.
The dual energy technique has the advantage to reveal pathogenesis that was obscured by overlapping tissue since it cancels out tissue structures. The potential of visualizing masses, areas of distortion, calcifications and studying the impact of breast density was the aim for the studies presented in this review paper. Since breast cancer is one of the most important health problems, a technique that could assist physicians to identify suspicious findings in early stages would be of great importance. Mammography is the gold standard; however dual energy technique could be an adjunct for more accurate diagnose. The results of the studies presented in this paper show the impact of dual energy technique not only on early diagnose but also on elimination of unneeded biopsies women undergo.
Author Contributions
Conceptualization, N.M., V.K., C.M. and G.F.; methodology, N.M., V.K., C.M. and G.F.; software, N.M. and V.K.; validation, N.M., V.K., C.M. and G.F.; formal analysis, N.M., V.K., C.M. and G.F.; investigation, N.M. and V.K.; resources, N.M. and V.K.; data curation, N.M., V.K., C.M. and G.F.; writing—original draft preparation, N.M., V.K. and C.M; writing—review and editing, N.M., V.K., C.M. and G.F.; visualization, N.M., and V.K.; supervision, C.M. and G.F.; project administration, C.M and G.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2012. Cancer J. Clin. 2012, 62, 10–29. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Cancer Report 2014; WHO: Geneva, Switzerland, 2014. [Google Scholar]
- American Cancer Society. Breast Cancer Facts and Figures 2011–2012; American Cancer Society: Atlanta, GA, USA, 2011. [Google Scholar]
- Seyyedi, S.; Cengiz, K.; Kamasak, M.; Yildirim, I. An object oriented simulator for 3D digital breast tomosynthesis imaging system. Comput. Math. Methods Med. 2013, 2013, 250689. [Google Scholar] [CrossRef] [PubMed]
- Mert, A.; Kılıc, N.; Bilgili, E.; Akan, A. Breast cancer detection with reduced feature set. Comput. Math. Methods Med. 2015, 2015, 265138. Available online: https://www.hindawi.com/journals/cmmm/2015/265138/ (accessed on 12 March 2020). [CrossRef] [PubMed]
- World Health Organization. World Health Statistics 2008; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Roberts, M.; Kahn, E.; Haddawy, P. Development of a Bayesian Network for Diagnosis of Breast Cancer; IJCAI-95 Workshop on Building Probabilistic Networks: Montréal, QC, Canada, 1995. [Google Scholar]
- Kappadath, S.C.; Shaw, C.C. Quantitative evaluation of dual-energy digital mammography for calcification imaging. Phys. Med. Biol. 2004, 49, 2563–2576. [Google Scholar] [CrossRef] [PubMed]
- Kappadath, S.C.; Shaw, C.C. Dual-energy digital mammography for calcification imaging: Scatter and nonuniformity corrections. Med. Phys. 2005, 32, 3395–3408. [Google Scholar] [CrossRef] [PubMed]
- Cox, R.F.; Morgan, P. Microcalcifications in breast cancer: Lessons from physiological mineralization. Bone 2013, 53, 437–450. [Google Scholar] [CrossRef]
- Cheng, H.D.; Cai, X.; Chen, X.; Hu, L.; Lou, X. Computer aided detection and classification of microcalcifications in mammograms: A survey. Pattern Recognit. 2003, 36, 2967–2991. [Google Scholar] [CrossRef]
- Majid, A.S.; de Paredes, E.S.; Doherty, R.D.; Sharma, N.R.; Salvador, X. Missed breast carcinoma: Pitfalls and pearls. Radiographics 2003, 23, 881–895. [Google Scholar] [CrossRef]
- Youk, J.H.; Kim, E.K.; Kim, M.J.; Kwak, J.Y.; Son, E.J. Performance of hand-held whole-breast ultrasound based on BI-RADS in women with mammographically negative dense breast. Eur. Radiol. 2011, 21, 667–675. [Google Scholar] [CrossRef]
- Loukas, C.; Kostopoulos, S.; Tanoglidi, A.; Glotsos, D.; Sfikas, C.; Cavouras, D. Breast cancer characterization based on image classification of tissue sections visualized under low magnification. Comput. Math. Methods Med. 2013, 2013, 829461. [Google Scholar] [CrossRef]
- Stone, N.; Matousek, P. Advanced transmission Raman spectroscopy: A promising tool for breast disease diagnosis. Cancer Res. 2008, 68, 4424–4430. [Google Scholar] [CrossRef] [PubMed]
- Taibi, A.; Vecchio, S. Breast Imaging. In Comprehensive Biomedical Physics; Elsevier: Amsterdam, The Netherlands, 2014; Volume 2, pp. 121–154. [Google Scholar]
- Sorenson, J.A.; Duke, P.R.; Smith, S.W. Simulation studies of dual energy X-ray absorptiometry. Med. Phys. 1989, 16, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Blake, G.M.; Fogelman, I. Technical Principles of dual energy X-ray absorptiometry. Semin. Nucl. Med. 1997, 27, 210–228. [Google Scholar] [CrossRef]
- Beaman, S.A.; Lillicrap, S.C. Optimum X-ray spectra for mammography. Phys. Med. Biol. 1982, 27, 1209–1220. [Google Scholar] [CrossRef] [PubMed]
- Lemacks, M.R.; Kappadath, S.C.; Shaw, C.C.; Liu, X.; Whitman, G.J. A dual-energy subtraction technique for microcalcification imaging in digital mammography—A signal-to-noise analysis. Med. Phys. 2002, 29, 1739–1751. [Google Scholar] [CrossRef]
- Brandan, M.E.; Ramirez, V.R. Evaluation of dual-energy subtraction of digital mammography images under conditions found in a commercial unit. Phys. Med. Biol. 2006, 51, 2307–2320. [Google Scholar] [CrossRef]
- Baldelli, P.; Bravin, A.; Di Maggio, C.; Gennaro, G.; Gambaccini, M.; Sarnelli, A.; Taibi, A. Evaluation of the minimum iodine concentration for contrast enhanced subtraction mammography. Nucl. Instrum. Methods Phys. Res. A 2007, 580, 1115–1118. [Google Scholar] [CrossRef]
- Dromain, C.; Thibault, F.; Diekmann, F.; Fallenberg, E.; Jong, R.; Koomen, M.; Hendrick, R.E.; Tarvidon, A.; Toledano, A. Dual-energy contrast-enhanced digital mammography: Initial clinical results of a multireader, multicase study. Breast Cancer Res. 2012, 14, R94. [Google Scholar] [CrossRef]
- Kappadath, S.C.; Shaw, C.C. Dual-energy digital mammography: Calibration and inverse-mapping technique to estimate calcification thickness and glandular-tissue ratio. Med. Phys. 2003, 30, 1110–1117. [Google Scholar] [CrossRef]
- Koukou, V.; Martini, N.; Michail, C.; Sotiropoulou, P.; Fountzoula, C.; Kalyvas, N.; Kandarakis, I.; Nikiforidis, G.; Fountos, G. Dual Energy Method for Breast Imaging: A Simulation Study. Comput. Math. Methods Med. 2015, 2015, 574238. [Google Scholar] [CrossRef]
- Koukou, V.; Martini, N.; Fountos, G.; Michail, C.; Sotiropoulou, P.; Bakas, A.; Kalyvas, N.; Kandarakis, I.; Speller, R.; Nikiforidis, G. Dual energy subtraction method for breast calcification imaging. Nucl. Instrum. Methods Phys. Res. A 2017, 848, 31–38. [Google Scholar] [CrossRef]
- Koukou, V.; Martini, N.; Fountos, G.; Michail, C.; Bakas, A.; Oikonomou, G.; Kandarakis, I.; Nikiforidis, G. Application of a dual energy X-ray imaging method on breast specimen. Results Phys. 2017, 7, 1634–1636. [Google Scholar] [CrossRef]
- Martini, N.; Koukou, V.; Fountos, G.; Michail, C.; Bakas, A.; Kandarakis, I.; Speller, R.; Nikiforidis, G. Characterization of breast calcification types using dual energy X-ray method. Phys. Med. Biol. 2017, 62, 7741–7764. [Google Scholar] [CrossRef] [PubMed]
- Saito, M. Dual-energy approach to contrast-enhanced mammography using the balanced filter method: Spectral optimization and preliminary phantom measurements. Med. Phys. 2007, 34, 4236–4246. [Google Scholar] [CrossRef] [PubMed]
- Ross, P.A. A new method of spectroscopy for faint X-radiations. J. Opt. Soc. Am. 1928, 16, 433–438. [Google Scholar] [CrossRef]
- Johns, P.C.; Yaffe, M.J. Theoretical optimization of dual-energy X-ray imaging with application to mammography. Med. Phys. 1985, 12, 289–296. [Google Scholar] [CrossRef]
- Boone, J.M.; Shaber, G.S.; Tecotzky, M. Dual-energy mammography: A detector analysis. Med. Phys. 1990, 17, 665–675. [Google Scholar] [CrossRef]
- Brettle, D.S.; Cowen, A.R. Dual-energy digital mammography utilizing stimulated phosphor computed radiography. Phys. Med. Biol. 1994, 39, 1984–2004. [Google Scholar] [CrossRef]
- Taibi, A.; Fabbri, S.; Baldelli, P.; di Maggio, C.; Gennaro, G.; Marziani, M.; Tuffanelli, A.; Gambaccini, M. Dual-energy imaging in full-field digital mammography: A phantom study. Phys. Med. Biol. 2003, 48, 1945–1956. [Google Scholar] [CrossRef]
- Kappadath, S.C.; Shaw, C.C. Dual-energy mammography for calcification imaging: Noise reduction techniques. Phys. Med. Biol. 2008, 53, 5421–5443. [Google Scholar] [CrossRef]
- Dromain, C.; Balleyguier, C.; Adler, G.; Garbay, J.R.; Delaloge, S. Contrast-enhanced digital mammography. Eur. J. Radiol. 2009, 69, 34–42. [Google Scholar] [CrossRef]
- Dromain, C.; Thibault, F.; Muller, S.; Rimareix, F.; Delaloge, S.; Tardivon, A.; Balleyguier, C. Dual-energy contrast-enhanced digital mammography: Initial clinical results. Eur. Radiol. 2011, 21, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Michail, C.; Karpetas, G.; Kalyvas, N.; Valais, I.; Kandarakis, I.; Agavanakis, K.; Panayiotakis, G.; Fountos, G. Information Capacity of Positron Emission Tomography Scanners. Crystals 2018, 8, 459. [Google Scholar] [CrossRef]
- Michail, C.; Kalyvas, N.; Bakas, A.; Ninos, K.; Sianoudis, I.; Fountos, G.; Kandarakis, I.; Panayiotakis, G.; Valais, I. Absolute Luminescence Efficiency of Europium-Doped Calcium Fluoride (CaF2:Eu) Single Crystals under X-ray Excitation. Crystals 2019, 9, 234. [Google Scholar] [CrossRef]
- Saatsakis, G.; Kalyvas, N.; Michail, C.; Ninos, K.; Bakas, A.; Fountzoula, C.; Sianoudis, I.; Karpetas, G.E.; Fountos, G.; Kandarakis, I.; et al. Optical Characteristics of ZnCulnS/ZnS (Core/Shell) Nanocrystal Flexible Films Under X-ray Excitation. Crystals 2019, 9, 343. [Google Scholar] [CrossRef]
- Ducote, J.L.; Molloi, S. Quantification of breast density with dual energy mammography: A simulation study. Med. Phys. 2008, 35, 5411–5418. [Google Scholar] [CrossRef] [PubMed]
- Del Lama, L.S.; Godeli, J.; Poletti, M.E. Monte Carlo simulation studies for the determination of microcalcification thickness and glandular ratio through dual-energy mammography. Radiat. Phys. Chem. 2017, 137, 157–162. [Google Scholar] [CrossRef]
- Del Lama, L.S.; Cunha, D.M.; Poletti, M.E. Validation of modified PENELOPE Monte Carlo code for applications in digital and dual-energy mammography. Radiat. Phys. Chem. 2017, 137, 151–156. [Google Scholar] [CrossRef]
- Frappart, L.; Boudeulle, M.; Boumendil, J.; Lin, H.C.; Martinon, I.; Palayer, C.; Mallet-Guy, Y.; Raudrant, D.; Bremond, A.; Rochet, Y.; et al. Structure and composition of microcalcifications in benign and malignant lesions of the breast: Study by light microscopy, microprobe analysis, and X-ray diffraction. Hum. Pathol. 1984, 15, 880–889. [Google Scholar] [CrossRef]
- Haka, A.S.; Shafer-Peltier, K.E.; Fitzmaurice, M.; Crowe, J.; Dasari, R.R.; Feld, M.S. Identifying microcalcifications in benign and malignant breast lesions by probing differences in their chemical composition using Raman spectroscopy. Cancer Res. 2002, 62, 5375–5380. [Google Scholar]
- Chan, H.; Doi, K. Physical characteristics of scattered radiation in diagnostic radiology: Monte Carlo simulation studies. Med. Phys. 1985, 12, 152–165. [Google Scholar] [CrossRef] [PubMed]
- Boone, J. Glandular breast dose for monoenergetic and high-energy X-ray beams: Monte Carlo assessment. Med. Phys. 1999, 213, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Boone, J.; Cooper, V., III. Scatter/primary in mammography: Monte Carlo validation. Med. Phys. 2000, 27, 1818–1831. [Google Scholar] [CrossRef] [PubMed]
- Cunha, D.; Tomal, A.; Poletti, M. Evaluation of scatter-to-primary ratio, grid performance and normalized average glandular dose in mammography by Monte Carlo simulation including interference and energy broadening effects. Phys. Med. Biol. 2010, 55, 4335–4359. [Google Scholar] [CrossRef] [PubMed]
- Dance, D.; Day, G. The computation of scatter in mammography by Monte Carlo methods. Phys. Med. Biol. 1984, 29, 237–247. [Google Scholar] [CrossRef] [PubMed]
- Barnea, G.; Dick, C. Monte Carlo studies of X-ray scattering in transmission diagnostic radiology. Med. Phys. 1986, 13, 490–495. [Google Scholar] [CrossRef]
- Boone, J.M.; Seibert, J.A. Monte Carlo simulation of the scattered radiation distribution in diagnostic radiology. Med. Phys. 1988, 15, 713–720. [Google Scholar] [CrossRef]
- Wu, X.; Barnes, G.; Tucker, D. Spectral dependence of glandular tissue dose in screen-film mammography. Radiology 1991, 179, 143–148. [Google Scholar] [CrossRef]
- Sechopoulos, I.; Suryanarayanan, S.; Vedantham, S.; D’Orsi, C.; Karellas, A. Computation of the glandular radiation dose in digital tomosynthesis of the breast. Med. Phys. 2007, 34, 221–232. [Google Scholar] [CrossRef]
- Alvarez, R.E.; Macovski, A. Energy-selective reconstruction in X-ray computerized tomography. Phys. Med. Biol. 1976, 21, 733–744. [Google Scholar] [CrossRef]
- Marziani, M.; Taibi, A.; Tuffanelli, A.; Gambaccini, M. Dual-energy tissue cancellation in mammography with quasi-monochromatic X-rays. Phys. Med. Biol. 2002, 47, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Gambaccini, M.; Tuffanelli, A.; Taibi, A.; Fantini, A.; Del Guerra, A. A Bragg diffraction based quasimonochromatic source for mammography using mosaic crystals. Proc. SPIE 1999, 3770, 174–184. [Google Scholar]
- Gambaccini, M.; Taibi, A.; Del Guerra, A.; Marziani, M.; Tuffanelli, A. MTF evaluation of a phosphor-coated CCD for X-ray imaging. Phys. Med. Biol. 1996, 41, 2799–2806. [Google Scholar] [CrossRef] [PubMed]
- Taibi, A.; Del Guerra, A.; Gambaccini, M.; Marziani, M.; Tuffanelli, A. Evaluation of a digital X-ray detector based on a phosphor-coated CCD for mammography. Nucl. Instrum. Methods Phys. Res. A 1997, 392, 210–213. [Google Scholar] [CrossRef]
- Baldelli, P.; Bravin, A.; Di Maggio, C.; Gennaro, G.; Sarnelli, A.; Taibi, A.; Gambaccini, M. Evaluation of the minimum iodine concentration for contrast-enhanced subtraction mammography. Phys. Med. Biol. 2006, 51, 4233–4251. [Google Scholar] [CrossRef]
- Kalyvas, N.; Valais, I.; Michail, C.; Fountos, G.; Kandarakis, I.; Cavouras, D. A theoretical study of CsI:Tl columnar scintillator image quality parameters by analytical modeling. Nucear Instrum. Methods Phys. Res. Sect. A 2015, 779, 18–24. [Google Scholar] [CrossRef]
- Michail, C.; Valais, I.; Seferis, I.; Kalyvas, N.; Fountos, G.; Kandarakis, I. Experimental Measurement of a High Resolution CMOS Detector Coupled to CsI Scintillators under X-ray Radiation. Radiat. Meas. 2015, 74, 39–46. [Google Scholar] [CrossRef]
- Michail, C.; Valais, I.; Martini, N.; Koukou, V.; Kalyvas, N.; Bakas, A.; Kandarakis, I.; Fountos, G. Determination of the Detective Quantum Efficiency (DQE) of CMOS/CsI Imaging Detectors following the novel IEC 62220-1-1:2015 International Standard. Radiat. Meas. 2016, 94, 8–17. [Google Scholar] [CrossRef]
- Kalender, W.A.; Klotz, E.; Kostaridou, L. An algorithm for noise suppression in dual energy CT material density images. IEEE Trans. Med. Imag. 1988, 7, 218–224. [Google Scholar] [CrossRef]
- Ducote, J.L.; Molloi, S. Quantification of breast density with dual energy mammography: An experimental study. Med. Phys. 2010, 37, 793–801. [Google Scholar] [CrossRef]
- Michail, C.; Valais, I.; Fountos, G.; Bakas, A.; Fountzoula, C.; Kalyvas, N.; Karabotsos, A.; Sianoudis, I.; Kandarakis, I. Luminescence Efficiency of Calcium Tungstate (CaWO4) under X-ray radiation: Comparison with Gd2O2S:Tb. Measurement 2018, 120, 213–220. [Google Scholar] [CrossRef]
- Michail, C.M.; Spyropoulou, V.A.; Fountos, G.P.; Kalyvas, N.E.; Valais, I.G.; Kandarakis, I.S.; Panayiotakis, G.S. Experimental and theoretical evaluation of a high resolution CMOS based detector under X-ray imaging conditions. IEEE Trans. Nucl. Sci. 2011, 58, 314–322. [Google Scholar] [CrossRef]
- ACR. Mammography, Quality Control Manual; American College of Radiology: Reston, VA, USA, 1999. [Google Scholar]
- Chen, X.; Mou, X.; Zhang, L. Indicator and calibration material for microcalcification in dualenergy mammography. In Proceedings of the 1st International Conference on Medical Biometrics, Hong Kong, China, 4–5 January 2008; pp. 265–272. [Google Scholar]
- Baker, R.; Matousek, P.; Ronayne, K.L.; Parker, A.W.; Rogers, K.; Stone, N. Depth profiling of calcifications in breast tissue using picosecond Kerr-gated Raman spectroscopy. Analyst 2007, 132, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.; Rogers, K.D.; Shepherd, N.; Stone, N. New relationships between breast microcalcifications and cancer. Br. J. Cancer 2010, 103, 1034–1039. [Google Scholar] [CrossRef] [PubMed]
- Kerssens, M.M.; Matousek, P.; Rogers, K.; Stone, N. Towards a safe non-invasive method for evaluation the carbonate substitution levels of hydroxyapatite (HAp) in micro-calcifications found in breast tissue. Analyst 2010, 135, 3156–3161. [Google Scholar] [CrossRef] [PubMed]
- Matousek, P.; Stone, N. Prospects for the diagnosis of breast cancer by noninvasive probing of calcifications using transmission Raman spectroscopy. J. Biomed. Opt. 2007, 12, 024008. [Google Scholar] [CrossRef]
- Matousek, P.; Stone, N. Recent advances in the development of Raman spectroscopy for deep non-invasive medical diagnosis. J. Biophotonics 2013, 6, 7–19. [Google Scholar] [CrossRef]
- Wang, Z.; Hauser, N.; Singer, G.; Trippel, M.; Kubik-Huch, R.A.; Chneider, C.W.; Stampanoni, M. Non-invasive classification of microcalcifications with phase-contrast X-ray mammography. Nat. Commun. 2014, 5, 3797. [Google Scholar] [CrossRef]
- Izatulina, A.R.; Nikolaev, A.M.; Kuz’mina, M.A.; Frank-Kamenetskaya, O.V.; Malyshev, V.V. Bacterial Effect on the Crystallization of Mineral Phases in a Solution Simulating Human Urine. Crystals 2019, 9, 259. [Google Scholar] [CrossRef]
- Busing, C.M.; Keppler, U.; Menges, V. Differences in microcalcification in breast tumors. Virchows Arch. A 1981, 393, 307–313. [Google Scholar] [CrossRef]
- Frappart, L.; Remy, I.; Lin, H.C.; Bremond, A.; Raudrant, D.; Grousson, B.; Vauzelle, J.L. Different types of microcalcifications observed in breast pathology. Virchows Arch. A 1987, 410, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Sugiura, Y.; Ishikawa, K. Effect of Calcium and Phosphate on Compositional Conversion from Dicalcium Hydrogen Phosphate Dihydrate Blocks to Octacalcium Phosphate Blocks. Crystals 2018, 8, 222. [Google Scholar] [CrossRef]
- Pajor, K.; Pajchel, L.; Kolodziejska, B.; Kolmas, J. Selenium-Doped Hydroxyapatite Nanocrystals-Synthesis, Physiochemical Properties and Biological Significance. Crystals 2018, 8, 188. [Google Scholar] [CrossRef]
- Xie, W.; Song, F.; Wang, R.; Sun, S.; Li, M.; Fan, Z.; Liu, B.; Zhang, Q.; Wang, J. Mechanically Robust 3D Graphene-Hydroxyapatite Hybrid Bioscaffolds with Enhanced Osteoconductive and Biocmpatible Performance. Crystals 2018, 8, 105. [Google Scholar] [CrossRef]
- Wang, H.; Yuan, L.; An, J. Crystallographic Characteristics of Hydroxyapatite in Hard Tissues of Cololabis saira. Crystals 2017, 7, 103. [Google Scholar] [CrossRef]
- Di Tommaso, D.; Prakash, M.; Lemaire, T.; Lewerenz, M.; De Leeuw, N.H.; Naili, S. Molecular Dynamics Simulations of Hydroxyapatite Nanopores in Contact with Electrolyte Solutions: The Effect of Nanoconfinement and Solvated Ions on the Surface Reactivity and the Structural, Dynamical, and Vibrational Properties of Water. Crystals 2017, 7, 57. [Google Scholar] [CrossRef]
- Vasquez-Quitral, P.; Arana, J.T.; Miras, M.C.; Acevedo, D.F.; Barbero, C.A.; Neira-Carrillo, A. Effect of Diazotated Sulphonated Polystyrene Films on the Calcium Oxalate Crystallization. Crystals 2017, 7, 70. [Google Scholar] [CrossRef]
- Wu, S.; Chiang, C.Y.; Zhou, W. Formation Mechanism of CaCO3 Spherulites in the Myostracum Layer of Limpet Shells. Crystals 2017, 7, 319. [Google Scholar] [CrossRef]
- Han, Y.; Sun, B.; Yan, H.; Tucker, M.E.; Zhao, Y.; Zhou, J.; Zhao, Y.; Zhao, H. Biomineralization of Carbonate Minerals Induced by The Moderate Halophile Staphylococcus Warneri YXY2. Crystals 2020, 10, 58. [Google Scholar] [CrossRef]
- Fandos-Morera, A.; Prats-Esteve, M.; Tura-Soteras, J.; Traveria-Cros, A. Breast tumors: Composition of microcalcifications. Radiology 1988, 169, 325–327. [Google Scholar] [CrossRef]
- Code of Federal Regulations, Title 21, Chapter I, Subchapter I, Part 900, Subpart BQuality Standards and Certification, §900.12; Revised 1 April 2015; OFR: College Park, MD, USA, 2015.
- Perry, N.; Broeders, M.; de Wolf, C.; Tornberg, S.; Holland, R.; von Karsa, L. European Guidelines for Quality Assurance in Breast Cancer Screening and Diagnosis, 4th ed.; European Communities: Brussels, Belgium, 2006. [Google Scholar]
- Cardinal, H.N.; Fenster, A. Theoretical optimization of a split septaless xenon ionization detector for dual-energy chest radiography. Med. Phys. 1988, 15, 167–180. [Google Scholar] [CrossRef] [PubMed]
- Johns, P.C.; Drost, D.J.; Yaffe, M.J.; Fenster, A. Dual-energy mammography: Initial experimental results. Med. Phys. 1985, 12, 297–304. [Google Scholar] [CrossRef] [PubMed]
- Lewin, J.M.; Isaacs, P.K.; Vance, V.; Larke, F.J. Dual-Energy Contrast-enhanced Digital Subtraction Mammography: Feasibility. Radiology 2003, 229, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Jochelson, M.S.; Dershaw, D.D.; Sung, J.S.; Heerdt, A.S.; Thornton, C.; Moskowitz, C.S.; Ferrara, J.; Morris, E.A. Bilateral Contrast-enhanced Dual-Energy Digital Mammography: Feasibility and Comparison with Conventional Digital Mammography and MR Imaging in Women with Known Breast Carcinoma. Radiology 2013, 266, 743–751. [Google Scholar] [CrossRef]
- Cheung, Y.C.; Lin, Y.C.; Wan, Y.L.; Yeow, K.M.; Huang, P.C.; Lo, Y.F.; Tsai, H.P.; Ueng, S.H.; Chang, C.J. Diagnostic performance of dual-energy contrast-enhanced subtracted mammography in dense breasts compared to mammography alone: Interobserver blind-reading analysis. Eur. Radiol. 2014, 24, 2394–2403. [Google Scholar] [CrossRef]
- Cheung, Y.C.; Tsai, H.P.; Lo, Y.F.; Ueng, S.H.; Huang, P.C.; Chen, S.C. Clinical utility of dual-energy contrast-enhanced spectral mammography for breast microcalcifications without associated mass: A preliminary analysis. Eur. Radiol. 2016, 26, 1082–1089. [Google Scholar] [CrossRef]
- Knogler, T.; Homolka, P.; Hörnig, M.; Leithner, R.; Langs, G.; Waitzbauer, M.; Pinker-Domenig, K.; Leitner, S.; Helbich, T.H. Contrast-enhanced dual energy mammography with a novel anode/filter combination and artifact reduction: A feasibility study. Eur. Radiol. 2016, 26, 1575–1581. [Google Scholar] [CrossRef]
- Knogler, T.; Homolka, P.; Hoernig, M.; Leithner, R.; Langs, G.; Waitzbauer, M.; Pinker, K.; Leitner, S.; Helbich, T.H. Application of BI-RADS Descriptors in Contrast-Enhanced Dual-Energy Mammography: Comparison with MRI. Breast Care 2017, 12, 212–216. [Google Scholar] [CrossRef]
- Sung, J.S.; Lebron, L.; Keating, D.; D’Alessio, D.; Comstock, C.E.; Lee, C.H.; Pike, M.C.; Ayhan, M.; Moskowitz, C.S.; Morris, E.A.; et al. Performance of Dual-Energy Contrast-enhanced Digital Mammography for screening Women at Increased Risk of Breast Cancer. Radiology 2019, 293, 81–88. [Google Scholar] [CrossRef]
- Del Medical Systems Group (Roselle, IL) 2005. Available online: http://www.delmedical.com (accessed on 12 March 2020).
- GE Healthcare. Available online: http://africa.gehealthcare.com/en/products/categories/mammography/mammography_systems/senographe_ds#tabs/tab16F1B92E81C840338FFD547C6292BB18 (accessed on 12 March 2020).
- GE Healthcare. Available online: https://www.gehealthcare.in/products/goldseal---refurbished-systems/goldseal-mammography/goldseal-certified-senographe-essential (accessed on 12 March 2020).
- Siemens Healthinees. Available online: https://www.siemens-healthineers.com/mammography/digital-mammography/mammomat-inspiration-prime (accessed on 12 March 2020).
- Radi, M.J. Calcium oxalate crystals in breast biopsies. An overlooked form of microcalcification associated with benign breast disease. Arch. Pathol. Lab. Med. 1989, 113, 1367–1369. [Google Scholar]
- Morgan, M.P.; Cooke, M.M.; Christopherson, P.A.; Westfall, P.R.; McCarthy, G.M. Calcium hydroxyapatite promotes mitogenesis and matrix metalloproteinase expression in human breast cancer cell lines. Mol. Carcinog. 2001, 32, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Morgan, M.P.; Cooke, M.M.; McCarthy, G.M. Microcalcifications associated with breast cancer: An epiphenomenon or biologically significant feature of selected tumors? J. Mammary Gland Biol. Neoplasia 2005, 10, 181–187. [Google Scholar] [CrossRef] [PubMed]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).