1. Introduction
Cancer is the second leading cause of death worldwide and is estimated to have caused 9.6 million deaths in 2018. Among the various types of cancer, gastric cancer is the sixth most common cancer type and the third leading cause of cancer death. As with other types of cancer, advanced stage patients are treated with chemotherapy. However, chemotherapy has limited efficacy, and new therapeutic agents are urgently needed.
During the early preclinical stage of developing new therapeutics, it is necessary to employ appropriate in vitro or in vivo preclinical models. In this sense, cell culture models have been widely used because of their availability and suitability for mass handling. However, there are often discrepancies between results obtained with cell line models and those obtained from clinical trials. Therefore, cell line models are not considered the most appropriate model for predicting the efficacy of new drugs, presumably because of a lack of heterogeneity and tissue structure.
Patient-derived xenograft (PDX) models involve the implantation of tissue or cells from a patient’s tumor into an immunodeficient mouse [
1,
2]. The advantage of using PDXs is that they retain the tumor tissue architecture, which is absent in cell culture models [
3]. Despite their limited availability and the difficulty in handling them, PDXs are considered a suitable preclinical model for evaluating drug sensitivity when developing new therapeutics, especially in oncology.
However, it is not clear if PDX models resemble the primary tumors from which they originated or how they do compare with CDX models. Therefore, it may be beneficial to directly compared PDX and cell line models established from the same tumor lesion. Another concern of using PDX models is their availability. For example, although there have been several studies using gastric cancer PDX models, most of them examined a relatively small number (less than 10) of PDX tumors [
4,
5,
6,
7,
8,
9,
10]. Therefore, it is necessary to provide a series of PDX models for each type of cancer. It is also important to have PDX models validated, especially if histology of the xenograft is comparable with the parental tumor [
11].
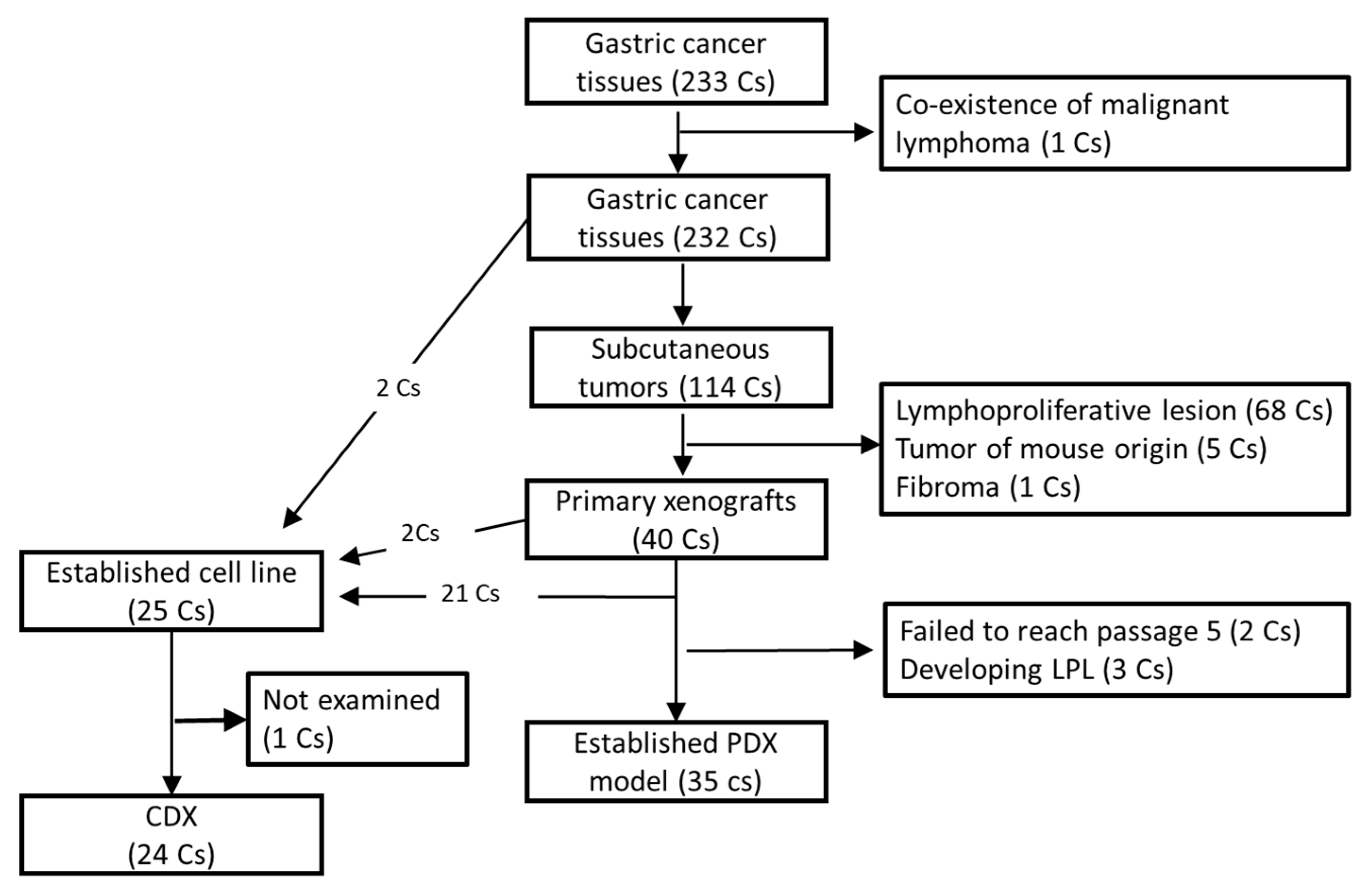
In this article, we describe 35 newly established gastric cancer PDX models as well as 32 gastric cancer CDX models. Among them, both PDX and CDX models were established from the same patient in 21 cases, allowing a direct histological comparison between primary, PDX, and CDX tumors. We also present clinicopathological factors associated with PDX and/or CDX establishment.
2. Materials and Methods
2.1. Patients
Two hundred fifty (250) gastric cancer patients treated at the National Cancer Center Hospital East (NCCHE) or the National Cancer Center Hospital (NCCH) from May 2013 to Feb 2017 were enrolled in this study. Two hundred thirty-two patients underwent surgical resection, and one (No. 214) was an autopsy case. One case (No. 238) harbored a malignant lymphoma in addition to a gastric cancer lesion, and malignant lymphoma tissue was taken for xenograft production. Therefore, the case was excluded from further analysis, and the remaining 232 cases including the autopsy case were designated as surgical cases. The remaining 17 cases received cell-free and concentrated ascites reinfusion therapy (CART) [
12,
13] for retaining ascites fluid caused by peritoneal dissemination of gastric cancer during the period and were designated as CART cases. CART is a method used for the treatment of ascites in patients who cannot receive higher doses of diuretics because of resistance to diuretic therapy or adverse effects (especially in patients with malignancies). Briefly, CART procedures were performed as follows: (i) drainage of the ascites by abdominal paracentesis; (ii) removal of malignant cells and other cell types by filtration and removal of excess fluid and electrolytes by concentration; and (iii) reinfusion of the filtered and concentrated ascites [
12]. All 17 patients enrolled in the study had malignant ascites caused by peritoneal dissemination of gastric cancer cells, and approximately 3–5 L of ascites were collected from each patient. Patient characteristics of all study participants, except for the malignant lymphoma case, and of all surgical cases are summarized in
Table 1 and
Table 2, respectively. Clinicopathological data were obtained from hospital medical records. Written informed consent was obtained from all enrolled patients, and this study was approved by our institute’s Institutional Review Board (No. 2012-328).
2.2. Animals
Female NOD/SCID/gamma-c null (NOG) mice [
14] were purchased from the Central Institute for Experimental Animals (CIEA, Kawasaki, Japan). Female ShiJic-scid Jcl (SCID) mice were purchased from CLEA Japan, Inc. (Tokyo, Japan). Female NOD.Cg-PrkdcscidIl2rgtm1Wjl/SzJ (NSG) mice were obtained from Charles River Laboratories International, Inc. (Kanagawa, Japan). All the mice were maintained in our animal facility under specific pathogen-free conditions. The experiments were performed according to the “Guidelines for Animal Experiments of the National Cancer Center” and were approved by the Institutional Ethics Review Committee for Animal Experimentation of the National Cancer Center (E21-M2-15, K16-004-M2).
2.3. Reagents
Dulbecco’s modified Eagle medium (DMEM), F-12 nutrient mixture (Ham’s F-12) and penicillin-streptomycin solution (PS) were purchased from Invitrogen (Carlsbad, CA, USA). Antibiotic-antimycotic mixed stock solutions (AAMS, 100×) were purchased from Nacalai Tesque Inc., (Kyoto, Japan). Fetal calf serum (FCS) was purchased from Biowest (Riverside, MO, USA). Cryopreservation reagents, Cell Banker, were purchased from Nippon Zenyaku Kogyo (Fukushima, Japan). Matrigel basement membrane matrix was purchased from Corning (Corning, NY, USA).
PAXgene tissue fix containers were purchased from QIAGEN (Tokyo, Japan). PATHWAY anti-HER-2/neu (4B5), INFORM HER2 Dual ISH DNA Probe Cocktail Assay (780-4422), and EBER 1 DNP Probe (760-1209) were purchased from Roche Diagnostics (Tokyo, Japan)
2.4. Establishing Xenograft Models
After examination by pathologists (T.K, S.S. or H.T.), about 25 mm3 of tumor tissue was resected from each primary lesion and transferred to tissue storage solution (DMEM supplemented with 10% FCS, 5% PS, and 5% AAMS). The tissue was washed extensively with wash solution (DMEM supplemented with 5% PS and 10% AAMS), dissected into 1-mm squares, and subcutaneously engrafted in NOG mice by using a transplantation needle (KN-391-20, Natume-seisakusho, Tokyo, Japan). NSG and SCID mice were used instead of NOD mice for 10 and 45 cases, respectively. When tumor tissues were engrafted into mice, matrigel was included in 63 cases (53 in NOG mice and all 10 cases in NSG mice).
The mice were observed daily for clinical signs and mortality. When subcutaneous tumors reached the size of 10 mm in diameter, the mice were sacrificed under anesthesia and the subcutaneous tumors were removed. The tumors were then dissected into pieces and either continuously engrafted to SCID mice, prepared for frozen stock, or fixed in PAXgene FIX for examining morphology.
For preparing CDXs, 10 million cells were subcutaneously engrafted into SCID mice, and subcutaneous tumors that arose were morphologically examined as described above.
2.5. Cell Culture
For patients who received CART, the cells originated in their ascites fluid and were trapped in the filtration filter during CART were recovered by washing in physiological saline. After centrifugation (2000 rpm, 10 min) and red blood cell removal using RBC lysis buffer (8.3% NH4Cl, 170 mM Tris-HCl (pH 7.65), cells were suspended in culture medium (50% DMEM, 50% Ham’s F-12) supplemented with 1% PS and 15% FCS. Tumor cells were seeded into 100 mm culture dishes (Falcon; Thermo Fisher Scientific, Waltham, MA, USA) and maintained at 37 °C in a humidified incubator with 5% CO2.
For establishing the cell lines from primary or xenograft tumors, tumor tissue was dissected into 1 mm cubic squares and explanted into 60 mm Corning Primaria dishes (Corning, NY, USA) with 1 mL of culture medium. An additional 4 mL culture medium was added the next day, and half the amount of culture medium was replaced twice weekly. Dishes containing tissue fragments were observed daily under an inverted phase microscope. The following three methods were used to selectively remove overgrowth fibroblasts: (i) trypsin treatment (0.05% trypsin and 0.02% EDTA, Thermo Fisher Scientifics): fibroblasts exfoliation by differences in trypsin sensitivity, with fresh medium added and washing performed to remove fibroblasts; (ii) physical treatment: change to serum-free medium and detachment of fibroblasts only using sharp silicone rubber under a microscope; and (iii) after exfoliating the cells using enzymatic treatment (Tumor Dissociation Kit # 130-095-929, Miltenyi Biotec, Tokyo, Japan), mouse-derived cells were removed using an antibody column (Mouse Cell Depletion Kit # 130-104-694, Miltenyi Biotec) according to the manufacturer’s protocol. When epithelial cell colonies were observed, they were transferred to another dish and continuously cultured. In some cases, we used the Mouse Cell Depletion Kit (Miltenyi Biotec, Tokyo, Japan) to remove mouse-derived cells. After 10 passages, the cells were considered an established line and subjected to short tandem repeat (STR)-analysis (Promega Japan, Tokyo, Japan). Cell lines were routinely tested for mycoplasma using a PCR mycoplasma detection technique at the Central Institute for Experimental Animals (Tokyo, Japan), and no contamination was detected.
2.6. Histology, Immunohistochemistry (IHC) and In Situ Hybridization (ISH)
Four micro-millimeter sliced tissue sections were prepared and subjected to H.E. staining, IHC, and ISH. Histological classifications were made based on the Japanese classification of gastric carcinoma (3rd English edition) [
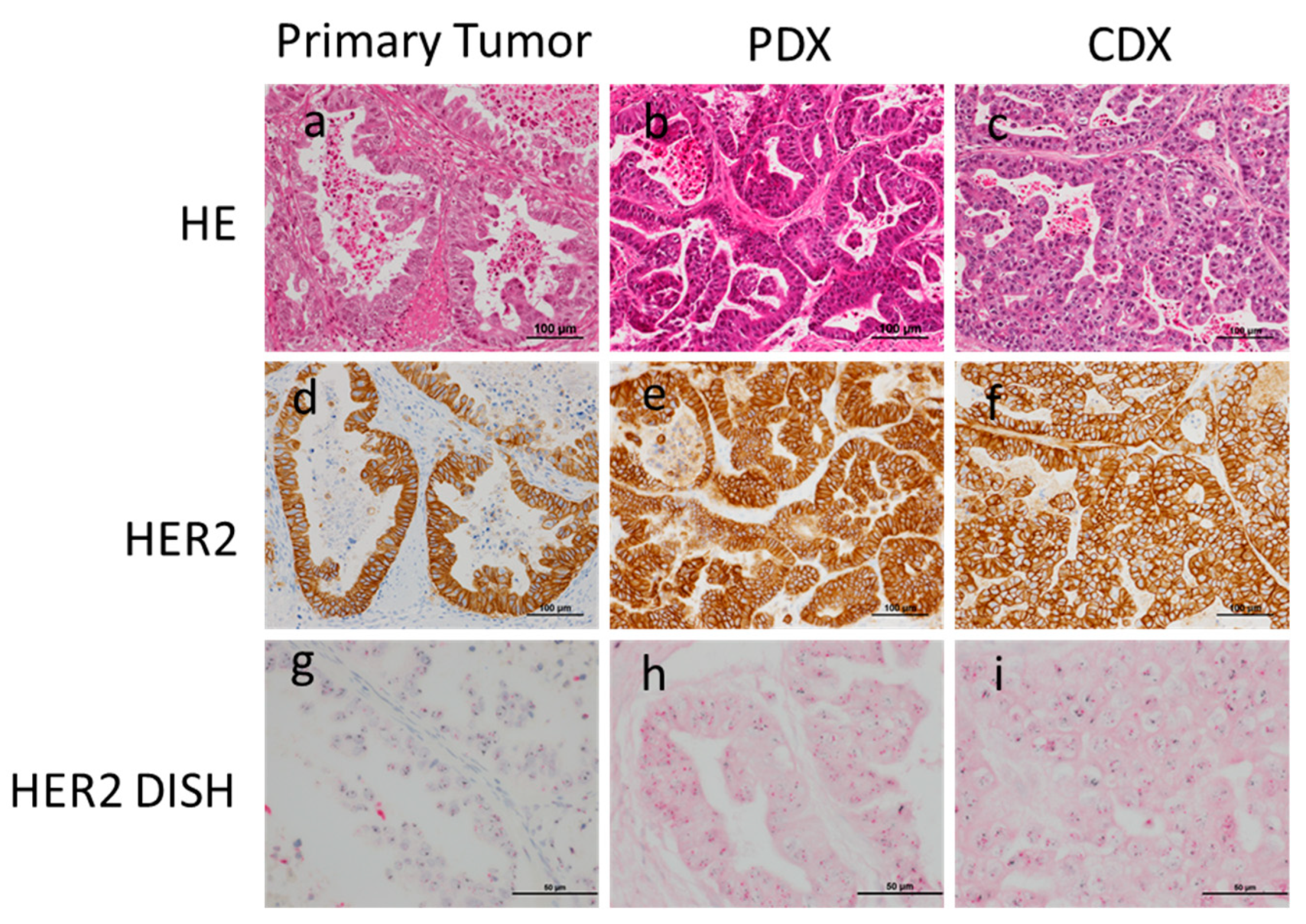
15], and differentiation grade was based on the presence/absence of glandular structure formation. IHC for HER2 expression and dual-IHC (DISH) assay for HER2 gene amplification were performed, as reported previously [
16]. Criteria for deciding if cells were HER2-positive were either strong membranous staining of the HER2 protein or moderate membranous staining of HER2 plus HER2 gene amplification. ISH for Epstein-Barr virus (EBV)-encoded small RNA (EBER) was performed, as reported previously [
17].
2.7. Statistics
Fisher’s exact test was performed using IBM SPSS Statistics version 22 (SPSS Inc., Chicago, IL, USA). The analyses performed were two-sided, and p < 0.05 was considered to be statistically significant.
4. Discussion
PDX models have recently been widely accepted as a preclinical model [
1,
2,
18,
19,
20,
21,
22,
23]. However, the utility of PDX models has not yet been fully exploited in most research laboratories, mainly because of the difficulty of accessing and maintaining PDXs. It is especially apparent for cancer types, including gastric cancer, not frequently encountered in Western countries [
11]. Although there have been several studies reporting gastric cancer PDX models [
4,
5,
6,
7,
8,
9,
10,
24,
25,
26,
27], a relatively small number of PDX models were examined in most of the cases. Therefore, it is urgently necessary to establish relatively large series of gastric cancer PDX models to obtain more accurate results from preclinical studies for predicting the efficacy of newly developed drugs specific to gastric cancer. The 35 gastric cancer PDX models we established in this study may contribute to solving this issue (summarized in
Table 8).
It has been considered that PDX models are biologically more similar to primary tumors than to CDX models. However, to our best knowledge, there have been no reports available describing the difference between primary, PDX, and CDX tumors obtained from the same primary gastric cancer lesion. In fact, one report argued that there was discordance between the histology of primary tumors and PDXs [
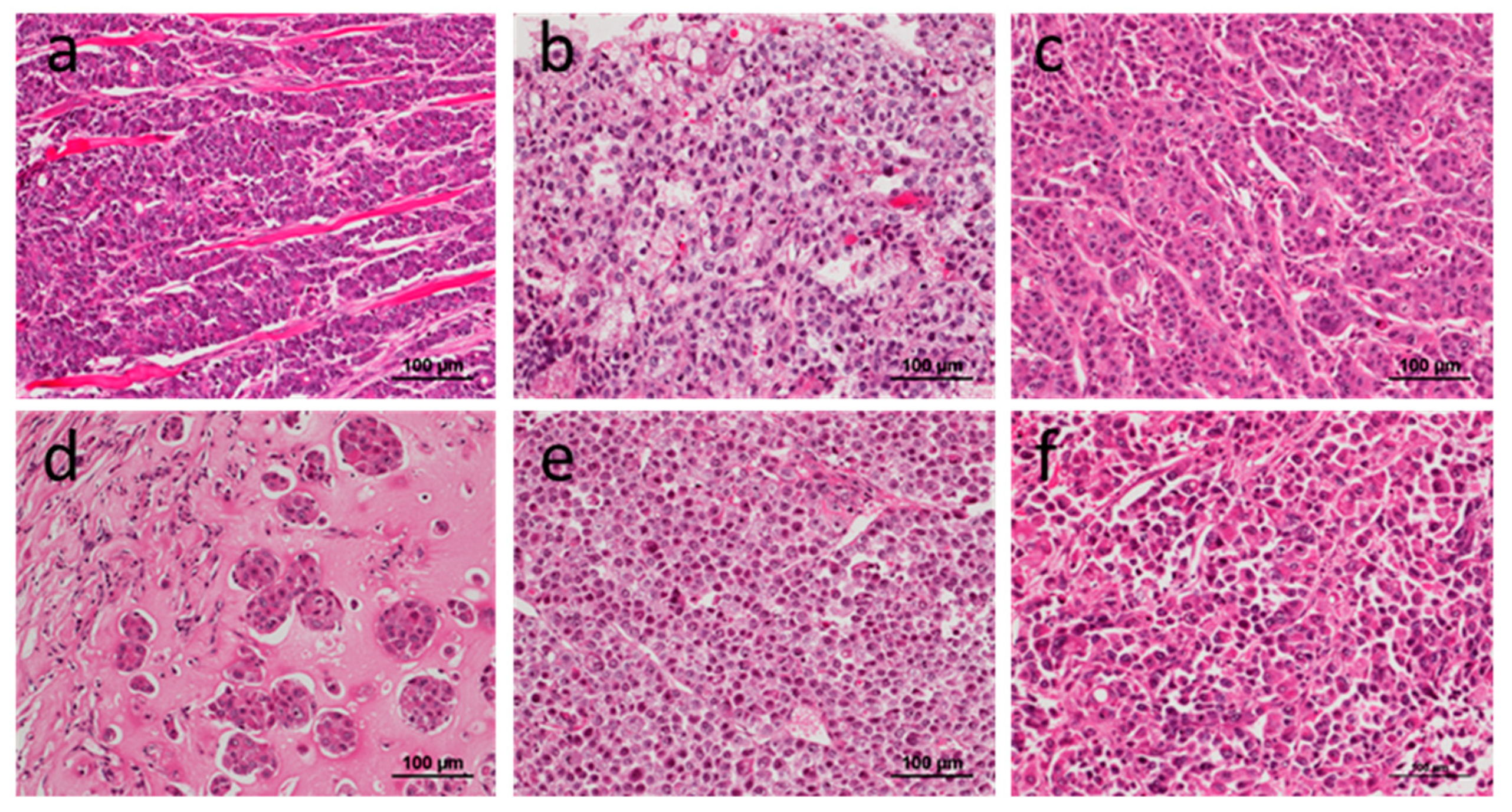
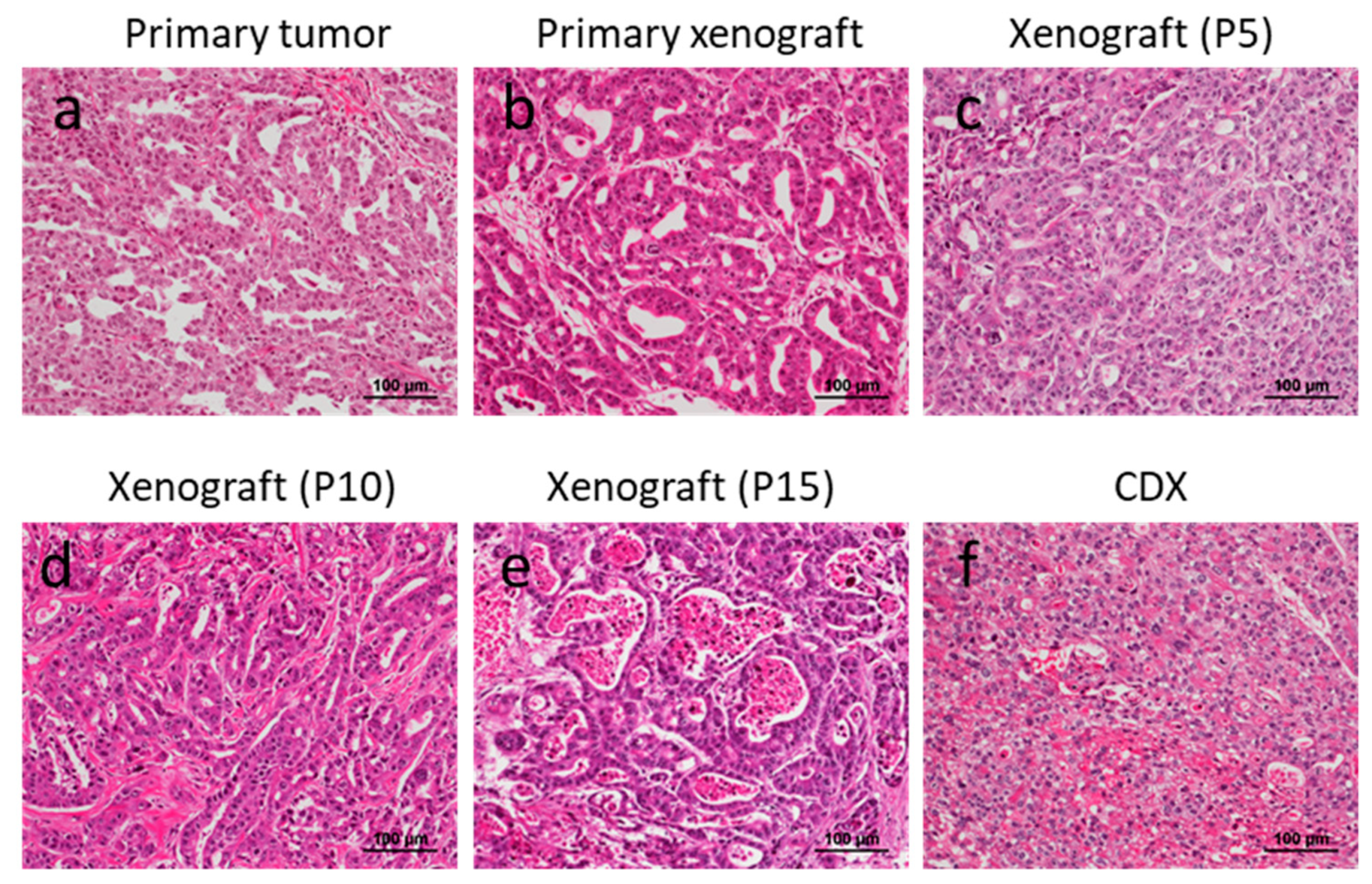
24]. In the present study, we have shown that most PDX tumors showed histologically consistent morphology with the primary tumors. Conversely, more than half of the CDX tumors showed discordance with the primary tumors in terms of histological differentiation grade. Although there may be several reasons to account for this discordance, one possibility is that the most aggressive and dedifferentiated clone(s) with higher proliferation activity, which are associated with poorly differentiated adenocarcinoma characteristics, take over the other clones during the culturing process for establishing cell lines. We also note the possibility that the relatively higher concentration of FCS (15%) used in the present study may have promoted the proliferation of more aggressive clones, although further studies are needed to confirm this. It is also noteworthy that PDX models were established more readily from differentiated adenocarcinomas, while cell line/CDXs were established more readily from poorly differentiated adenocarcinomas. Although the reason why differentiated adenocarcinoma was more readily established than poorly differentiated adenocarcinoma remains to be elucidated, one possibility is that the former places fewer demands on stromal cells. For example, poorly differentiated adenocarcinoma is known to utilize TGF-beta during stromal reactions, although human TGF-beta may not interact with mouse stromal cells.
It was reported previously that the success rate of PDX establishment is higher with more advanced lesions [
28]. In this study, we showed that lesions having LN metastases had a higher success rate compared with lesions without metastases. To our surprise, the existence of distant metastases (pM) failed to show a significant association with success rate. For establishing gastric cancer cell lines, the cells recovered from ascites fluid in CART cases showed a higher success rate than surgical cases. However, it should be noted that all of the CDXs derived from CART cases had a poorly differentiated phenotype.
In this study, a strong negative factor interfering with the establishment of PDXs was the development of LPLs. Previously, it was reported that 33.3% of these gastric cancer tissues developed lymphomas in NOG mice [
7]. In this present study, LPLs were observed at similar frequencies (30.6%, 61/272). Although the previous study reported that lymphoma development was specific to NOG mice, in this study, LPLs developed in not only NOG but also in SCID mice. More recently, Corso et al. reported the occurrence of lymphoma after gastric cancer tissue engraftment in NOD/SCID mice [
29]. We further identified that most of the LPLs were derived from B lymphocytes and were not EBV-associated, although Corso et al. observed that the lymphomas that developed in their study were EBV-associated. We do not deny the potential contribution of EBV in LPLs in the present study, however, as at least one of the cases showed diffuse EBER expression in proliferating B cells. Further studies will be needed to determine what percent of LPLs observed in this study are a clonal disease and whether the developing LPLs are specific for gastric cancer.
Our study has some limitations. First, intratumoral heterogeneity was not evaluated in this study. Second, because molecular classification is applied in various types of cancer, including gastric cancer [
30], it would be interesting to examine whether the molecular profiles were conserved between primary, PDX, and CDX tumors [
25]. Here, we have presented only a single case in which HER2 overexpression was observed in the primary, PDX, and CDX tumors. Other molecular profiles are under investigation and will be presented in the future. Third, none of the PDX or CDX models developed metastatic lesions in mice. Therefore, the models are not suitable for examining the mechanism of tumor metastasis. Fourth, since immunodeficient mice are required for the development of PDX/CDX models, these models are not suitable for the evaluation of immunotherapies unless a humanized immune system is restored by co-transplantation of immune cells from the same patient.

 ,
, 






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}