

CILP-1 Is a Biomarker for Backward Failure and Right Ventricular Dysfunction in HFrEF
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. Echocardiography and Right Heart Cathetherization
2.3. Determination of Circulating CILP-1 Levels
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
3.2. Comparability of Different Commercially Available Human CILP-1 Assays
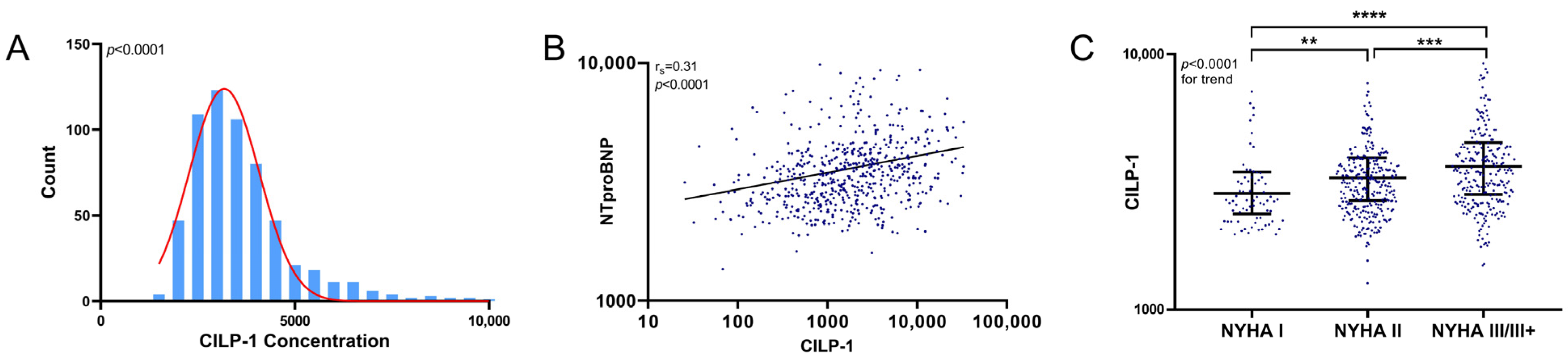
3.3. CILP-1 Distribution and Association with HFrEF Severity
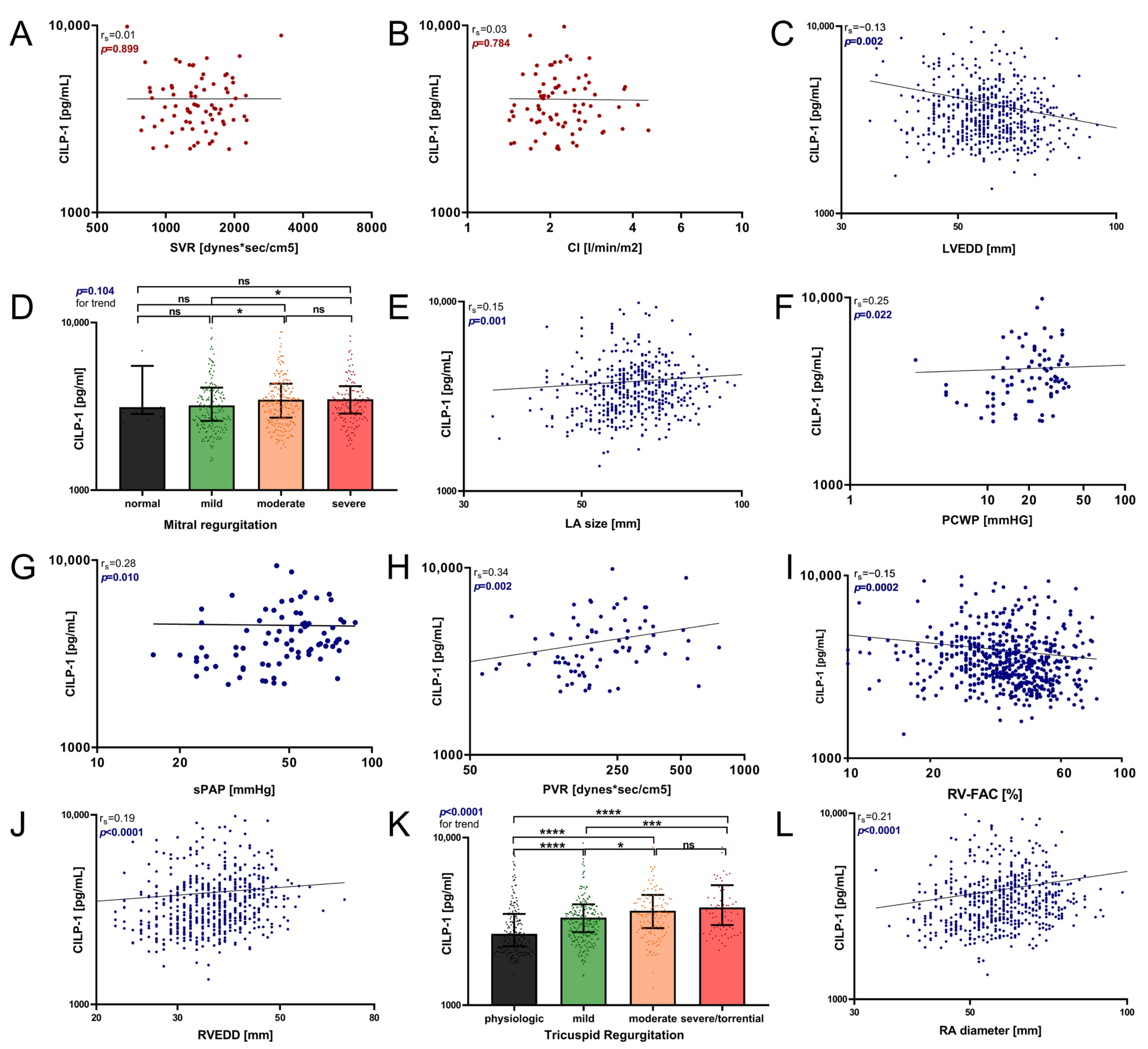
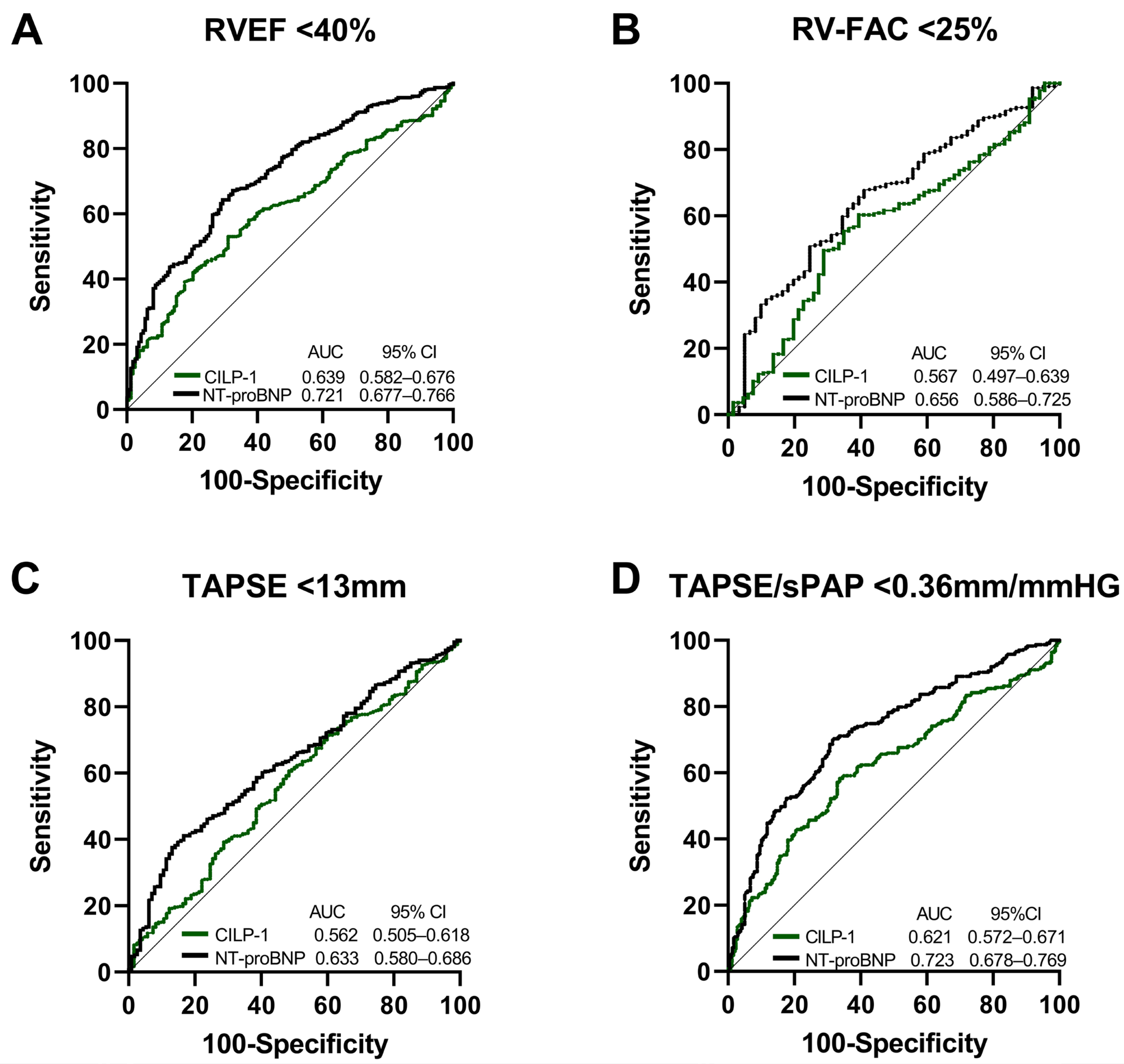
3.4. Association of CILP-1 with Echocardiographic and Hemodynamic Markers of Cardiac Dimensions and Function
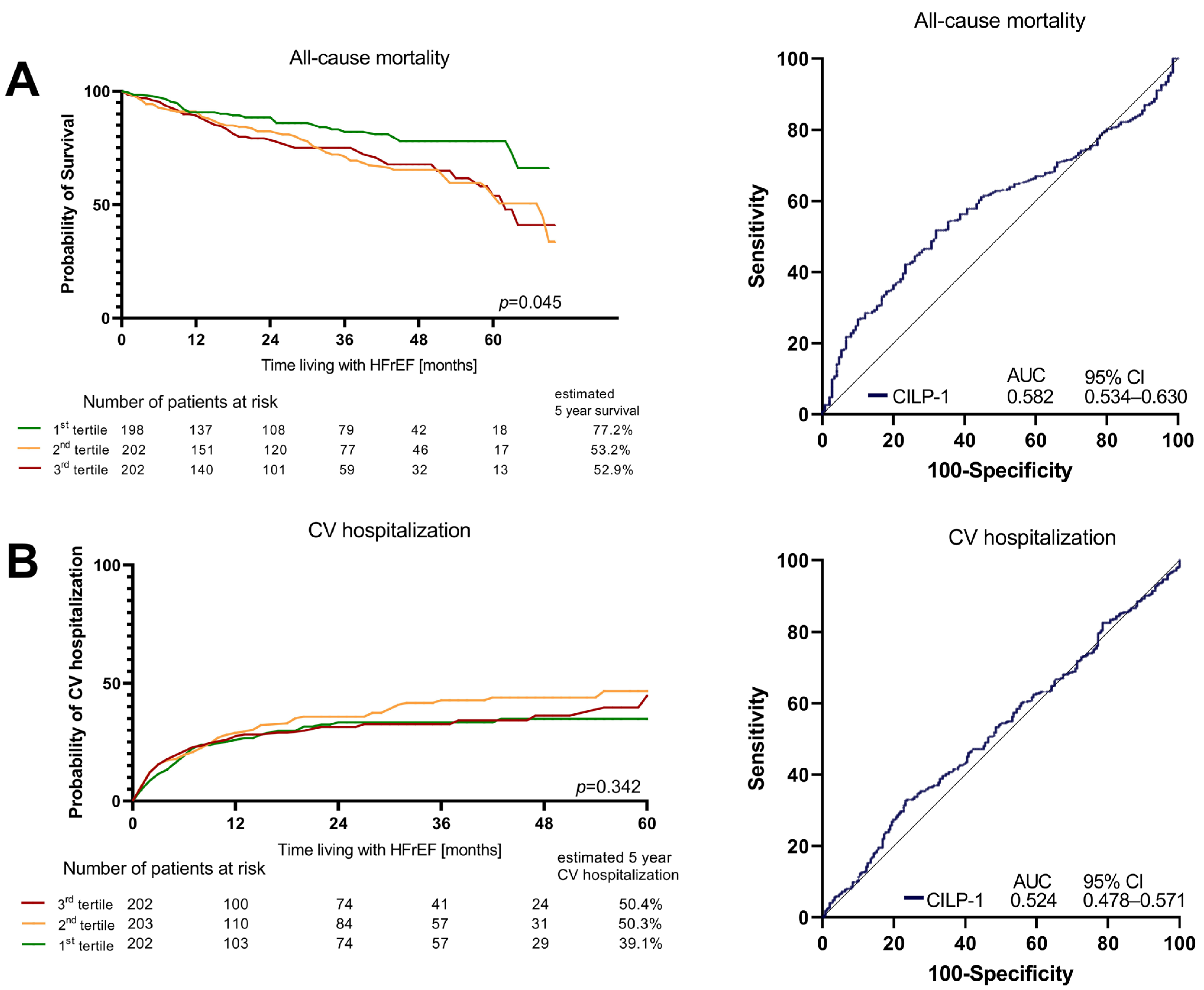
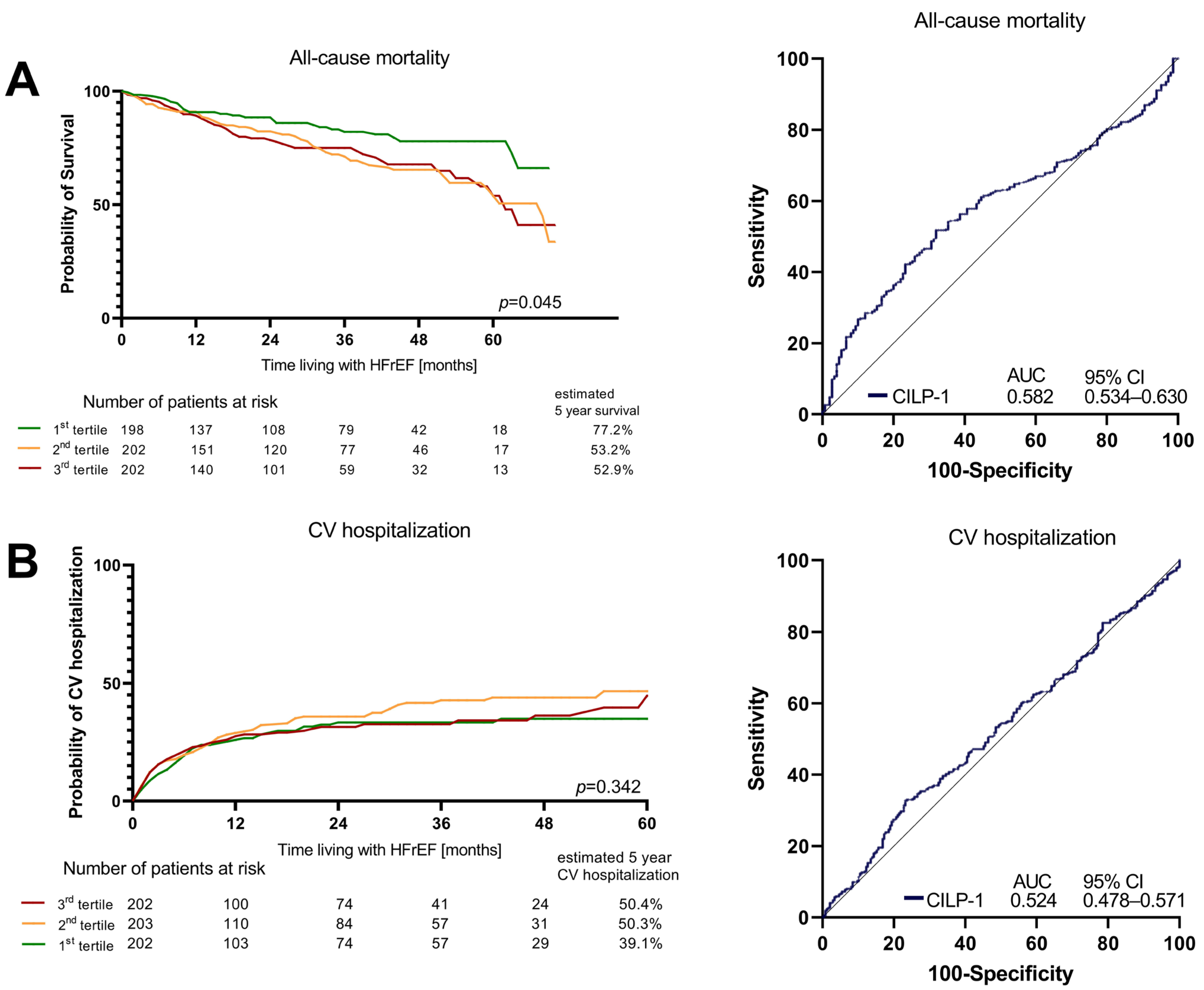
3.5. Association of CILP-1 with Prognosis in HFrEF
4. Discussion
4.1. Comparison of CILP-1 Levels in CV Disease and HF
4.2. Association of CILP-1 with Disease Severity and Functional and Hemodynamic Parameters in HF and Outcome
5. Conclusions
Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AUC | Area under the curve |
| BB | Beta-blocker |
| CI | Cardiac index |
| CILP-1 | Cartilage intermediate layer protein 1 |
| cMRI | Cardiac magnet resonance imaging |
| CO | Cardiac output |
| GDMT | Guideline-directed medical therapy |
| HF | Heart failure |
| HFrEF | Heart failure with reduced ejection fraction |
| LV | Left ventricle |
| LVEF | Left ventricular ejection fraction |
| LVEDD | Left ventricular end-diastolic diameter |
| MR | Mitral regurgitation |
| MRA | Mineralocorticoid-receptor antagonist |
| NYHA | New York Heart Association |
| PCWP | Pulmonary capillary wedge pressure |
| PH | Pulmonary hypertension |
| PVR | Pulmonary vascular resistance |
| RASi | Renin–angiotensin system inhibitor |
| RA | Right atrium |
| RV | Right ventricle |
| RVD | Right ventricular dysfunction |
| RVEF | Right ventricular ejection fraction |
| RVEDD | Right ventricular end-diastolic diameter |
| RVF | Right ventricular function |
| RV-FAC | Right ventricular fractional area change |
| ROC | Receiver operating characteristic |
| SGLT2i | Sodium-glucose transporter 2 inhibitor |
| sPAP | Systolic pulmonary artery pressure |
| SVR | Systemic vascular resistance |
| TAPSE | Tricuspid annular plane systolic excursion |
| TR | Tricuspid regurgitation |
References
- Keranov, S.; Dorr, O.; Jafari, L.; Troidl, C.; Liebetrau, C.; Kriechbaum, S.; Keller, T.; Voss, S.; Bauer, T.; Lorenz, J.; et al. CILP1 as a biomarker for right ventricular maladaptation in pulmonary hypertension. Eur. Respir. J. 2021, 57. [Google Scholar] [CrossRef]
- Greyson, C.R. Pathophysiology of right ventricular failure. Crit. Care Med. 2008, 36, S57–S65. [Google Scholar] [CrossRef] [PubMed]
- Meyer, P.; Filippatos, G.S.; Ahmed, M.I.; Iskandrian, A.E.; Bittner, V.; Perry, G.J.; White, M.; Aban, I.B.; Mujib, M.; Dell’Italia, L.J.; et al. Effects of right ventricular ejection fraction on outcomes in chronic systolic heart failure. Circulation 2010, 121, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Haddad, F.; Doyle, R.; Murphy, D.J.; Hunt, S.A. Right ventricular function in cardiovascular disease, part II: Pathophysiology, clinical importance, and management of right ventricular failure. Circulation 2008, 117, 1717–1731. [Google Scholar] [CrossRef] [PubMed]
- Tretter, J.T.; Redington, A.N. The Forgotten Ventricle? The Left Ventricle in Right-Sided Congenital Heart Disease. Circ. Cardiovasc. Imaging 2018, 11, e007410. [Google Scholar] [CrossRef]
- Thandavarayan, R.A.; Chitturi, K.R.; Guha, A. Pathophysiology of Acute and Chronic Right Heart Failure. Cardiol. Clin. 2020, 38, 149–160. [Google Scholar] [CrossRef]
- Galie, N.; Humbert, M.; Vachiery, J.L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Heart J. 2016, 37, 67–119. [Google Scholar] [CrossRef]
- Keranov, S.; Jafari, L.; Haen, S.; Vietheer, J.; Kriechbaum, S.; Dorr, O.; Liebetrau, C.; Troidl, C.; Rutsatz, W.; Rieth, A.; et al. CILP1 as a biomarker for right ventricular dysfunction in patients with ischemic cardiomyopathy. Pulm. Circ. 2022, 12, e12062. [Google Scholar] [CrossRef]
- Bernardo, B.C.; Belluoccio, D.; Rowley, L.; Little, C.B.; Hansen, U.; Bateman, J.F. Cartilage intermediate layer protein 2 (CILP-2) is expressed in articular and meniscal cartilage and down-regulated in experimental osteoarthritis. J. Biol. Chem. 2011, 286, 37758–37767. [Google Scholar] [CrossRef]
- Zhang, C.L.; Zhao, Q.; Liang, H.; Qiao, X.; Wang, J.Y.; Wu, D.; Wu, L.L.; Li, L. Cartilage intermediate layer protein-1 alleviates pressure overload-induced cardiac fibrosis via interfering TGF-beta1 signaling. J. Mol. Cell Cardiol. 2018, 116, 135–144. [Google Scholar] [CrossRef]
- Lorenzo, P.; Bayliss, M.T.; Heinegard, D. A novel cartilage protein (CILP) present in the mid-zone of human articular cartilage increases with age. J. Biol. Chem. 1998, 273, 23463–23468. [Google Scholar] [CrossRef]
- Van Nieuwenhoven, F.A.; Munts, C.; Op’t Veld, R.C.; Gonzalez, A.; Diez, J.; Heymans, S.; Schroen, B.; van Bilsen, M. Cartilage intermediate layer protein 1 (CILP1): A novel mediator of cardiac extracellular matrix remodelling. Sci. Rep. 2017, 7, 16042. [Google Scholar] [CrossRef]
- Park, S.; Ranjbarvaziri, S.; Zhao, P.; Ardehali, R. Cardiac Fibrosis Is Associated with Decreased Circulating Levels of Full-Length CILP in Heart Failure. JACC Basic. Transl. Sci. 2020, 5, 432–443. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Jian, W.; Luo, Q.; Cui, J.; Qing, Y.; Qin, C.; Li, G.; Chen, W. Prognostic value of cartilage intermediate layer protein 1 in chronic heart failure. ESC Heart Fail. 2022, 9, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.J.; He, Y.; Li, Y.; Shen, H.; Lin, L.; Zhu, M.; Wang, Z.; Luo, X.; Hill, J.A.; Cao, D.; et al. Matricellular Protein Cilp1 Promotes Myocardial Fibrosis in Response to Myocardial Infarction. Circ. Res. 2021, 129, 1021–1035. [Google Scholar] [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Bohm, M.; Burri, H.; Butler, J.; Celutkiene, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Bartko, P.E.; Hulsmann, M.; Hung, J.; Pavo, N.; Levine, R.A.; Pibarot, P.; Vahanian, A.; Stone, G.W.; Goliasch, G. Secondary valve regurgitation in patients with heart failure with preserved ejection fraction, heart failure with mid-range ejection fraction, and heart failure with reduced ejection fraction. Eur. Heart J. 2020, 41, 2799–2810. [Google Scholar] [CrossRef] [PubMed]
- Grayburn, P.A.; Sannino, A.; Packer, M. Proportionate and Disproportionate Functional Mitral Regurgitation: A New Conceptual Framework That Reconciles the Results of the MITRA-FR and COAPT Trials. JACC Cardiovasc. Imaging 2019, 12, 353–362. [Google Scholar] [CrossRef] [PubMed]
- Grayburn, P.A.; Packer, M. The Complex Phenotypic Expressions of Functional Mitral Regurgitation. J. Am. Coll. Cardiol. 2021, 78, 2422–2424. [Google Scholar] [CrossRef]
- Bartko, P.E.; Heitzinger, G.; Arfsten, H.; Pavo, N.; Spinka, G.; Andreas, M.; Mascherbauer, J.; Hengstenberg, C.; Hulsmann, M.; Goliasch, G. Disproportionate Functional Mitral Regurgitation: Advancing a Conceptual Framework to Clinical Practice. JACC Cardiovas. Imaging 2019, 12, 2088–2090. [Google Scholar] [CrossRef] [PubMed]
- Dutta, T.; Aronow, W.S. Echocardiographic evaluation of the right ventricle: Clinical implications. Clin. Cardiol. 2017, 40, 542–548. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Cohort (n = 610) | CILP-1 Tertile 1 (n = 203) | CILP-1 Tertile 2 (n = 204) | CILP-1 Tertile 3 (n = 203) | p-Value | |
|---|---|---|---|---|---|
| CILP-1, pg/mL (Q1–Q3) Range | 3341 | 2520 | 3341 | 4620 | - |
| (2714–4170) | (2249–2715) | (3116—3615) | (4169–5951) | ||
| 1354–33,480 | 1354–2870 | 2873–3813 | 3820–33,480 | ||
| Basic demographics | |||||
| Age, years (Q1–Q3) | 62 (52–72) | 57 (46–67) | 66 (56–73) | 65 (55–75) | <0.0001 |
| Male gender, n (%) | 475 (77.9%) | 150 (73.9) | 170 (83.3) | 155 (76.4) | 0.058 |
| BMI, kg/m2 (Q1–Q3) | 27.7 (23.9–31.0) | 27.7 (24.2–31.6) | 28.3 (24.7–31.1) | 26.4 (22.9–30.1) | 0.009 |
| Systolic BP, mmHg (Q1–Q3) | 125 (110–140) | 120 (110–135) | 125 (110–142) | 129 (110–140) | 0.154 |
| Diastolic BP, mmHG (Q1–Q3) | 78 (70–85) | 77 (70–85) | 80 (70–85) | 75 (70–87) | 0.826 |
| Heart rate, bpm (Q1–Q3) | 70 (61–81) | 70 (60–79) | 69 (61–80) | 70 (62–84) | 0.668 |
| NYHA class, n = 591; n (%) | <0.0001 | ||||
| I | 71 (12.0%) | 39 (19.9%) | 22 (11.3%) | 10 (5.0%) | |
| II | 276 (46.7%) | 93 (47.4%) | 101 (51.8%) | 82 (41.0%) | |
| III/IV | 244 (41.3%%) | 64 (32.7%) | 72 (36.9%) | 108 (54.0%) | |
| Comorbidities | |||||
| Coronary artery disease, n (%) | 339 (55.6%) | 109 (53.7%) | 109 (53.4%) | 121 (59.6%) | 0.373 |
| Atrial fibrillation, n (%) | 131 (21.5%) | 29 (14.3%) | 46 (22.5%) | 56 (27.6%) | 0.004 |
| Diabetes mellitus, n (%) | 221 (36.2%) | 56 (27.6%) | 75 (36.8%) | 90 (44.3%) | 0.014 |
| Arterial hypertension, n (%) | 328 (53.8%) | 100 (49.3%) | 111 (54.4) | 117 (57.6%) | 0.453 |
| Chronic kidney disease, n = 601; n (%) | 319 (53.1%) | 80 (40.0%) | 114 (56.7%) | 125 (62.5%) | <0.0001 |
| Dyslipidemia n = 597; n (%) | 227 (38.0%) | 95 (47.7%) | 69 (34.5%) | 63 (31.8%) | 0.002 |
| Medication and device therapy | |||||
| Beta-blocker, n (%) | 561 (92.0%) | 186 (91.6%) | 188 (92.2%) | 187 (92.1%) | 0.633 |
| ACEi, n (%) | 275 (45.1%) | 94 (46.3%) | 99 (48.5) | 82 (40.4%) | 0.338 |
| ARB, n (%) | 109 (17.9%) | 29 (14.3%) | 35 (17.2%) | 45 (22.2%) | 0.239 |
| ARNI, n (%) | 166 (27.2%) | 54 (26.6%) | 54 (26.5%) | 58 (28.6%) | 0.612 |
| MRA, n (%) | 444 (72.8%) | 150 (73.9%) | 157 (77.0%) | 137 (67.5%) | 0.203 |
| SGLT2 inhibitors, n (%) | 60 (9.8%) | 27 (13.3%) | 16 (7.8%%) | 17 (8.4%) | 0.263 |
| Ivabradin, n (%) | 37 (6.1%) | 12 (5.9%) | 9 (4.4%) | 16 (7.9%) | 0.401 |
| Diuretics, n (%) | 278 (45.6%) | 83 (40.9%) | 84 (41.2%) | 111 (54.7%) | 0.006 |
| ICD, n (%) | 251 (41.1%) | 85 (41.9%) | 81 (39.7%) | 85 (41.9%) | 0.391 |
| CRT, n (%) | 163 (26.7%) | 42 (20.7%) | 64 (31.4%) | 57 (28.1%) | 0.025 |
| PM, n (%) | 58 (9.5%) | 21 (10.3%) | 15 (7.4%) | 22 (10.8%) | 0.316 |
| Laboratory parameters | |||||
| NT-proBNP, pg/mL (Q1–Q3) | 1810.0 (676.1–3978.0) | 923.7 (412.9–2232.8) | 1907.0 (882.9–4138.5) | 2656.0 (1326.3–5928.5) | <0.0001 |
| eGFR, mL/min/1.73 m² | 57.7 (41.9–75.3) | 65.2 (49.5–80.2) | 56.9 (41.2–70.6) | 49.7 (37.6–68.1) | <0.0001 |
| CREA, mg/dL (Q1–Q3) | 1.21 (0.98–1.58) | 1.11 (0.90–1.37) | 1.25 (1.01–1.58) | 1.35 (1.06–1.76) | <0.0001 |
| Urea, mmol/L (Q1–Q3) | 23.7 (17.1–33.6) | 20.9 (15.9–28.9) | 24.1 (17.5–34.4) | 26.6 (17.1–36.7) | <0.0001 |
| Sodium, mmol/L (Q1–Q3) | 140.0 (138.0–141.0) | 140.0 (137.3–141.8) | 140.0 (138.0–141.0) | 140.0 (138.0–141.0) | 0.876 |
| Potassium, mmol/L (Q1–Q3) | 4.8 (4.4–5.1) | 4.8 (4.4–5.1) | 4.8 (4.4–5.1) | 4.7 (4.4–5.1) | 0.696 |
| Total bilirubin, mg/dL (Q1–Q3) | 0.6 (0.4–0.8) | 0.5 (0.4–0.8) | 0.6 (0.4–0.8) | 0.6 (0.4–0.9) | 0.064 |
| BChE, U/L (Q1–Q3) | 7.01 (5.67–8.36) | 7.77 (6.47–8.76) | 6.91 (5.67–8.09) | 6.50 (5.19–7.78) | <0.0001 |
| AST (GOT), U/L (Q1–Q3) | 24 (19–29) | 23 (19–27) | 24 (20–29) | 25 (19–31) | 0.070 |
| ALT (GPT), U/L (Q1–Q3) | 23 (17–33) | 23 (17–32) | 22 (16–34) | 23 (16–33) | 0.714 |
| GGT, U/L (Q1–Q3) | 44 (26–91) | 36 (21–61) | 43 (24–94) | 63 (32–124) | <0.0001 |
| Total cholesterol, mg/dL (Q1–Q3) | 154 (124–188) | 163 (131–196) | 151 (121–185) | 149 (124–188) | 0.035 |
| Hemoglobin, g/dL (Q1–Q3) | 13.6 (12.2–14.7) | 13.7 (12.6–14.8) | 13.7 (12.2–14.7) | 13.4 (11.8–14.7) | 0.062 |
| Ferritin, µg/L (Q1–Q3) | 150.8 (81.4–256.2) | 153.4 (65.2–260.2) | 147.4 (68.3–256.3) | 155.3 (94.1–251.3) | 0.553 |
| Transferrin saturation, % (Q1–Q3) | 21.4 (14.7–30.0) | 24.3 (16.6–31.3) | 20.6 (14.2–29.6) | 19.9 (14.3–28.7) | 0.027 |
| Uric acid, µmol/L (Q1–Q3) | 6.8 (5.5–8.2) | 6.6 (5.3–7.8) | 6.9 (5.7–8.2) | 7.0 (5.8–8.9) | 0.009 |
| Leukocyte count, G/L (Q1–Q3) | 7.6 (6.3–8.9) | 7.8 (6.6–9.0) | 7.4 (6.1–8.9) | 7.6 (6.3–9.1) | 0.428 |
| CRP, mg/dL (Q1–Q3) | 0.3 (0.1–0.7) | 0.3 (0.1–0.6) | 0.3 (0.1–0.6) | 0.4 (0.2–1.1) | 0.002 |
| Echocardiographic Parameters | Total Cohort n = 610 | CILP-1 Tertile 1 (n = 203) | CILP-1 Tertile 2 (n = 204) | CILP-1 Tertile 3 (n = 203) | p-Value |
|---|---|---|---|---|---|
| LVEF, n (%) recovered/mildly/ moderately/severely reduced | 22 (3.6%), 35 (5.7%). 87 (14.3%), 466 (76.4%) | 11 (5.4%), 12 (5.9%), 31 (15.3%), 149 (73.4%) | 7 (3.4%), 12 (5.9%), 27 (13.2%), 158 (77.5%) | 4 (2.0%), 11 (5.4%), 29 (14.3%), 159 (78.3%) | 0.670 |
| LVEDD, mm (Q1–Q3) | 57 (51–64) | 58 (51–65) | 58 (52–64) | 55 (49–61) | 0.003 |
| LA Diameter, mm (Q1–Q3) | 62 (56–70) | 58 (54–66) | 64 (58–71) | 63 (58–69) | <0.0001 |
| RVEF, reduced, n (%) normal/mildly/moderately/severely reduced | 252 (41.3%), 144 (23.6%), 135 (22.1%), 79 (13.0%) | 113 (55.7%), 48 (23.6%), 26 (12.8%), 16 (7.9%) | 70 (34.3%), 53 (26.0%), 50 (24.5%), 31 (15.2%) | 69 (34.0%), 43 (21.2%), 59 (29.1%), 32 (15.8%) | <0.0001 |
| TDI-RV m/s (Q1–Q3) | 0.10 (0.08–0.12) | 0.11 (0.09–0.13) | 0.09 (0.08–0.12) | 0.10 (0.08–0.12) | 0.002 |
| RV-FAC, % (Q1–Q3) | 39 (30–48) | 43 (34–51) | 37 (29–47) | 37 (28–48) | <0.0001 |
| TAPSE, mm (Q1–Q3) | 17 (13–20) | 18 (14–21) | 16 (13–20) | 16 (12–19) | <0.0001 |
| RVEDD, mm (Q1–Q3) | 36 (31–40) | 34 (30–38) | 37 (32–41) | 37 (33–42) | <0.0001 |
| RA diameter, mm (Q1–Q3) | 58 (51–65) | 54 (48–61) | 59 (52–68) | 60 (54–65) | <0.0001 |
| MR, n = 599; n (%) no/mild/moderate/severe | 17 (2.8%), 202 (33.7%), 237 (39.6%), 143 (23.9%) | 7 (3.5%), 84 (42.0%), 72 (36.0%), 37 (18.5%) | 5 (2.5%), 57 (28.5%), 80 (40.0%), 58 (29.0%) | 5 (2.5%), 61 (30.7%), 85 (42.7%), 48 (24.1%) | 0.051 |
| TR, n= 606; n (%) physiologic/mild/moderate/severe | 155 (25.6%), 158 (26.1%), 180 (29.7%), 113 (18.6) | 72 (36.0%), 55 (27.5%), 50 (25.0%), 23 (11.5%) | 42 (20.6%), 61 (29.9%), 66 (32.4%), 35 (17.2%) | 41 (20.3%), 42 (20.8%), 64 (31.7%), 55 (27.2%) | <0.0001 |
| sPAP, mmHg (Q1–Q3) | 44 (35–56) | 38 (30–51) | 48 (39–58) | 46 (37–60) | <0.0001 |
| Hemodynamic parameters (n = 84) | Total cohort (n = 84) | CILP-1 Tertile 1 (n = 16) | CILP-1 Tertile 2 (n = 32) | CILP-1 Tertile 3 (n = 36) | |
| RA pressure mean, mmHg (Q1–Q3) | 11 (7–18) | 9 (4–15) | 11 (5–18) | 15 (9–18) | 0.063 |
| RV pressure end-diastolic, mmHg (Q1–Q3) | 11 (8–16) | 9 (6–17) | 11 (8–16) | 12 (9–18) | 0.023 |
| Mean PA pressure, mmHg (Q1–Q3) | 33 (24–44) | 25 (19–32) | 35 (21–46) | 36 (29–44) | 0.021 |
| PCWP, mmHg (Q1–Q3) | 22 (14–29) | 15 (10–23) | 23 (13–31) | 24 (17–29) | 0.021 |
| AV O2, %/mL (Q1–Q3) | 68.7 (56.2–81.4) | 65.2 (50.6–79.1) | 72.4 (60.0–91.2) | 66.8 (56.3–78.6) | 0.187 |
| RV max, mmHg/sec (Q1–Q3) | 317 (248–410) | 274 (213–361) | 321 (237–414) | 331 (256–424) | 0.348 |
| Stroke volume, mL/stroke (Q1–Q3) | 55.4 (45.9–70.7) | 62.4 (49.0–89.9) | 55.6 (43.3–70.6) | 55.1 (46.2–67.4) | 0.294 |
| Cardiac index/L/min/m2 (Q1–Q3) | 2.1 (1.8–2.6) | 2.3 (1.8–3.0) | 2.1 (1.8–2.6) | 2.1 (1.9–2.5) | 0.596 |
| PVR, dynes × sec/cm5 (Q1–Q3) | 189 (150–280) | 168 (146–184) | 188 (131–296) | 239 (176–324) | 0.064 |
| SVR, dynes × sec/cm5 (Q1–Q3) | 1358 (1100–1721) | 1331 (1067–1600) | 1454 (1236–1728) | 1334 (1065–1843) | 0.740 |
| TPR, dynes × sec/cm5 (Q1–Q3) | 634 (454–853) | 408 (302–553) | 648 (430–855) | 660 (599–815) | 0.009 |
| TSR, dynes × sec/cm5 (Q1–Q3) | 1570 (1336–2009) | 1489 (1163–1884) | 1683 (1326–2021) | 1530 (1336–2048) | 0.544 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weidenhammer, A.; Prausmüller, S.; Partsch, C.; Spinka, G.; Luckerbauer, B.; Larch, M.; Arfsten, H.; Abdel Mawgoud, R.; Bartko, P.E.; Goliasch, G.; et al. CILP-1 Is a Biomarker for Backward Failure and Right Ventricular Dysfunction in HFrEF. Cells 2023, 12, 2832. https://doi.org/10.3390/cells12242832
Weidenhammer A, Prausmüller S, Partsch C, Spinka G, Luckerbauer B, Larch M, Arfsten H, Abdel Mawgoud R, Bartko PE, Goliasch G, et al. CILP-1 Is a Biomarker for Backward Failure and Right Ventricular Dysfunction in HFrEF. Cells. 2023; 12(24):2832. https://doi.org/10.3390/cells12242832
Chicago/Turabian StyleWeidenhammer, Annika, Suriya Prausmüller, Clemens Partsch, Georg Spinka, Bianca Luckerbauer, Mirella Larch, Henrike Arfsten, Ramy Abdel Mawgoud, Philipp E. Bartko, Georg Goliasch, and et al. 2023. "CILP-1 Is a Biomarker for Backward Failure and Right Ventricular Dysfunction in HFrEF" Cells 12, no. 24: 2832. https://doi.org/10.3390/cells12242832
APA StyleWeidenhammer, A., Prausmüller, S., Partsch, C., Spinka, G., Luckerbauer, B., Larch, M., Arfsten, H., Abdel Mawgoud, R., Bartko, P. E., Goliasch, G., Kastl, S., Hengstenberg, C., Hülsmann, M., & Pavo, N. (2023). CILP-1 Is a Biomarker for Backward Failure and Right Ventricular Dysfunction in HFrEF. Cells, 12(24), 2832. https://doi.org/10.3390/cells12242832