
Hashimoto’s Thyroiditis and Graves’ Disease in Genetic Syndromes in Pediatric Age


 ,
,  , and
, and 
Abstract
:1. Introduction
1.1. Genetic Susceptibility in Autoimmune Thyroid Diseases
1.2. Autoimmune Thyroid Diseases in Pediatric General Population
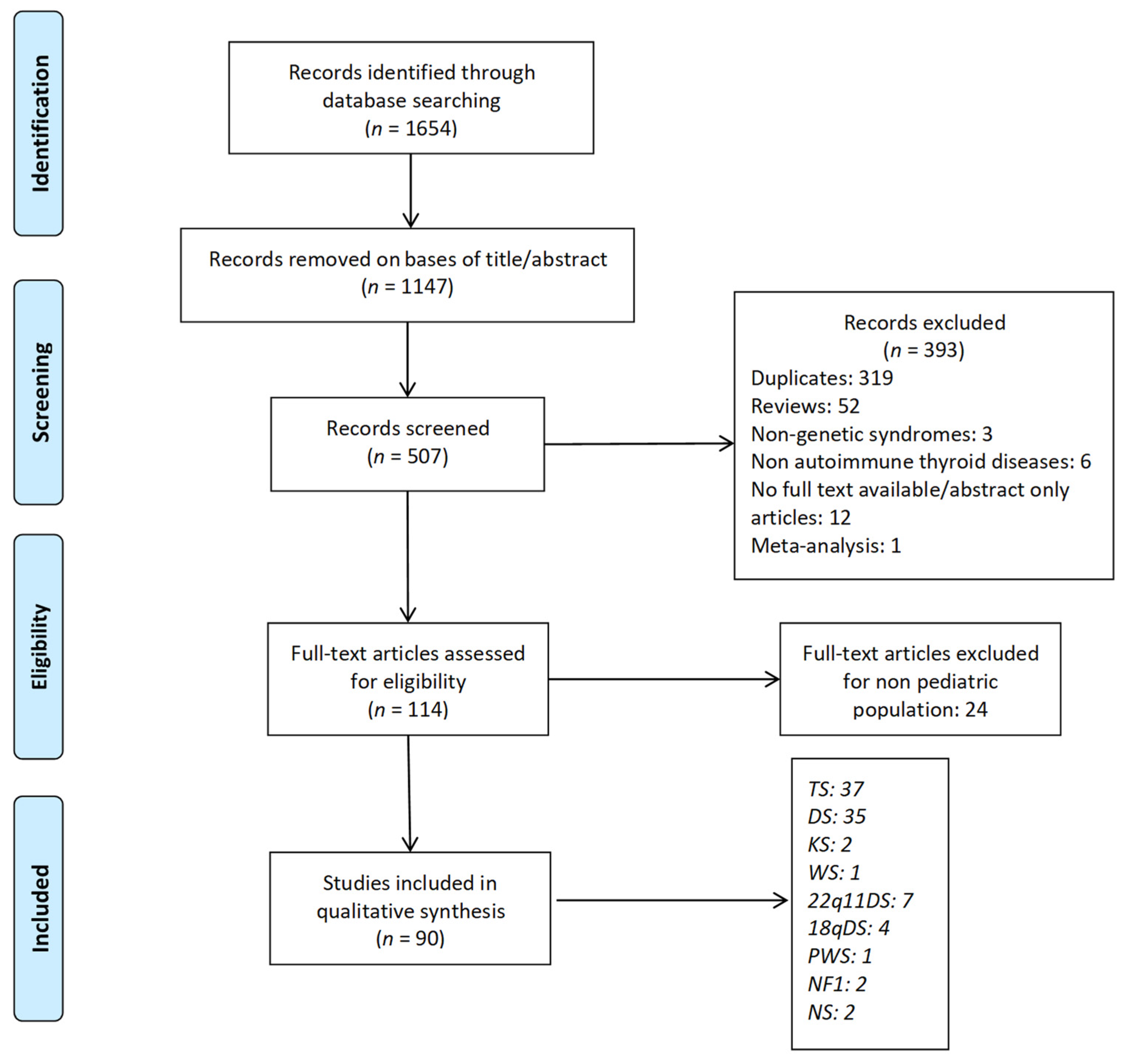
2. Materials and Methods
3. Results
4. Discussion
4.1. Autoimmune Thyroid Diseases and Chromosomopathies
4.1.1. Turner Syndrome
4.1.2. Down Syndrome
4.1.3. Klinefelter Syndrome
- -
- Endocrine organ-specific autoantibodies can be detected in 13% of KS subjects; the frequency progressively increases in those with higher-grade aneuploidies and is higher in children than in adults.
- -
- The influence of sex hormones as modulators of the immune response and X-linked gene dosage has been implicated in the pathogenesis of autoimmunity in KS.
- -
- In KS patients, measurement of TSH and free T4 (fT4) levels at diagnosis and annually thereafter is suggested.
- -
- Screening for thyroid autoantibodies should be considered in KS cases with TSH elevation and/or the presence of goiter or periodically in the absence of suggestive clinical or biochemical signs.
4.2. Autoimmune Thyroid Diseases and Deletion Syndromes
4.2.1. Williams Syndrome
4.2.2. 22q11.2 Deletion Syndrome
4.2.3. 18q Deletion Syndrome
4.3. Autoimmune Thyroid Diseases and Imprinting Disorders
Prader–Willi Syndrome
4.4. Autoimmune Thyroid Diseases and RASopathies
Neurofibromatosis Type 1 and Noonan Syndrome
4.5. Other Syndromes
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jacobson, D.L.; Gange, S.J.; Rose, N.R.; Graham, N.M. Epidemiology and Estimated Population Burden of Selected Autoimmune Diseases in the United States. Clin. Immunol. Immunopathol. 1997, 84, 223–243. [Google Scholar] [CrossRef] [Green Version]
- Cappa, M.; Bizzarri, C.; Crea, F. Autoimmune Thyroid Diseases in Children. J. Thyroid Res. 2010, 2011, 675703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saranac, L.; Zivanovic, S.; Bjelakovic, B.; Stamenkovic, H.; Novak, M.; Kamenov, B. Why Is the Thyroid so Prone to Autoimmune Disease? Horm. Res. Paediatr. 2011, 75, 157–165. [Google Scholar] [CrossRef]
- Tomer, Y.; Davies, T.F. Searching for the Autoimmune Thyroid Disease Susceptibility Genes: From Gene Mapping to Gene Function. Endocr. Rev. 2003, 24, 694–717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomer, Y.; Menconi, F. Type 1 Diabetes and Autoimmune Thyroiditis: The Genetic Connection. Thyroid Off. J. Am. Thyroid Assoc. 2009, 99–102. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Li, C.W.; Hammerstad, S.S.; Stefan, M.; Tomer, Y. Immunogenetics of Autoimmune Thyroid Diseases: A Comprehensive Review. J. Autoimmun. 2015, 64, 82–90. [Google Scholar] [CrossRef] [Green Version]
- Brand, O.J.; Barrett, J.C.; Simmonds, M.J.; Newby, P.R.; McCabe, C.J.; Bruce, C.K.; Kysela, B.; Carr-Smith, J.D.; Brix, T.; Hunt, P.J.; et al. Association of the Thyroid Stimulating Hormone Receptor Gene (TSHR) with Graves’ Disease. Hum. Mol. Genet. 2009, 18, 1704–1713. [Google Scholar] [CrossRef] [Green Version]
- Chu, X.; Pan, C.-M.; Zhao, S.-X.; Liang, J.; Gao, G.-Q.; Zhang, X.-M.; Yuan, G.-Y.; Li, C.-G.; Xue, L.-Q.; Shen, M.; et al. A Genome-Wide Association Study Identifies Two New Risk Loci for Graves’ Disease. Nat. Genet. 2011, 43, 897–901. [Google Scholar] [CrossRef]
- Graves, P.N.; Tomer, Y.; Davies, T.F. Cloning and Sequencing of a 1.3 KB Variant of Human Thyrotropin Receptor MRNA Lacking the Transmembrane Domain. Biochem. Biophys. Res. Commun. 1992, 187, 1135–1143. [Google Scholar] [CrossRef]
- Tomer, Y. Mechanisms of Autoimmune Thyroid Diseases: From Genetics to Epigenetics. Annu. Rev. Pathol. 2014, 9, 147–156. [Google Scholar] [CrossRef] [Green Version]
- Jacobson, E.M.; Huber, A.; Tomer, Y. The HLA Gene Complex in Thyroid Autoimmunity: From Epidemiology to Etiology. J. Autoimmun. 2008, 30, 58–62. [Google Scholar] [CrossRef] [Green Version]
- Jacobson, E.M.; Tomer, Y. The Genetic Basis of Thyroid Autoimmunity. Thyroid 2007, 17, 949–961. [Google Scholar] [CrossRef]
- Bennett, C.L.; Christie, J.; Ramsdell, F.; Brunkow, M.E.; Ferguson, P.J.; Whitesell, L.; Kelly, T.E.; Saulsbury, F.T.; Chance, P.F.; Ochs, H.D. The Immune Dysregulation, Polyendocrinopathy, Enteropathy, X-Linked Syndrome (IPEX) Is Caused by Mutations of FOXP3. Nat. Genet. 2001, 27, 20–21. [Google Scholar] [CrossRef] [PubMed]
- Ban, Y.; Tozaki, T.; Tobe, T.; Ban, Y.; Jacobson, E.M.; Concepcion, E.S.; Tomer, Y. The Regulatory T Cell Gene FOXP3 and Genetic Susceptibility to Thyroid Autoimmunity: An Association Analysis in Caucasian and Japanese Cohorts. J. Autoimmun. 2007, 28, 201–207. [Google Scholar] [CrossRef] [PubMed]
- Inoue, N.; Watanabe, M.; Morita, M.; Tomizawa, R.; Akamizu, T.; Tatsumi, K.; Hidaka, Y.; Iwatani, Y. Association of Functional Polymorphisms Related to the Transcriptional Level of FOXP3 with Prognosis of Autoimmune Thyroid Diseases. Clin. Exp. Immunol. 2010, 162, 402–406. [Google Scholar] [CrossRef] [PubMed]
- Brand, O.J.; Lowe, C.E.; Heward, J.M.; Franklyn, J.A.; Cooper, J.D.; Todd, J.A.; Gough, S.C.L. Association of the Interleukin-2 Receptor Alpha (IL-2Ralpha)/CD25 Gene Region with Graves’ Disease Using a Multilocus Test and Tag SNPs. Clin. Endocrinol. (Oxf.) 2007, 66, 508–512. [Google Scholar] [CrossRef] [PubMed]
- Tomer, Y.; Concepcion, E.; Greenberg, D.A. A C/T Single-Nucleotide Polymorphism in the Region of the CD40 Gene Is Associated with Graves’ Disease. Thyroid 2002, 12, 1129–1135. [Google Scholar] [CrossRef]
- Tomer, Y.; Huber, A. The Etiology of Autoimmune Thyroid Disease: A Story of Genes and Environment. J. Autoimmun. 2009, 32, 231–239. [Google Scholar] [CrossRef] [Green Version]
- Nithiyananthan, R.; Heward, J.M.; Allahabadia, A.; Franklyn, J.A.; Gough, S.C.L. Polymorphism of the CTLA-4 Gene Is Associated with Autoimmune Hypothyroidism in the United Kingdom. Thyroid 2002, 12, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Teft, W.A.; Kirchhof, M.G.; Madrenas, J. A Molecular Perspective of CTLA-4 Function. Annu. Rev. Immunol. 2006, 24, 65–97. [Google Scholar] [CrossRef] [Green Version]
- Velaga, M.R.; Wilson, V.; Jennings, C.E.; Owen, C.J.; Herington, S.; Donaldson, P.T.; Ball, S.G.; James, R.A.; Quinton, R.; Perros, P.; et al. The Codon 620 Tryptophan Allele of the Lymphoid Tyrosine Phosphatase (LYP) Gene Is a Major Determinant of Graves’ Disease. J. Clin. Endocrinol. Metab. 2004, 89, 5862–5865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ban, Y.; Davies, T.F.; Greenberg, D.A.; Concepcion, E.S.; Osman, R.; Oashi, T.; Tomer, Y. Arginine at Position 74 of the HLA-DR Beta1 Chain Is Associated with Graves’ Disease. Genes Immun. 2004, 5, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Ban, Y.; Davies, T.F.; Greenberg, D.A.; Concepcion, E.S.; Tomer, Y. The Influence of Human Leucocyte Antigen (HLA) Genes on Autoimmune Thyroid Disease (AITD): Results of Studies in HLA-DR3 Positive AITD Families. Clin. Endocrinol. (Oxf.) 2002, 57, 81–88. [Google Scholar] [CrossRef]
- Hunter, I.; Greene, S.A.; MacDonald, T.M.; Morris, A.D. Prevalence and Aetiology of Hypothyroidism in the Young. Arch. Dis. Child. 2000, 83, 207–210. [Google Scholar] [CrossRef] [Green Version]
- Segni, M.; Leonardi, E.; Mazzoncini, B.; Pucarelli, I.; Pasquino, A.M. Special Features of Graves’ Disease in Early Childhood. Thyroid 1999, 9, 871–877. [Google Scholar] [CrossRef]
- Aversa, T.; Lombardo, F.; Valenzise, M.; Messina, M.F.; Sferlazzas, C.; Salzano, G.; De Luca, F.; Wasniewska, M. Peculiarities of Autoimmune Thyroid Diseases in Children with Turner or Down Syndrome: An Overview. Ital. J. Pediatr. 2015, 41, 39. [Google Scholar] [CrossRef] [Green Version]
- Wasniewska, M.; Vigone, M.C.; Cappa, M.; Aversa, T.; Rubino, M.; De Luca, F. Acute Suppurative Thyroiditis in Childhood: Relative Frequency among Thyroid Inflammatory Diseases*. J. Endocrinol. Investig. 2007, 346–347. [Google Scholar] [CrossRef]
- Wasniewska, M.; Corrias, A.; Salerno, M.; Mussa, A.; Capalbo, D.; Messina, M.F.; Aversa, T.; Bombaci, S.; De Luca, F.; Valenzise, M. Thyroid Function Patterns at Hashimoto’s Thyroiditis Presentation in Childhood and Adolescence Are Mainly Conditioned by Patients’ Age. Horm. Res. Paediatr. 2012, 78, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Wasniewska, M.; Corrias, A.; Arrigo, T.; Lombardo, F.; Salerno, M.; Mussa, A.; Vigone, M.C.; De Luca, F. Frequency of Hashimoto’s Thyroiditis Antecedents in the History of Children and Adolescents with Graves’ Disease. Horm. Res. Paediatr. 2010, 73, 473–476. [Google Scholar] [CrossRef]
- Aversa, T.; Corrias, A.; Salerno, M.; Tessaris, D.; Di Mase, R.; Valenzise, M.; Corica, D.; De Luca, F.; Wasniewska, M. Five-Year Prospective Evaluation of Thyroid Function Test Evolution in Children with Hashimoto’s Thyroiditis Presenting with Either Euthyroidism or Subclinical Hypothyroidism. Thyroid 2016, 26, 1450–1456. [Google Scholar] [CrossRef]
- Wasniewska, M.; Corrias, A.; Salerno, M.; Lombardo, F.; Aversa, T.; Mussa, A.; Capalbo, D.; De Luca, F.; Valenzise, M. Outcomes of Children with Hashitoxicosis. Horm. Res. Paediatr. 2012, 77, 36–40. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Stoklasova, J.; Zapletalova, J.; Frysak, Z.; Hana, V.; Cap, J.; Pavlikova, M.; Soucek, O.; Lebl, J. An Isolated Xp Deletion Is Linked to Autoimmune Diseases in Turner Syndrome. J. Pediatr. Endocrinol. Metab. 2019, 32, 479–488. [Google Scholar] [CrossRef] [PubMed]
- Villanueva-Ortega, E.; Ahedo, B.; Fonseca-Sánchez, M.A.; Pérez-Durán, J.; Garibay-Nieto, N.; Macías-Galavíz, M.T.; Trujillo-Cabrera, Y.; García-Latorre, E.; Queipo, G. Analysis of PTPN22, ZFAT and MYO9B Polymorphisms in Turner Syndrome and Risk of Autoimmune Disease. Int. J. Immunogenet. 2017, 44, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Grossi, A.; Palma, A.; Zanni, G.; Novelli, A.; Loddo, S.; Cappa, M.; Fierabracci, A. Multiorgan Autoimmunity in a Turner Syndrome Patient with Partial Monosomy 2q and Trisomy 10p. Gene 2013, 515, 439–443. [Google Scholar] [CrossRef]
- Kucharska, A.M.; Czarnocka, B.; Demkow, U. Anti-Natrium/Iodide Symporter Antibodies and Other Anti-Thyroid Antibodies in Children with Turner’s Syndrome. Adv. Exp. Med. Biol. 2013, 756, 131–138. [Google Scholar] [CrossRef] [PubMed]
- Gawlik, A.; Gawlik, T.; Januszek-Trzciakowska, A.; Patel, H.; Malecka-Tendera, E. Incidence and Dynamics of Thyroid Dysfunction and Thyroid Autoimmunity in Girls with Turner’s Syndrome: A Long-Term Follow-up Study. Horm. Res. Paediatr. 2011, 76, 314–320. [Google Scholar] [CrossRef]
- Calcaterra, V.; Klersy, C.; Muratori, T.; Caramagna, C.; Brizzi, V.; Albertini, R.; Larizza, D. Thyroid Ultrasound in Patients with Turner Syndrome: Influence of Clinical and Auxological Parameters. J. Endocrinol. Invest. 2011, 34, 260–264. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, I.; Hizuka, N.; Kurimoto, M.; Morita, J.; Tanaka, S.; Yamakado, Y.; Takano, K. Autoimmune Thyroid Diseases in 65 Japanese Women with Turner Syndrome. Endocr. J. 2009, 56, 983–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medeiros, C.C.M.; de Lemos-Marini, S.H.V.; Filho, M.B.; Camargo, E.E.; Santos, A.O.; Magna, L.A.; Guerra-Júnior, G.; Baptista, M.T.M.; Maciel-Guerra, A.T. Turner’s Syndrome and Subclinical Autoimmune Thyroid Disease: A Two-Year Follow-up Study. J. Pediatr. Endocrinol. Metab. 2009, 22, 109–118. [Google Scholar] [CrossRef]
- Mortensen, K.H.; Cleemann, L.; Hjerrild, B.E.; Nexo, E.; Locht, H.; Jeppesen, E.M.; Gravholt, C.H. Increased Prevalence of Autoimmunity in Turner Syndrome—Influence of Age. Clin. Exp. Immunol. 2009, 156, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Bettendorf, M.; Doerr, H.G.; Hauffa, B.P.; Lindberg, A.; Mehls, O.; Partsch, C.-J.; Schwarz, H.-P.; Stahnke, N.; Ranke, M.B. Prevalence of Autoantibodies Associated with Thyroid and Celiac Disease in Ullrich-Turner Syndrome in Relation to Adult Height after Growth Hormone Treatment. J. Pediatr. Endocrinol. Metab. 2006, 19, 149–154. [Google Scholar] [CrossRef]
- Livadas, S.; Xekouki, P.; Fouka, F.; Kanaka-Gantenbein, C.; Kaloumenou, I.; Mavrou, A.; Constantinidou, N.; Dacou-Voutetakis, C. Prevalence of Thyroid Dysfunction in Turner’s Syndrome: A Long-Term Follow-up Study and Brief Literature Review. Thyroid 2005, 15, 1061–1066. [Google Scholar] [CrossRef]
- El-Mansoury, M.; Bryman, I.; Berntorp, K.; Hanson, C.; Wilhelmsen, L.; Landin-Wilhelmsen, K. Hypothyroidism Is Common in Turner Syndrome: Results of a Five-Year Follow-Up. J. Clin. Endocrinol. Metab. 2005, 90, 2131–2135. [Google Scholar] [CrossRef] [Green Version]
- Witkowska-Sędek, E.; Borowiec, A.; Kucharska, A.; Chacewicz, K.; Rumińska, M.; Demkow, U.; Pyrżak, B. Thyroid Autoimmunity in Girls with Turner Syndrome. Adv. Exp. Med. Biol. 2017, 1022, 71–76. [Google Scholar] [CrossRef]
- Elsheikh, M.; Wass, J.A.; Conway, G.S. Autoimmune Thyroid Syndrome in Women with Turner’s Syndrome—The Association with Karyotype. Clin. Endocrinol. (Oxf.) 2001, 55, 223–226. [Google Scholar] [CrossRef] [PubMed]
- Chang, P.; Tsai, W.Y.; Hou, J.W.; Hsiao, P.H.; Lee, J.S. Autoimmune Thyroiditis in Children with Turner Syndrome. J. Formos. Med. Assoc. 2000, 99, 823–826. [Google Scholar] [PubMed]
- Medeiros, C.C.; Marini, S.H.; Baptista, M.T.; Guerra, G.J.; Maciel-Guerra, A.T. Turner’s Syndrome and Thyroid Disease: A Transverse Study of Pediatric Patients in Brazil. J. Pediatr. Endocrinol. Metab. 2000, 13, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, M.; Inamo, Y.; Harada, K. A Case Report of Turner Syndrome with Graves’ Disease during Recombinant Human GH Therapy and Review of Literature. Clin. Pediatr. Endocrinol. Case Rep. Clin. Investig. Off. J. Jpn. Soc. Pediatr. Endocrinol. 2006, 15, 55–59. [Google Scholar] [CrossRef] [Green Version]
- Jin, W.; Cheng, F.-X.; Xiao, M.-S.; Fan, Y.; Dong, W. Concurrent Occurrence of Chronic Lymphocytic Thyroiditis with Hypothyroidism and Growth Hormone Deficiency in a Turner’s Syndrome Patient. J. Pediatr. Endocrinol. Metab. 2011, 24, 237–239. [Google Scholar] [CrossRef]
- Zeng, W.-H.; Xu, J.-J.; Jia, M.-Y.; Ren, Y.-Z. Pseudohypoparathyroidism with Hashimoto’s Thyroiditis and Turner Syndrome: A Case Report. Gynecol. Endocrinol. Off. J. Int. Soc. Gynecol. Endocrinol. 2014, 30, 694–696. [Google Scholar] [CrossRef]
- Haltrich, I.; Pikó, H.; Pamjav, H.; Somogyi, A.; Völgyi, A.; David, D.; Beke, A.; Garamvölgyi, Z.; Kiss, E.; Karcagi, V.; et al. Complex X Chromosome Rearrangement Associated with Multiorgan Autoimmunity. Mol. Cytogenet. 2015, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wasniewska, M.; Aversa, T.; Salerno, M.; Corrias, A.; Messina, M.F.; Mussa, A.; Capalbo, D.; De Luca, F.; Valenzise, M. Five-Year Prospective Evaluation of Thyroid Function in Girls with Subclinical Mild Hypothyroidism of Different Etiology. Eur. J. Endocrinol. 2015, 173, 801–808. [Google Scholar] [CrossRef] [Green Version]
- Wasniewska, M.; Salerno, M.; Corrias, A.; Mazzanti, L.; Matarazzo, P.; Corica, D.; Aversa, T.; Messina, M.F.; De Luca, F.; Valenzise, M. The Evolution of Thyroid Function after Presenting with Hashimoto Thyroiditis Is Different between Initially Euthyroid Girls with and Those without Turner Syndrome. Horm. Res. Paediatr. 2016, 86, 403–409. [Google Scholar] [CrossRef]
- Hanew, K.; Tanaka, T.; Horikawa, R.; Hasegawa, T.; Yokoya, S. Prevalence of Diverse Complications and Its Association with Karyotypes in Japanese Adult Women with Turner Syndrome-a Questionnaire Survey by the Foundation for Growth Science. Endocr. J. 2018, 65, 509–519. [Google Scholar] [CrossRef] [Green Version]
- Cyniak-Magierska, A.; Lasoń, A.; Smyczyńska, J.; Lewiński, A. Autoimmune Polyglandular Syndrome Type 2 Manifested as Hashimoto’s Thyroiditis and Adrenocortical Insufficiency, in Turner Syndrome Woman, with Onset Following Introduction of Treatment with Recombinant Human Growth Hormone. Neuro Endocrinol. Lett. 2015, 36, 119–123. [Google Scholar]
- Wegiel, M.; Antosz, A.; Gieburowska, J.; Szeliga, K.; Hankus, M.; Grzybowska-Chlebowczyk, U.; Wiecek, S.; Malecka-Tendera, E.; Gawlik, A. Autoimmunity Predisposition in Girls with Turner Syndrome. Front. Endocrinol. (Lausanne) 2019, 10, 511. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Zhang, X.; Yang, M. Clinical Case Report: A Case of Turner Syndrome with Graves’ Disease. Medicine (Baltimore) 2020, 99, e19518. [Google Scholar] [CrossRef] [PubMed]
- Gawlik, A.M.; Berdej-Szczot, E.; Blat, D.; Klekotka, R.; Gawlik, T.; Blaszczyk, E.; Hankus, M.; Malecka-Tendera, E. Immunological Profile and Predisposition to Autoimmunity in Girls with Turner Syndrome. Front. Endocrinol. (Lausanne) 2018, 9, 307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, O.T.; Smolinski, K.N.; Yan, A.C.; Grimberg, A. PTU-Associated Vasculitis in a Girl with Turner Syndrome and Graves’ Disease. Pediatr. Emerg. Care 2006, 22, 52–54. [Google Scholar] [CrossRef]
- Wasniewska, M.; Corrias, A.; Messina, M.F.; Crisafulli, G.; Salzano, G.; Valenzise, M.; Mussa, A.; De Luca, F. Graves’ Disease Prevalence in a Young Population with Turner Syndrome. J. Endocrinol. Investig. 2010, 33, 69–70. [Google Scholar] [CrossRef] [PubMed]
- Oueslati, I.; Khiari, K.; Ali, I.H.; Abdallah, N. Ben. Coexisting Turner’s Syndrome, Hashimoto’s Thyroiditis, and Growth Hormone Deficiency. Indian J. Endocrinol. Metab. 2016, 20, 573–574. [Google Scholar] [CrossRef]
- Yeşilkaya, E.; Bereket, A.; Darendeliler, F.; Baş, F.; Poyrazoğlu, Ş.; Küçükemre Aydın, B.; Darcan, Ş.; Dündar, B.; Büyükinan, M.; Kara, C.; et al. Turner Syndrome and Associated Problems in Turkish Children: A Multicenter Study. J. Clin. Res. Pediatr. Endocrinol. 2015, 7, 27–36. [Google Scholar] [CrossRef]
- Marques, I.; Silva, A.; Castro, S.; Lopes, L. Down Syndrome, Insulin-Dependent Diabetes Mellitus and Hyperthyroidism: A Rare Association. BMJ Case Rep. 2015, 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pepe, G.; Corica, D.; De Sanctis, L.; Salerno, M.; Faienza, M.F.; Tessaris, D.; Tuli, G.; Scala, I.; Penta, L.; Alibrandi, A.; et al. Prospective Evaluation of Autoimmune and Non-Autoimmune Subclinical Hypothyroidism in Down Syndrome Children. Eur. J. Endocrinol. 2020, 182, 385–392. [Google Scholar] [CrossRef] [PubMed]
- AlAaraj, N.; Soliman, A.T.; Itani, M.; Khalil, A.; De Sanctis, V. Prevalence of Thyroid Dysfunctions in Infants and Children with Down Syndrome (DS) and the Effect of Thyroxine Treatment on Linear Growth and Weight Gain in Treated Subjects versus DS Subjects with Normal Thyroid Function: A Controlled Study. Acta Biomed. 2019, 90, 36–42. [Google Scholar] [CrossRef]
- Aversa, T.; Messina, M.F.; Mazzanti, L.; Salerno, M.; Mussa, A.; Faienza, M.F.; Scarano, E.; De Luca, F.; Wasniewska, M. The Association with Turner Syndrome Significantly Affects the Course of Hashimoto’s Thyroiditis in Children, Irrespective of Karyotype. Endocrine 2015, 50, 777–782. [Google Scholar] [CrossRef]
- Abdulrazzaq, Y.; El-Azzabi, T.I.; Al Hamad, S.M.; Attia, S.; Deeb, A.; Aburawi, E.H. Occurrence of Hypothyroidism, Diabetes Mellitus, and Celiac Disease in Emirati Children with Down’s Syndrome. Oman Med. J. 2018, 33, 387–392. [Google Scholar] [CrossRef]
- Pierce, M.J.; LaFranchi, S.H.; Pinter, J.D. Characterization of Thyroid Abnormalities in a Large Cohort of Children with Down Syndrome. Horm. Res. Paediatr. 2017. [Google Scholar] [CrossRef] [Green Version]
- Aversa, T.; Valenzise, M.; Corrias, A.; Salerno, M.; Iughetti, L.; Tessaris, D.; Capalbo, D.; Predieri, B.; De Luca, F.; Wasniewska, M. In Children with Autoimmune Thyroid Diseases the Association with Down Syndrome Can Modify the Clustering of Extra-Thyroidal Autoimmune Disorders. J. Pediatr. Endocrinol. Metab. 2016, 29, 1041–1046. [Google Scholar] [CrossRef]
- Aversa, T.; Valenzise, M.; Salerno, M.; Corrias, A.; Iughetti, L.; Radetti, G.; De Luca, F.; Wasniewska, M. Metamorphic Thyroid Autoimmunity in Down Syndrome: From Hashimoto’s Thyroiditis to Graves’ Disease and Beyond. Ital. J. Pediatr. 2015, 41, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aversa, T.; Salerno, M.; Radetti, G.; Faienza, M.F.; Iughetti, L.; Corrias, A.; Predieri, B.; Mussa, A.; Mirabelli, S.; De Luca, F.; et al. Peculiarities of Presentation and Evolution over Time of Hashimoto’s Thyroiditis in Children and Adolescents with Down’s Syndrome. Hormones (Athens) 2015, 14, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Barcons, M.; Casteràs, A.; del Pilar Armengol, M.; Porta, E.; Correa, P.A.; Marín, A.; Pujol-Borrell, R.; Colobran, R. Autoimmune Predisposition in Down Syndrome May Result from a Partial Central Tolerance Failure Due to Insufficient Intrathymic Expression of AIRE and Peripheral Antigens. J. Immunol. 2014, 193, 3872–3879. [Google Scholar] [CrossRef] [Green Version]
- Pellegrini, F.P.; Marinoni, M.; Frangione, V.; Tedeschi, A.; Gandini, V.; Ciglia, F.; Mortara, L.; Accolla, R.S.; Nespoli, L. Down Syndrome, Autoimmunity and T Regulatory Cells. Clin. Exp. Immunol. 2012, 169, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Bhat, M.H.; Saba, S.; Ahmed, I.; Kamili, M.M.A.; Khan, S.A. Graves’ Disease in a Down’s Syndrome Patient. J. Pediatr. Endocrinol. Metab. 2010, 23, 1181–1183. [Google Scholar] [CrossRef] [PubMed]
- Pirgon, O.; Atabek, M.E.; Sert, A. Diabetic Ketoacidosis, Thyroiditis and Alopecia Areata in a Child with Down Syndrome. Indian J. Pediatr. 2009, 76, 1263–1264. [Google Scholar] [CrossRef]
- De Luca, F.; Corrias, A.; Salerno, M.; Wasniewska, M.; Gastaldi, R.; Cassio, A.; Mussa, A.; Aversa, T.; Radetti, G.; Arrigo, T. Peculiarities of Graves’ Disease in Children and Adolescents with Down’s Syndrome. Eur. J. Endocrinol. 2010, 162, 591–595. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.-M.; Zhang, Y.; Yang, X.-H.; Lin, X.-Q.; Yuan, X. Thyroid Disease in Chinese Girls with Turner Syndrome. J. Pediatr. Endocrinol. Metab. 2015, 28, 201–205. [Google Scholar] [CrossRef]
- Salzano, G.; Lombardo, F.; Arrigo, T.; Sferlazzas, C.; Wasniewska, M.; Valenzise, M.; De Luca, F. Association of Five Autoimmune Diseases in a Young Woman with Down’s Syndrome. J. Endocrinol. Investig. 2010, 202–203. [Google Scholar] [CrossRef]
- Nebesio, T.D.; Eugster, E.A. Unusual Thyroid Constellation in Down Syndrome: Congenital Hypothyroidism, Graves’ Disease, and Hemiagenesis in the Same Child. J. Pediatr. Endocrinol. Metab. 2009, 22, 263–268. [Google Scholar] [CrossRef]
- Lämmer, C.; Weimann, E. Early Onset of Type I Diabetes Mellitus, Hashimoto’s Thyroiditis and Celiac Disease in a 7-Yr-Old Boy with Down’s Syndrome. Pediatr. Diabetes 2008, 9, 423–425. [Google Scholar] [CrossRef]
- Unachak, K.; Tanpaiboon, P.; Pongprot, Y.; Sittivangkul, R.; Silvilairat, S.; Dejkhamron, P.; Sudasna, J. Thyroid Functions in Children with Down’s Syndrome. J. Med. Assoc. Thai. 2008, 91, 56–61. [Google Scholar]
- Söderbergh, A.; Gustafsson, J.; Ekwall, O.; Hallgren, A.; Nilsson, T.; Kämpe, O.; Rorsman, F.; Annerén, G. Autoantibodies Linked to Autoimmune Polyendocrine Syndrome Type I Are Prevalent in Down Syndrome. Acta Paediatr. 2006, 95, 1657–1660. [Google Scholar] [CrossRef] [PubMed]
- Goldacre, M.J.; Wotton, C.J.; Seagroatt, V.; Yeates, D. Cancers and Immune Related Diseases Associated with Down’s Syndrome: A Record Linkage Study. Arch. Dis. Child. 2004, 89, 1014–1017. [Google Scholar] [CrossRef] [Green Version]
- Gruñeiro de Papendieck, L.; Chiesa, A.; Bastida, M.G.; Alonso, G.; Finkielstain, G.; Heinrich, J.J. Thyroid Dysfunction and High Thyroid Stimulating Hormone Levels in Children with Down’s Syndrome. J. Pediatr. Endocrinol. Metab. 2002, 15, 1543–1548. [Google Scholar] [CrossRef]
- Shalitin, S.; Phillip, M. Autoimmune Thyroiditis in Infants with Down’s Syndrome. J. Pediatr. Endocrinol. Metab. 2002, 15, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.H.; Lee, C.P.; Chao, M.C. Coexistent Insulin Dependent Diabetes Mellitus and Hyperthyroidism in a Patient with Down’s Syndrome. Kaohsiung J. Med. Sci. 2000, 16, 210–213. [Google Scholar] [PubMed]
- Zwaveling-Soonawala, N.; Witteveen, M.E.; Marchal, J.P.; Klouwer, F.C.C.; Ikelaar, N.A.; Smets, A.M.J.B.; van Rijn, R.R.; Endert, E.; Fliers, E.; van Trotsenburg, A.S.P. Early Thyroxine Treatment in Down Syndrome and Thyroid Function Later in Life. Eur. J. Endocrinol. 2017, 176, 505–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenzise, M.; Aversa, T.; Corrias, A.; Mazzanti, L.; Cappa, M.; Ubertini, G.; Scarano, E.; Mussa, A.; Messina, M.F.; De Luca, F.; et al. Epidemiology, Presentation and Long-Term Evolution of Graves’ Disease in Children, Adolescents and Young Adults with Turner Syndrome. Horm. Res. Paediatr. 2014, 81, 245–250. [Google Scholar] [CrossRef]
- Spahiu, L.; Jashari, H.; Mulliqi-Kotori, V.; Elezi-Rugova, B.; Merovci, B. Hashimoto Thyroiditis and Nephrocalcinosis in a Child with Down Syndrome. Acta Inform. Med. AIM J. Soc. Med Inform. Bosnia Herzeg. Cas. Drus. Za Med. Inform. BiH. 2016, 143–145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faria, C.D.C.; Ribeiro, S.; Kochi, C.; da Silva, A.P.N.; Ribeiro, B.N.F.; Marçal, L.T.; Santos, F.H.Y.; Eduardo, C.P.L.; Monte, O.; Longui, C.A. TSH Neurosecretory Dysfunction (TSH-Nd) in Down Syndrome (DS): Low Risk of Progression to Hashimoto’s Thyroiditis. Arq. Bras. Endocrinol. Metabol. 2011, 55, 628–631. [Google Scholar] [CrossRef] [Green Version]
- Helene, V.; Patrick, V.; Boel, D.P.; Gini, B.; Bruno, B.; Rudy, V.C. Hashimoto Encephalopathy and Antibodies against Dimethylargininase-1: A Rare Cause of Cognitive Decline in a Pediatric Down’s Syndrome Patient. Clin. Neurol. Neurosurg. 2011, 113, 678–679. [Google Scholar] [CrossRef] [PubMed]
- Popova, G.; Paterson, W.F.; Brown, A.; Donaldson, M.D.C. Hashimoto’s Thyroiditis in Down’s Syndrome: Clinical Presentation and Evolution. Horm. Res. 2008, 70, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Kinik, S.T.; Ozçay, F.; Varan, B. Type I Diabetes Mellitus, Hashimoto’s Thyroiditis and Celiac Disease in an Adolescent with Down Syndrome. Pediatr. Int. 2006, 48, 433–435. [Google Scholar] [CrossRef]
- Ersoy, B.; Seniha, K.Y.; Kızılay, D.; Yılmaz, M.; Coşkun, Ş. Diagnostic Difficulties by the Unusual Presentations in Children and Adolescents with Hashimoto Thyroiditis. Ann. Pediatr. Endocrinol. Metab. 2016, 21, 164–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahluwalia, A.I.; Narayan, S. Graves Disease in an Eight Year Old Boy of Down Syndrome. Indian Pediatrics 2005, 42, 76–77. [Google Scholar]
- Goday-Arno, A.; Cerda-Esteva, M.; Flores-Le-Roux, J.A.; Chillaron-Jordan, J.J.; Corretger, J.M.; Cano-Pérez, J.F. Hyperthyroidism in a Population with Down Syndrome (DS). Clin. Endocrinol. (Oxf.) 2009, 71, 110–114. [Google Scholar] [CrossRef]
- Creo, A.L.; Candela, N.; Lee, M.M.; Feldman, P.M. An Unusual Manifestation of Celiac Disease in an Adolescent With Down Syndrome and Graves Disease. J. Pediatr. Gastroenterol. Nutr. 2017, 65, e20–e22. [Google Scholar] [CrossRef]
- Dos Santos, T.J.; Martos-Moreno, G.Á.; Muñoz-Calvo, M.T.; Pozo, J.; Rodríguez-Artalejo, F.; Argente, J. Clinical Management of Childhood Hyperthyroidism with and without Down Syndrome: A Longitudinal Study at a Single Center. J. Pediatr. Endocrinol. Metab. 2018, 31, 743–750. [Google Scholar] [CrossRef]
- Grossi, A.; Crinò, A.; Luciano, R.; Lombardo, A.; Cappa, M.; Fierabracci, A. Endocrine Autoimmunity in Turner Syndrome. Ital. J. Pediatr. 2013, 39, 79. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, H.; Sato, K.; Yoshimura, S.; Hayashi, Y.; Izumo, T.; Tokunaga, Y. Moyamoya Disease Associated with Graves’ Disease and Down Syndrome: A Case Report and Literature Review. J. stroke Cerebrovasc. Dis. Off. J. Natl. Stroke Assoc. 2021, 30, 105414. [Google Scholar] [CrossRef] [PubMed]
- Balercia, G.; Bonomi, M.; Giagulli, V.A.; Lanfranco, F.; Rochira, V.; Giambersio, A.; Accardo, G.; Esposito, D.; Allasia, S.; Cangiano, B.; et al. Thyroid Function in Klinefelter Syndrome: A Multicentre Study from KING Group. J. Endocrinol. Invest. 2019, 42, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Panimolle, F.; Tiberti, C.; Granato, S.; Anzuini, A.; Pozza, C.; Lenzi, A.; Radicioni, A.F. Evidence of Increased Humoral Endocrine Organ-Specific Autoimmunity in Severe and Classic X-Chromosome Aneuploidies in Comparison with 46,XY Control Subjects. Autoimmunity 2018, 51, 175–182. [Google Scholar] [CrossRef]
- Stagi, S.; Lapi, E.; D’Avanzo, M.G.; Perferi, G.; Romano, S.; Giglio, S.; Ricci, S.; Azzari, C.; Chiarelli, F.; Seminara, S.; et al. Coeliac Disease and Risk for Other Autoimmune Diseases in Patients with Williams-Beuren Syndrome. BMC Med. Genet. 2014, 15, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, J.-H.; Shin, Y.-L.; Kim, G.-H.; Seo, E.-J.; Kim, Y.; Park, I.-S.; Yoo, H.-W. Endocrine Manifestations of Chromosome 22q11.2 Microdeletion Syndrome. Horm. Res. 2005, 63, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Ueda, Y.; Uraki, S.; Inaba, H.; Nakashima, S.; Ariyasu, H.; Iwakura, H.; Ota, T.; Furuta, H.; Nishi, M.; Akamizu, T. Graves’ Disease in Pediatric and Elderly Patients with 22q11.2 Deletion Syndrome. Intern. Med. 2017, 56, 1169–1173. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.J.; Datta, V.; Browning, M.J.; Swift, P.G.F. Graves’ Disease in DiGeorge Syndrome: Patient Report with a Review of Endocrine Autoimmunity Associated with 22q11.2 Deletion. J. Pediatr. Endocrinol. Metab. 2004, 17, 1575–1579. [Google Scholar] [CrossRef] [PubMed]
- Segni, M.; Zimmerman, D. Autoimmune Hyperthyroidism in Two Adolescents with DiGeorge/Velocardiofacial Syndrome (22q11 Deletion). Eur. J. Pediatrics 2002, 161, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Davies, E.G.; Cheung, M.; Gilmour, K.; Maimaris, J.; Curry, J.; Furmanski, A.; Sebire, N.; Halliday, N.; Mengrelis, K.; Adams, S.; et al. Thymus Transplantation for Complete DiGeorge Syndrome: European Experience. J. Allergy Clin. Immunol. 2017, 140, 1660–1670.e16. [Google Scholar] [CrossRef] [Green Version]
- Meek, C.L.; Kaplan, F.; Pereira, R.S.; Viljoen, A. Hypocalcemia Following Treatment for Hyperthyroidism. Clin. Chem. 2011, 57, 811–814. [Google Scholar] [CrossRef] [Green Version]
- Aversa, T.; Lombardo, F.; Corrias, A.; Salerno, M.; De Luca, F.; Wasniewska, M. In Young Patients with Turner or Down Syndrome, Graves’ Disease Presentation Is Often Preceded by Hashimoto’s Thyroiditis. Thyroid 2014, 24, 744–747. [Google Scholar] [CrossRef]
- Kawame, H.; Adachi, M.; Tachibana, K.; Kurosawa, K.; Ito, F.; Gleason, M.M.; Weinzimer, S.; Levitt-Katz, L.; Sullivan, K.; McDonald-McGinn, D.M. Graves’ Disease in Patients with 22q11.2 Deletion. J. Pediatr. 2001, 139, 892–895. [Google Scholar] [CrossRef] [PubMed]
- Hogendorf, A.; Lipska-Zietkiewicz, B.S.; Szadkowska, A.; Borowiec, M.; Koczkowska, M.; Trzonkowski, P.; Drozdz, I.; Wyka, K.; Limon, J.; Mlynarski, W. Chromosome 18q Deletion Syndrome with Autoimmune Diabetes Mellitus: Putative Genomic Loci for Autoimmunity and Immunodeficiency. Pediatr. Diabetes 2016, 17, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Lomenick, J.P.; Smith, W.J.; Rose, S.R. Autoimmune Thyroiditis in 18q Deletion Syndrome. J. Pediatr. 2005, 147, 541–543. [Google Scholar] [CrossRef]
- Tutunculer, F.; Darendeliler, F.; Gunoz, H.; Karaman, B.; Kayserili, H. 18q Deletion Syndrome Associated with Autoimmune Thyroid Disease Presenting as Hyperthyroidism. J. Pediatric Endocrinol. Metab. JPEM. 2005, 419–420. [Google Scholar] [CrossRef] [PubMed]
- Ohkubo, K.; Ihara, K.; Ohga, S.; Ishimura, M.; Hara, T. Hypothyroidism and Levothyroxine-Responsive Liver Dysfunction in a Patient with Ring Chromosome 18 Syndrome. Thyroid 2012, 22, 1080–1083. [Google Scholar] [CrossRef] [Green Version]
- Sharkia, M.; Michaud, S.; Berthier, M.T.; Giguère, Y.; Stewart, L.; Deladoëy, J.; Deal, C.; Van Vliet, G.; Chanoine, J.P. Thyroid Function from Birth to Adolescence in Prader-Willi Syndrome. J. Pediatr. 2013, 163, 800–805. [Google Scholar] [CrossRef]
- Güler, S.; Yeşil, G.; Önal, H. Endocrinological Evaluations of a Neurofibromatosis Type 1 Cohort: Is It Necessary to Evaluate Autoimmune Thyroiditis in Neurofibromatosis Type 1? Balkan Med. J. 2017, 34, 522–526. [Google Scholar] [CrossRef]
- Nanda, A. Autoimmune Diseases Associated with Neurofibromatosis Type 1. Pediatr. Dermatol. 2008, 25, 392–393. [Google Scholar] [CrossRef]
- Quaio, C.R.D.C.; Carvalho, J.F.; da Silva, C.A.; Bueno, C.; Brasil, A.S.; Pereira, A.C.; Jorge, A.A.L.; Malaquias, A.C.; Kim, C.A.; Bertola, D.R. Autoimmune Disease and Multiple Autoantibodies in 42 Patients with RASopathies. Am. J. Med. Genet. A 2012, 158A, 1077–1082. [Google Scholar] [CrossRef]
- Lee, M.J.; Kim, B.Y.; Ma, J.S.; Choi, Y.E.; Kim, Y.O.; Cho, H.J.; Kim, C.J. Hashimoto Thyroiditis with an Unusual Presentation of Cardiac Tamponade in Noonan Syndrome. Korean J. Pediatr. 2016, 59 (Suppl. 1), S112–S115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamza, R.T.; Raof, N.A.; Abdallah, K.O. Prevalence of Multiple Forms of Autoimmunity in Egyptian Patients with Turner Syndrome: Relation to Karyotype. J. Pediatr. Endocrinol. Metab. 2013, 26, 545–550. [Google Scholar] [CrossRef]
- Bondy, C.A. Care of Girls and Women with Turner Syndrome: A Guideline of the Turner Syndrome Study Group. J. Clin. Endocrinol. Metab. 2007, 92, 10–25. [Google Scholar] [CrossRef] [Green Version]
- Jørgensen, K.T.; Rostgaard, K.; Bache, I.; Biggar, R.J.; Nielsen, N.M.; Tommerup, N.; Frisch, M. Autoimmune Diseases in Women with Turner’s Syndrome. Arthritis Rheum. 2010, 62, 658–666. [Google Scholar] [CrossRef]
- Zinn, A.R.; Tonk, V.S.; Chen, Z.; Flejter, W.L.; Gardner, H.A.; Guerra, R.; Kushner, H.; Schwartz, S.; Sybert, V.P.; Van Dyke, D.L.; et al. Evidence for a Turner Syndrome Locus or Loci at Xp11.2-P22.1. Am. J. Hum. Genet. 1998, 63, 1757–1766. [Google Scholar] [CrossRef] [Green Version]
- Bakalov, V.K.; Gutin, L.; Cheng, C.M.; Zhou, J.; Sheth, P.; Shah, K.; Arepalli, S.; Vanderhoof, V.; Nelson, L.M.; Bondy, C.A. Autoimmune Disorders in Women with Turner Syndrome and Women with Karyotypically Normal Primary Ovarian Insufficiency. J. Autoimmun. 2012, 38, 315–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianco, B.; Verreschi, I.T.N.; Oliveira, K.C.; Guedes, A.D.; Galera, B.B.; Galera, M.F.; Barbosa, C.P.; Lipay, M.V.N. PTPN22 Polymorphism Is Related to Autoimmune Disease Risk in Patients with Turner Syndrome. Scand. J. Immunol. 2010, 72, 256–259. [Google Scholar] [CrossRef] [PubMed]
- Stenberg, A.E.; Sylvén, L.; Magnusson, C.G.M.; Hultcrantz, M. Immunological Parameters in Girls with Turner Syndrome. J. Negat. Results Biomed. 2004, 3, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cacciari, E.; Masi, M.; Fantini, M.P.; Licastro, F.; Cicognani, A.; Pirazzoli, P.; Villa, M.P.; Specchia, F.; Forabosco, A.; Franceschi, C.; et al. Serum Immunoglobulins and Lymphocyte Subpopulations Derangement in Turner’s Syndrome. Int. J. Immunogenet. 1981, 8, 144–337. [Google Scholar] [CrossRef]
- Su, M.A.; Stenerson, M.; Liu, W.; Putnam, A.; Conte, F.; Bluestone, J.A.; Anderson, M.S. The Role of X-Linked FOXP3 in the Autoimmune Susceptibility of Turner Syndrome Patients. Clin. Immunol. 2009, 131, 139–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, Y.A.; Kim, H.R.; Lee, J.S.; Jung, H.W.; Kim, H.Y.; Lee, G.M.; Lee, J.; Sim, J.H.; Oh, S.J.; Chung, D.H.; et al. CD4+FOXP3+ Regulatory T Cells Exhibit Impaired Ability to Suppress Effector T Cell Proliferation in Patients with Turner Syndrome. PLoS ONE 2015, 10, e0144549. [Google Scholar] [CrossRef] [Green Version]
- Sznurkowska, K.; Boćkowska, M.; Zieliński, M.; Plata-Nazar, K.; Trzonkowski, P.; Liberek, A.; Kamińska, B.; Szlagatys-Sidorkiewicz, A. Peripheral Regulatory T Cells and Anti-Inflammatory Cytokines in Children with Juvenile Idiopathic Arthritis. Acta Biochim. Pol. 2018, 65, 119–123. [Google Scholar] [CrossRef]
- Roizen, N.J.; Patterson, D. Down’s Syndrome. Lancet (Lond. Engl.) 2003, 361, 1281–1289. [Google Scholar] [CrossRef]
- Weijerman, M.E.; De Winter, J.P. Clinical Practice: The Care of Children with Down Syndrome. Eur. J. Pediatrics 2010, 169, 1445–1452. [Google Scholar] [CrossRef] [Green Version]
- Kazemi, M.; Salehi, M.; Kheirollahi, M. Down Syndrome: Current Status, Challenges and Future Perspectives. Int. J. Mol. Cell. Med. 2016, 5, 125–133. [Google Scholar] [CrossRef]
- Bull, M.J. Health Supervision for Children with Down Syndrome. Pediatrics 2011, 128, 393–406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whooten, R.; Schmitt, J.; Schwartz, A. Endocrine Manifestations of Down Syndrome. Curr. Opin. Endocrinol. Diabetes. Obes. 2018, 25, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Amr, N.H. Thyroid Disorders in Subjects with down Syndrome: An Update. Acta Biomed. 2018, 89, 132–139. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, R.; Debom, G.; Soares, F.; Machado, C.; Pureza, J.; Peres, W.; De Lima Garcias, G.; Duarte, M.F.; Schetinger, M.R.C.; Stefanello, F.; et al. Alterations of Ectonucleotidases and Acetylcholinesterase Activities in Lymphocytes of Down Syndrome Subjects: Relation with Inflammatory Parameters. Clin. Chim. Acta 2014, 433, 105–110. [Google Scholar] [CrossRef] [Green Version]
- Kyritsi, E.M.; Kanaka-Gantenbein, C. Autoimmune Thyroid Disease in Specific Genetic Syndromes in Childhood and Adolescence. Front. Endocrinol. (Lausanne) 2020, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- Meyerovitch, J.; Antebi, F.; Greenberg-Dotan, S.; Bar-Tal, O.; Hochberg, Z. Hyperthyrotropinaemia in Untreated Subjects with Down’s Syndrome Aged 6 Months to 64 Years: A Comparative Analysis. Arch. Dis. Child. 2012, 97, 595–598. [Google Scholar] [CrossRef]
- Damle, N.; Das, K.; Bal, C. Graves’ Disease in a Down’s Syndrome Patient Responds Well to Radioiodine Rather than Antithyroid Drugs. J. Pediatric Endocrinol. Metab. JPEM. 2011, 24, 611. [Google Scholar] [CrossRef] [PubMed]
- Smals, A.G.H.; Kloppenborg, P.W.C.; Lequin, R.L.; Beex, L.; Ross, A.; Benraad, T.J. The Pituitary Thyroid Axis in Klinefelter’s Syndrome. Acta Endocrinol. (Copenh) 1977, 84, 72–79. [Google Scholar] [CrossRef]
- Wortsman, J.; Moses, H.W.; Dufau, M.L. Increased Incidence of Thyroid Disease among Men with Hypergonadotropic Hypogonadism. Am. J. Med. 1986, 80, 1055–1059. [Google Scholar] [CrossRef]
- Tahani, N.; Ruga, G.; Granato, S.; Spaziani, M.; Panimolle, F.; Anzuini, A.; Lenzi, A.; Radicioni, A.F. A Combined Form of Hypothyroidism in Pubertal Patients with Non-Mosaic Klinefelter Syndrome. Endocrine 2017, 55, 513–518. [Google Scholar] [CrossRef]
- Belling, K.; Russo, F.; Jensen, A.B.; Dalgaard, M.D.; Westergaard, D.; De Meyts, E.R.; Skakkebaek, N.E.; Juul, A.; Brunak, S. Klinefelter Syndrome Comorbidities Linked to Increased X Chromosome Gene Dosage and Altered Protein Interactome Activity. Hum. Mol. Genet. 2017, 26, 1219–1229. [Google Scholar] [CrossRef] [Green Version]
- Seminog, O.O.; Seminog, A.B.; Yeates, D.; Goldacre, M.J. Associations between Klinefelter’s Syndrome and Autoimmune Diseases: English National Record Linkage Studies. Autoimmunity 2015, 48, 125–128. [Google Scholar] [CrossRef] [PubMed]
- Pober, B.R. Williams-Beuren Syndrome. N. Engl. J. Med. 2010, 362, 239–252. [Google Scholar] [CrossRef] [PubMed]
- Selicorni, A.; Fratoni, A.; Pavesi, M.A.; Bottigelli, M.; Arnaboldi, E.; Milani, D. Thyroid Anomalies in Williams Syndrome: Investigation of 95 Patients. Am. J. Med. Genet. 2006, 140, 1098–1101. [Google Scholar] [CrossRef]
- Stagi, S.; Bindi, G.; Neri, A.S.; Lapi, E.; Losi, S.; Jenuso, R.; Salti, R.; Chiarelli, F. Thyroid Function and Morphology in Patients Affected by Williams Syndrome. Clin. Endocrinol. (Oxf.) 2005, 63, 456–460. [Google Scholar] [CrossRef]
- Allegri, L.; Baldan, F.; Mio, C.; De Felice, M.; Amendola, E.; Damante, G. BAZ1B Is a Candidate Gene Responsible for Hypothyroidism in Williams Syndrome. Eur. J. Med. Genet. 2020, 63, 103894. [Google Scholar] [CrossRef]
- Morris, C.A.; Braddock, S.R. Health Care Supervision for Children With Williams Syndrome. Pediatrics 2020, 145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cambiaso, P.; Orazi, C.; Digilio, M.C.; Loche, S.; Capolino, R.; Tozzi, A.; Faedda, A.; Cappa, M. Thyroid Morphology and Subclinical Hypothyroidism in Children and Adolescents with Williams Syndrome. J. Pediatr. 2007, 50, 62–65. [Google Scholar] [CrossRef]
- Chen, W.-J.; Ji, C.; Yao, D.; Zhao, Z.-Y. Thyroid Evaluation of Children and Adolescents with Williams Syndrome in Zhejiang Province. J. Pediatr. Endocrinol. Metab. 2017, 30, 1271–1276. [Google Scholar] [CrossRef]
- Amenta, S.; Sofocleous, C.; Kolialexi, A.; Thomaidis, L.; Giouroukos, S.; Karavitakis, E.; Mavrou, A.; Kitsiou, S.; Kanavakis, E.; Fryssira, H. Clinical Manifestations and Molecular Investigation of 50 Patients with Williams Syndrome in the Greek Population. Pediatr. Res. 2005, 57, 789–795. [Google Scholar] [CrossRef] [Green Version]
- Brunet, A.; Gabau, E.; Perich, R.M.; Valdesoiro, L.; Brun, C.; Caballín, M.R.; Guitart, M. Microdeletion and Microduplication 22q11.2 Screening in 295 Patients with Clinical Features of DiGeorge/Velocardiofacial Syndrome. Am. J. Med. Genet. A 2006, 140, 2426–2432. [Google Scholar] [CrossRef] [PubMed]
- Bassett, A.S.; McDonald-McGinn, D.M.; Devriendt, K.; Digilio, M.C.; Goldenberg, P.; Habel, A.; Marino, B.; Oskarsdottir, S.; Philip, N.; Sullivan, K.; et al. Practical Guidelines for Managing Patients with 22q11.2 Deletion Syndrome. J. Pediatr. 2011, 159, 332–9.e1. [Google Scholar] [CrossRef]
- Sullivan, K.E. Chromosome 22q11.2 Deletion Syndrome and DiGeorge Syndrome. Immunol. Rev. 2019, 287, 186–201. [Google Scholar] [CrossRef]
- Sullivan, K.E.; McDonald-McGinn, D.; Zackai, E.H. CD4(+) CD25(+) T-Cell Production in Healthy Humans and in Patients with Thymic Hypoplasia. Clin. Diagn. Lab. Immunol. 2002, 9, 1129–1131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McLean-Tooke, A.; Spickett, G.P.; Gennery, A.R. Immunodeficiency and Autoimmunity in 22q11.2 Deletion Syndrome. Scand. J. Immunol. 2007, 66, 1–7. [Google Scholar] [CrossRef]
- Marom, T.; Roth, Y.; Goldfarb, A.; Cinamon, U. Head and Neck Manifestations of 22q11.2 Deletion Syndromes. Eur. Arch. Otorhinolaryngol. 2012, 269, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Stagi, S.; Lapi, E.; Gambineri, E.; Salti, R.; Genuardi, M.; Colarusso, G.; Conti, C.; Jenuso, R.; Chiarelli, F.; Azzari, C.; et al. Thyroid Function and Morphology in Subjects with Microdeletion of Chromosome 22q11 (Del(22)(Q11)). Clin. Endocrinol. (Oxf.) 2010, 72, 839–844. [Google Scholar] [CrossRef]
- Shugar, A.L.; Shapiro, J.M.; Cytrynbaum, C.; Hedges, S.; Weksberg, R.; Fishman, L. An Increased Prevalence of Thyroid Disease in Children with 22q11.2 Deletion Syndrome. Am. J. Med. Genet. A 2015, 167, 1560–1564. [Google Scholar] [CrossRef]
- de Almeida, J.R.; James, A.L.; Papsin, B.C.; Weksburg, R.; Clark, H.; Blaser, S. Thyroid Gland and Carotid Artery Anomalies in 22q11.2 Deletion Syndromes. Laryngoscope 2009, 119, 1495–1500. [Google Scholar] [CrossRef]
- Cody, J.D.; Ghidoni, P.D.; DuPont, B.R.; Hale, D.E.; Hilsenbeck, S.G.; Stratton, R.F.; Hoffman, D.S.; Muller, S.; Schaub, R.L.; Leach, R.J.; et al. Congenital Anomalies and Anthropometry of 42 Individuals with Deletions of Chromosome 18q. Am. J. Med. Genet. 1999, 85, 455–462. [Google Scholar] [CrossRef]
- Stricker, R.B.; Linker, C.A. Pernicious Anemia, 18q Deletion Syndrome, and IgA Deficiency. JAMA 1982, 248, 1359–1360. [Google Scholar] [CrossRef]
- Rosen, P.; Hopkin, R.J.; Glass, D.N.; Graham, T.B. Another Patient with Chromosome 18 Deletion Syndrome and Juvenile Rheumatoid Arthritis. J. Rheumatol. 2004, 31, 998–1000. [Google Scholar] [PubMed]
- Schaub, R.L.; Hale, D.E.; Rose, S.R.; Leach, R.J.; Cody, J.D. The Spectrum of Thyroid Abnormalities in Individuals with 18q Deletions. J. Clin. Endocrinol. Metab. 2005, 90, 2259–2263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passone, C.B.G.; Pasqualucci, P.L.; Franco, R.R.; Ito, S.S.; Mattar, L.B.F.; Koiffmann, C.P.; Soster, L.A.; Carneiro, J.D.A.; Cabral Menezes-Filho, H.; Damiani, D. Prader-willi Syndrome: What is the General Pediatrician Supposed to Do?—A review. Rev. Paul. Pediatr. 2018, 36, 345–352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angulo, M.A.; Butler, M.G.; Cataletto, M.E. Prader-Willi Syndrome: A Review of Clinical, Genetic, and Endocrine Findings. J. Endocrinol. Invest. 2015, 38, 1249–1263. [Google Scholar] [CrossRef] [Green Version]
- Iughetti, L.; Vivi, G.; Balsamo, A.; Corrias, A.; Crinò, A.; Delvecchio, M.; Gargantini, L.; Greggio, N.A.; Grugni, G.; Hladnik, U.; et al. Thyroid Function in Patients with Prader-Willi Syndrome: An Italian Multicenter Study of 339 Patients. J. Pediatr. Endocrinol. Metab. 2019, 32, 159–165. [Google Scholar] [CrossRef]
- Rad, E.; Tee, A.R. Neurofibromatosis Type 1: Fundamental Insights into Cell Signalling and Cancer. Semin. Cell Dev. Biol. 2016, 52, 39–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, J.L.; Gutmann, D.H. Neurofibromatosis Type 1. Handb. Clin. Neurol. 2015, 132, 75–86. [Google Scholar] [CrossRef]
- Roberts, A.E.; Allanson, J.E.; Tartaglia, M.; Gelb, B.D. Noonan Syndrome. Lancet (Lond. Engl.) 2013, 381, 333–342. [Google Scholar] [CrossRef] [Green Version]
- Cho, E.-K.; Kim, J.; Yang, A.; Ki, C.-S.; Lee, J.-E.; Cho, S.Y.; Jin, D.-K. Clinical and Endocrine Characteristics and Genetic Analysis of Korean Children with McCune-Albright Syndrome: A Retrospective Cohort Study. Orphanet J. Rare Dis. 2016, 11, 113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tessaris, D.; Corrias, A.; Matarazzo, P.; De Sanctis, L.; Wasniewska, M.; Messina, M.F.; Vigone, M.C.; Lala, R. Thyroid Abnormalities in Children and Adolescents with McCune-Albright Syndrome. Horm. Res. Paediatr. 2012, 78, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Tufano, M.; Ciofi, D.; Amendolea, A.; Stagi, S. Auxological and Endocrinological Features in Children with McCune Albright Syndrome: A Review. Front. Endocrinol. (Lausanne) 2020, 11, 522. [Google Scholar] [CrossRef]
- Merchant, N.; Viau-Colindres, J.M.; Hicks, K.A.; Balazs, A.E.; Wesson, D.E.; Lopez, M.E.; Karaviti, L. McCune-Albright Syndrome with Unremitting Hyperthyroidism at Early Age: Management Perspective for Early Thyroidectomy. Glob. Pediatr. Health 2019, 6, 2333794X19875153. [Google Scholar] [CrossRef] [PubMed]
- Congedo, V.; Celi, F.S. Thyroid Disease in Patients with McCune-Albright Syndrome. Pediatr. Endocrinol. Rev. 2007, 4 (Suppl. 4), 429–433. [Google Scholar] [PubMed]
- Legrand, M.A.; Raverot, G.; Nicolino, M.; Chapurlat, R. GNAS Mutated Thyroid Carcinoma in a Patient with Mc Cune Albright Syndrome. Bone Rep. 2020, 13, 100299. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors, Years | TS Population (n) | TS Population Age Range or Mean (y) | HT Prevalence (%) | GD Prevalence (%) | Autoimmune Associated Disease and Prevalence (%) | Association with AITDs and Specific Karyotype |
|---|---|---|---|---|---|---|
| Stoklasova et al., 2019 [33] | 286 | 2.8–43.3 | NA | NA | 8.7% CD, 2.1% V, 1.4% AA, 1.4% P, 0.7% IBD | Yes (Xp deletion/triple X mosaicism) |
| Witkowska-Sędek et al., 2017 [45] | 41 | 6–18 | 19.5% | NA | NA | No |
| Chen et al., 2015 [78] | 69 | 0.2–18 | 10% | 4.3% | DMT1 | No |
| Valenzise et al., 2014 [89] | 408 | 1–40 | NA | 1.7% | DMT1, CD | No |
| Grossi et al., 2013 [100] | 66 | 1–29.8 | 21% | 0 | 3% CD, 1.5% AA, 1.5% DMT1, 1.5% V, | Yes (isoXq) |
| Hamza et al., 2013 [122] | 80 | 4.7–22.3 | 6.3% | 1.3% | 12.5% CD, 3.75% anti-GAD-65, 1.25% ACA | Yes (IsoXq) |
| Kucharska et al., 2013 [36] | 54 | 1–18 | 20% | 0 | NA | NA |
| Gawlik et al., 2011 [37] | 86 | 0–17.4 | 17% | 0 | NA | No |
| Fukuda et al., 2009 [39] | 65 | 15–61 | 31% | 4.6% | NA | No |
| Medeiros et al., 2009 [40] | 17 | 5.9–22.6 | 23.5% | 5.8% | NA | NA |
| Mortensen et al., 2009 [41] | 107 | 6–60 | 15% | 1.8% | 18% CD, 4% anti-GAD-65 | Only for anti-GAD-65 and isoXq |
| Bettendorf et al., 2006 [42] | 120 | >16 | 26% | 0 | CD | No |
| Livadas et al., 2005 [43] | 84 | 0.5–19 | 21% | 2.5% | NA | No |
| El-Mansoury et al., 2005 [44] | 91 | 16–71 | 25% | 2% | NA | No |
| Elsheikh et al., 2001 [46] | 145 | 16–52 | 15% | 0.7% | NA | Yes (isoXq) |
| Medeiros et al., 2000 [48] | 71 | 0–19.9 | 9.8% | NA | NA | No |
| Hanew et al., 2018 [55] | 492 | 17-42 | 25.2% | 1.8% | 1.8% IBD | No |
| Gawlik et al., 2018 [59] | 37 | 6.3–19.9 | NA | NA | CD, V | Yes (isoXq) |
| Yeşilkaya et al., 2015 [63] | 842 | 0–18 | 11.1% | 0.4% | NA | Yes (isoXq) |
| Wegiel et al., 2019 [57] | 134 | 0.4–17 | 14.9% | 0 | 1.5% P, 2.2% V, 0.7% AA, 0.7% LS, 2.7% CD, 1.5% DMT1 | No |
| Syndrome | HT Prevalence (%) | GD Prevalence (%) | Studies Considered (n) |
|---|---|---|---|
| Turner Syndrome | 6.3–31% | 0.4–5.8% | 18 [*] |
| Down Syndrome | 1.4–52.6% | 0.7–5.2% | 9 [**] |
| Prader–Willi Syndrome | sporadic | ND | 1 [117] |
| 22q11.2 Deletion Syndrome | 1.6% | 1.6% | 1 [105] |
| Williams Syndrome | ND | ND | 1 [104] |
| RASopathies | 7% | ND | 1 [120] |
| Klinefelter Syndrome | 7% | ND | 1 [102] |
| Neurofibromatosis Type 1 | 2.5% | ND | 1 [118] |
| Author, Year | DS Population (n) | DS Population Age Range or Mean (y) | HT Prevalence (%) | GD Prevalence (%) | Autoimmune-Associated Diseases and Prevalence (%) |
|---|---|---|---|---|---|
| Pepe et al., 2020 [65] | 101 | 2–17 | 36.6% | NA | 4% CD, 2% DMT1, 1% V |
| Zwaveling-Soonawala et al., 2017 [88] | 123 | 10.7 (mean) | 21.9% | 0.7% | 4% CD |
| Aversa et al., 2016 [70] | 174 | 1–18 | NA | NA | 14.3% CD, 4% DMT1, 27% AA, 13% V |
| Giménez-Barcons et al., 2014 [73] | 19 | 0–10 | 52.6% | 5.2% | 5.2% CD |
| Pellegrini et al., 2012 [74] | 29 | 1.4–22.8 | 17.2% | 3.4% | 3.5% V, 10.5% CD |
| Unachak et al., 2008 [82] | 140 | 0-14 | 1.4% | 1.4% | NA |
| Soderbergh et al., 2006 [83] | 48 | 11–56 | 18.7% | 0 | 4% CD, 4% AA, 12.5% APS1 related antibodies |
| Pierce et al., 2017 [69] | 508 | 0.05–26 | 5.1% | 1.6% | 3.7% CD, 0.8% DMT1 |
| Gruñeiro de Papendieck et al., 2002 [85] | 137 | 0.04–16 | 15.3% | 2.9% | NA |
| AlAaraj et al., 2019 [66] | 102 | 2.3 ± 3 (mean) | NA | NA | 1.96% DMT1 |
| Abdulrazzaq et al., 2018 [68] | 92 | <18 | 14.1% | NA | 4.3% DMT1, 1.1% CD |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casto, C.; Pepe, G.; Li Pomi, A.; Corica, D.; Aversa, T.; Wasniewska, M. Hashimoto’s Thyroiditis and Graves’ Disease in Genetic Syndromes in Pediatric Age. Genes 2021, 12, 222. https://doi.org/10.3390/genes12020222
Casto C, Pepe G, Li Pomi A, Corica D, Aversa T, Wasniewska M. Hashimoto’s Thyroiditis and Graves’ Disease in Genetic Syndromes in Pediatric Age. Genes. 2021; 12(2):222. https://doi.org/10.3390/genes12020222
Chicago/Turabian StyleCasto, Celeste, Giorgia Pepe, Alessandra Li Pomi, Domenico Corica, Tommaso Aversa, and Malgorzata Wasniewska. 2021. "Hashimoto’s Thyroiditis and Graves’ Disease in Genetic Syndromes in Pediatric Age" Genes 12, no. 2: 222. https://doi.org/10.3390/genes12020222
APA StyleCasto, C., Pepe, G., Li Pomi, A., Corica, D., Aversa, T., & Wasniewska, M. (2021). Hashimoto’s Thyroiditis and Graves’ Disease in Genetic Syndromes in Pediatric Age. Genes, 12(2), 222. https://doi.org/10.3390/genes12020222