
Potential of Fibrin Glue and Mesenchymal Stem Cells (MSCs) to Regenerate Nerve Injuries: A Systematic Review

 , ,
, ,  and
and 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Bibliographic Search Strategy
2.2. Study Eligibility
3. Results

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Stem Cells Source | Treatment Groups Delivery System | Intervention Implantation Site | Analysis | Main Outcomes Conclusions |
|---|---|---|---|---|---|
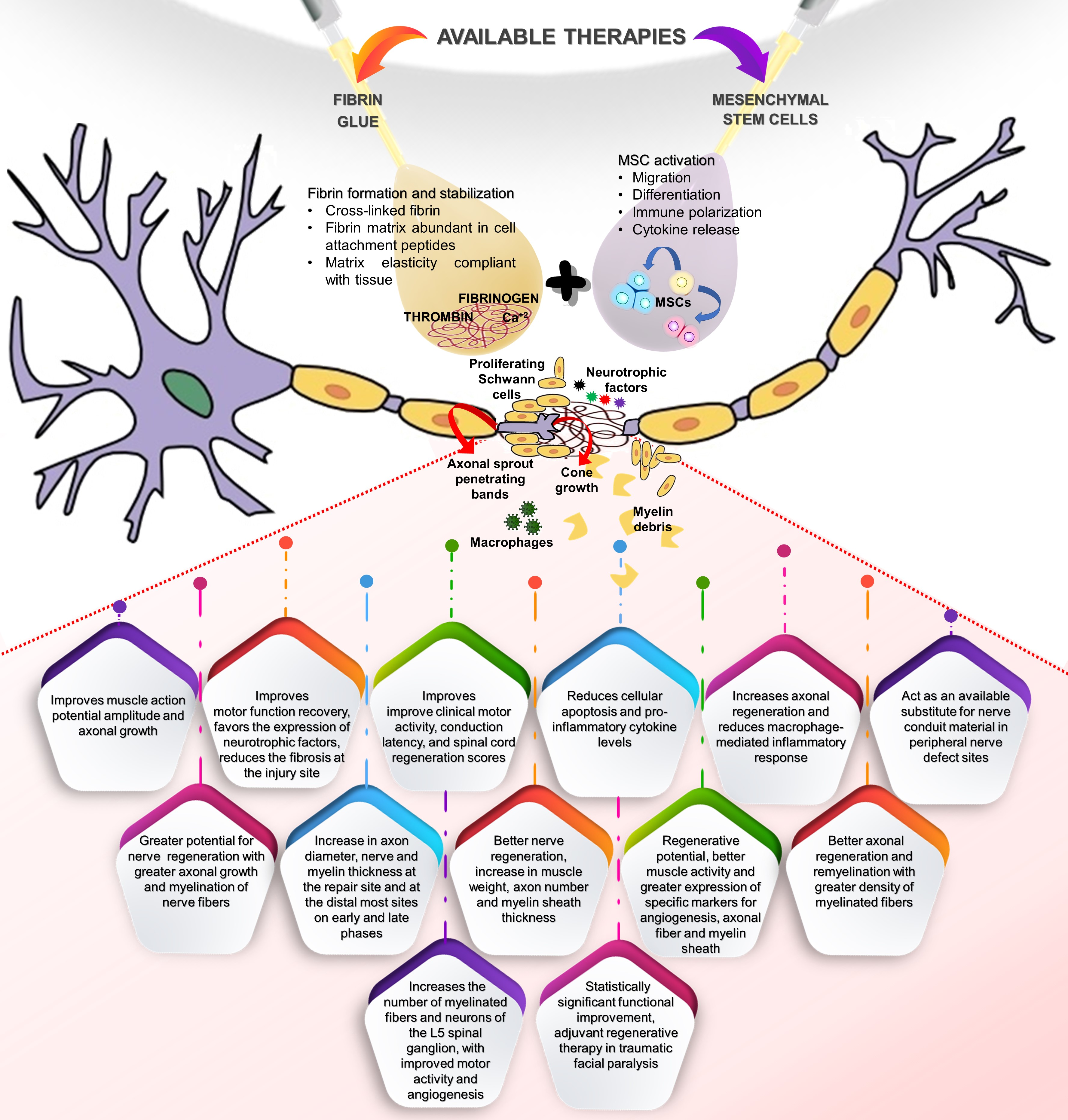
| Pan et al. (2006) [50] | Allogeneic MSCs (amniotic fluid) | G1: Fibrin glue (FG) + Surgicel® G2: FG + MSCs + Surgicel® | Rats sciatic nerve injuries were sutured, the gap (5 mm) was filled with MSCs + FG + Surgicel or FG + Surgicel (n = 10). Analyses were performed after 8 weeks of the procedures. | Electrophysiological and immunohistochemical analysis. | MSCs + FG + Surgicel® significantly improved muscle action potential amplitude and axonal growth. Compound muscle action potential values for G1 and G2 were 28.5 ± 1.3% and 42.5 ± 1.25%, respectively. Amniotic MSCs significantly improved nerve regeneration in a sciatic nerve gap. |
| Pan et al. (2007) [48] | Allogeneic rats MSCs (amniotic fluid) | G1: Fibrin glue (FG) + Surgicel® G2: FG + MSCs + Surgicel® | Rats sciatic nerve injuries (crush site) were sutured and wrapped with FG (n = 20) or FG + MSCs (n = 30). Analyzes were performed after 4 weeks of the procedures. | Enzyme-linked immunosorbent assay (ELISA), immunocytochemistry, motor function, electrophysiology, histology and immunocytochemistry | FG + MSCs significantly improved the motor function recovery, reduced the fibrosis at the injury site and favored the expression of neurotrophic factors, such as CNTF and NT-3.Compound muscle action potential values for G1 and G2 were 27.8 ± 4.22% and 67 ± 6.98%, with conduction latency of 3.91 ± 0.303 and 1.33 ± 0.048 msec, respectively. MSCs favored the sciatic nerve regeneration after crush injury. |
| Pan et al. (2009) [54] | Human amniotic fluid MSCs | G1: Fibrin glue (FG) + Surgicel® G2: FG + Surgicel® + Natto G3: MSCs + FG + Surgicel® G4: MSCs + FG + Surgicel® + Natto | Rats sciatic nerve injuries (crush site) were sutured and wrapped with FG or FG + MSCs (n = 6). G2/G4 were fed with Natto extract (16 mg/day) for 7 days. Analyzes were performed after 7 and 28 days of the procedures. | Electrophysiological, immunohistochemical, histological, cell apoptosis (Tunel assay) and pro-inflammatory cytokines analysis. | MSCs + FG + Surgicel® promoted better nerve regeneration than the FG + Surgicel® alone. Compound muscle action potential values for G1, G2, G3 and G4 were 0.25 ± 0.04%, 0.47 ± 0.03%, 0.51 ± 0.02% and 0.68 ± 0.02%, with conduction latency of 3.92 ± 0.31%, 1.85 ± 0.07%, 1.84 ± 0.08%, and 1.38 ± 0.11% respectively. Natto, alone or combined with MSCs, reduced cell apoptosis and proinflammatory cytokines levels, such as TNF-α and IL-1β. Combined treatment of MSCs+Natto showed the most beneficial effects. |
| McGrath et al. (2012) [47] | Human BM-MSCs (iliac crest) | G1:fibrin conduit (FC) + fibrin matrix (FG, Tisseel®) G2: FC + FG + cyclosporine G3: FC + FG + BM-MSCs G4: FC + FG + BM-MSCs + cyclosporine | Implantation of the fibrin conduit (14 mm) in rats sciatic nerve injuries (gap 10 mm). The conduct was sutured and filled with FG containing BM-MSCs. G2/G4 received daily intraperitoneally injections of cyclosporine A. Analyses were performed after 3 weeks of the procedures. | Immunohistochemistry | FC + FG + MSCs + cyclosporine was the most effective treatment to increase axonal regeneration and to reduce the macrophage-mediated inflammatory response. |
| Park et al. (2012) [23] | Autologous porcine SMSCs (ear skin) | G1: Collagen membrane (Lyoplant®) + fibrin glue (FG) + SMSCs G2: FG | Implantation of the collagen membrane in porcine femoral nerve injuries (gap 10 mm). The membrane was sutured and filled with FG containing SMSCs (n = 4). Analyses were performed after 2 and 4 weeks of the procedures. | Immunohistochemical and histological analysis. | G1 showed remarkable nerve regeneration with complete nerve bundles and higher expression of S-100 protein and p75 nerve growth factor. Autologous SMSCs and fibrin glue may act as an available substitute for nerve conduit material in peripheral nerve defect sites. |
| Zhao et al. (2014) [26] | Allogeneic rats BM-MSCs (femurs/tibias) | G1: Autograft G2: Acellular allograft (AL) + Fibrin glue (FG) + BM-MSCs (MSCs injected inside the graft) G3: AL + FG + BM-MSCs (MSCs injected around the graft) G4: AL + FG | Implantation of the graft in rats sciatic nerve injuries (gap 12 mm), suture and injection of FG containing BM-MSCs into/around the graft. Analyzes were performed after 2 weeks (n = 5) and 12 weeks (n = 8) of the procedures. | Muscle weight, histological, histomorphometric, sensory and motor functional analysis. | G1, G2 and G3 groups showed greater potential for nerve regeneration with greater axonal growth and myelination of nerve fibers. The graft implant with FG + BM-MSCs is successful in maintaining nerve structure and may support nerve regeneration. |
| Kurwale et al. (2015) [45] | Allogeneic rats BM-MNCs (femurs/tibias) | G1: Fibrin glue (FG) (Tisseel®) G2: FG + BM-MNCs | Rats sciatic nerve injuries were microsutured, the gap (2 mm) was filled with BM-MNCs and covered with FG (n = 5, per group/period). Analyses were performed after 15 and 60 days of the procedures. | Histological, immunohistochemical and morphometric analysis | FG + BM-MNCs showed a significant increase in axon diameter, nerve and myelin thickness at the repair site and at the distal most sites on early and late phases, respectively. Transplantation of BM-MNCs to the site of peripheral nerve injury leads to a significantly better recovery. |
| Reichenberger et al. (2015) [51] | Allogeneic rats AD-MSCs (inguinal tissue) | G1: Fibrin glue (FG) (Beriplast®) G2:FG + AD-MSCs | Sciatic nerve injuries of 50 rats were microsutured and the gap was filled with FG or FG containing AD-MSCs. Analyses were performed after 7, 21, 35 and 63 days of the procedures. | Immunofluorescence, muscle weight, histological and histomorphometric analysis. | FG + AD-MSCs showed better nerve regeneration with significant increase in muscle weight, axon number and myelin sheath thickness. AD-MSCs significantly enhanced the regeneration of peripheral nerve injuries after primary coaptation. |
| Ullah et al. (2017) [24] | Human dental pSCs (pulp-derived stem cells) | G1: Sham (n = 4) G2: Collagen membrane (Lyoplant®) + fibrin glue (FG) G3:Lyoplant® + FG + pSCs G4:Lyoplant® + FG + DpSCs | Implantation of the collagen membrane in rats sciatic nerve injuries (gap 5 mm). The membrane was sutured and filled with FG containing pSCs or differentiated neuronal cells (DpSCs) (n = 6/per group). Analyzes were performed after 12 weeks of the procedures. | Muscle contraction activity, immunohistochemical and histological analysis. | G3 and G4 showed considerable and similar regenerative potential, better muscle activity and greater expression of specific markers for angiogenesis, axonal fiber and myelin sheath, such as VEGFR-1, GFAP, S-100 protein, MBP-2 and p75NGFR. pSCs could exhibit excellent peripheral nerve regeneration potential. |
| Goel et al. (2019) [44] | Allogeneic rats BM-MNCs (femurs/tibias) | G1: Fibrin glue (FG) (Tisseel®) G2:FG + BM-MNCs | Rats’ sciatic nerve injuries were microsutured, filled with BM-MNCs and covered with FG (n = 5, per group/period). Analyses were performed after 30 and 60 days of the procedures. | Histological analysis | FG + BM-MNCs presented better axonal regeneration and remyelination with greater density of myelinated fibers. Local delivery of BM-MNCs improved peripheral nerve regeneration. |
| Masgutov et al. (2019) [46] | Allogeneic rats AD-MSCs (inguinal tissue) | G1:autologous nerve graft (AG) + fibrin glue (FG) + AD-MSCs Tissucol-Kit® G2: AG + FG G3: AG G4: Intact animals | Rats’ sciatic nerve injuries (gap 5 mm) were filled with AG, sutured and covered with FG containing AD-MSCs (n = 5). Analyses were performed after 30 and 60 days of the procedures. | Functional motor test, electromyography, EasyLDI laser Doppler and morphological analysis | AG + FG + AD-MSCs increased the number of myelinated fibers and neurons of the L5 spinal ganglion, with improved motor activity and angiogenesis. AG + FG + AD-MSCs resulted in motor function recovery after injury. |
| Bayir et al. (2021) [52] | Allogeneic rats NMSCs (fetal brain) | G1: No treatment G2: NMSCs G3: Fibrin glue (FG) Tisseel® G4: NMSCs + FG | Injection of NMSCs or NMSCs + FG in rats mandibular facial nerve injuries(crush). Analyses were performed immediately after surgery and after 3, 5 and 8 weeks of the procedures. | Physical examination, TUNEL assay and histochemical analysis. | NMSCs + FG showed a statistically significant functional improvement. NMSCs + FG may play a promising role as adjuvant regenerative therapy in traumatic facial paralysis. |
| Reference | Stem Cells Source | Treatment Groups Delivery System | Intervention Implantation Site | Analysis | Main Outcomes Conclusions |
|---|---|---|---|---|---|
| Pan et al. (2008) [53] | Allogeneic rats NSCs (fetal brain) | G1: Fibrin glue (FG) G2: FG + granulocyte colony-stimulating factor (G-CSF) G3: FG + NSCs G4: FG + NSCs + G-CSF | Injection of NSCs into the rats spinal cord (T8-T9) gap (2 mm) and sealing with FG + gelfoam. Subcutaneous injection of G-CSF for 5 days in G2/G3 groups (n = 10). Analyses were performed after 3 months of the procedures. | Electrophysiological, hind-limb motor function, histological and immunohistochemical analysis. | FG + NSCs + G-CSF significantly improved clinical motor activity, conduction latency and spinal cord regeneration scores. Motor evoked potential values for G1, G2, G3 and G4 were 24.69 ± 3.51, 31.64 ± 3.06, 38.97 ± 2.30 and 47.7 ± 3.17 mV, with conduction latency of 1.54 ± 0.04, 1.39 ± 0.03, 1.39 ± 0.04 and 1.29 ± 0.02 msec, respectively. Therapy associated with NSCs and C-CSF promoted better spinal cord regeneration. |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, Y.; Zhang, Y.; Li, X.; Zhang, Q. The progress of biomaterials in peripheral nerve repair and regeneration. J. Neurorestoratol. 2020, 8, 252–269. [Google Scholar] [CrossRef]
- Yi, S.; Xu, L.; Gu, X. Scaffolds for peripheral nerve repair and reconstruction. Exp. Neurol. 2019, 319, 112761. [Google Scholar] [CrossRef]
- Siemionow, M.; Brzezicki, G. Chapter 8: Current techniques and concepts in peripheral nerve repair. Int. Rev. Neurobiol. 2009, 87, 141–172. [Google Scholar] [CrossRef]
- Pan, D.; Mackinnon, S.E.; Wood, M.D. Advances in the repair of segmental nerve injuries and trends in reconstruction. Muscle Nerve 2020, 61, 726–739. [Google Scholar] [CrossRef] [PubMed]
- Fernandez, L.; Komatsu, D.E.; Gurevich, M.; Hurst, L.C. Emerging strategies on adjuvant therapies for nerve recovery. J. Hand Surg. Am. 2018, 43, 368–373. [Google Scholar] [CrossRef]
- Isaacs, J. Major peripheral nerve injuries. Hand Clin. 2013, 29, 371–382. [Google Scholar] [CrossRef] [PubMed]
- Ray, W.Z.; Mackinnon, S.E. Nerve problems in the lower extremity. Foot Ankle Clin. 2011, 16, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Rivlin, M.; Sheikh, E.; Isaac, R.; Beredjiklian, P.K. The role of nerve allografts and conduits for nerve injuries. Hand Clin. 2010, 26, 435–446. [Google Scholar] [CrossRef]
- Sinis, N.; Kraus, A.; Papagiannoulis, N.; Werdin, F.; Schittenhelm, J.; Meyermann, R.; Haerle, M.; Geuna, S.; Schaller, H.E. Concepts and developments in peripheral nerve surgery. Clin. Neuropathol. 2009, 28, 247–262. [Google Scholar]
- Safa, B.; Buncke, G. Autograft substitutes: Conduits and processed nerve allografts. Hand Clin. 2016, 32, 127–140. [Google Scholar] [CrossRef]
- Schmidt, C.E.; Leach, J.B. Neural tissue engineering: Strategies for repair and regeneration. Annu. Rev. Biomed. Eng. 2003, 5, 293–347. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assinck, P.; Duncan, G.J.; Hilton, B.J.; Plemel, J.R.; Tetzlaff, W. Cell transplantation therapy for spinal cord injury. Nat. Neurosci. 2017, 20, 637–647. [Google Scholar] [CrossRef]
- di Summa, P.G.; Kingham, P.J.; Raffoul, W.; Wiberg, M.; Terenghi, G.; Kalbermatten, D.F. Adipose-derived stem cells enhance peripheral nerve regeneration. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, 1544–1552. [Google Scholar] [CrossRef] [PubMed]
- Di Summa, P.G.; Schiraldi, L.; Cherubino, M.; Oranges, C.M.; Kalbermatten, D.F.; Raffoul, W.; Madduri, S. Adipose derived stem cells reduce fibrosis and promote nerve regeneration in rats. Anat. Rec. 2018, 301, 1714–1721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaakxs, D.; Kalbermatten, D.F.; Pralong, E.; Raffoul, W.; Wiberg, M.; Kingham, P.J. Poly-3-hydroxybutyrate strips seeded with regenerative cells are effective promoters of peripheral nerve repair. J. Tissue Eng. Regen. Med. 2017, 11, 812–821. [Google Scholar] [CrossRef]
- Schiraldi, L.; Sottaz, L.; Madduri, S.; Campisi, C.; Oranges, C.M.; Raffoul, W.; Kalbermatten, D.F.; di Summa, P.G. Split-sciatic nerve surgery: A new microsurgical model in experimental nerve repair. J. Plast. Reconstr. Aesthet. Surg. 2018, 71, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Pan, J.; Wang, D.; Liu, J. The use of stem cells in neural regeneration: A review of current opinion. Curr. Stem Cell Res. 2018, 13, 608–617. [Google Scholar] [CrossRef]
- Brown, C.; McKee, C.; Bakshi, S.; Walker, K.; Hakman, E.; Halassy, S.; Svinarich, D.; Dodds, R.; Govind, C.K.; Chaudhry, G.R. Mesenchymal stem cells: Cell therapy and regeneration potential. J. Tissue Eng. Regen. Med. 2019, 13, 1738–1755. [Google Scholar] [CrossRef]
- Murphy, M.B.; Moncivais, K.; Caplan, A.I. Mesenchymal stem cells: Environmentally responsive therapeutics for regenerative medicine. Exp. Mol. Med. 2013, 45, e54. [Google Scholar] [CrossRef] [Green Version]
- Han, Y.; Li, X.; Zhang, Y.; Han, Y.; Chang, F.; Ding, J. Mesenchymal stem cells for regenerative medicine. Cells 2019, 8, 886. [Google Scholar] [CrossRef] [Green Version]
- Squillaro, T.; Peluso, G.; Galderisi, U. Clinical trials with mesenchymal stem cells: An update. Cell Transplant. 2016, 25, 829–848. [Google Scholar] [CrossRef] [Green Version]
- Wu, X.; Ren, J.; Li, J. Fibrin glue as the cell-delivery vehicle for mesenchymal stromal cells in regenerative medicine. Cytotherapy 2012, 14, 555–562. [Google Scholar] [CrossRef]
- Park, B.W.; Kang, D.H.; Kang, E.J.; Byun, J.H.; Lee, J.S.; Maeng, G.H.; Rho, G.J. Peripheral nerve regeneration using autologous porcine skin-derived mesenchymal stem cells. J. Tissue Eng. Regen. Med. 2012, 6, 113–124. [Google Scholar] [CrossRef]
- Ullah, I.; Park, J.M.; Kang, Y.H.; Byun, J.H.; Kim, D.G.; Kim, J.H.; Kang, D.H.; Rho, G.J.; Park, B.W. Transplantation of human dental pulp-derived stem cells or differentiated neuronal cells from human dental pulp-derived stem cells identically enhances regeneration of the injured peripheral nerve. Stem Cells Dev. 2017, 26, 1247–1257. [Google Scholar] [CrossRef]
- Yousefi, F.; Arab, F.L.; Nikkhah, K.; Amiri, H.; Mahmoudi, M. Novel approaches using mesenchymal stem cells for curing peripheral nerve injuries. Life Sci. 2019, 221, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Wang, Y.; Peng, J.; Ren, Z.; Zhang, L.; Guo, Q.; Xu, W.; Lu, S. Improvement in nerve regeneration through a decellularized nerve graft by supplementation with bone marrow stromal cells in fibrin. Cell Transplant. 2014, 23, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Tsutsui, T. Human dental mesenchymal stem cells and neural regeneration. Hum. Cell 2013, 26, 91–96. [Google Scholar] [CrossRef]
- Chun, S.Y.; Lim, J.O.; Lee, E.H.; Han, M.H.; Ha, Y.S.; Lee, J.N.; Kim, B.S.; Park, M.J.; Yeo, M.G.; Jung, B.; et al. Preparation and Characterization of Human Adipose Tissue-Derived Extracellular Matrix, Growth Factors, and Stem Cells: A Concise Review. Tissue Eng. Regen. Med. 2019, 16, 385–393. [Google Scholar] [CrossRef]
- Man, A.J.; Kujawski, G.; Burns, T.S.; Miller, E.N.; Fierro, F.A.; Leach, J.K.; Bannerman, P. Neurogenic potential of engineered mesenchymal stem cells overexpressing VEGF. Cell Mol. Bioeng. 2016, 9, 96–106. [Google Scholar] [CrossRef] [Green Version]
- Gardin, C.; Vindigni, V.; Bressan, E.; Ferroni, L.; Nalesso, E.; Puppa, A.D.; D’Avella, D.; Lops, D.; Pinton, P.; Zavan, B. Hyaluronan and fibrin biomaterial as scaffolds for neuronal differentiation of adult stem cells derived from adipose tissue and skin. Int. J. Mol. Sci. 2011, 12, 6749–6764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, T.A.; Dare, E.V.; Hincke, M. Fibrin: A versatile scaffold for tissue engineering applications. Tissue Eng. Part B Rev. 2008, 14, 199–215. [Google Scholar] [CrossRef] [PubMed]
- Breen, A.; O’Brien, T.; Pandit, A. Fibrin as a delivery system for therapeutic drugs and biomolecules. Tissue Eng. Part B Rev. 2009, 15, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Brower, J.; Blumberg, S.; Carroll, E.; Pastar, I.; Brem, H.; Chen, W. Mesenchymal stem cell therapy and delivery systems in nonhealing wounds. Adv. Skin Wound Care 2011, 24, 524–532. [Google Scholar] [CrossRef] [PubMed]
- Heher, P.; Mühleder, S.; Mittermayr, R.; Redl, H.; Slezak, P. Fibrin-based delivery strategies for acute and chronic wound healing. Adv. Drug Deliv. Rev. 2018, 129, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Montana, M.; Tabélé, C.; Curti, C.; Terme, T.; Rathelot, P.; Gensollen, S.; Vanelle, P. Organic glues or fibrin glues from pooled plasma: Efficacy, safety and potential as scaffold delivery systems. J. Pharm. Pharm. Sci. 2012, 15, 124–140. [Google Scholar] [CrossRef] [PubMed]
- Valbonesi, M. Fibrin glues of human origin. Best Pract. Res. Clin. Haematol. 2006, 19, 191–203. [Google Scholar] [CrossRef]
- Whelan, D.; Caplice, N.M.; Clover, A.J. Fibrin as a delivery system in wound healing tissue engineering applications. J. Control. Release 2014, 196, 1–8. [Google Scholar] [CrossRef]
- Khodakaram-Tafti, A.; Mehrabani, D.; Shaterzadeh-Yazdi, H. An overview on autologous fibrin glue in bone tissue engineering of maxillofacial surgery. Dent. Res. J. 2017, 14, 79–86. [Google Scholar]
- Jeschke, M.G.; Finnerty, C.C.; Shahrokhi, S.; Branski, L.K.; Dibildox, M. Wound coverage technologies in burn care: Novel techniques. J. Burn Care Res. 2013, 34, 612–620. [Google Scholar] [CrossRef]
- Krug, C.; Beer, A.; Hartmann, B.; Prein, C.; Clause-Schaumann, H.; Holzbach, T.; Aszodi, A.; Giunta, R.E.; Saller, M.M.; Volkmer, E. Fibrin glue displays promising in vitro characteristics as a potential carrier of adipose progenitor cells for tissue regeneration. J. Tissue Eng. Regen. Med. 2019, 13, 359–368. [Google Scholar] [CrossRef]
- Noori, A.; Ashrafi, S.J.; Vaez-Ghaemi, R.; Hatamian-Zaremi, A.; Webster, T.J. A review of fibrin and fibrin composites for bone tissue engineering. Int. J. Nanomed. 2017, 12, 4937–4961. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.S.; Sung, H.M.; You, H.K.; Lee, J. Effects of fibrinogen concentration on fibrin glue and bone powder scaffolds in bone regeneration. J. Biosci. Bioeng. 2014, 118, 469–475. [Google Scholar] [CrossRef]
- Kalbermatten, D.F.; Kingham, P.J.; Mahay, D.; Mantovani, C.; Pettersson, J.; Raffoul, W.; Balcin, H.; Pierer, G.; Terenghi, G. Fibrin matrix for suspension of regenerative cells in an artificial nerve conduit. J. Plast. Reconstr. Aesthet. Surg. 2008, 61, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Goel, R.K.; Suri, V.; Suri, A.; Sarkar, C.; Mohanty, S.; Sharma, M.C.; Yadav, P.K.; Srivastava, A. Effect of bone marrow-derived mononuclear cells on nerve regeneration in the transection model of the rat sciatic nerve. J. Clin. Neurosci. 2009, 16, 1211–1217. [Google Scholar] [CrossRef]
- Kurwale, N.S.; Suri, V.; Srivastava, A.; Suri, A.; Mohanti, S.; Yadav, P.; Sharma, M.C.; Sarkar, C. Role of bone marrow derived pluripotent stem cells in peripheral nerve repair in adult rats: A morphometric evaluation. J. Neurosci. Rural Pract. 2015, 6, 152–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Masgutov, R.; Masgutova, G.; Mullakhmetova, A.; Zhuravleva, M.; Shulman, A.; Rogozhin, A.; Syromiatnikova, V.; Andreeva, D.; Zeinalova, A.; Idrisova, K.; et al. Adipose-Derived Mesenchymal Stem Cells Applied in Fibrin Glue Stimulate Peripheral Nerve Regeneration. Front. Med. 2019, 6, 68. [Google Scholar] [CrossRef]
- McGrath, A.M.; Brohlin, M.; Kingham, P.J.; Novikov, L.N.; Wiberg, M.; Novikova, L.N. Fibrin conduit supplemented with human mesenchymal stem cells and immunosuppressive treatment enhances regeneration after peripheral nerve injury. Neurosci. Lett. 2012, 516, 171–176. [Google Scholar] [CrossRef]
- Pan, H.C.; Cheng, F.C.; Chen, C.J.; Lai, S.Z.; Lee, C.W.; Yang, D.Y.; Chang, M.H.; Ho, S.P. Post-injury regeneration in rat sciatic nerve facilitated by neurotrophic factors secreted by amniotic fluid mesenchymal stem cells. J. Clin. Neurosci. 2007, 14, 1089–1098. [Google Scholar] [CrossRef]
- Pan, H.C.; Chin, C.S.; Yang, D.Y.; Ho, S.P.; Chen, C.J.; Hwang, S.M.; Chang, M.H.; Cheng, F.C. Human amniotic fluid mesenchymal stem cells in combination with hyperbaric oxygen augment peripheral nerve regeneration. Neurochem. Res. 2009, 34, 1304–1316. [Google Scholar] [CrossRef] [PubMed]
- Pan, H.C.; Yang, D.Y.; Chiu, Y.T.; Lai, S.Z.; Wang, Y.C.; Chang, M.H.; Cheng, F.C. Enhanced regeneration in injured sciatic nerve by human amniotic mesenchymal stem cell. J. Clin. Neurosci. 2006, 13, 570–575. [Google Scholar] [CrossRef]
- Reichenberger, M.A.; Mueller, W.; Hartmann, J.; Diehm, Y.; Lass, U.; Koellensperger, E.; Leimer, U.; Germann, G.; Fischer, S. ADSCs in a fibrin matrix enhance nerve regeneration after epineural suturing in a rat model. Microsurgery 2016, 36, 491–500. [Google Scholar] [CrossRef] [PubMed]
- Bayır, Ö.; Karagöz, T.; Pınarlı, F.A.; Sarıbaş, G.S.; Özoğul, C.; Keseroğlu, K.; Saylam, G.; Tatar, E.Ç.; Karahan, S.; Öcal, B.; et al. Impact of fetal brain tissue derived mesenchymal stem cell and fibrin glue on facial nerve crash injury. Turk. J. Med. Sci. 2021, 51, 1481–1490. [Google Scholar] [CrossRef]
- Pan, H.C.; Cheng, F.C.; Lai, S.Z.; Yang, D.Y.; Wang, Y.C.; Lee, M.S. Enhanced regeneration in spinal cord injury by concomitant treatment with granulocyte colony-stimulating factor and neuronal stem cells. J. Clin. Neurosci. 2008, 15, 656–664. [Google Scholar] [CrossRef]
- Pan, H.C.; Chen, C.J.; Cheng, F.C.; Ho, S.P.; Liu, M.J.; Hwang, S.M.; Chang, M.H.; Wang, Y.C. Combination of G-CSF administration and human amniotic fluid mesenchymal stem cell transplantation promotes peripheral nerve regeneration. Neurochem. Res. 2009, 34, 518–527. [Google Scholar] [CrossRef]
- Fawcett, J.W.; Keynes, R.J. Peripheral nerve regeneration. Annu Rev. Neurosci. 1990, 13, 43–60. [Google Scholar] [CrossRef]
- Fornasari, B.E.; Carta, G.; Gambarotta, G.; Raimondo, S. Natural-Based Biomaterials for Peripheral Nerve Injury Repair. Front. Bioeng. Biotechnol. 2020, 8, 554257. [Google Scholar] [CrossRef] [PubMed]
- Grinsell, D.; Keating, C.P. Peripheral nerve reconstruction after injury: A review of clinical and experimental therapies. Biomed. Res. Int. 2014, 2014, 698256. [Google Scholar] [CrossRef] [Green Version]
- Heo, J.S.; Choi, Y.; Kim, H.S.; Kim, H.O. Comparison of molecular profiles of human mesenchymal stem cells derived from bone marrow, umbilical cord blood, placenta and adipose tissue. Int. J. Mol. Med. 2016, 37, 115–125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ortiz, A.d.C.; Fideles, S.O.M.; Pomini, K.T.; Reis, C.H.B.; Bueno, C.R.d.S.; Pereira, E.d.S.B.M.; Rossi, J.d.O.; Novais, P.C.; Pilon, J.P.G.; Rosa Junior, G.M.; et al. Effects of Therapy with Fibrin Glue combined with Mesenchymal Stem Cells (MSCs) on Bone Regeneration: A Systematic Review. Cells 2021, 10, 2323. [Google Scholar] [CrossRef]
- Dekmak, A.; Mantash, S.; Shaito, A.; Toutonji, A.; Ramadan, N.; Ghazale, H.; Kassem, N.; Darwish, H.; Zibara, K. Stem cells and combination therapy for the treatment of traumatic brain injury. Behav. Brain Res. 2018, 340, 49–62. [Google Scholar] [CrossRef]
- Zibara, K.; Ballout, N.; Mondello, S.; Karnib, N.; Ramadan, N.; Omais, S.; Nabbouh, A.; Caliz, D.; Clavijo, A.; Hu, Z.; et al. Combination of drug and stem cells neurotherapy: Potential interventions in neurotrauma and traumatic brain injury. Neuropharmacology 2019, 145 Pt B, 177–198. [Google Scholar] [CrossRef]
- Nasser, M.; Bejjani, F.; Raad, M.; Abou-El-Hassan, H.; Mantash, S.; Nokkari, A.; Ramadan, N.; Kassem, N.; Mondello, S.; Hamade, E.; et al. Traumatic Brain Injury and Blood-Brain Barrier Cross-Talk. CNS Neurol. Disord. Drug Targets 2016, 15, 1030–1044. [Google Scholar] [CrossRef] [PubMed]
- Merimi, M.; Lewalle, P.; Meuleman, N.; Agha, D.M.; El-Kehdy, H.; Bouhtit, F.; Ayoub, S.; Burny, A.; Fahmi, H.; Lagneaux, L.; et al. Mesenchymal Stem/Stromal Cell Therapeutic Features: The Bridge between the Bench and the Clinic. J. Clin. Med. 2021, 10, 905. [Google Scholar] [CrossRef] [PubMed]
- Merimi, M.; Lagneaux, L.; Agha, D.M.; Lewalle, P.; Meuleman, N.; Burny, A.; Fahmi, H.; Najar, M. Mesenchymal Stem/Stromal Cells in Immunity and Disease: A Better Understanding for an Improved Use. J. Clin. Med. 2020, 9, 1516. [Google Scholar] [CrossRef] [PubMed]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortiz, A.d.C.; Fideles, S.O.M.; Pomini, K.T.; Bellini, M.Z.; Pereira, E.d.S.B.M.; Reis, C.H.B.; Pilon, J.P.G.; de Marchi, M.Â.; Trazzi, B.F.d.M.; da Silva, W.S.; et al. Potential of Fibrin Glue and Mesenchymal Stem Cells (MSCs) to Regenerate Nerve Injuries: A Systematic Review. Cells 2022, 11, 221. https://doi.org/10.3390/cells11020221
Ortiz AdC, Fideles SOM, Pomini KT, Bellini MZ, Pereira EdSBM, Reis CHB, Pilon JPG, de Marchi MÂ, Trazzi BFdM, da Silva WS, et al. Potential of Fibrin Glue and Mesenchymal Stem Cells (MSCs) to Regenerate Nerve Injuries: A Systematic Review. Cells. 2022; 11(2):221. https://doi.org/10.3390/cells11020221
Chicago/Turabian StyleOrtiz, Adriana de Cássia, Simone Ortiz Moura Fideles, Karina Torres Pomini, Márcia Zilioli Bellini, Eliana de Souza Bastos Mazuqueli Pereira, Carlos Henrique Bertoni Reis, João Paulo Galletti Pilon, Miguel Ângelo de Marchi, Beatriz Flavia de Moraes Trazzi, Willian Saranholi da Silva, and et al. 2022. "Potential of Fibrin Glue and Mesenchymal Stem Cells (MSCs) to Regenerate Nerve Injuries: A Systematic Review" Cells 11, no. 2: 221. https://doi.org/10.3390/cells11020221