
Role of Copeptin and hs-cTnT to Discriminate AHF from Uncomplicated NSTE-ACS with Baseline Elevated hs-cTnT—A Derivation and External Validation Study
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
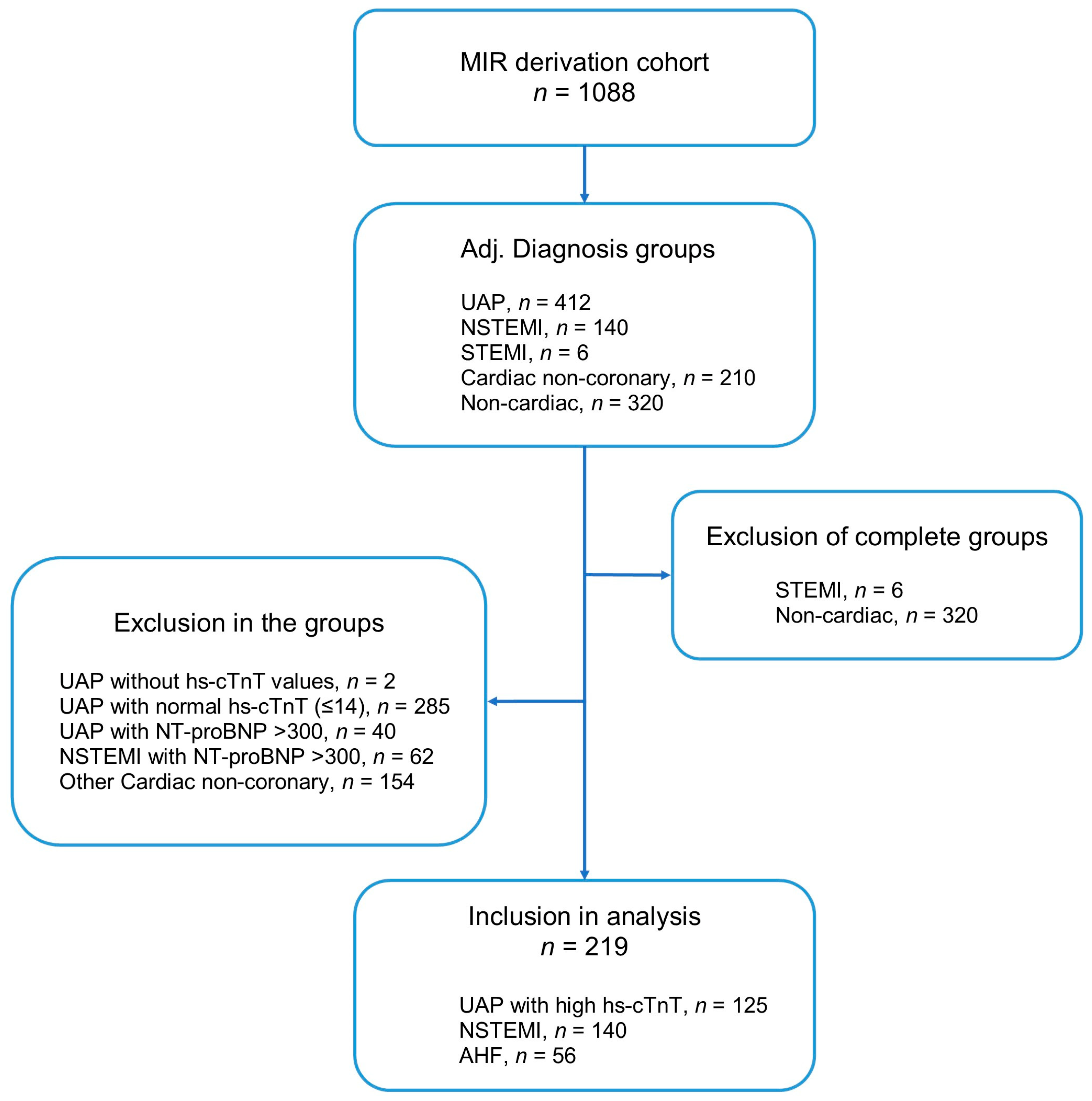
2.1. Derivation Cohort
2.2. Validation Cohort
2.3. Biomarker Analysis
2.4. Statistical Analysis
3. Results
3.1. Discrimination between NSTE-ACS and Acute HF
3.2. Prediction of 365-Day Mortality Using hs-cTnT and Copeptin
3.3. Validation Study
4. Discussion
5. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC); American College of Cardiology (ACC); American Heart Association (AHA); et al. Fourth Universal Definition of Myocardial Infarction (2018). Glob. Heart 2018, 13, 305–338. [Google Scholar] [CrossRef]
- Fanaroff, A.C.; Rymer, J.A.; Goldstein, S.A.; Simel, D.L.; Newby, L.K. Does This Patient With Chest Pain Have Acute Coronary Syndrome?: The Rational Clinical Examination Systematic Review. JAMA 2015, 314, 1955–1965. [Google Scholar] [CrossRef]
- Carlton, E.W.; Than, M.; Cullen, L.; Khattab, A.; Greaves, K. Chest pain typicality’ in suspected acute coronary syndromes and the impact of clinical experience. Am. J. Med. 2015, 128, 1109–1116. [Google Scholar] [CrossRef] [Green Version]
- Giannitsis, E.; Katus, H.A. Pros and cons of high-sensitivity assays for cardiac troponin. Nat. Rev. Cardiol. 2012, 9, 616–618. [Google Scholar] [CrossRef]
- André, F.; Buss, S.J.; Friedrich, M.G. The role of MRI and CT for diagnosis and work-up in suspected ACS. Diagnosis 2016, 3, 143–154. [Google Scholar] [CrossRef] [PubMed]
- Papolos, A.; Narula, J.; Bavishi, C.; Chaudhry, F.A.; Sengupta, P.P. U.S. Hospital Use of Echocardiography: Insights From the Nationwide Inpatient Sample. J. Am. Coll. Cardiol. 2016, 67, 502–511. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2022, 24, 4–131. [Google Scholar] [CrossRef]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367, Erratum in Eur. Heart J. 2021, 42, 1908; Erratum in Eur. Heart J. 2021, 42, 1925; Erratum in Eur. Heart J. 2021, 42, 2298. [Google Scholar] [CrossRef]
- Wiviott, S.D.; de Lemos, J.A.; Morrow, D.A. Pathophysiology, prognostic significance and clinical utility of B-type natriuretic peptide in acute coronary syndromes. Clin. Chim. Acta 2004, 346, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Widera, C.; Pencina, M.J.; Bobadilla, M.; Reimann, I.; Guba-Quint, A.; Marquardt, I.; Bethmann, K.; Korf-Klingebiel, M.; Kempf, T.; Lichtinghagen, R.; et al. Incremental prognostic value of biomarkers beyond the GRACE (Global Registry of Acute Coronary Events) score and high-sensitivity cardiac troponin T in non-ST-elevation acute coronary syndrome. Clin. Chem. 2013, 59, 1497–1505. [Google Scholar] [CrossRef] [Green Version]
- Waldsperger, H.; Biener, M.; Stoyanov, K.M.; Vafaie, M.; Katus, H.A.; Giannitsis, E.; Mueller-Hennessen, M. Prognostic Value of Elevated Copeptin and High-Sensitivity Cardiac Troponin T in Patients with and without Acute Coronary Syndrome: The ConTrACS Study. J. Clin. Med. 2020, 9, 3627. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.; Mueller, C.; Neath, S.X.; Christenson, R.H.; Morgenthaler, N.G.; McCord, J.; Nowak, R.M.; Vilke, G.; Daniels, L.B.; Hollander, J.E.; et al. Copeptin helps in the early detection of patients with acute myocardial infarction: Primary results of the CHOPIN trial (Copeptin Helps in the early detection of Patients with acute myocardial INfarction). J. Am. Coll. Cardiol. 2013, 62, 150–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maisel, A.; Xue, Y.; Shah, K.; Mueller, C.; Nowak, R.; Peacock, W.F.; Ponikowski, P.; Mockel, M.; Hogan, C.; Wu, A.H.; et al. Increased 90-day mortality in patients with acute heart failure with elevated copeptin: Secondary results from the Biomarkers in Acute Heart Failure (BACH) study. Circ. Heart Fail. 2011, 4, 613–620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipinski, M.J.; Escárcega, R.O.; D’Ascenzo, F.; Magalhães, M.A.; Baker, N.C.; Torguson, R.; Chen, F.; Epstein, S.E.; Miró, O.; Llorens, P.; et al. A systematic review and collaborative meta-analysis to determine the incremental value of copeptin for rapid rule-out of acute myocardial infarction. Am. J. Cardiol. 2014, 113, 1581–1591. [Google Scholar] [CrossRef] [PubMed]
- Möckel, M.; Searle, J.; Hamm, C.; Slagman, A.; Blankenberg, S.; Huber, K.; Katus, H.; Liebetrau, C.; Müller, C.; Muller, R.; et al. Early discharge using single cardiac troponin and copeptin testing in patients with suspected acute coronary syndrome (ACS): A randomized, controlled clinical process study. Eur. Heart J. 2015, 36, 369–376. [Google Scholar] [CrossRef]
- Biener, M.; Giannitsis, E.; Thum, T.; Bär, C.; Costa, A.; Andrzejewski, T.; Stoyanov, K.M.; Vafaie, M.; Meder, B.; Katus, H.A.; et al. Diagnostic value of circulating microRNAs compared to high-sensitivity troponin T for the detection of non-ST-segment elevation myocardial infarction. Eur. Heart J. Acute Cardiovasc. Care 2021, 10, 653–660. [Google Scholar] [CrossRef]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D.; Writing Group on the Joint ESC/ACCF/AHA/WHF Task Force for the Universal Definition of Myocardial Infarction. Third universal definition of myocardial infarction. Eur. Heart J. 2012, 33, 2551–2567. [Google Scholar] [CrossRef] [Green Version]
- Baggish, A.L.; Siebert, U.; Lainchbury, J.G.; Cameron, R.; Anwaruddin, S.; Chen, A.; Krauser, D.G.; Tung, R.; Brown, D.F.; Richards, A.M.; et al. A validated clinical and biochemical score for the diagnosis of acute heart failure: The ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) Acute Heart Failure Score. Am. Heart J. 2006, 151, 48–54. [Google Scholar] [CrossRef]
- Eagle, K.A.; Lim, M.J.; Dabbous, O.H.; Pieper, K.S.; Goldberg, R.J.; Van de Werf, F.; Goodman, S.G.; Granger, C.B.; Steg, P.G.; Gore, J.M.; et al. A validated prediction model for all forms of acute coronary syndrome: Estimating the risk of 6-month postdischarge death in an international registry. JAMA 2004, 291, 2727–2733. [Google Scholar] [CrossRef] [Green Version]
- Neumann, J.T.; Sörensen, N.A.; Ojeda, F.; Schwemer, T.; Lehmacher, J.; Gönner, S.; Jarsetz, N.; Keller, T.; Schaefer, S.; Renné, T.; et al. Immediate Rule-Out of Acute Myocardial Infarction Using Electrocardiogram and Baseline High-Sensitivity Troponin I. Clin. Chem. 2017, 63, 394–402. [Google Scholar] [CrossRef] [Green Version]
- Neumann, J.T.; Sörensen, N.A.; Schwemer, T.; Ojeda, F.; Bourry, R.; Sciacca, V.; Schaefer, S.; Waldeyer, C.; Sinning, C.; Renné, T.; et al. Diagnosis of Myocardial Infarction Using a High-Sensitivity Troponin I 1-Hour Algorithm. JAMA Cardiol. 2016, 1, 397–404. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Giannitsis, E.; Kurz, K.; Hallermayer, K.; Jarausch, J.; Jaffe, A.S.; Katus, H.A. Analytical Validation of a High-Sensitivity Cardiac Troponin T Assay. Clin. Chem. 2010, 56, 254–261. [Google Scholar] [CrossRef] [Green Version]
- Saenger, A.K.; Beyrau, R.; Braun, S.; Cooray, R.; Dolci, A.; Freidank, H.; Giannitsis, E.; Gustafson, S.; Handy, B.; Katus, H.; et al. Multicenter analytical evaluation of a high-sensitivity troponin T assay. Clin. Chim. Acta 2011, 412, 748–754. [Google Scholar] [CrossRef] [PubMed]
- Kargoli, F.; Levsky, J.; Bulcha, N.; Mustehsan, M.H.; Brown-Manhertz, D.; Furlani, A.; Polanco, D.; Mizrachi, S.; Makkiya, M.; Golive, A.; et al. Comparison Between Anatomical and Functional Imaging Modalities for Evaluation of Chest Pain in the Emergency Department. Am. J. Cardiol. 2020, 125, 1809–1814. [Google Scholar] [CrossRef]
- Mikami, T.; Ishii, M.; Yamamoto, N.; Marume, K.; Nakai, M.; Ogata, S.; Kaichi, R.; Ikebe, S.; Mori, T.; Komaki, S.; et al. Association of early administration of furosemide with improved oxygenation in patients with acute heart failure. ESC Heart Fail. 2021, 8, 3354–3359. [Google Scholar] [CrossRef] [PubMed]
- Matsue, Y.; Damman, K.; Voors, A.A.; Kagiyama, N.; Yamaguchi, T.; Kuroda, S.; Okumura, T.; Kida, K.; Mizuno, A.; Oishi, S.; et al. Time-to-Furosemide Treatment and Mortality in Patients Hospitalized with Acute Heart Failure. J. Am. Coll. Cardiol. 2017, 69, 3042–3051. [Google Scholar] [CrossRef] [PubMed]
- Rubini Gimenez, M.; Wildi, K.; Mueller, C. What cardiologists should know about copeptin. Rev. Esp. Cardiol. 2014, 67, 519–521. [Google Scholar] [CrossRef]
- Voors, A.A.; von Haehling, S.; Anker, S.D.; Hillege, H.L.; Struck, J.; Hartmann, O.; Bergmann, A.; Squire, I.; van Veldhuisen, D.J.; Dickstein, K.; et al. C-terminal provasopressin (copeptin) is a strong prognostic marker in patients with heart failure after an acute myocardial infarction: Results from the OPTIMAAL study. Eur. Heart J. 2009, 30, 1187–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Düngen, H.D.; Tscholl, V.; Obradovic, D.; Radenovic, S.; Matic, D.; Musial Bright, L.; Tahirovic, E.; Marx, A.; Inkrot, S.; Hashemi, D.; et al. Prognostic performance of serial in-hospital measurements of copeptin and multiple novel biomarkers among patients with worsening heart failure: Results from the MOLITOR study. ESC Heart Fail. 2018, 5, 288–296. [Google Scholar] [CrossRef]
- von Haehling, S.; Papassotiriou, J.; Morgenthaler, N.G.; Hartmann, O.; Doehner, W.; Stellos, K.; Wurster, T.; Schuster, A.; Nagel, E.; Gawaz, M.; et al. Copeptin as a prognostic factor for major adverse cardiovascular events in patients with coronary artery disease. Int. J. Cardiol. 2012, 162, 27–32. [Google Scholar] [CrossRef]
- Hellenkamp, K.; Pruszczyk, P.; Jiménez, D.; Wyzgał, A.; Barrios, D.; Ciurzyński, M.; Morillo, R.; Hobohm, L.; Keller, K.; Kurnicka, K.; et al. Prognostic impact of copeptin in pulmonary embolism: A multicentre validation study. Eur. Respir. J. 2018, 51, 1702037. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hellenkamp, K.; Schwung, J.; Rossmann, H.; Kaeberich, A.; Wachter, R.; Hasenfuß, G.; Konstantinides, S.; Lankeit, M. Risk stratification of normotensive pulmonary embolism: Prognostic impact of copeptin. Eur. Respir. J. 2015, 46, 1701–1710. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| All Patients (n = 219) | Acute HF (n = 56) | NSTE-ACS (n = 163) | p-Value | |
|---|---|---|---|---|
| Age | 70.27 ± 12.41 | 73.27 ± 12.33 | 69.24 ± 12.31 | 0.036 |
| Age > 75 years | 96 (44%) | 31 (55%) | 65 (40%) | 0.044 |
| Male (%) | 163 (74%) | 37 (66%) | 126 (77%) | 0.097 |
| eGFR (ml/min/1.73 m2) | 73.2 (51.5–89.9) | 53.5 (38.1–76.9) | 78.6 (61.7–91.6) | <0.001 |
| eGFR < 60 mL/min/1.73 m2 | 68 (31%) | 33 (59%) | 35 (26%) | <0.001 |
| eGFR < 30 mL/min/1.73 m2 | 13 (6%) | 7 (13%) | 6 (4%) | 0.016 |
| CV Risk | ||||
| Hypertension, No. (%) | 184 (84%) | 50 (90%) | 134 (82%) | 0.212 |
| Diabetes mellitus, No. (%) | 64 (29%) | 12 (21%) | 52 (32%) | 0.117 |
| Hypercholesterolemia, No. (%) | 142 (65%) | 42 (75%) | 100 (61%) | 0.065 |
| Chief complaint | ||||
| Chest Pain, No. (%) | 193 (88%) | 37 (66%) | 156 (96%) | <0.001 |
| Dyspnea, No. (%) | 117 (53%) | 47 (84%) | 70 (43%) | <0.001 |
| Medical history | ||||
| Previous MI, No. (%) | 65 (29.7%) | 17 (30.4%) | 8 (29.4%) | 0.898 |
| Previous PCI/CABG, No. (%) | 120 (54.8%) | 36 (64.3%) | 84 (51.5%) | 0.098 |
| History of HF, No. (%) | 22 (10.0%) | 17 (30.4%) | 5 (3.1%) | <0.001 |
| Previous stroke, No. (%) | 20 (9.1%) | 6 (10.7%) | 14 (8.6%) | 0.634 |
| GRACE score | 115.43 ± 26.16 | 127.91 ± 26.8 | 111.09 ± 24.57 | <0.001 |
| Laboratory | ||||
| Copeptin (pmol/L) | 9.2 (4.9–17.7) | 17.14 (8.8–54.5) | 7.7 (4–14.5) | <0.001 |
| Hs-cTnT 0 h (ng/L) | 26 (17–47) | 25.5 (15–40.8) | 26 (18–47) | 0.373 |
| Hs-cTnT 3 h (ng/L) | 27 (18–50.5) | 24 (16–37) | 27.5 (18–53.5) | 0.236 |
| Hs-cTnT delta | 3 (1–8) | 2 (1–4) | 3 (1–11) | 0.054 |
| Maximum hs-cTnT | 28 (19–64) | 25.5 (16–40.8) | 29 (19–73) | 0.022 |
| NT-proBNP (admission) pg/mL | 283 (134–3114) (n = 111) | 3287 (2155–6250) (n = 53) | 135 (52–204) (n = 58) | <0.001 |
| Group | Median within Group | Median Below or Equal Cut-Off | Median Above Cut-Off | |
|---|---|---|---|---|
| Copeptin cut-off = 10 pmol/L | All | 9.2 (4.9–17.7) n = 219 | 5.2 (3.4–7.5) n = 119 (54.3%) | 21.3 (14.04–56.03) n = 100 (45.7%) |
| Acute HF | 17.14 (8.8–54.5) n = 56 | 5.8 (4.5–8.6) n = 16 (28.6%) | 28.5 (16.2–57.3) n = 40 (71.4%) | |
| NSTE-ACS | 7.7 (4–14.5) n = 163 | 5.0 (3.3–6.95) n = 103 (63.2%) | 16.9 (13.1–48.2) n = 60 (36.8%) | |
| Hs-cTnT 0 h cut-off = 14 ng/L | All | 26 (17–47) n = 219 | 12 (10–13) n = 19 (8.68%) | 27 (18.3–50.3) n = 200 (91.32%) |
| Acute HF | 25.5 (15–40.8) n = 56 | 13 (10–13) n = 11 (19.6%) | 31 (21.5–49) n = 45 (80.4%) | |
| NSTE-ACS | 26 (18–47) n = 163 | 11.5 (8.5–13) n = 8 (4.9%) | 27 (18–52) n = 155 (95.1%) | |
| Hs-cTnT 3 h cut-off = 14 ng/L | All | 27 (18–50.5) n = 173 | 13 (12–14) n = 15 (8.7%) | 28 (19.8–55) n = 158 (91.3%) |
| Acute HF | 24 (16–37) n = 45 | 12 (11.5–12.5) n = 5 (11.1%) | 26.5 (19.3–42.5) n = 40 (88.9%) | |
| NSTE-ACS | 27.5 (18–53.5) n = 128 | 14 (12.75–14) n = 10 (7.8%) | 28 (20.5–56) n = 118 (92.2%) |
| All Patients (n = 219) | Death (n = 21) | Alive (n = 198) | p-Value | |
|---|---|---|---|---|
| Age | 70.27 ± 12.41 | 79.05 ± 10.23 | 69.34 ± 12.28 | <0.001 |
| Age > 75 years | 96 (44%) | 17 (81%) | 79 (40%) | <0.001 |
| m/f | 163/56 (74%/26%) | 15/6 (71%/29%) | 148/50 (75%/25%) | 0.740 |
| aHF/NSTE-ACS | 56/163 (25.6%/74.4%) | 15/6 (71.4%/28.6%) | 41/157 (20.7%/79.3%) | <0.001 |
| GRACE score | 115.43 ± 26.16 | 138.62 ± 0 | 112.94 ± 138.62 | <0.001 |
| eGFR | 73.2 (51.5–89.9) | 54 (25.9–66.8) | 76.5 (56–91.3) | <0.001 |
| eGFR < 60 mL/min | 68 (31%) | 14 (67%) | 54 (27%) | <0.001 |
| eGFR < 30 mL/min | 13 (6%) | 6 (29%) | 7 (4%) | <0.001 |
| Laboratory | ||||
| Copeptin | 9.2 (4.9–17.7) | 31.6 (12.3–63.8) | 8.5 (4.4–16.1) | <0.001 |
| Hs-cTnT 0 h | 26 (17–47) | 35 (24.5–68.5) | 24 (17–46) | 0.041 |
| Hs-cTnT 3 h | 27 (18–50.5) | 32 (25–62.5) | 25 (18–51.3) | 0.145 |
| Hs-cTnT delta | 3 (1–8) | 3 (1–11.5) | 3 (1–8) | 0.894 |
| Maximum hs-cTnT | 28 (19–64) | 37 (27–68.5) | 28 (18–64.5) | 0.185 |
| Univariable Model | Multivariable Model 1 * | Multivariable Model 2 ** | ||||
|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95%CI) | p-Value | HR (95% CI) | p-Value | |
| Copeptin (log) | 6.50 (2.82–15.01) | <0.001 | 5.4 (2.29–12.6) | <0.001 | 4.7 (1.9–11.45) | 0.001 |
| Hs-cTnT 0 h (log) | 1.78 (0.78–4.07) | 0.174 | 1.5 (0.59–3.92) | 0.384 | ||
| Hs-cTnT 3 h (log) | 1.39 (0.57–3.38) | 0.465 | ||||
| Age | 1.10 (1.04–1.16) | 0.001 | 1.08 (1.03–1.1) | 0.003 | 1.1 (1.03–1.15) | 0.005 |
| Male | 0.85 (0.33–2.19) | 0.736 | 0.88 (0.34–2.3) | 0.802 | 0.84 (0.32–2.2) | 0.729 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
von Haehling, S.; Müller-Hennessen, M.; Garfias-Veitl, T.; Goßling, A.; Neumann, J.T.; Sörensen, N.A.; Haller, P.M.; Hartikainen, T.; Vollert, J.O.; Möckel, M.; et al. Role of Copeptin and hs-cTnT to Discriminate AHF from Uncomplicated NSTE-ACS with Baseline Elevated hs-cTnT—A Derivation and External Validation Study. Cells 2023, 12, 1062. https://doi.org/10.3390/cells12071062
von Haehling S, Müller-Hennessen M, Garfias-Veitl T, Goßling A, Neumann JT, Sörensen NA, Haller PM, Hartikainen T, Vollert JO, Möckel M, et al. Role of Copeptin and hs-cTnT to Discriminate AHF from Uncomplicated NSTE-ACS with Baseline Elevated hs-cTnT—A Derivation and External Validation Study. Cells. 2023; 12(7):1062. https://doi.org/10.3390/cells12071062
Chicago/Turabian Stylevon Haehling, Stephan, Matthias Müller-Hennessen, Tania Garfias-Veitl, Alina Goßling, Johannes T. Neumann, Nils A. Sörensen, Paul M. Haller, Tau Hartikainen, Jörn Ole Vollert, Martin Möckel, and et al. 2023. "Role of Copeptin and hs-cTnT to Discriminate AHF from Uncomplicated NSTE-ACS with Baseline Elevated hs-cTnT—A Derivation and External Validation Study" Cells 12, no. 7: 1062. https://doi.org/10.3390/cells12071062