
Pharmacogenetic Testing of Cytochrome P450 Drug Metabolizing Enzymes in a Case Series of Patients with Prader-Willi Syndrome



Abstract
:1. Introduction
1.1. Prader-Willi Syndrome (PWS)
1.2. Pharmacogenetics of the Cytochrome P450 System
2. Methods
3. Results
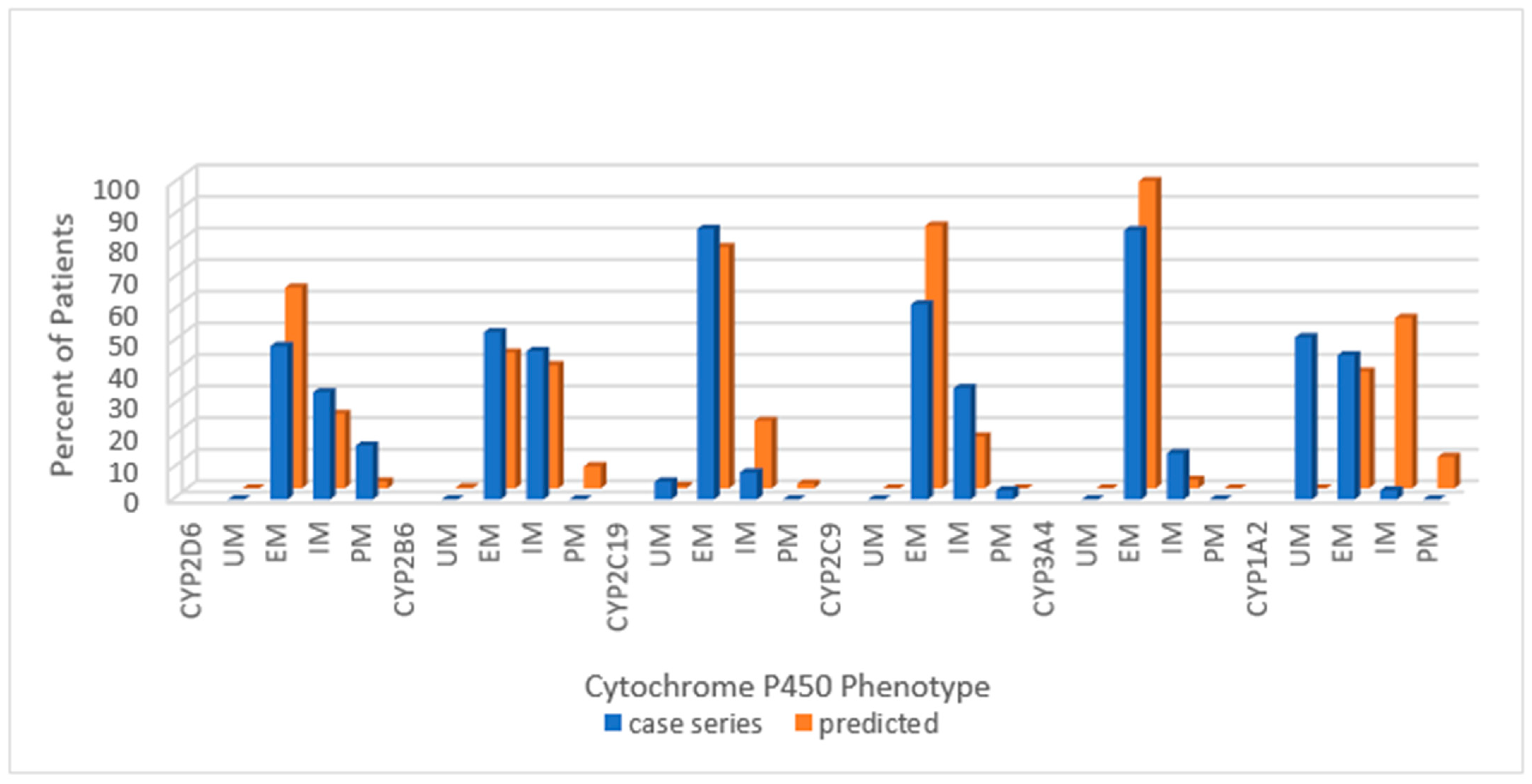
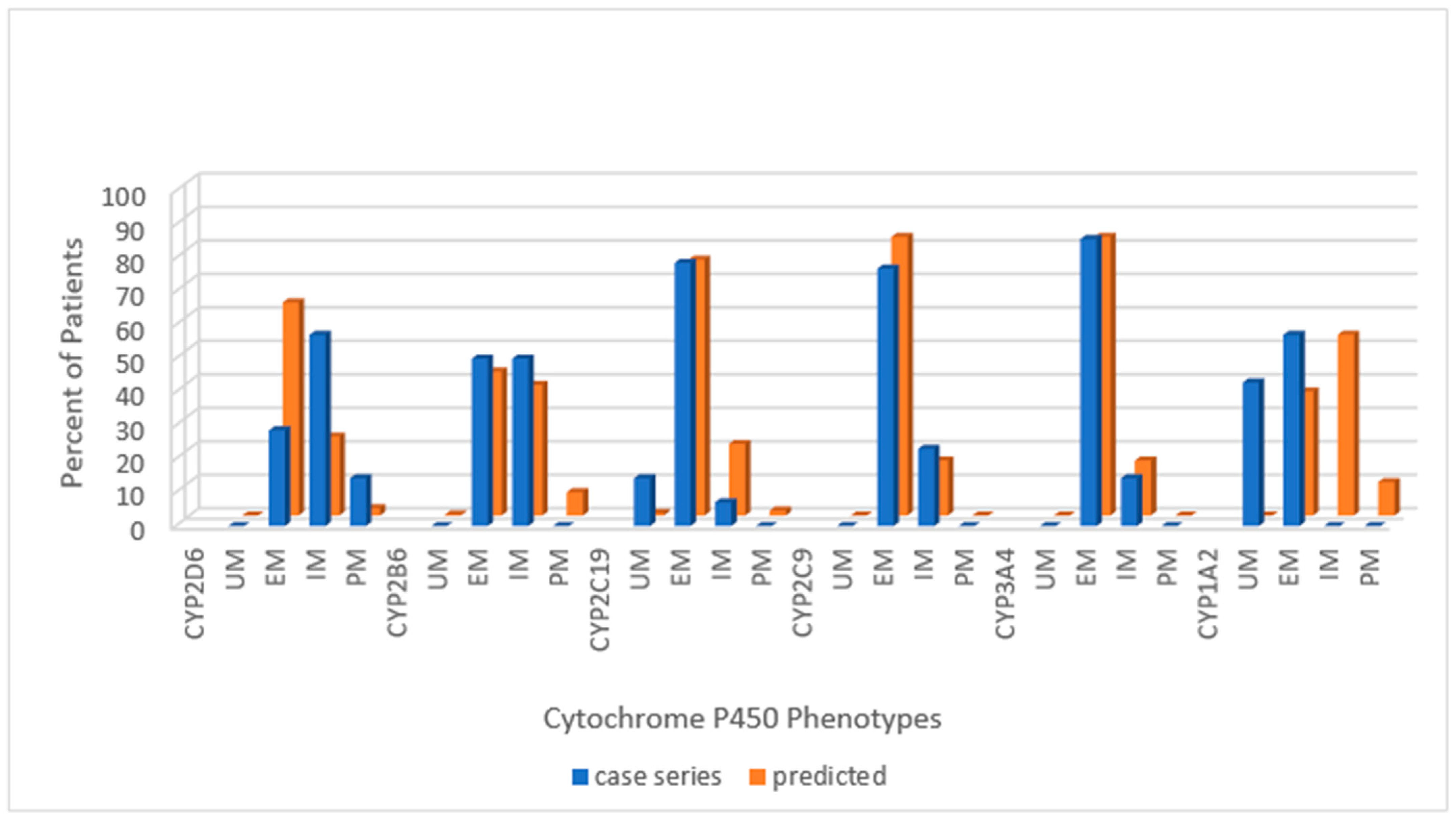
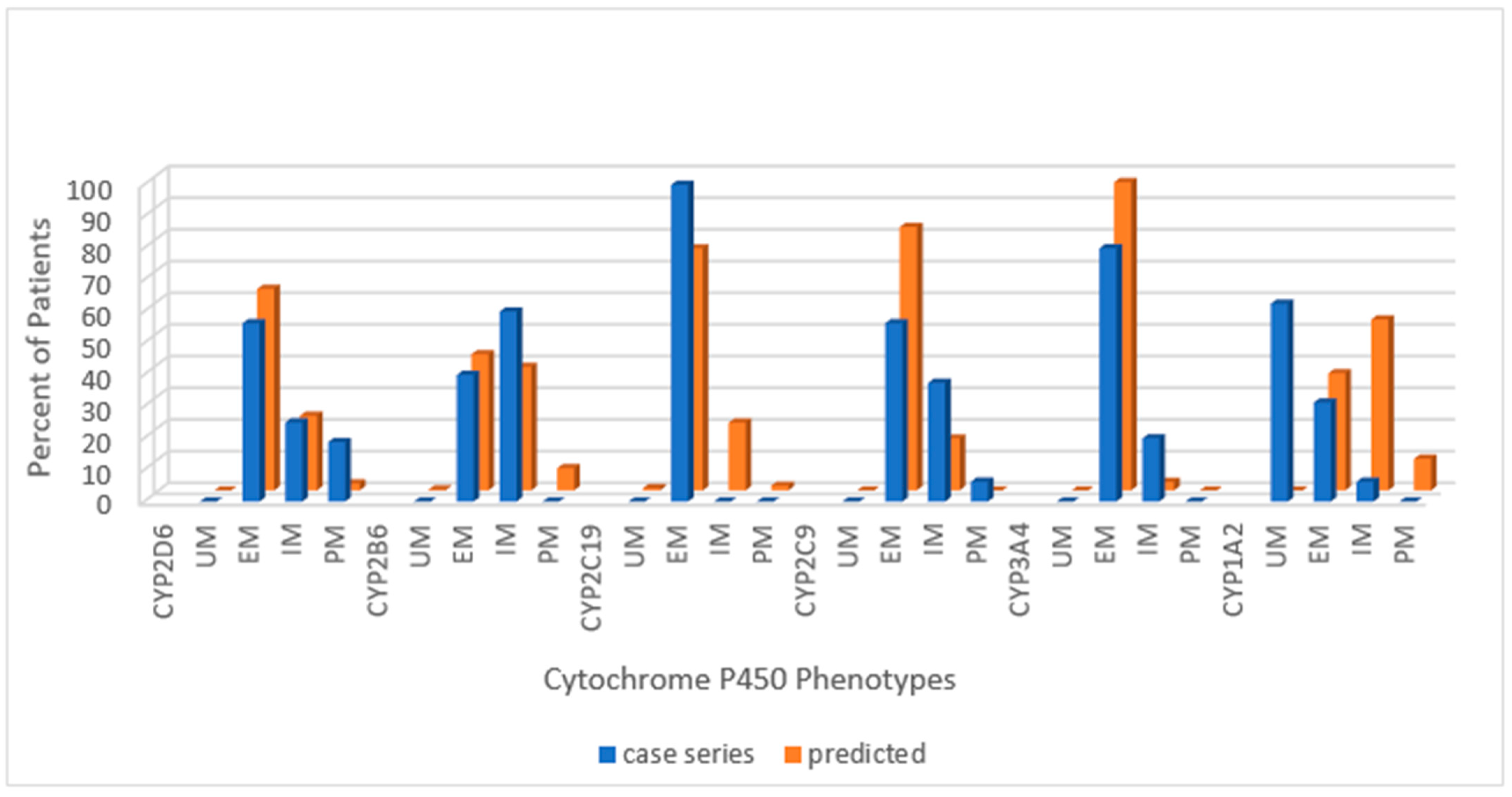
3.1. Cytochrome P450 Genotypes, Phenotypes and Genetic Subtype of PWS
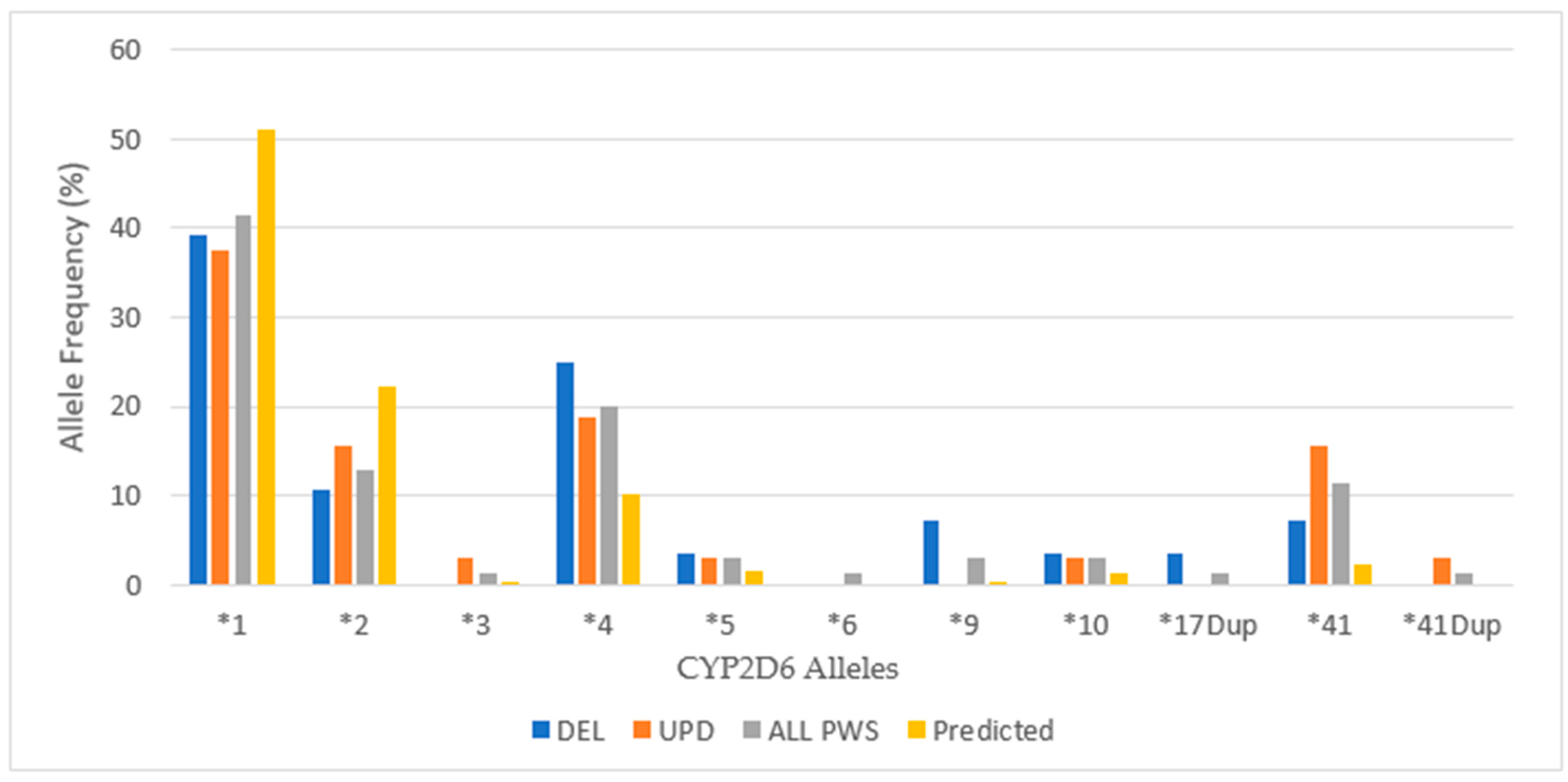
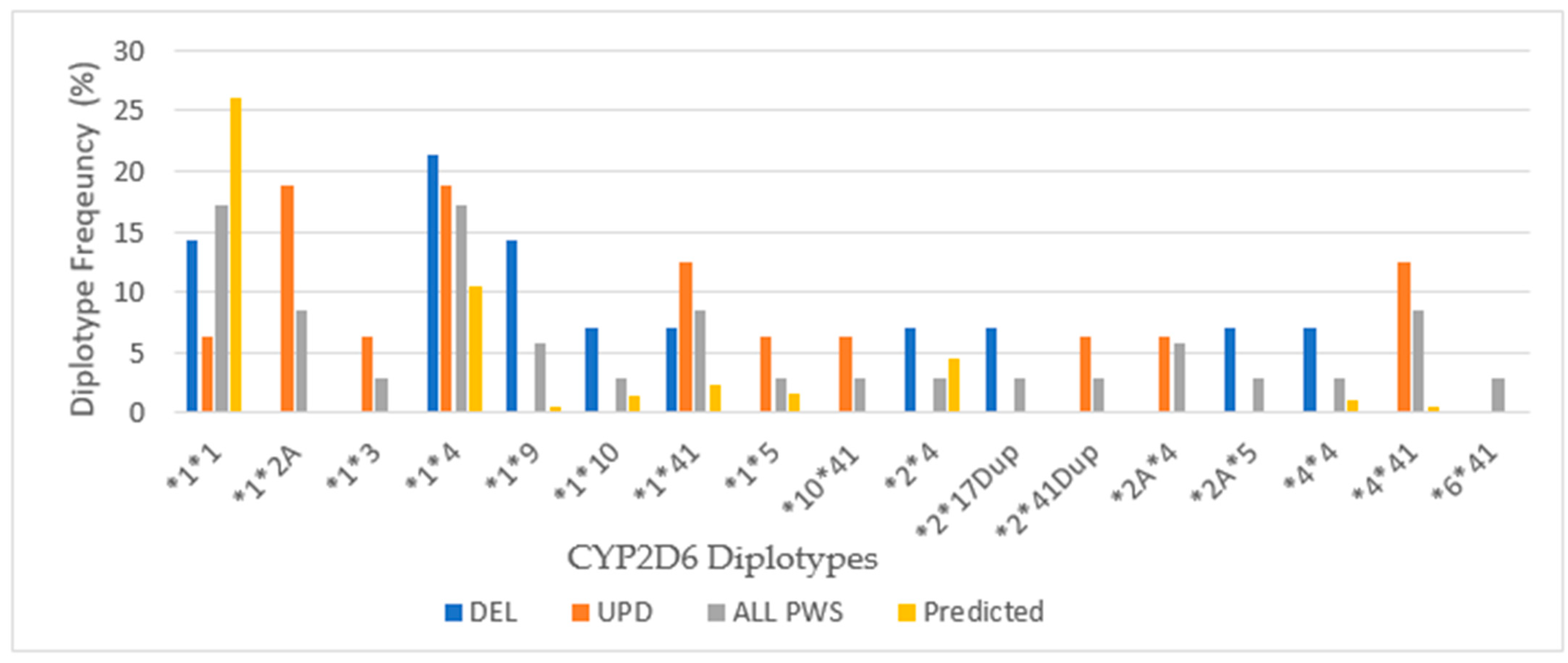
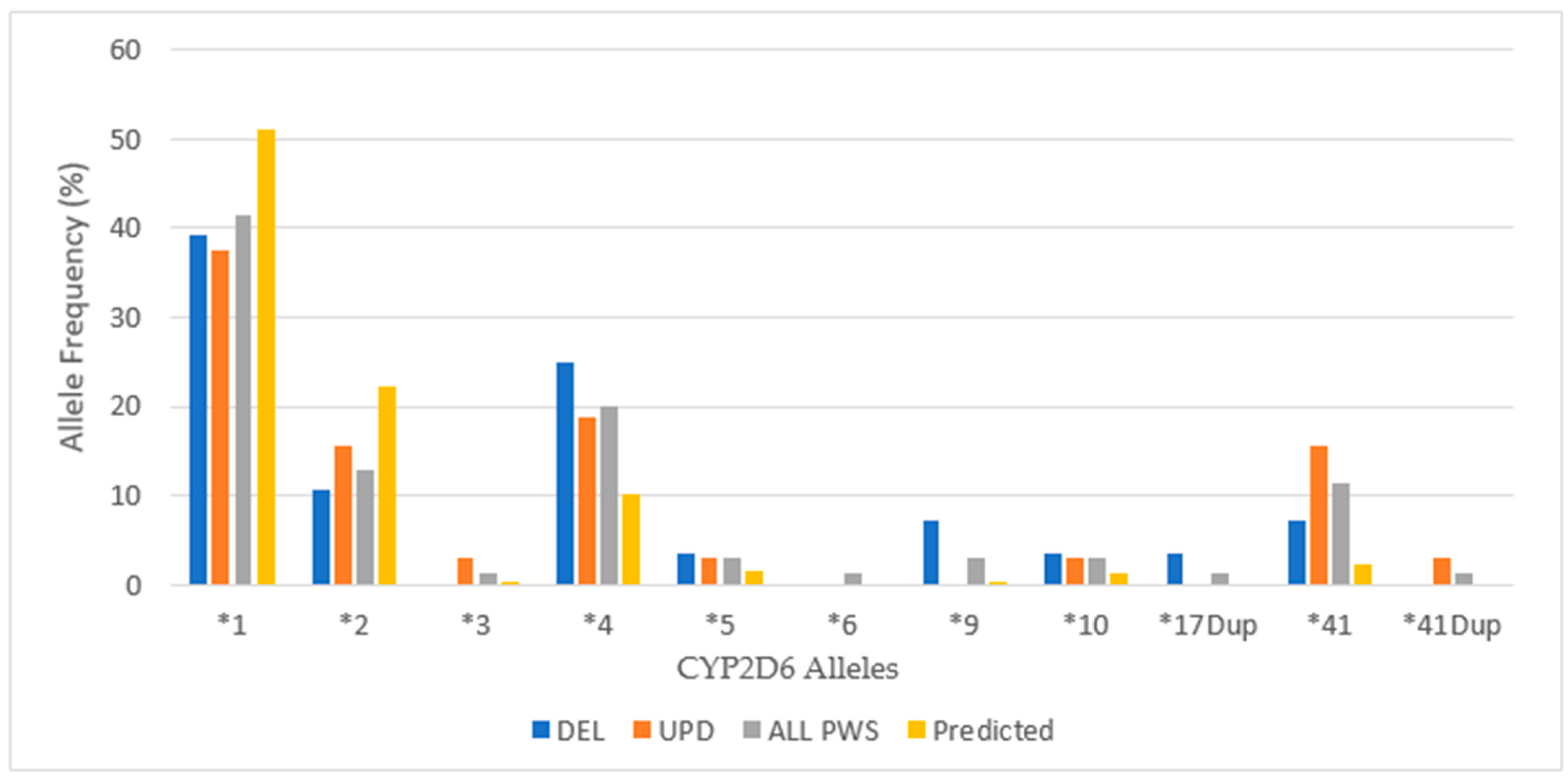
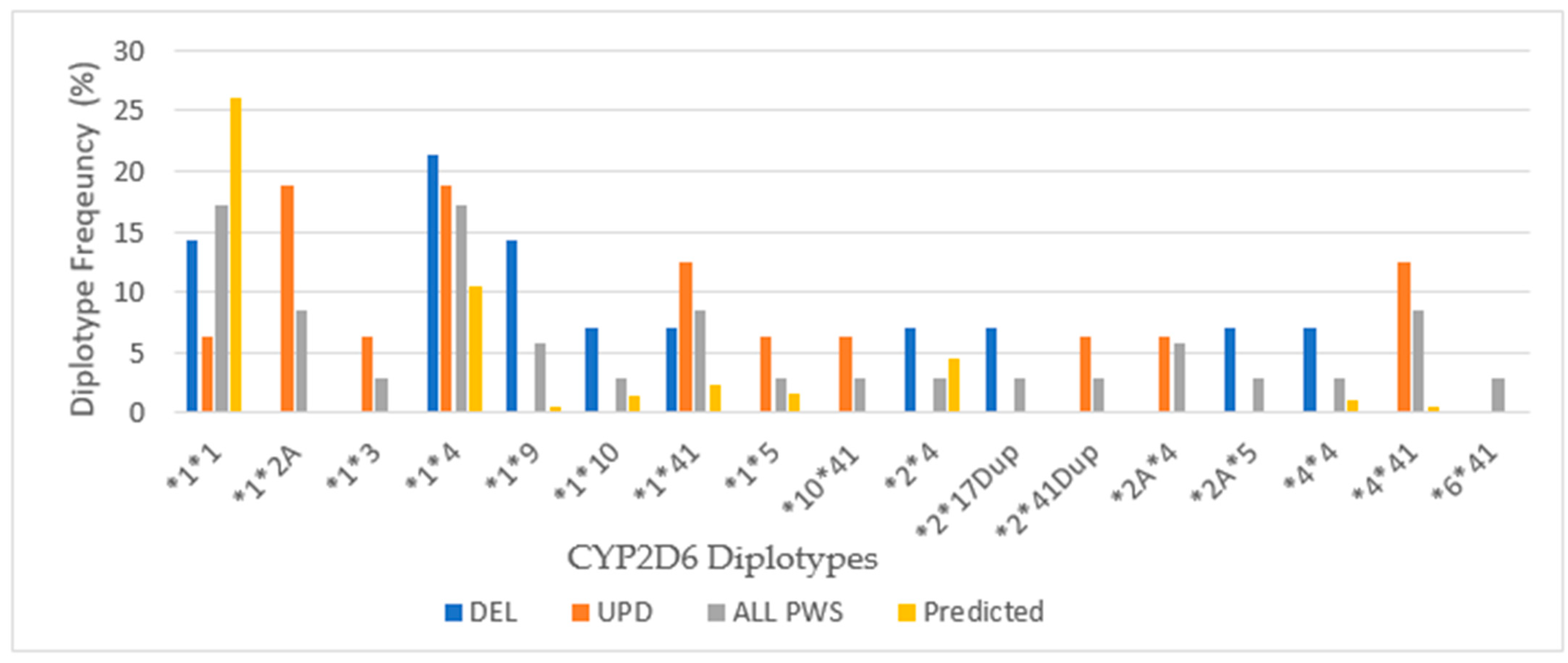
3.2. CYP2D6
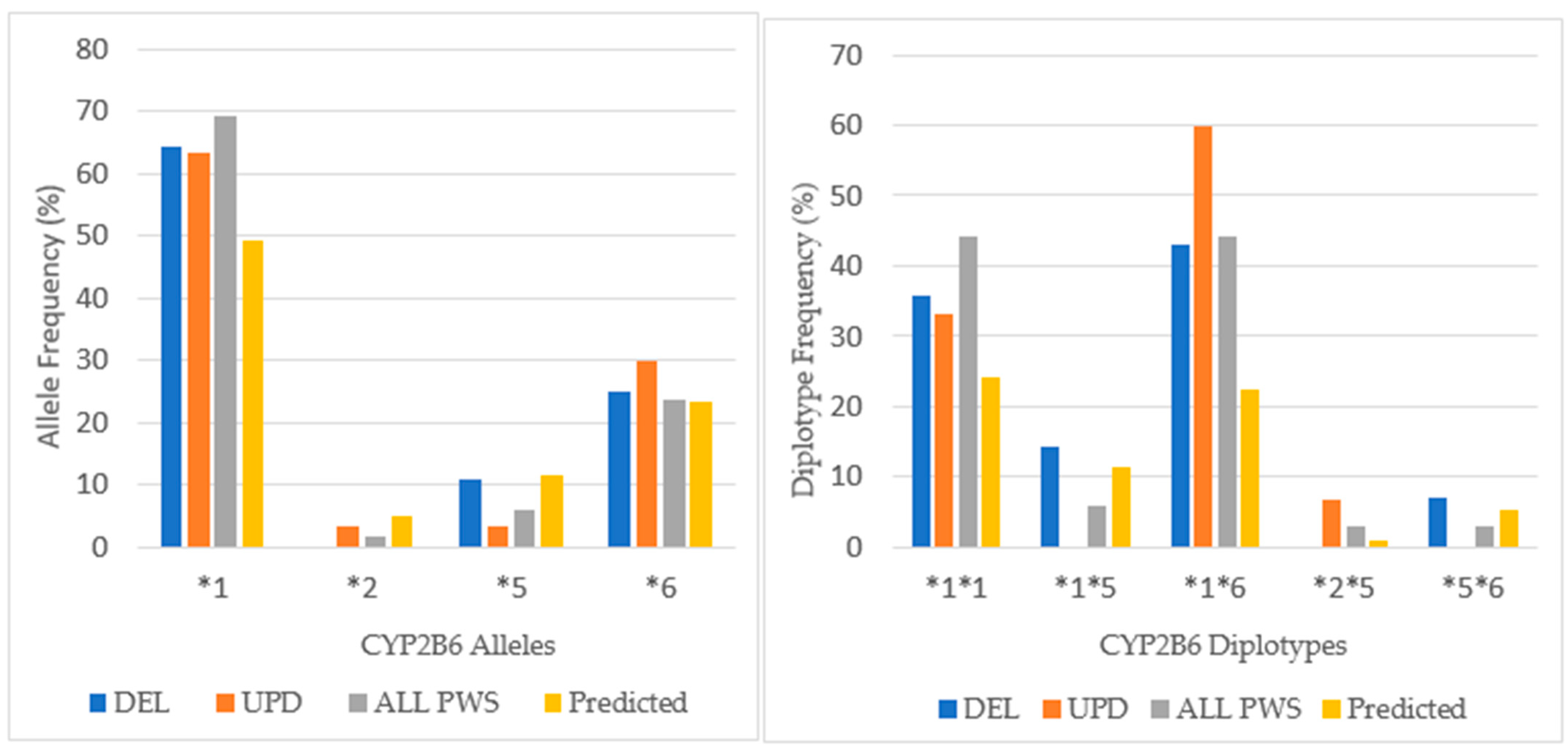
3.3. CYP2B6
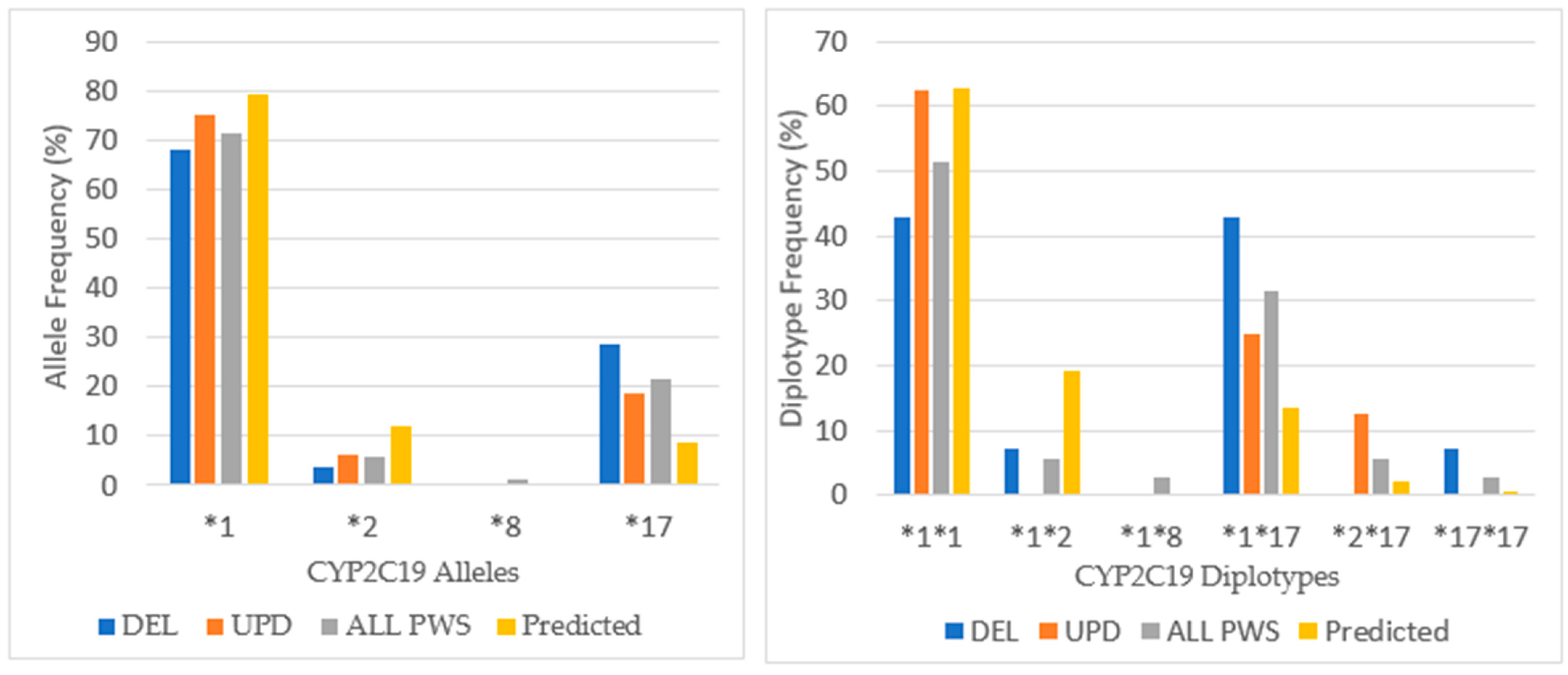
3.4. CYP2C19
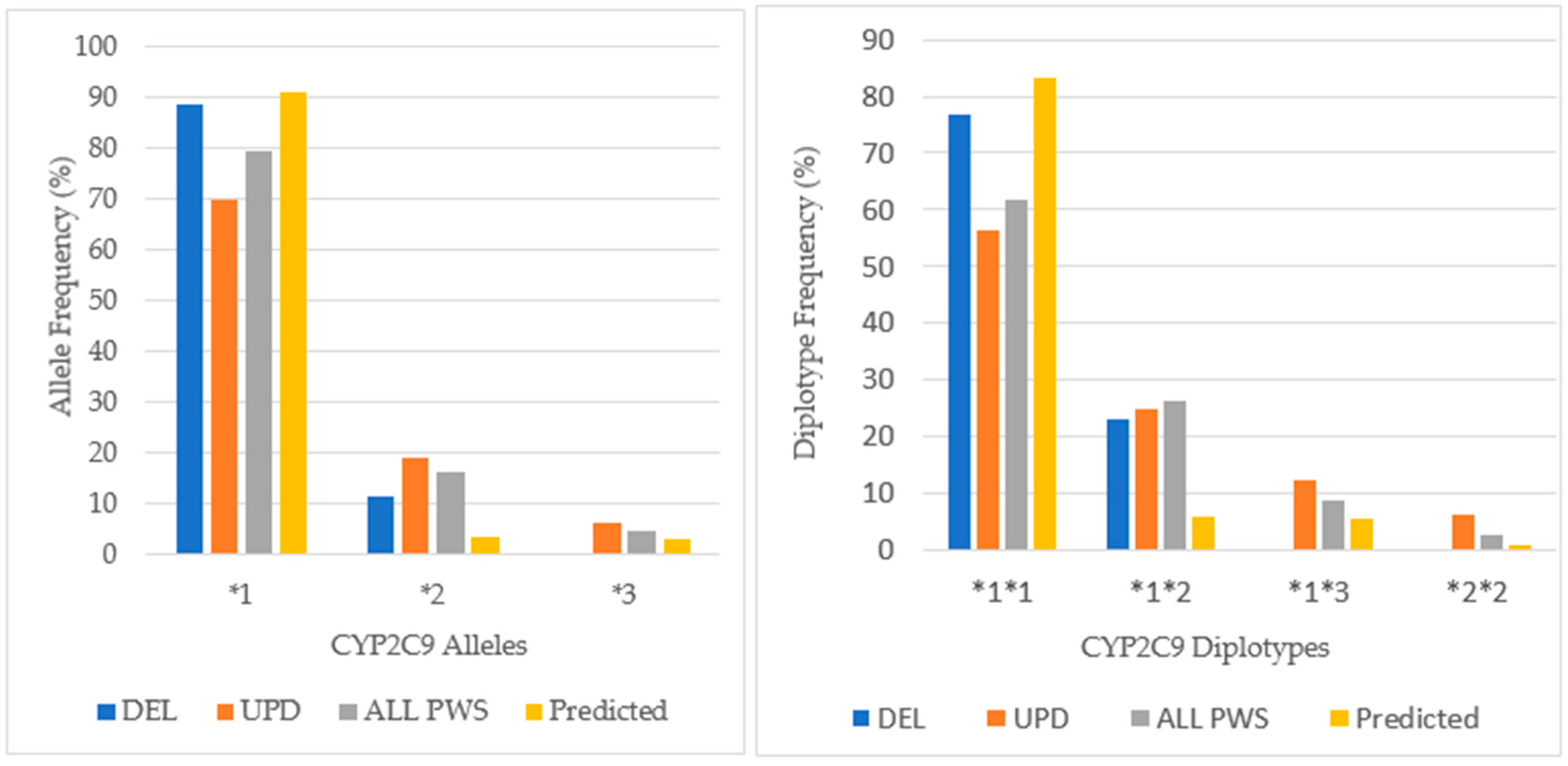
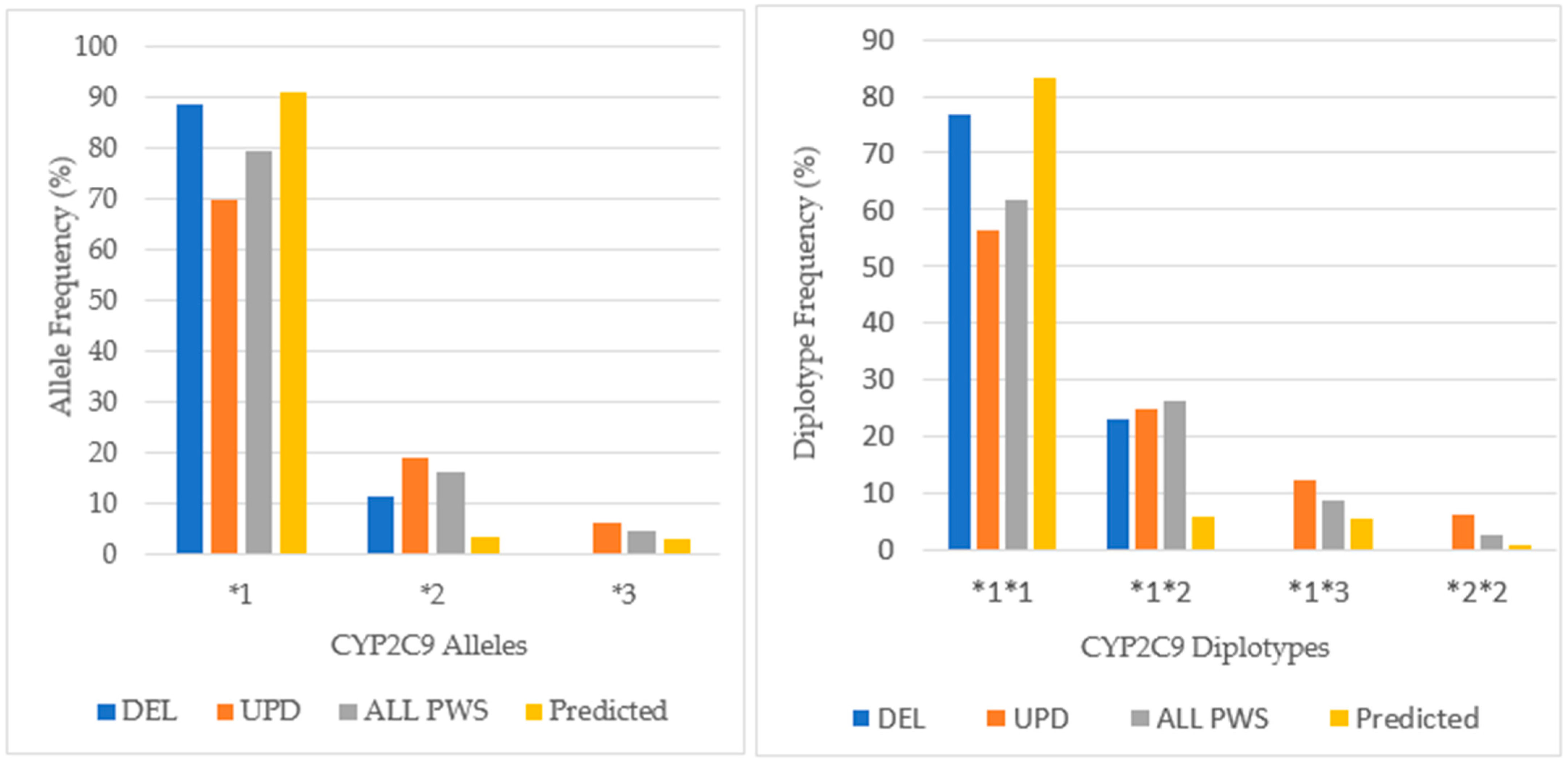
3.5. CYP2C9
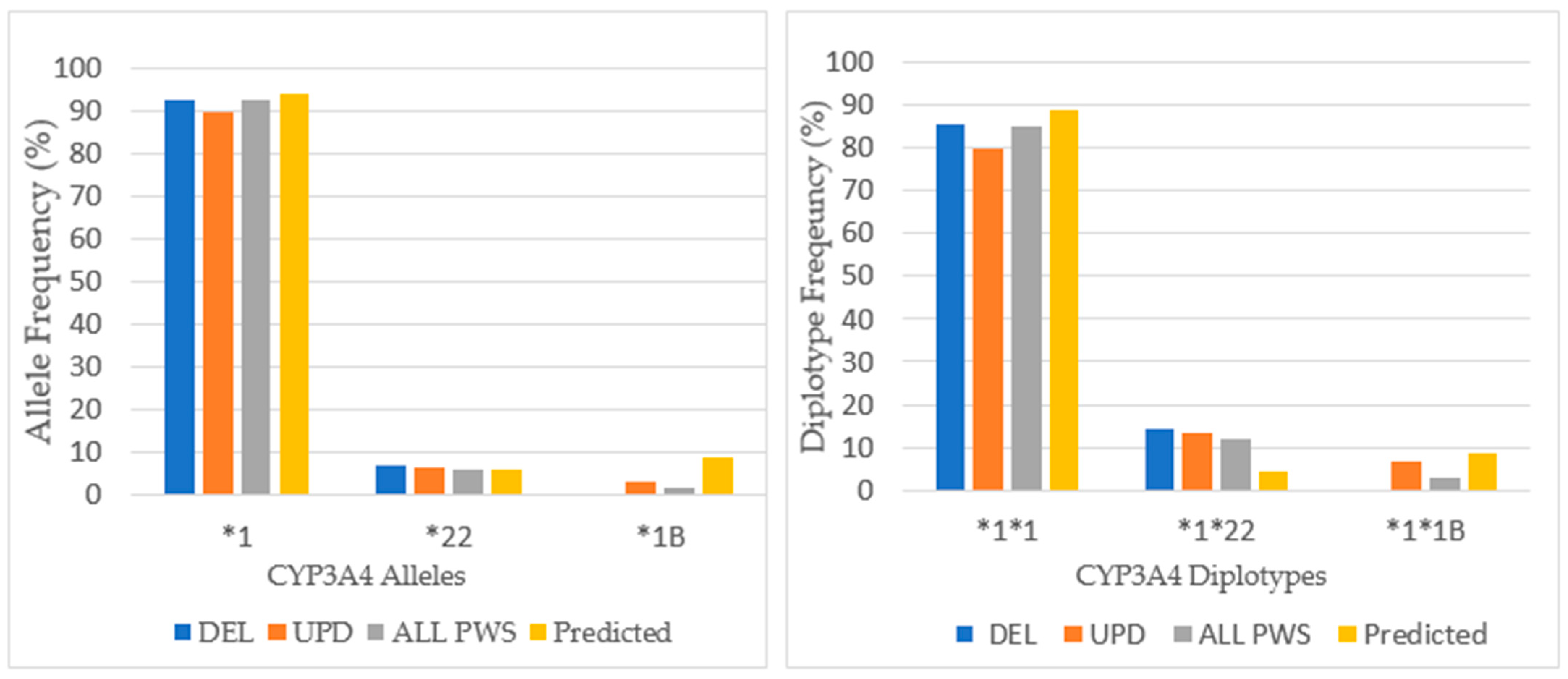
3.6. CYP3A4
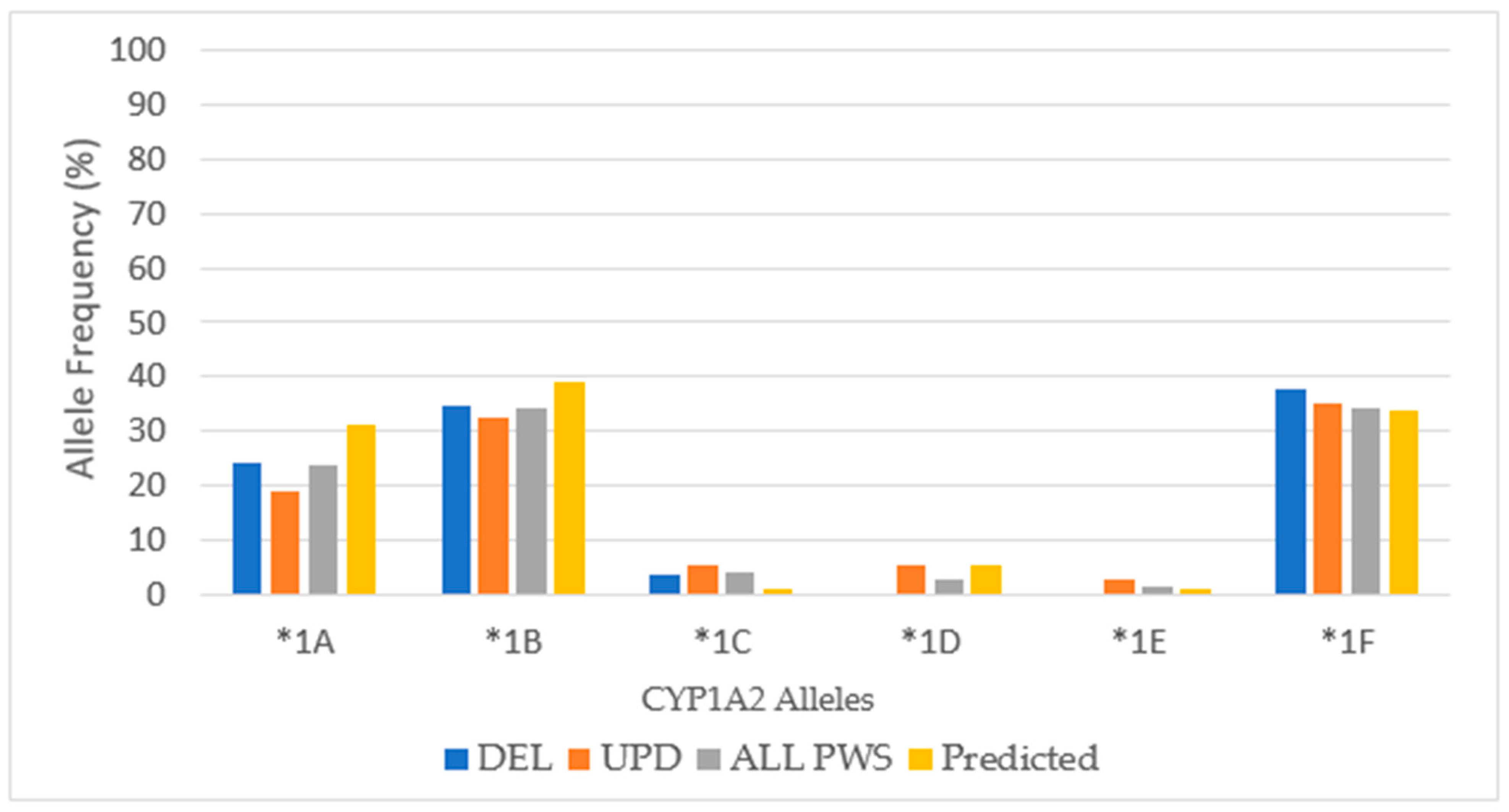
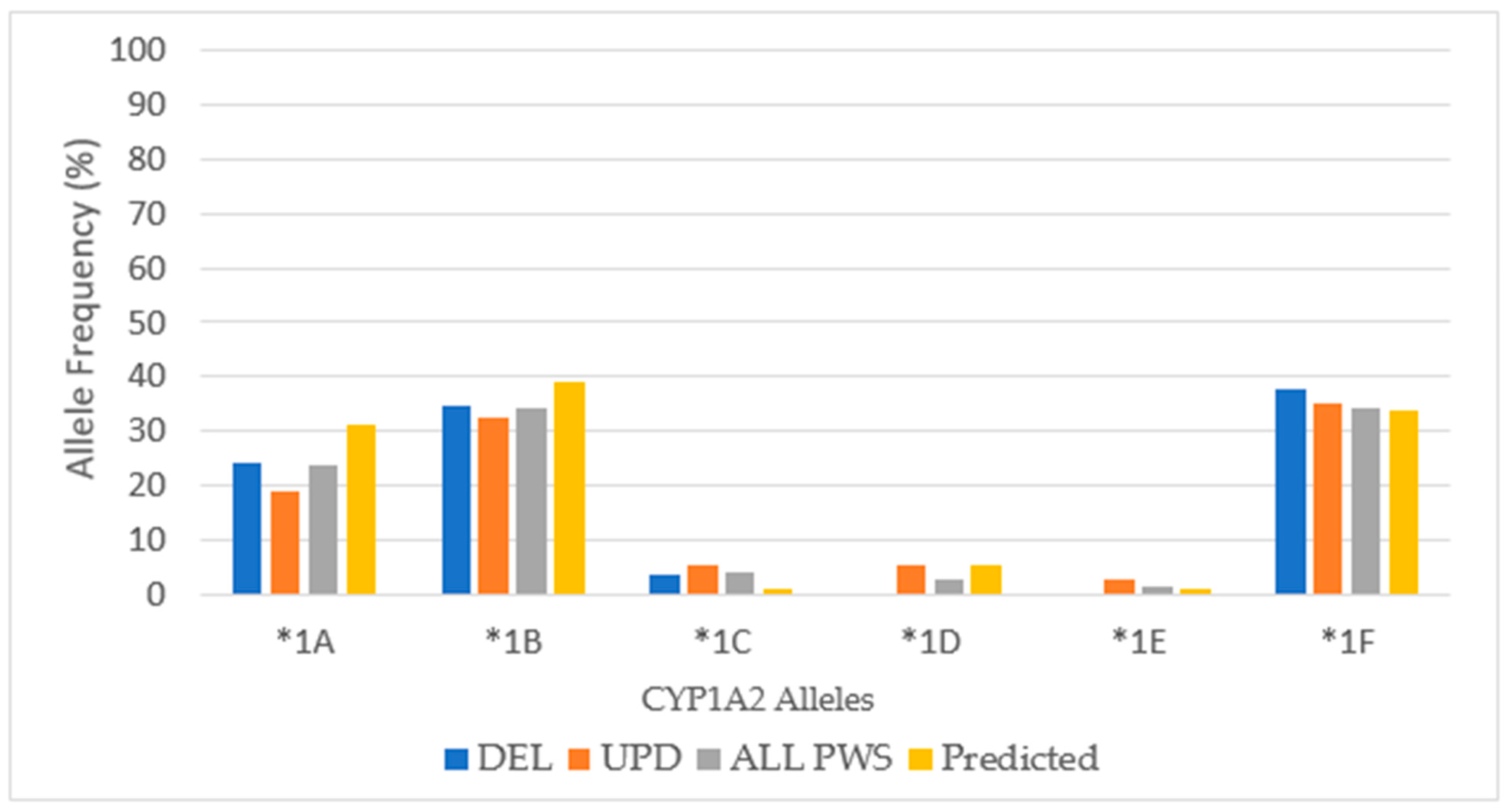
3.7. CYP1A2
4. Discussion
4.1. Drug–Drug Interactions
4.2. Specific Relevance of Cytochrome P450 Enzyme System to PWS
4.3. Non-Genetic Factors Affecting Drug Pharmacokinetics in PWS
4.4. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cytochrome P450 | Chromosome Location | Common Alleles and Phenotypic Action |
|---|---|---|
| CYP2D6 | 22q13.1 | *1 (wildtype); *2 (normal); *2A (increased action); *9, *10, *17, *41 (decreased action); *4, *3,* 5, *6 (inactive). |
| CYP2B6 | 19q13.2 | *1 (wildtype); *2, *5, *17 (normal); *4, *22 (increased action); *6, *7, *9, *16, *19, *20 (decreased action); *8, *12, *13, *18,*24 (inactive). |
| CYP2C19 | 10q24.1–q24.3 | *1 (wildtype); *11, *13, *15, *18,*28 (normal); *17 (increased action); *9, *10, *16, *19, *25, *26 (decreased action); *2-*8, *22, *24, *35-*37 (inactive). |
| CYP2C9 | 10q23.33 | *1 (wildtype); *9 (normal); *2, *3 (decreased action); *6, *15, *25 (inactive). |
| CYP3A4 | 7q22.1 | *1 (wildtype); *7, *9, *10 (normal); *1B, *2-*6, *8, *11-*13, *15-*18, *22 (decreased action); *20, *26 (inactive). |
| CYP1A2 | 15q24.1 | *1, *1A, *1B (wildtype); *1D (T-delT), *1F(C/A) increased action when induced; *1C(G/A); *1K(C/A); *3(T/C), *4(A/T), *7(G/A) (decreased action). |
| CYP2D6 | CYP2B6 | CYP2C19 | CYP2C9 | CYP3A4 | CYP1A2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lab | Alleles | PT | Alleles | PT | Alleles | PT | Alleles | PT | Alleles | PT | Alleles | PT |
| GS | *1/*1 | EM | *1/*6 | IM | *1/*1 | EM | *1/*1 | EM | *1/*1 | EM | *1F/*1B | UM |
| GS | *4/*41 | PM | *1/*6 | IM | *1/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1A/*1B | EM |
| GS | *2/*17 DUP | EM | *1/*6 | IM | *1/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1A/*1B | EM |
| GS | *2/*4 | IM | *1/*1 | EM | *1/*17 | EM | *1/*1 | EM | *1/*22 | IM | *1A/*1B | EM |
| GS | *1/*10 | IM | *1/*6 | IM | *17/*17 | UM | *1/*1 | EM | *1/*1 | EM | *1F/*1B | UM |
| GL | *2A/*5 | IM | *1/*5 | EM | *1/*1 | EM | NA | NA | *1/*22 | IM | *1A/*1A | EM |
| GS | *4/*4 | PM | *1/*1 | EM | *1/*1 | EM | *1/*1 | EM | *1/*1 | EM | *1F/*1B | UM |
| GS | *1/*41 | EM | *1/*1 | EM | *1/*2 | IM | *1/*1 | EM | *1/*1 | EM | *1F/*1B | UM |
| GS | *1/*9 | IM | *1/*6 | IM | *1/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1F/*1B | UM |
| GS | *1/*9 | IM | *1/*1 | EM | *1/*17 | EM | *1/*2 | IM | *1/*1 | EM | *1A/*1B | EM |
| GL | *1/*4 | IM | *1/*5 | EM | *1/*1 | EM | *1/*2 | IM | *1/*1 | EM | *1A/*1F | HI |
| GL | *1/*4 | IM | *1/*6 | IM | *1/*1 | EM | *1/*1 | EM | *1/*1 | EM | *1C*1F/*1F | HI |
| GS | *1/*4 | IM | *1/*1 | EM | *1/*1 | EM | *1/*2 | IM | *1/*1 | EM | *1F/*1B | UM |
| GL | *1/*1 | EM | *5/*6 | IM | *1/*17 | UM | *1/*1 | EM | *1/*1 | EM | *1F/*1F | HI |
| CYP2D6 | CYP2B6 | CYP2C19 | CYP2C9 | CYP3A4 | CYP1A2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lab | Alleles | PT | Alleles | PT | Alleles | PT | Alleles | PT | Alleles | PT | Alleles | PT |
| GS | *1/*1 | EM | *1/*6 | IM | *1/*1 | EM | *1/*1 | EM | *1/*1 | EM | *1C*1D/ *1F*1B | UM |
| GS | *1/*4 | IM | *1/*6 | IM | *1/*1 | EM | *1/*3 | IM | *1/*1 | EM | *1F/*1B | UM |
| GS | *1/*2A | EM | *1/*6 | IM | *1/*1 | EM | *1/*1 | EM | *1/*1 | EM | *1F/*1B | UM |
| GS | *1/*41 | EM | *1/*6 | IM | *1/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1A*1C/ *1B | IM |
| GS | *1/*4 | EM | *1/*6 | IM | *1/*1 | EM | *1/*2 | IM | *1/*1 | EM | *1D*1E/ *1F*1B | UM |
| GS | *2A/*4 | EM | *1/*1 | EM | *2/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1F/*1B | UM |
| GS | *1/*2A | EM | *1/*6 | IM | *1/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1F/*1B | UM |
| GS | *10/*41 | PM | *1/*1 | EM | *1/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1A/*1B | EM |
| GS | *1/*5 | IM | *1/*1 | EM | *1/*1 | EM | *1/*2 | IM | *1/*1 | EM | *1F/*1B | UM |
| GS | *1/*3 | IM | NA | NA | *1/*1 | EM | *1/*3 | IM | NA | NA | *1F/*1B | UM |
| GS | *1/*41 | EM | *1/*6 | IM | *2/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1A/*1A | EM |
| GS | *4/*41 | PM | *1/*1 | EM | *1/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1A/*1A | EM |
| GS | *4/*41 | PM | *1/*6 | IM | *1/*1 | EM | *2/*2 | PM | *1/*1 | EM | *1F/*1B | UM |
| GM | *2/*41 Dup | EM | *1/*6 | EM | *1/*1 | EM | *1/*1 | EM | *1/*22 | IM | *1A/*1F | EM |
| GS | *1/*4 | IM | *1/*1 | EM | *1/*1 | EM | *1/*2 | IM | *1/*22 | IM | *1F/*1B | UM |
| GL | *1/*2A | EM | *2/*5 | IM | *1/*1 | EM | *1/*2 | IM | *1/*1B | IM | *1F/*1F | HI |
| CYP2D6 | CYP2B6 | CYP2C19 | CYP2C9 | CYP3A4 | CYP1A2 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lab | Alleles | PT | Alleles | PT | Alleles | PT | Alleles | PT | Alleles | PT | Alleles | PT |
| GS | *2A/*4 | EM | *1/*1 | EM | *1/*1 | EM | *1/*3 | IM | *1/*1 | EM | *1A/*1B | EM |
| GS | *1/*1 | EM | *1/*1 | EM | *1/*8 | IM | *1/*2 | IM | *1/*1 | EM | *1F/*1B | UM |
| GS | *1/*1 | EM | *1/*1 | EM | *1/*1 | EM | *1/*2 | IM | *1/*1 | EM | *1A/*1B | EM |
| GS | *6/*41 | PM | *1/*1 | EM | *1/*17 | EM | *1/*1 | EM | *1/*1 | EM | *1F/*1B | UM |
| GS | *1/*1 | EM | *1/*1 | EM | *1/*2 | IM | *1/*1 | EM | *1/*1 | EM | *1A/*1A | EM |
| PWS | CYP2D6 | CYP2B6 | CYP2C19 | CYP2C9 | CYP3A4 | CYP1A2 |
|---|---|---|---|---|---|---|
| DEL | 4EM:8IM:2PM | 7EM:7IM | 2UM:11EM:1IM | 10EM:3IM | 12EM:2IM | 6UM:3HI:5EM |
| UPD | 9EM:4IM:3PM | 6EM:9IM | 16EM | 9EM:6IM:1PM | 12EM:3IM | 10UM:1HI:4EM:1IM |
| UnSpec | 4EM:1PM | 5EM | 3EM:2IM | 2EM:3IM | 5EM | 2UM:3EM |
References
- Butler, M.G.; Lee, P.D.K.; Whitman, B.Y. Management of Prader-Willi Syndrome; Springer: New York, NY, USA, 2006. [Google Scholar]
- Butler, M.G.; Hartin, S.N.; Hossain, W.A.; Manzardo, A.M.; Kimonis, V.; Dykens, E.; Gold, J.A.; Kim, S.J.; Weisensel, N.; Tamura, R.; et al. Molecular genetic classification in Prader-Willi syndrome: A multisite cohort study. J. Med. Genet. 2019, 56, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.G.; Manzardo, A.M.; Forster, J.L. Prader-Willi syndrome: Clinical genetics and diagnostic aspects with treatment approaches. Curr. Pediatr. Rev. 2016, 12, 136–166. [Google Scholar] [CrossRef] [PubMed]
- Miller, J.L.; Lynn, C.H.; Driscoll, D.C.; Goldstone, A.P.; Gold, J.A.; Kimonis, V.; Dykens, E.; Butler, M.G.; Shuster, J.J.; Dris-coll, D.J. Nutritional phases in Prader-Willi syndrome. Am. J. Med. Genet. A 2011, 155, 1040–1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crinò, A.; Fintini, D.; Bocchini, S.; Grugni, G. Obesity management in Prader-Willi syndrome: Current perspectives. Diabetes Metab. Syndr. Obes. 2018, 11, 579–593. [Google Scholar] [CrossRef] [Green Version]
- Skokauskas, N.; Sweeny, E.; Meehan, J.; Gallagher, L. Mental health problems in children with Prader-Willi syndrome. J. Can. Acad. Child. Adolesc. Psychiatry 2012, 21, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Zarcone, J.; Napolitano, D.; Peterson, C.; Breidbord, J.; Ferraioli, S.; Caruso-Anderson, M.; Holsen, L.; Butler, M.G.; Thomp-son, T. The relationship between compulsive behaviour and academic achievement across the three genetic subtypes of Prader-Willi syndrome. J. Intellect. Disabil. Res. 2007, 51 Pt 6, 478–487. [Google Scholar] [CrossRef]
- Novell-Alsina, R.; Esteba-Castillo, S.; Caixàs, A.; Gabau, E.; Giménez-Palop, O.; Pujol, J.; Deus, J.; Torrents-Rodas, D. Com-pulsions in Prader-Willi syndrome: Occurrence and severity as a function of genetic subtype. Actas Esp. Psiquiatr. 2019, 47, 79–87. [Google Scholar] [PubMed]
- Bennett, J.A.; Germani, T.; Haqq, A.M.; Zwaigenbaum, L. Autism spectrum disorder in Prader-Willi syndrome: A systematic review. Am. J. Med. Gen. A 2015, 167, 2936–2944. [Google Scholar] [CrossRef]
- Sinnema, M.; Boer, H.; Collin, P.; Maaskant, M.A.; van Roozendaal, K.E.; Schrander-Stumpel, C.T.; Curfs, L.M. Psychiatric illness in a cohort of adults with Prader-Willi syndrome. Res. Dev. Disabil. 2011, 32, 1729–1735. [Google Scholar] [CrossRef]
- Manzardo, A.M.; Weisensel, N.; Ayala, S.; Hossain, W.; Butler, M.G. Prader-Willi syndrome genetic subtypes and clinical neuropsychiatric diagnoses in residential care adults. Clin. Genet. 2018, 93, 622–631. [Google Scholar] [CrossRef]
- Butler, M.G.; Kimonis, V.; Dykens, E.; Gold, J.A.; Miller, J.; Tamura, R.; Driscoll, D.J. Prader-Willi syndrome and early-onset morbid obesity NIH rare disease consortium: A review of natural history study. Am. J. Med. Genet. A 2018, 176, 368–375. [Google Scholar] [CrossRef] [PubMed]
- Forster, J.L. Pearls: Use of psychotropic medication in PWS. In Proceedings of the Scientific Conference of the Prader-Willi Syndrome Association-USA Conference, Orlando, FL, USA, 23–24 October 2019. [Google Scholar]
- Samer, C.F.; Lorenzini, K.I.; Rollason, V.; Daali, Y.; Desmeules, J.A. Applications of CYP450 testing in the clinical setting. Mol. Diag. 2013, 17, 165–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miksys, S.L.; Tyndale, R.F. Drug-metabolizing cytochrome P450s in the brain. J. Psychiatry Neurosci. 2002, 27, 406–415. [Google Scholar] [PubMed]
- Nebert, D.W.; Wikvall, K.; Miller, W.L. Human cytochromes P450 in health and disease. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2013, 368, 20120431. [Google Scholar] [CrossRef] [PubMed]
- Zanger, U.M.; Schwab, M. Cytochrome P450 enzymes in drug metabolism: Regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef]
- Butler, M.G. Pharmacogenetics and psychiatric care: A review and commentary. J. Ment. Health Clin. Psychol. 2018, 2, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Gross, T.; Daniel, J. Overview of pharmacogenomic testing in clinical practice. Ment. Health Clin. 2018, 8, 235–241. [Google Scholar] [CrossRef]
- Zhou, Y.; Ingelman-Sundberg, M.; Lauschke, V.M. Worldwide distribution of cytochrome P450 alleles: A meta-analysis of population-scale sequencing projects. Clin. Pharm. 2017, 102, 688–700. [Google Scholar] [CrossRef] [Green Version]
- Roof, E.; Dykens, E. The use of psychotropic medications in Prader-Willi syndrome. Gathered View 2006, 31, 3. [Google Scholar]
- Durette, J.R.; Gourash, L.G.; Forster, J.L. Risks and benefits of SSRI medication in young people with PWS. In Proceedings of the PWSA Scientific Conference, Baton Rouge, LA, USA, 17–20 October 2012. [Google Scholar]
- Gourash, L.M.; Durette, J.R.; Forster, J.L. SSRI medication in children, adolescents and young adults with PWS: A cautionary report. In Proceedings of the PWS Mental Health Research Strategy Workshop, Bethesda, ML, USA, 1–3 March 2015. [Google Scholar]
- Martis, S.; Peter, I.; Hulot, J.S.; Kornreich, R.; Desnick, R.J.; Scott, S.A. Multi-ethnic distribution of clinically relevant CYP2C genotypes and haplotypes. Pharm. J. 2013, 13, 369–377. [Google Scholar] [CrossRef] [Green Version]
- Li-Wan-Po, A.; Girard, T.; Farndon, P.; Cooley, C.; Lithgow, J. Pharmacogenetics of CYP2C19: Functional and clinical im-plications of a new variant CYP2C19*17. Br. J. Clin. Pharmacol. 2010, 69, 222–230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, M.A.; Lang, N.P.; Young, J.F.; Caporaso, N.E.; Vineis, P.; Hayes, R.B.; Teitel, C.H.; Massengill, J.P.; Lawsen, M.F.; Kadlubar, F.F. Determination of CYP1A2 and NAT2 phenotypes in human populations by analysis of caffeine urinary me-tabolites. Pharmacogenetics 1992, 2, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Muscat, J.E.; Pittman, B.; Kleinman, W.; Lazarus, P.; Stellman, S.D.; Richie, J.P., Jr. Comparison of CYP1A2 and NAT2 pheno-types between black and white smokers. Biochem. Pharmacol. 2008, 76, 929–937. [Google Scholar] [CrossRef] [Green Version]
- Al-Ahmad, M.M.; Amir, N.; Dhanasekaran, S.; John, A.; Abdulrazzaq, Y.M.; Ali, B.R.; Bastaki, S. Genetic polymorphisms of cytochrome P450-1A2 (CYP1A2) among Emiratis. PLoS ONE 2017, 12, e0183424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wehry, A.M.; Ramsey, L.; Dulemba, S.E.; Mossman, S.A.; Strawn, J.R. Pharmacogenomic Testing in Child and Adolescent Psychiatry: An Evidence-Based Review. Curr. Probl. Pediatr. Adol. Health Care 2018, 48, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Kirchheiner, J.; Nickchen, K.; Bauer, M.; Wong, M.L.; Licinio, J.; Roots, I.; Brockmöller, J. Pharmacogenetics of antidepres-sants and antipsychotics: The contribution of allelic variations to the phenotype of drug response. Mol. Psychiatry 2004, 9, 442–473. [Google Scholar] [CrossRef] [PubMed]
- Flockhart, D.A.; Oesterheld, J.R. Cytochrome P450-mediated drug interactions. Child. Adolesc. Psychiatr. Clin. N. Am. 2000, 9, 43–76. [Google Scholar] [CrossRef] [PubMed]
- Flockhart, D.A. Drug Interactions: Cytochrome P450 Drug Interaction Table. Indiana University School of Medicine. 2007. Available online: https://drug-interactions.medicine.iu.edu (accessed on 12 July 2020).
- Zeigler-Johnson, C.M.; Walker, A.H.; Mancke, B.; Spangler, E.; Jalloh, M.; McBride, S.; Deitz, A.; Malkowicz, S.B.; Ofori-Adjei, D.; Gueye, S.M.; et al. Ethnic differences in the frequency of prostate cancer susceptibility alleles at SRD5A32 and CYP3A4. Hum. Hered. 2002, 54, 13–21. [Google Scholar] [CrossRef]
- Saiz-Rodríguez, M.; Almenara, S.; Navares-Gómez, M.; Ochoa, D.; Román, M.; Zubiaur, P.; Koller, D.; Santos, M.; Mejía, G.; Borobia, A.M.; et al. Effect of the Most Relevant CYP3A4 and CYP3A5 Polymorphisms on the Pharmacokinetic Parameters of 10 CYP3A Substrates. Biomedicines 2020, 8, 94. [Google Scholar] [CrossRef]
- Elens, L.; van Gelder, T.; Hesselink, D.A.; Haufroid, V.; van Schaik, R.H. CYP3A4*22: Promising newly identified CYP3A4 variant allele for personalizing pharmacotherapy. Pharmacogenomics 2013, 14, 47–62. [Google Scholar] [CrossRef]
- Świechowski, R.; Jeleń, A.; Mirowski, M.; Talarowska, M.; Gałecki, P.; Pietrzak, J.; Wodziński, D.; Balcerczak, E. Estimation of CYP3A4*1B single nucleotide polymorphism in patients with recurrent Major Depressive Disorder. Mol. Genet. Genom. Med. 2019, 7, e669. [Google Scholar] [CrossRef] [PubMed]
- Sachse, C.; Bhambra, U.; Smith, G.; Lightfoot, T.J.; Barrett, J.H.; Scollay, J.; Garner, R.C.; Boobis, A.R.; Wolf, C.R.; Gooderham, N.J. Colorectal Cancer Study Group Polymorphisms in the cytochrome P450 CYP1A2 gene (CYP1A2) in colorectal cancer patients and controls: Allele frequencies, linkage disequilibrium and influence on caffeine metabolism. Br. J. Clin. Pharm. 2003, 55, 68–76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mrazek, D. Psychiatric Pharmacogenomics; Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Bradley, P.; Shiekh, M.; Mehra, V.; Vrbicky, K.; Layle, S.; Olson, M.C.; Maciel, A.; Cullors, A.; Garces, J.A.; Lukowiak, A.A. Improved efficacy with targeted pharmacogenetic-guided treatment of patients with depression and anxiety: A randomized clinical trial demonstrating clinical utility. J. Psychiatr. Res. 2018, 96, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Greden, J.F.; Parikh, S.V.; Rothschild, A.J.; Thase, M.E.; Dunlop, B.W.; DeBattista, C.; Conway, C.R.; Forester, B.P.; Mondimore, F.M.; Shelton, R.C.; et al. Impact of pharmacogenomics on clinical outcomes in major depressive disorder in the GUIDED trial: A large, patient- and rater-blinded, randomized, controlled study. J. Psychiatr. Res. 2019, 111, 59–67. [Google Scholar] [CrossRef]
- Takahashi, P.Y.; Ryu, E.; Pathak, J.; Jenkins, G.D.; Batzler, A.; Hathcock, M.A.; Black, J.L.; Olson, J.E.; Cerhan, J.R.; Bielinski, S.J. Increased risk of hospitalization for ultra-rapid metabolizers of cytochrome P450 2D6. Pharm. Pers. Med. 2017, 10, 39–47. [Google Scholar] [CrossRef] [Green Version]
- Ruaño, G.; Szarek, B.L.; Villagra, D.; Gorowski, K.; Kocherla, M.; Seip, R.L.; Goethe, J.W.; Schwartz, H.I. Length of psychiatric hospitalization is correlated with CYP2D6 functional status in inpatients with major depressive disorder. Biomark. Med. 2013, 7, 429–439. [Google Scholar] [CrossRef] [Green Version]
- Laika, B.; Leucht, S.; Heres, S.; Steimer, W. Intermediate metabolizer: Increased side effects in psychoactive drug therapy. The key to cost-effectiveness of pretreatment CYP2D6 screening? Pharm. J. 2009, 9, 395–403. [Google Scholar] [CrossRef]
- Seeringer, A.; Kirchheiner, J. Pharmacogenetics-guided dose modifications of antidepressants. Clin. Lab. Med. 2008, 28, 619–626. [Google Scholar] [CrossRef]
- Mrazek, D.A. Psychiatric pharmacogenomic testing in clinical practice. Dialogues Clin. Neurosci. 2010, 12, 69–76, PMCID:PMC3181940. [Google Scholar] [PubMed]
- Fallah, M.S.; Shaikh, M.R.; Neupane, B.; Rusiecki, D.; Bennett, T.A.; Beyene, J. Atypical Antipsychotics for Irritability in Pe-diatric Autism: A Systematic Review and Network Meta-Analysis. J. Child. Adolesc. Psychopharmacol. 2019, 29, 168–180. [Google Scholar] [CrossRef]
- Troost, P.W.; Lahuis, B.E.; Hermans, M.H.; Buitelaar, J.K.; van Engeland, H.; Scahill, L.; Minderaa, R.B.; Hoekstra, P.J. Prolac-tin release in children treated with risperidone: Impact and role of CYP2D6 metabolism. J. Clin. Psychopharmacol. 2007, 27, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Oshikoya, K.A.; Neely, K.M.; Carroll, R.J.; Aka, I.T.; Maxwell-Horn, A.C.; Roden, D.M.; Van Driest, S.L. CYP2D6 genotype and adverse events to risperidone in children and adolescents. Pediatr. Res. 2019, 85, 602–606. [Google Scholar] [CrossRef] [PubMed]
- Guengerich, F.P. A history of the roles of cytochrome P450 enzymes in the toxicity of drugs. Toxicol. Res. 2020, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Klomp, S.D.; Manson, M.L.; Guchelaar, H.J.; Swen, J.J. Phenoconversion of Cytochrome P450 Metabolism: A Systematic Re-view. J. Clin. Med. 2020, 9, 2890. [Google Scholar] [CrossRef] [PubMed]
- Kiss, Á.; Menus, Á.; Tóth, K.; Déri, M.; Sirok, D.; Gabri, E.; Belic, A.; Csukly, G.; Bitter, I.; Monostory, K. Phenoconversion of CYP2D6 by inhibitors modifies aripiprazole exposure. Eur. Arch. Psychiatry Clin. Neurosci. 2020, 270, 71–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kloosterboer, S.M.; McGuire, T.; Deckx, L.; Moses, G.; Verheij, T.; van Driel, M.L. Self-medication for cough and the common cold: Information needs of consumers. Aust. Fam. Physician 2015, 44, 497–501. [Google Scholar] [PubMed]
- Härtter, S.; Wang, X.; Weigmann, H.; Friedberg, T.; Arand, M.; Oesch, F.; Hiemke, C. Differential effects of fluvoxamine and other antidepressants on the biotransformation of melatonin. J. Clin. Psychopharm. 2001, 21, 167–174. [Google Scholar] [CrossRef] [Green Version]
- Woroń, J.; Siwek, M. Unwanted effects of psychotropic drug interactions with medicinal products and diet supplements containing plant extracts. Psychiatry Pol. 2018, 52, 983–996. [Google Scholar] [CrossRef]
- Zhang, X.L.; Chen, M.; Zhu, L.L.; Zhou, Q. Therapeutic risk and benefits of concomitantly using herbal medicines and con-ventional medicines: From the perspectives of evidence based on randomized controlled trials and clinical risk manage-ment. Evid. Based Complement. Altern. Med. 2017, 2017, 9296404. [Google Scholar] [CrossRef]
- Lucas, C.J.; Galettis, P.; Schneider, J. The pharmacokinetics and the pharmacodynamics of cannabinoids. Br. J. Clin Pharmacol. 2018, 84, 2477–2482. [Google Scholar] [CrossRef] [Green Version]
- Miller, L.J.; Girgis, C.; Gupta, R. Depression and related disorders during the female reproductive cycle. Women’s Health (Lond.) 2009, 5, 577–587. [Google Scholar] [CrossRef] [PubMed]
- Roomruangwong, C.; Carvalho, A.F.; Comhaire, F.; Maes, M. Lowered plasma steady-state levels of progesterone com-bined with declining progesterone levels during the luteal phase predict peri-menstrual syndrome and its major subdo-mains. Front. Psychol. 2019, 10, 2446. [Google Scholar] [CrossRef] [PubMed]
- Sinués, B.; Mayayo, E.; Fanlo, A.; Mayayo, E., Jr.; Bernal, M.L.; Bocos, P.; Bello, E.; Labarta, J.I.; Ferrández-Longás, A. Effects of growth hormone deficiency and rhGH replacement therapy on the 6beta-hydroxycortisol/free cortisol ratio, a marker of CYP3A activity, in growth hormone-deficient children. Eur. J. Clin. Pharm. 2004, 60, 559–564. [Google Scholar] [CrossRef]
- Landi, M.T.; Sinha, R.; Lang, N.P.; Kadlubar, F.F. Human cytochrome P4501A2. IARC Sci. Publ. 1999, 148, 173–195. [Google Scholar] [PubMed]
- Anderson, G.D.; Lynn, A.M. Optimizing pediatric dosing: A developmental pharmacologic approach. Pharmacotherapy 2009, 29, 680–690. [Google Scholar] [CrossRef]
- Yenilmez, E.D.; Tamam, L.; Karaytug, O.; Tuli, A. Characterization of CYP1A2, CYP2C9, CYP2C19 and CYP2D6 polymor-phisms using HRMA in psychiatry patients with schizophrenia and bipolar disease for personalized medicine. Comb. Chem High Throughput Screen. 2018, 21, 374–380. [Google Scholar] [CrossRef]
- Xie, C.; Pogribna, M.; Word, B.; Lyn-Cook, L., Jr.; Lyn-Cook, B.D.; Hammons, G.J. In vitro analysis of factors influencing CYP1A2 expression as potential determinants of interindividual variation. Pharmacol. Res. Perspect. 2017, 5, e00299. [Google Scholar] [CrossRef] [Green Version]
- Gourash, L.M.; Hanchett, J.E.; Forster, J.L. Inpatient Crisis Intervention for Persons with PWS. In Management of Prader-Willi Syndrome, 3rd ed.; Butler, L., Whitman, Eds.; Springer: Cham, Switzerland, 2006; p. 418. [Google Scholar]
- Butler, M.G.; Miller, J.L.; Forster, J.L. Prader-Willi Syndrome—Clinical Genetics, Diagnosis and Treatment Approaches: An Update. Curr. Pediatr. Rev. 2019, 15, 207–244. [Google Scholar] [CrossRef]
- Saeves, R.; Strøm, F.; Sandvik, L.; Nordgarden, H. Gastro-oesophageal reflux—An important causative factor of severe tooth wear in Prader-Willi syndrome? Orphanet. J. Rare Dis. 2018, 13, 64. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Canet, M.J.; Clarke, J.D.; Billheimer, D.; Xanthakos, S.A.; Lavine, J.E.; Erickson, R.P.; Cherrington, N.J. Pediatric cyto-chrome P450 activity alterations in nonalcoholic steatohepatitis. Drug Metab. Dispos. 2017, 45, 1317–1325. [Google Scholar] [CrossRef] [Green Version]
- López, F.A.; Leroux, J.R. Long-acting stimulants for treatment of attention-deficit/hyperactivity disorder: A focus on ex-tended-release formulations and the prodrug lisdexamfetamine dimesylate to address continuing clinical challenges. Atten. Defic. Hyperact. Disord. 2013, 5, 249–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamba, J.K.; Lin, Y.S.; Schuetz, E.G.; Thummel, K.E. Genetic contribution to variable human CYP3A-mediated metabolism. Adv. Drug Del. Rev. 2002, 54, 1271–1294. [Google Scholar] [CrossRef]
- Anderson, G.D. Gender differences in pharmacological response. Int. Rev. Neurobiol. 2008, 83, 1–10. [Google Scholar] [CrossRef] [PubMed]





| CYP Gene/Metabolizer Phenotype | CYP Phenotype Frequency | Substrate Frequency | |||||
|---|---|---|---|---|---|---|---|
| PWS Referred Cohort | Typical Population | PWS Clinic Patients | |||||
| DEL | UPD | Unspec | All PWS | Frequency/Reference | NIH PWS Registry [12,13] | ||
| CYP2D6 | (n = 14) | (n = 16) | (n = 5) | (n = 35) | (n = 56,945) | (n = 265) | |
| EM | 28.5% † | 56.3% | 4 | 48.6% | 63.6% | http://www.pharmgkb.org/page/cyp2d6RefMaterials | Fluoxetine (21.9%), Risperidone (14%), Sertraline (14%), Aripiprazole (9.8%), Citalopram (8.7%), Escitalopram (5.7%), Paroxetine (4.5%), Bupropion (4.5%), Amphetamine (4.2%), Clonidine (3%), Ziprasidone (3%) |
| IM | 57.1% * | 25.0% | 0 | 34.0% | 23.6% | ||
| PM | 14.3% † | 18.8% * | 1 | 17.1% * | 2.2% | ||
| CYP2B6 | (n = 14) | (n = 15) | (n = 5) | (n = 34) | (n = 56,945) | ||
| EM | 50% | 40% | 5 | 53% | 43% | http://www.pharmgkb.org/page/cyp2B6RefMaterials | Sertraline (14%), Bupropion (4.5%) |
| IM | 50% | 60% | 0 | 47% | 39% | ||
| CYP2C19 | (n = 14) | (n = 16) | (n = 5) | (n = 35) | (n = 56,945) | ||
| EM | 78.6% | 100% † | 3 | 85.7% | 76.4% | http://www.pharmgkb.org/page/cyp2C19RefMaterials | Fluoxetine (21.9%), Sertraline (14%), Citalopram (8.7%), Escitalopram (5.7%) |
| IM | 7.1% | 0% † | 2 | 8.6% | 21.4% | ||
| UM | 14.3% † | 0% | 0 | 5.7% | 0.74% | ||
| CYP2C9 | (n = 14) | (n = 16) | (n = 5) | (n = 35) | (n = 56,945) | ||
| EM | 76.9% | 56.2% * | 2 | 61.8% * | 83.2% | http://www.pharmgkb.org/page/cyp2C9RefMaterials | Fluoxetine (21.9%), Sertraline (14%), Valproate (6.4%) |
| IM | 23.0% | 37.5% * | 3 | 35.3% * | 16.4% | ||
| PM | 0% | 6.3% † | 0 | 2.9% | 0% | ||
| CYP3A4 | (n = 14) | (n = 15) | (n = 5) | (n = 34) | (n = 5789) | ||
| EM | 85.7% † | 80.0% † | 5 | 85.3% * | 97.3% | Zhou et al., 2017 [20] | Risperidone (14%), Sertraline (14%), Modafinil (12.8%), Aripiprazole (9.8%), Citalopram (8.7%), Clonazepam (6.8%), Escitalopram (5.7%), Bupropion (4.5%), Ziprasidone (3%) |
| IM | 14.3% † | 20.0% † | 0 | 14.7% * | 2.7% | ||
| CYP1A2 | (n = 14) | (n = 16) | (n = 5) | (n = 35) | (n = 183) | ||
| UM | 42.9% * | 62.5% * | 2 | 51.4% * | 0% | Muscat et al., 2008 [27] | Fluvoxamine (1.1%), Haloperidol (1.1%), Thioridazine (1.1%), Olanzapine (0.4%), Chlorpromazine (0.4%), Imipramine (0.4%) |
| EM/HI | 57.1% | 31.2% | 3 | 45.7% | 37.0% | ||
| IM | 0% † | 6.25% † | 0 | 2.85% | 54.0% | ||
| PM | 0% | 0% | 0 | 0% † | 10.0% | ||
| Cytochrome | CYP1A2 | CYP2B6 | CYP2C19 | CYP2C9 | CYP2D6 | CYP3A4-5 |
|---|---|---|---|---|---|---|
| Substrate | Acetaminophen Amitriptyline, 3 Benztropine, 2 Caffeine Cannabidiol, 3 Chlorpromazine, 2 Clomipramine, 2 Clozapine, 1 Duloxetine, 1 Estradiol Fluvoxamine, 1 Haloperidol, 3 Imipramine, 2 Melatonin Mirtazapine, 3 Olanzapine, 1 Pimozide Propranolol, 1 Tacrine Thioridazine, 2 | Bupropion, 1 Selegiline Sertraline, 1 Sibutramine | Amitriptyline, 1 Benztropine, 3 Cannabis, 1 Cannabidiol, 2 Citalopram, 1 Clomipramine, 1 Clozapine, 2 Diazepam Doxepin, 2 Escitalopram, 1 Estradiol Fluoxetine,3 Imipramine, 1 Nortriptyline, 2 Omeprazole Phenytoin Progesterone, 1 Sertraline, 2 Testosterone, 1 Venlafaxine, 2 | Amitriptyline, 2 Benztropine, 4 Cannabidiol, 3 Cannabis, 3 Celecoxib Fluoxetine, 2 Ibuprofen, 1 Progesterone, 2 Sertraline, 3 Valproate Warfarin | Amitriptyline, 2 Amphetamine Aripiprazole, 2 Asenapine Atomoxetine Bupropion, 2 Cannabidiol, 3 Chlorpromazine, 1 Citalopram, 3 Clomipramine, 4 Clonidine Clozapine, 3 Desipramine, 4 Dextromethorphan Diphenhydramine Doxepin, 1 Escitalopram, 3 Fluoxetine, 1 Fluvoxamine, 2 Haloperidol, 1 Hydroxyzine Imipramine, 2 Mirtazapine, 2 Nortriptyline, 1 Olanzapine, 2 Paroxetine, 1 Perphenazine Propranolol, 2 Quetiapine, 2 Ranitidine Risperidone, 1 Sertraline, 2 Thioridazine, 1 Trazadone, 2 Venlafaxine, 1 Ziprasidone, 3 | Alprazolam Aripiprazole, 1 Benztropine, 1 Bupropion, 2 Buspirone Cannabis, 2 Cannabidiol, 1 Cisapride Citalopram, 2 Clomipramine, 3 Clonazepam Carbamazepine Desvenlafaxine Dextromethorphan Duloxetine, 3 Escitalopram, 2 Estradiol Erythromycin Fexofenadine Guanfacine Haloperidol, 2 Loratadine Lurasidone Mirtazapine, 1 Modafinil Pimozide Progesterone, 3 Quetiapine, 1 Risperidone, 2 Sertraline, 3 Testosterone Trazadone, 1 Tiagabine Ziprasidone, 1 Zolpidem |
| Inhibitor | Cannabidiol Cannabis Celecoxib Cimetidine Citalopram Ciprofloxacin Clarithromycin Erythromycin Estradiol Fluvoxamine Isoniazid Ketoconazole Modafinil | Cannabidiol Cannabis | Cannabidiol Cannabis Cimetidine Contraceptives Fluconazole Fluoxetine Fluvoxamine Indomethacin Isoniazid Ketoconazole Lansoprazole Modafinil Omeprazole Oxcarbazepine Probenecid Topiramate | Cannabidiol Cannabis Cimetidine Contraceptives Fluconazole Fluoxetine Fluvoxamine Isoniazid Ketoconazole Methylphenidate Modafinil Omeprazole Paroxetine Sertraline Sulfonamides Tacrine | Asenapine Bupropion Cannabis Cannabidiol Diphenhydramine Fluoxetine Goldenseal Haloperidol Hydroxyzine Methylphenidate Paroxetine Propranolol Quinidine Ranitidine | Cannabidiol Cimetidine Ciprofloxacin Clarithromycin Cyclosporine Erythromycin Goldenseal Grapefruit juice Isoniazid Ketoconazole Prednisone Sertraline Verapamil |
| Inducer | Carbamazepine Cruciferous vegetables Cannabis (smoke) Char-grilling Omeprazole Phenytoin St. John’s wort Tobacco (smoke) | Carbamazepine Modafinil Phenytoin Phenobarbital Rifampin | Rifampin | Carbamazepine Phenobarbital Rifampin St. John’s wort | Carbamazepine Cruciferous vegetables Ginseng Modafinil Phenytoin Rifampin St. John’s wort |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forster, J.; Duis, J.; Butler, M.G. Pharmacogenetic Testing of Cytochrome P450 Drug Metabolizing Enzymes in a Case Series of Patients with Prader-Willi Syndrome. Genes 2021, 12, 152. https://doi.org/10.3390/genes12020152
Forster J, Duis J, Butler MG. Pharmacogenetic Testing of Cytochrome P450 Drug Metabolizing Enzymes in a Case Series of Patients with Prader-Willi Syndrome. Genes. 2021; 12(2):152. https://doi.org/10.3390/genes12020152
Chicago/Turabian StyleForster, Janice, Jessica Duis, and Merlin G. Butler. 2021. "Pharmacogenetic Testing of Cytochrome P450 Drug Metabolizing Enzymes in a Case Series of Patients with Prader-Willi Syndrome" Genes 12, no. 2: 152. https://doi.org/10.3390/genes12020152
APA StyleForster, J., Duis, J., & Butler, M. G. (2021). Pharmacogenetic Testing of Cytochrome P450 Drug Metabolizing Enzymes in a Case Series of Patients with Prader-Willi Syndrome. Genes, 12(2), 152. https://doi.org/10.3390/genes12020152