Abstract
In recent years, there has been an observed increase in infections caused by carbapenem-resistant Klebsiella pneumonia (Kp) strains. The aim of this study was the phenotypic and genotypic analysis of eight K. pneumoniae NDM (Kp NDM) isolates, recovered in Poland during the years 2016 and 2018 from seven patients with urinary tract infections (UTIs), asymptomatic bacteriuria (ABU), or colonization of the gut. PCR melting profile genotyping indicated a close relationship between the strains derived from 2018, which were not related to the strain isolated in 2016. WGS results were analyzed in relation to international Kp isolates. Clonal and phylogenetic analyses were performed based on multilocus sequence typing (MLST) and single nucleotide polymorphisms (SNPs) of the core genome. The metallo-β-lactamase was assigned to the NDM-1 type and the sequence was identified as ST11. Eleven antimicrobial resistance genes were detected, mostly from plasmid contigs. Unprecedented profiles of plasmid replicons were described with the IncFII/pKPX-1 dominant replicon. In terms of the KL24 and O2v1 capsular antigen profiles, these isolates corresponded to Greek strains. Strains isolated from UTI, ABU, and colonization GI tract patients were not carrying environment-specific virulence genes. Based on the assessment of strain relationships at the genome level and their direction of evolution, the international character of the sublines was demonstrated, with a documented epidemic potential in Poland and Greece. In conclusion, some groups of patients, e.g., renal transplant recipients or those with complicated UTIs, who are frequently hospitalized and undergoing antibiotic therapy, should be monitored not only for the risk of UTI, but also for colonization by Kp NDM strains.
1. Introduction
In recent years, there has been a substantial increase in the number of reported cases and outbreaks caused by K. pneumoniae (Kp) strains, both extended spectrum β-lactamase (ESBL) strains and Kp carbapenemase (KPC)- and metallo-β-lactamase (MBL)-producing strains [1,2]. The persistence of these carbapenemase-producing enterobacteriaceae (CPE) in the hospital environment and their ability to spread between patients make Kp strains a serious problem in European hospitals and around the world [3]. European countries have documented around 16.8% of the total global NDM-1 producers, the American continent around 10.8%, Africa around 10.8%, and Australia 1.6% [4].
The greatest epidemic threat to the hospital environment is now the strains of Kp, which produce New Delhi metallo-β-lactamases (NDMs) [5,6]. The resistance of Kp New Delhi strains to carbapenems is the result of an enzyme coded by the blaNDM gene, which is capable of hydrolyzing almost all β-lactam antibiotics [5,7]. The genes encoding NDMs are often located on plasmids, particularly IncX3, IncFII, IncA/C, FIA/B, and transposon types, and can thus be transferred between bacterial strains by vertical and horizontal transfer. Additionally, mobile genetic elements such as insertion sequences (ISs) can change their location inside the genome, pick up adjacent sequences, and mobilize resistance genes to move (ISCR27), or take part in the expression of carbapenemase genes (ISAba125) [8,9,10].
The metallo-β-lactamase NDM is a lipoprotein anchored to the bacterial outer membrane. This increases the stability of the enzyme, and its secretion in outer membrane vesicles protects against the action of β-lactam antibiotics [11]. It is also conducive to rapid spreading of both the bacteria themselves and the transfer of plasmids carrying the blaNDM gene [12].
Fuursted et al. have described the virulence potential of Kp carrying NDM-1 using mouse and nematode models, and suggested a role for this virulence in rapid global spread [13]. Virulence-associated factors (VFs) are associated with different types of infection. They include fimbriae (i.e., 1, 3), siderophores (i.e., enterobactin, salmochelin, aerobactin, yersiniabactin), lipopolysaccharide (LPS) [14,15], and 79 serological K types of capsules [16]. The hypermucoviscosity (HM) phenotype of Kp was initially associated with several specific types of capsules, but it is now known that the HM phenotype is related to the expression of the rmpA and rmpA2 genes and not the capsule type [17,18]. Strain-specific VFs are included in the flexible gene pool, which are responsible for adaptation to a specific replicative niche. The location on the genomic island, genomic islets, phages, plasmids, near integrons, and transposons can all facilitate their horizontal or vertical transfer [14].
Based on seven loci (mdh, infB, tonB, gapA, phoE, pgi, and rpoB), we classified MDR Kp strains by sequence type (ST). There are 29 recorded NDM variants across several bacterial species [19], which differ in their amino acid substitutions. NDM-1 is the most common variant, and for epidemic (very fast spread, difficult eradication) and clinical (multi-drug resistance, limited therapeutic options) reasons, these strains are a big problem within the hospital environment [3,20]. The most common sequence types of strains of Kp with NDM expression include ST11, ST14, ST15, ST147, ST149, ST231, and ST 258 [21,22,23,24]. Since 2012, there has been a massive expansion of Kp ST11 producing NDM-1 in Poland, which is one of the most remarkable recent phenomena in CPE epidemiology in Europe [20,25]. Since 2016, there has been an uncontrolled spread of these strains in Poland, and their occurrence is now reported in all provinces [26,27]. The multi-resistance of bacteria and the lack of new effective antibiotics reduce the chance of therapeutic success in the treatment of infections. Therefore, prevention is necessary, in particular screening, as well as cutting off transmission pathways of epidemic clumps through hand hygiene and isolation of infected and colonized patients. Scientific research is also needed; that is, detection, analysis, and tracking of the spread of epidemic Kp NDM-1 clones in various regions of Poland.
K. pneumoniae contributes to the inflammation of the lungs, liver abscesses, and sepsis, and is an etiological agent of urinary tract infections (UTIs). UTI is the most common infectious complication after renal transplantation (RTx) [28,29]. Most episodes of UTI occur during the first 6 months after transplantation and one of the utmost frequently isolated microorganisms is Klebsiella spp. [30,31,32]. Here, we present the phylogenetic relationships and genomic characteristics of Kp NDM isolates from the recent outbreak causing urinary tract infection, and inter alia for renal transplant recipients. We discuss the problem of Kp NDM colonization of the gastrointestinal tract and asymptomatic bacteriuria (ABU) in the context of the risk of UTI, nosocomial infection, and problems with treatment for immunodeficient patients. We used meta-analysis of genomes for genome comparisons of our strains to nationally and internationally recorded strains, exploring their epidemic and evolutionary origins.
2. Materials and Methods
2.1. Patients and K. pneumoniae Collection
A total of eight Kp NDM isolates were tested, seven of which had been isolated in either 2016 or 2018, from six patients (one patient with two isolates) hospitalized in the Department of Nephrology, Transplantology, and Internal Medicine, the Medical University of Gdańsk, Poland. An eighth isolate was sent for diagnostic purposes to the University Clinical Laboratory in Gdańsk from another hospital in Poland (Toruń) and it was also used as a reference strain for genotyping. The list of strains and their origin is given in Table 1 and Figure S1. The strains were stored at −80 °C (microbank, BioMaxima S.A. Lublin, Poland) for further analysis. The strains were routinely cultured at 37 °C using Lysogeny agar (LA) and broth (LB).

Table 1.
Overview of patient and strain details used in the epidemiological analysis.
2.2. Antibiotic Susceptibility Testing
Identification and antibiotic susceptibility were determined using the VITEK® 2 Compact (bioMérieux, Marcy l’Étoile, France). Susceptibility assays were interpreted according to EUCAST v 10.0 (2020) recommendations [33]. ESBL production was confirmed using E-test (Etest® strips, bioMérieux, Marcy l’Étoile, France) and carbapenemase production was confirmed with a β-CARBA® test (Bio-Rad Laboratories, Marnes-la-Coquette, France). The presence of the blaNDM-1 gene was detected by the PCR technique, as described [34].
2.3. Ethical Statements
This study was approved by the Local Bioethics Committee at the Medical University of Gdańsk (Gdańsk, Poland) (decision no. NKBBN/120/2019). The medical personnel responsible for the taking of samples were not involved in authoring the study, and information about patients was not available to the authors of the publication.
2.4. DNA Isolation
Genomic DNA was extracted from 3–4 colonies on an LA agar plate using the Genomic DNA Kit (Bioline, Ltd. England), as detailed in the manufacturer’s instructions. The DNA concentrations were measured using a NanoDrop ND-100 (Thermo Fisher Scientific, Spectro-Lab, Łomianki/Warsow, Poland) and were at the level of 10–40 ng μL−1.
2.5. Clonal Genetic Relatedness Analysis by PCR MP Genotyping
A PCR MP method was used according to the procedure described by Stojowska et al. [35], with the slight modification described by Gołębiewska et al. [36]. Comparisons of electrophoretic profiles, based on band position, were made using Bio-Rad software (FPQuestTM software, BioRad, Ver. 4.5) and UPGMA (unweighted pair-group method with arithmetic averages). The Pi cut-off for genotype definition was 96%.
2.6. Whole Genome Sequencing (WGS) and Genome Assembling
Genomes of all isolates were sequenced with the Illumina MiSeq platform (Illumina, Wellcome Trust Sanger Centre, Hinxton, UK). Read cleaning (i.e., removing the sequencing adapters), filtration, and trimming according to quality and length criteria were performed using Trimmomatic (Ver. 0.36) [33]. The genomes were de novo assembled using SPAdes (Ver. 3.10.1) [37]. Bacterial sequence reads were assembled into primary contigs, which were deposited in the NCBI’s database with BioProject and BioSamples accession numbers PRJNA688074 and SAMN17168596–603, respectively. Quast (Ver. 5.0.2) [38] was used to generate summary statistics for each assembly (Table S1).
2.7. Phylogenetic Analysis of K. pneumoniae Genomes
The draft genomes were annotated with Prokka (Ver. 1.11) [39] using default parameters, and the pangenome analysis was completed using Roary (Ver. 3.6.0) [40], specifying 95% identity blastp. Using a custom-made pipeline, a multi-FASTA file was obtained for each target core gene. These were aligned gene-by-gene using Muscle (Ver. 3.8.31) [41], then concatenated using a custom python script. The maximum-likelihood (ML) core gene phylogenetic tree was generated from the concatenated alignment core genes using the GTR model in RAxML (randomized accelerated maximum likelihood) (Ver. 8.2.12) [42]. The ggtree R package (Ver. 1.15.6) [43] was used for the visualization, manipulation, and annotation of the phylogenetic trees. The cluster was defined by rhierBAPS [44]. In silico MLST was performed using a BLAST-based tool [45] on de novo genome assemblies. The eight isolates were subjected to phylogenetic analysis against 71 carbapenemase-producing Kp ST11 isolates from Poland, including 67 representatives of the NDM-1 epidemic from 2012–2018 and 4 other known Polish carbapenemase-positive Kp ST11 sequences available from GenBank (accessed on 24 April 2020) [32]. Additionally, data from 101 random Kp genomes publicly available in the PATRIC database (accessed on 24 April 2020) were downloaded for inclusion in the analysis, including 90 Kp isolates belonging to sequence type ST11 and 11 Kp isolates belonging to sequence type ST258, a worldwide dominant carbapenem-resistant Kp clone that is closely related to ST11. Another ST was added in order to give context with other important STs.
A diagram showing the groups of the analyzed strains in this work is presented in Figure S2. Metadata were provided for all bacterial isolates included in the study (Table S2). These include year, country, and city of isolation; source; specimen type; infection status; clinical information where available (e.g., clinical syndrome, type of infection); patient outcome (e.g., died in hospital, discharged); and mode of acquisition (nosocomial if isolated more than 48 h after admission to hospital, otherwise community acquired).
2.8. Single Nucleotide Polymorphism (SNP) Identification
An SNP pairwise difference matrix from the core gene was obtained for ST11 and other STs using snp-dists (Ver. 0.6.3). The SNP analysis of the core genome alignment was completed by aligning the short-reads data from each isolate against the reference, the first outbreak isolate from Poland from 2012 (BioSample accession number SAMN14314560), for a comparison in high resolution among ST11 using Snippy (Ver. 3.1) [46]. The analysis pipeline was as follows: paired-end reads of each strain were mapped to the reference genome, variants were identified and annotated, and the effects of each variant on genes were predicted using the SnpEff tool (Ver. 4.3t) [47].
2.9. Virulence Factors and Resistance Gene Analysis
The ABRicate tool was used to identify antimicrobial resistance and virulence genes by running local assemblies. Antimicrobial resistance genes were detected using ResFinder 3.1 [48], with a cut-off of 100% sequence identity. Virulence gene allele sequences were retrieved from the K. pneumoniae BIGSdb database at Institut Pasteur [49], with a 95% identity threshold.
2.10. K/O Serotypes and Mobile Genetic Element Analysis
Capsule (K) and LPS (O) antigen types were differentiated among the isolates using the Kaptive tool [50]. Plasmid replicon types were identified using PlasmidFinder 2.1. [51]. Comparisons of plasmids were carried out using BLASTn, and the results were visualized using R [52]. The presence of integrative and conjugative elements, ICEKp1 and ICEKp2, was investigated using gene markers described previously [53]. BLAST was used to identify these gene markers in sequence data from our isolates.
2.11. Scoring Contigs as Plasmid or Chromosomal from Draft Genomes
The RFplasmid tool [54] was used to predict plasmid and chromosomal contigs from draft assemblies. Therefore, each contig was assigned a plasmid or chromosomal score.
2.12. Data Availability
Contig sequences for each genome were deposited in the NCBI’s database, with BioProject and BioSamples accession numbers of PRJNA688074 and SAMN17168596–603, respectively.
3. Results
3.1. Patients and Samples from the Local Hospital
The seven included Kp NDM cultures were isolated in 2016 and 2018 in the Department of Nephrology, Transplantology, and Internal Medicine, the Medical University of Gdańsk, from six patients with a medical history of kidney disease (Table 1, Figure S1). The eighth isolate was sent for analysis from another hospital in Poland to confirm resistance to carbapenems by molecular methods. It was treated as a reference strain not related to our hospital. Six Kp NDM strains were isolated from the urine of patients with symptoms of UTI (three isolates) or ABU (three isolates), including two renal transplant (RTx) recipients. The other two isolates were from the GI tract (anal swab samples), one from a RTx patient positive for Kp NDM in the urine, and the other from a patient hospitalized at the same time, in the same ward, but without UTI symptoms.
3.2. K. pneumoniae Antibiotic Susceptibility Profile
Antibiotic resistance profiles were prepared for each of the Kp NDM isolates (Table 2). ESBL production was confirmed by E-test, and carbapenemase production was confirmed with a β-CARBA® test. By obtaining a 621 bp PCR product, we also confirmed the presence of the blaNDM-1 gene in all eight isolates. Most of the tested Kp NDM strains showed similar patterns of resistance. All NDM strains were resistant to penicillins, penicillins with β-lactamase inhibitors, all generations of cephalosporins, fluoroquinolones, ertapenem, meropenem, and cefoperazone/sulbactam. In the case of the remaining carbapenems (imipenem), the degree of resistance of the strains varied. Resistance to imipenem was found in four strains, and four strains were also characterized by moderate susceptibility to this drug. We observed large differences in sensitivity to aminoglycosides. None of the strains were resistant to gentamicin while only one strain was resistant, and two strains were moderately sensitive to amikacin. One strain of NDM showed resistance to tobramycin. Most strains remained resistant to trimethoprim/sulfamethoxazole, except for strain number ND32, isolated in 2016. In the analyzed material, one strain was also found to be moderately sensitive to tigecycline. All strains remained sensitive to colistin.
Table 2.
Antibiotic susceptibility profiles for the tested K. pneumoniae strains.
3.3. Clonality of Strains from a Local Outbreak
The main aim of this task was to determine whether the strains isolated from kidney disease patients and kidney recipients were from the community or were hospital-acquired. Owing to the emergence of NDM-producing Kp in January 2018 at the Department of Nephrology, Transplantology, and Internal Diseases of the Medical University of Gdańsk, the patients had been monitored for infection and colonization during the period from January to April 2018.
Genotyping of seven Kp strains isolated from six patients, and a reference Kp strain (from another hospital, used as an outlier control), revealed three distinct genotypes, A–C (Figure 1). The Dice similarity coefficient was 96%.

Figure 1.
Genetic relatedness of 7 K. pneumoniae NDM-1 strains isolated from six patients and a reference K. pneumoniae NDM-1 strain (from another hospital used as a control) based on the PCR MP method. A dendrogram of similarity of the genetic profiles of the tested strains was developed using FPQuest Software version 4.5 (BIO-RAD) (Dice, UPGMA). Cp—the complete similarity equal to 73%; Pi—the level of identity equal to 96%; unique genotypes (Gp) are marked with the letters A–C; IS—isolate; P—patient.
The strain from 2016 (ND32) and the first strain from 2018 (ND24) had unique genotypes, A and B, respectively, indicating a new strain being present in the clinic’s renal ward in 2018. The other strains from 2018 were assigned a third, ‘C’, genotype, and were not consistent with the first strain isolated in 2018. For one patient (P4) from which two isolates were taken (ND88 and ND34), two distinct subgenotypes (C1 and C2) were described. One isolate came from the urine and the other from the patient’s GI tract (anal swab samples). The strains from the local outbreak (ND33) and the reference strain (ND27/Ref) were characterized by a high degree of similarity (98%), and were assigned to a subgenotype, C3.
3.4. Whole Genome Sequence Analysis
3.4.1. Phylogenetic Analysis
The seven studied isolates were subjected to phylogenetic analysis against the non-outbreak reference isolate sequenced by us, and 71 publicly available Polish Kp genomes, 67 of which were NDM-1 Tn125A isolates; 4 other known Polish carbapenemase-positive Kp ST11 strains, as described previously [32]; 90 randomly selected Kp strains with sequence type ST11; and 11 randomly selected Kp strains with sequence type ST258 available from the PATRIC database (Figure 2). The core-gene phylogenetic tree for eight isolates from this study is presented in Figure S3.
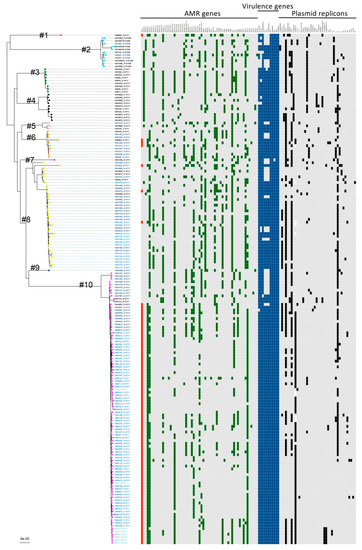
Figure 2.
K. pneumoniae core-gene phylogenetic tree. A maximum likelihood phylogenetic tree was constructed using 4014 core genes with the genome sequences of 180 K. pneumoniae isolates. The cluster numbers (#1–#10) are labelled on the phylogenetic tree and the colour of the circle in the external node is linked to the cluster (purple—cluster no. 1, cyan—cluster no. 2, green—cluster no. 3, black—cluster no. 4, pink—cluster no. 5, orange—cluster no. 6, red—cluster no. 7, yellow—cluster no. 8, blue—cluster no. 9, magenta—cluster no. 10). The origin of the isolates is distinguished by font colours in the tree: light blue—isolates sequenced in this work; blue—from Poland; deep blue—from Europe; black—from other countries. The sequence type (ST) is indicated for each isolate, following the isolate name. Numbers after the isolate name correspond to original numbers of the study isolates or GenBank assembly numbers. In the heatmap, the presence of the blaNDM-1 gene is indicated by red (present) or gray (absent) and the presence/absence profile of the genotype for 60 genes encoding antimicrobial resistance (green—present, gray—absent), 11 genes encoding virulence determinants (blue—present, gray—absent), and 40 plasmid replicons is indicated.
Phylogenetic analysis with concatenated alignment core genes showed that all seven examined isolates from our hospital represented the ST11 sequence type, with high homogeneity. The seven studied isolates were included in one clade, with 68 Polish isolates (all NDM-1) and 21 isolates from different countries around the world, 10 of which had the blaNDM-1 gene. These 21 isolates were collected in 2013–2016 in Greece (n = 9, all NDM-1), Slovakia (n = 5), the Czech Republic (n = 3), India (n = 2), Spain (n = 1), and USA (n = 1, NDM-1) (mainly from the EuSCAPE study). Five Kp NDM-1 sequences from the public database were not included in this clade. These isolates were collected in 2012–2013 in Pakistan (n = 2), Turkey (n = 1), Norway (n = 1), and Romania (n = 1). Two Kp NDM-1 sequences from Izdebski et al. [32] were also not included in this clade.
3.4.2. SNP Diversity of Core Genomes
Analysis of the cgSNP (core genome SNP) in relation to the reference strain (BioSample accession number SAMN14314560) revealed 7–88 SNPs between the individual Polish isolates sampled in this study. The timing of individual isolates from the outbreak was reflected by a gradual reduction in the number of SNP differences between temporally closer epidemic isolates, from 88 SNP differences between the January 2018 isolate and the April 2018 isolate, to 16 SNP differences between the two April 2018 isolates, showing the process of population diversification.
The isolates collected during the study showed the fewest differences to strains from Poland and Greece; differing from Greece isolates by 46–79 SNPs. Isolate no. ND32 (SAMN17168599), the first isolate from the ward, showed the fewest differences compared with strains from Greece, differing from them by 46–56 SNPs. The analysis showed that isolate no. ND27 (SAMN17168596), isolated at the same time (May 2018) as the outbreak strains, but from a different hospital, differed from the outbreak strains by 16–86 SNPs. Similarly, in the SNPs’ pairwise distance from core gene analysis, a Polish isolate taken from the public database (No. KN21460, 2013) was the closest to the studied isolates, differing from the outbreak strains by 43–64 SNPs and from strains originating in Greece by 25–36 SNPs (Table S3). The SNP distribution divided the isolates in this homogeneous clade into groups clustering with Polish, Greek, and other international isolates.
3.4.3. Resistomes
Eleven antimicrobial resistance genes in total were detected in the seven isolates from the hospital in Gdańsk, which could be used to split the strains into seven different gene profiles (Table 3 and Table S4). The resistomes comprised 5 to 10 acquired genes and an average isolate had 7.6 of these.
Table 3.
K. pneumoniae NDM-1 ST11 isolates included in this study and from the PATRIC database—plasmid replicon profile and resistomes based on sequencing WGS.
A phenotype of resistance to β-lactams was generated from the blaNDM-1, blaCTX-M-15, blaOXA-1, and blaTEM-1 genes. All four genes were present in the ND34 (GpC2)- and ND88 (GpC1)-related isolates; three genes (blaNDM-1, blaCTX-M-15, blaOXA-1) in ND32 (GpA), ND111 (GpC), ND96 (GpC), and ND27 (ref) (GpC3); and only two (blaNDM-1, blaCTX-M-15) in ND24 (GpB) and ND33 (GpC3). The aac (6′)-Ib gene, which is responsible for aminoglycoside resistance, was detected in seven isolates. The aadA1 gene was only detected in isolate ND33. Resistance to phenicols was encoded by the cat1 and cat4 genes for ND111 and ND88, and for other isolates by the catA1gene only. The ND24 isolate lacked resistance genes for this group of antibiotics. The sul1 gene, responsible for sulfonamide resistance, was included in all isolates. One or both of the dfrA1/dfrA14 genes, which contribute to resistance to trimethoprim, were detected in all isolates. Most of the genes were determined to be plasmidic. Overall, these genes enabled us to specify a perfect phenotype to genotype correlation for antibiotic susceptibility data.
3.4.4. Plasmid Analysis
The previous Polish outbreak study revealed a prevailing presence of the IncFII/pKPX-1 and IncR replicons, and high differentiation of the species. This study provides new data on the plasmid content of the epidemic genotypes resulting from a local outbreak of a nationally distributed clone. Eight replicons in total were detected across the seven isolates, which could be split into four profiles of one to six replicons each (Table 2 and Table 3), again showing the heterogeneity of the organism. The dominant replicon was IncFII/pKPX-1, which was present in six isolates.
3.4.5. Mobile Genetic Elements Analysis
The frequency of integrative conjugation elements (ICEs) ICEKp1 and ICEKp2 in clinical Kp isolates was determined. ICEKp1 was identified in 113 (70.2%) international strains and all eight strains tested in this study. ICEKp2 was present in 159 out of 161 (98.8%) international genomes, and in all genomes sequenced by us. Its presence was not correlated with ICEKp1. Among the Kp NDM-1 strains, both ICEKp1 and ICEKp were identified in 89 (96.7%) strains. The presence of ICEKp2 correlated with the presence of ICEKp1 for Kp NDM-1 strains. Additionally, the presence of two closely related sequence types, as demonstrated by the genome analysis, suggests a stable inheritance of ICEKp2. ICE contributes to the spread of antimicrobial multi-resistance genes and pathogenicity [55].
Among the eight studied strains of Kp NDM-1, ICEKp2 did not coexist with the plasmid carrying the rmpA and rmpA2 genes encoding the so-called ‘mucus factor’, which are associated with the overexpression of proteins in strains with the K1 or K2 capsule type, and increased virulence [55,56]. In contrast, the seven international strains of Kp carrying the plasmid including the rmpA and rmpA2 genes always had ICEKp2 and a partial (n = 5) or complete (n = 2) ICEKp1 element (Figure S4, Table S5).
3.4.6. Serotypes
The K and O antigens of the outbreak isolates were identified as KL24 and O2 variant 1 (O2v1), respectively, with no differences between the Polish ST11 NDM-1 strains and some of the international ST11 NDM-1 strains, especially from Greece (Table 4 and Table S6). The within-study serotype diversity of the ST11 isolates and control ST258 isolates used was significant, corresponding to previous reports.
Table 4.
K. pneumoniae NDM-1 ST11 isolates sequenced in this study and those included from the PATRIC database, serotype data, and virulomes. Legend: 0—absence, 1—presence.
3.4.7. Virulomes
Virulence-associated gene analysis (Table 4 and Table S6) showed an identical arrangement for all strains, including the chromosomal fimA-K operon, responsible for the type 1 fimbriae involved in adhesion, and the chromosomal mrkABCDF and mrkHIJ operons, responsible for the type 3 fimbriae, involved in adhesion and biofilm formation. Additional groups of virulence genes considered included those for iron secretion systems: the fyuA, irp1/2, and ybtAEPQSTUX genes specifying synthesis and secretion of yersiniabactin; iroE specifying synthesis of salmochelin; and the ybdA, entABCEF, fes, and fepABCDG genes specifying synthesis and secretion of enterobactin. The same virulence gene profile was found in close relatives of the outbreak isolates from Poland, Greece, Romania, Norway, and Turkey.
4. Discussion
Klebsiella pneumoniae (Kp) is responsible for many nosocomial infections, especially in immunocompromised patients [36,57]. Hospital wards with immunocompromised or immunosuppressed patients have reported more frequent outbreaks of Kp [58]. The Kp is characterized by a high epidemic risk in hospitals owing to increasingly common multi-drug resistance and easy acquisition of fitness genes and various virulence factors. These bacteria have the ability to create a biofilm, which makes it easier for them to colonize various ecological niches, and at the same time hinders eradication.
In some patients, colonization is associated with carrier status for multi-drug-resistant strains. UTIs, ABU, and colonization/carriage are a serious problem as they are mainly responsible for the global expansion of carbapenemase-producing Kp clones [59].
Among our patients were RTx recipients with symptomatic UTI, patients with asymptomatic bacteriuria, and patients with GI tract colonization. All these patients had a history of either chronic or kidney failure or acute kidney injury and were hospitalized in one hospital, and from each of them, Kp NDM-1 was isolated.
In patients with kidney failure, including RTx recipients, the choice of antibiotics can be limited by impaired renal function and the possibility of interaction with other drugs; it is very difficult to determine an optimal prophylaxis [60]. Many antibiotics prove ineffective owing to the lack of a capture point in both structurally and functionally altered cells. Owing to the increasing, and sometimes inappropriate, use of antibiotics, especially in this group of patients, many reports emphasize the growing incidence of multi-drug-resistant strains, in particular those from the Enterobacteriaceae family [60,61].
In recurrent UTIs, the probability that a carbapenem-resistant strain will be the etiological factor increases with each subsequent episode [62]. The use of amoxicillin with clavulanic acid, metronidazole, clindamycin, or piperacillin with tazobactam increases the intensity of gastrointestinal colonization with Kp ESBL (+). UTIs or ABU can be caused by the same Kp bacteria that colonize the patient’s digestive system. Urinary tract infections caused by ESBL strains require treatment with carbapenems, and that therapy often generates carbapenem-resistant Kp.
The causes of ABU can be explained in two ways. On one hand, uropathogenic strains are less virulent, or some genes are not expressed because of mutations (deletions, insertions). According to Zdziarski et al., asymptomatic bacteriuria is a result of genome reduction and inactivation of genes encoding virulence-associated factors by the accumulation of point mutations or deletions [63]. Attenuation of virulence may also occur among isolates during long-term carriage in the urinary tract [64]. On the other hand, the innate immunity response may be too weak to cause symptoms. ABU favors the acquisition of resistance because bacteria colonize the urinary tract, forming a biofilm, which is a perfect environment for horizontal gene transfer, similar to the GI tract.
In recent years, there have been numerous reports of epidemic outbreaks caused by MDR K. pneumoniae strains [65,66,67]. The first stage of our research was to assess the epidemic situation in the Department of Nephrology, Transplantology, and Internal Medicine, considering either commensal strains carried by the patient or strains of hospital origin. In a patient who stays in the hospital environment for a long time, the commensal intestinal microbiota can be replaced by the hospital microbiota. The Kp NDM strains showed a high degree of genetic similarity (GpC) among subgenotypes (Cp1–Cp3), distinguishing them from the 2016 strain (GpA) and the first strain that appeared in 2018 (GpB) (Figure 1). Our starting hypothesis that an endemic GpA strain could be responsible for the epidemic situation was thus rejected. Isolate no. ND24 (no. 2), with the unrelated genotype GpB, was probably a community-acquired or commensal strain associated with the microbiota of a patient. High genetic similarity of the DNA patterns for other isolates could indicate a clonal origin and local epidemic situation.
All strains showed an identical or similar resistance profile. Only for imipenem, amikacin, and tigecycline were differences in antibiotic resistance noticeable. These differences were also reflected in the genotypes and sub-genotypes of these isolates. These slight differences in genotypes and resistance profiles are associated with the progression of the isolation timeline of the Kp NDM-1 strains. To answer the question of how much variability exists at the genomic level among Kp NDM strains, we used WGS to determine the level of genetic relatedness among our isolates and between these and other strains from worldwide sources.
We have shown that our carbapenem-resistant isolates belong to the NDM-1 variant. The NDM-1 variant is considered a pandemic and has been recorded in as many as 86 countries around the world, including in Poland [68,69,70].
Phylogenetic analysis with cgMLST indicated high homogeneity with respect to sequence type (ST). All of our isolates belong to the lineage ST11, whose role in the hospital environment is significant. It has been shown that elements of ST11, together with ST340, participated in the evolution of the clonal complex CC258, which has global dissemination [71,72]. Kp core-genome phylogenetic tree analysis confirmed that these strains, belonging to one big clade in Poland [32], have a high similarity to European isolates from Greece, Slovakia, the Czech Republic, Spain, and other more distant countries such as India and the USA (Figure 2).
Analysis of the cgSNP profiles indicated 7–88 SNP differences between the individual Polish isolates. The first isolate that appeared in 2018 on the ward was the least different from Greek strains, and the isolates reveal the phenomenon of an increase in SNP differences from Greek strains over the course of the epidemic situation, in line with the diversification of the population. Although related Kp ST11 strains belonging to the same basal clade occurred globally (Table S3), the analyzed genotype appeared mainly in Europe, especially in South-Central Europe. This study demonstrates the international character of these sublines, with documented epidemic potential in Poland and Greece.
The rapid spread of Kp NDM strains to all continents is largely related to the global development of tourism [71]. Therefore, microbiological testing of patients coming back from travel, immediately after their hospital admission, is extremely important, especially if they were hospitalized at that time in countries with endemic NDM-positive strains [72,73]. The reasons for dissemination of Kp NDM should also be looked at among medical personnel coming back from medical missions in other countries with a high rate of Kp NDM incidence.
The virulence properties of Kp have been documented in many reports [36,74,75]. Capsule, LPS, siderophores, type 1 and 3 fimbriae, and biofilm formation are all subjects of recent pathogenesis research. Whole-genome sequencing (WGS) is the best molecular tool for examination of the capsular locus and the population structure of Kp. The capsule is essential for infection and protection against the host immune system. Based on association with capsule lineages, strain typing can be performed more efficiently than with MLST [50].
WGS analysis showed the same virulence profile of genes for all isolates, regardless of each sample’s origin (ABU/UTI/GI tract). Based on the type of K24 capsule, LPS o2v1 antigen, and type 1 and 3 fimbriae were detected for our isolates. The K24 capsule type is found in Polish ST11 NDM-1 strains and some strains from Greece (Figure 2). Many observations have confirmed the roles of type 1 fimbriae and type 3 fimbriae in biofilm formation, especially during chronic infections [76,77,78]. Biofilm protects against the effects of many antibiotics and promotes the growth of resistance to antibiotics. Biofilm is also produced in the GI tract, and creates an environmental niche in which different populations of bacteria come into contact with each other and can exchange genes, determining resistance to antibiotics and virulence.
Kp acquire iron through a system based on genes encoding siderophores such as yersiniabactin, salmochelin, and enterobactin, enabling the high virulence of multi-drug-resistant Kp NDM strains. The presence of the yersiniabactin high-pathogenicity island contributes to high virulence in our isolates. This type of siderophore is mainly characteristic of Kp strains responsible for the colonization of the respiratory system [79,80,81], but has also been reported in strains isolated from UTI patients [82,83]. In the case of ABU, the expression of yersiniabactin with the presence of an efficiently forming biofilm was confirmed in human urine [82]. The environment of the urinary tract is iron-poor, and bacteria must thus compete for iron. The adoption of an additional iron uptake system that is able to avoid sequestration by lipocalin-2 is thus beneficial for pathogenic bacteria. Yersiniabactin was detected among Kp NDM-1 strains isolated from Poland, Greece, Romania, Norway, and Turkey. Salmochelin and enterobactin, but not aerobactin, have additionally been implicated in Kp NDM-1 virulence.
Based on WGS, we found no differences in virulence profile across the strains responsible for UTI or ABU, and for isolates colonizing the gastrointestinal tract. The virulence of Kp probably does not determine the appearance or absence of symptoms of the disease. However, further research is required to examine strains from a larger population.
Besides clonal transmission, mobile genetic elements, including transposons and plasmids, play a role in the dissemination of multidrug-resistant clones of Kp. The blaNDM-1, blaKPC-2, blaVIM, blaIMP, and blaOXA-48 genes are responsible for resistance to carbapenems, and are transferred to other microorganisms via horizontal gene transfer [84]. The co-existence of several unrelated plasmids carrying the blaNDM-1gene and other genes encoding resistance to carbapenems, e.g., blaOXA-48, has been reported in the same bacterial cell [85]. Additionally, other antibiotic-resistant markers were detected in Kp, classifying them as an alert pathogen [6,86].
In our research, Kp NDM-1 isolates carrying the blaNDN-1gene were also carriers of genes related to resistance to antibiotics belonging to different classes: β-lactams (blaOXA-1, blaCTX-15, blaTEM), aminoglycosides (Aac (6′)-Ib, aadA1), phenicols (cat1, cat4, catA1), sulfonamides (sul1), and trimethoprim (dfrA1/dfrA14). Various types of plasmids such as IncR, IncF, IncA/C, and IncNIncL/M are involved in the carriage of the blaNDM-1 gene [87]. Concerning plasmids and replicons, our isolates showed heterogeneity (Table 3) and such profiles have not been detected previously. The strains that showed different genotypes from those identified in previous epidemiological studies also carried different sets of plasmid replicons from those strains considered epidemically related. The epidemic strains were characterized by rich plasmid replicon profiles: FIB (K), FII (K), FII (pKPX1), HI1A (NDM-CIT), and HI1B (pNDM-CIT) or FIB (K), FII (K), FII (pKPX1), HI1A (NDM-CIT), HI1B (pNDM-CIT), and X1, while the strain isolated in 2016 carried only the FII (pKPX1) plasmid replicon. Only two plasmid replicons, FII (Yp) and R, were detected for the first Kp NDM-1 strain from 2018. This is further evidence of a different origin of these strains.
Mobile genetic elements, e.g., integrative conjugation elements (ICEs), are widely recognized as contributing to the spread of antimicrobial resistance and virulence genes included in islands of pathogenicity. ICEKp1 and ICEKp2 can co-exist in Kp, and were documented during our global analysis of Kp NDM-1. ICEKp2 is often detected in the presence of a plasmid carrying the rmpA and rmpA2 genes, which is typically associated with Kp (hvKp) strains with a hypermucoviscous phenotype [55,56]. Despite the presence of the ICEK2 plasmid, our strains did not show co-existence of this plasmid. The presence of several plasmids in the same strain carrying genes related to antibiotic resistance and high-pathogenicity islands makes Kp dangerous both in hospital environments and outside of them [88].
5. Conclusions
In the case of renal transplant recipients, UTI is common because long-term immunosuppression is associated with many side effects, particularly an increased risk of infection. Organ recipients are subjected to preventive antibiotic therapy before and after transplant surgery, in order to minimize the risk of complications. Antibiotic therapy may alter the urinary microbiome composition and enrich for uropathogenic species [68]. For chronic recurrent UTI, repeated antibiotic treatment is required, hence the accumulation of antibiotic resistance in uropathogenic Kp strains.
In addition, this group of patients is particularly exposed to hospital infections; therefore, it was necessary to analyze the epidemic situation in the hospital ward.
Asymptomatic bacteriuria is also a significant problem. We ask ourselves whether or not to treat asymptomatic bacteriuria, especially considering that treatment of asymptomatic bacteriuria with targeted or empiric antibiotic therapy leads to the formation of multi-drug-resistant strains, e.g., producing carbapenemase.
Researchers are constantly looking for differences in strains that cause symptoms of UTI and those associated only with the carrier and ABU. Hence our interest in Kp NDM strains isolated not only from UTI, but also from ABU and GI tract colonization.
The aim of the study was the phenotypic and genotypic characterization of Kp strains producing metallo-β lactamase NDM, isolated from patients with kidney diseases and RTx recipients. We used WGS analysis to assess the genome diversity of local isolates in relation to national and global strains of Kp NDM-1 with the sequence type ST11. The correlation between strains was determined using PCR MP genotyping, confirming the presence of local outbreak and strains unrelated to the epidemic situation. Mobile genetic elements, in particular, integrative conjugative elements, are responsible for the dissemination of multi-drug resistance and virulence. Meta-analysis of genomes did not show signatures of UTI- and ABU-associated strains with high antimicrobial resistance. Colonization and immunosuppression can be additional risk factors, although this is seldom reported. In immunocompromised patients or those treated with antibiotics for prevention, the gut or ABU can act as reservoirs for the transmission of Kp NDM in the hospital setting.
Supplementary Materials
The following are available online at https://www.mdpi.com/article/10.3390/genes12081285/s1, Figure S1: Timeline of events in the epidemiologically linked cases of New Delhi metallo-β-lactamase 1-producing Klebsiella pneumoniae. Dates are given as month/year. Abbreviations: IS—isolate. Figure S2: Diagram showing the groups of the analyzed strains in this work. Figure S3: The core-gene phylogenetic tree for eight K. pneumoniae isolates from this study. The sequence type (ST) is indicated for each isolate, following the isolate name. In the heatmap, the presence of the blaNDM-1 gene is indicated by red (present) or gray (absent) and the presence/absence profile of the genotype for 60 genes encoding antimicrobial resistance (green—present, gray—absent), 11 genes encoding virulence determinants (blue—present, gray—absent), and 40 plasmid replicons is indicated. Figure S4: Occurrence of integrative conjugation elements (ICEKp1 and ICEKp2) in clinical isolates of K. pneumoniae. Genome core phylogenetic tree generated for 180 K. pneumoniae isolates. The color of the isolate corresponds to the presence or absence of the blaNDM-1 gene (red—present, black—absent). The sequence type (ST) is indicated for each isolate after the isolate name. The presence and co-existence of ICEKp1 and ICEKp2 (marker genes) is shown in the heatmap on the right (black—present, gray—absent). The virulence-related genes rmpA and rmpA2 were also included in the analysis to determine their correlation with the presence/absence of ICEKp1 and ICEKp2. The scale bar shown in the lower left corner shows the average number of substitutions per locus. Table S1: Strain metadata. Characteristics of the single isolates, including collection details, genome assembly statistics, and genomic features. Table S2: Metadata for all additional bacterial isolates included in the study from PATRIC database and Izdebski et al. paper [32]. Table S3: The matrix of the core genome SNPs’ differences determined against the reference genome from the same ST. Table S4: K. pneumoniae isolates included in this study from the PATRIC database—basic epidemiological data and resistomes based on sequencing WGS. Table S5: Occurrence of integrative conjugation elements (ICEKp1 and ICEKp2) in clinical isolates of K. pneumoniae sequenced in this study and from the PATRIC database as well as the paper of Izdebski et al. [32] (0—absence, 1—presence). Table S6: K. pneumoniae isolates (non NDM-1) from PATRIC database included in the study—serotypes data and virulomes (0—absence, 1—presence).
Author Contributions
Conceptualization: M.W., J.G. and B.K.; methodology: M.W.; software: M.W. and R.Z.; formal analysis: M.W., M.R.O., R.Z., J.G. and B.K.; investigation: M.W.; resources: M.B. and J.G.; data curation, M.W., M.R.O., R.Z., M.B. and J.G.; writing—original draft preparation: M.W., B.K. and R.Z.; writing—review and editing: B.K.; visualization: M.W.; supervision: M.R.O.; project administration: B.K.; funding acquisition: B.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Local Bioethics Committee at the Medical University of Gdańsk (Gdańsk, Poland) (decision no. NKBBN/120/2019).
Informed Consent Statement
Not applicable.
Data Availability Statement
Contig sequences for each genome were deposited in the NCBI’s database with BioProject and BioSamples accession numbers PRJNA688074 and SAMN17168596–603, respectively.
Acknowledgments
The work is carried out as a part of Magdalena Wysocka’s doctoral dissertation. The supervisor of the doctoral dissertation is Beata Krawczyk.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Wyres, K.L.; Holt, K.E. Klebsiella pneumoniae Population Genomics and Antimicrobial-Resistant Clones. Trends Microbiol. 2016, 24, 944–956. [Google Scholar] [CrossRef]
- Magiorakos, A.P.; Srinivasan, A.; Carey, R.B.; Carmeli, Y.; Falagas, M.E.; Giske, C.G.; Harbarth, S.; Hindler, J.F.; Kahlmeter, G.; Olsson-Liljequist, B.; et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: An international expert proposal for interim standard definitions for acquired resistance. Clin. Microbiol. Infect. 2012, 18, 268–281. [Google Scholar] [CrossRef] [PubMed]
- Albiger, B.; Glasner, C.; Struelens, M.J.; Grundmann, H.; Monnet, D.L. European Survey of Carbapenemase-Producing Enterobacteriaceae (EuSCAPE) working group. Carbapenemase-producing Enterobacteriaceae in Europe: Assessment by national experts from 38 countries, May 2015. Eurosurveillance 2015, 20, 30062. [Google Scholar] [CrossRef]
- Khan, A.U.; Maryam, L.; Zarrilli, R. Structure, Genetics and Worldwide Spread of New Delhi Metallo-β-lactamase (NDM): A threat to public health. BMC Microbiol. 2017, 17, 1–12. [Google Scholar] [CrossRef]
- Yong, D.; Toleman, M.A.; Giske, C.G.; Cho, H.S.; Sundman, K.; Lee, K.; Walsh, T.R. Characterization of a new metallo-β-lactamase gene, bla(NDM-1), and a novel erythromycin esterase gene carried on a unique genetic structure in Klebsiella pneumoniae sequence type 14 from India. Antimicrob. Agents Chemother. 2009, 53, 5046–5054. [Google Scholar] [CrossRef] [PubMed]
- Kumarasamy, K.K.; Toleman, M.A.; Walsh, T.R.; Bagaria, J.; Butt, F.; Balakrishnan, R.; Chaudhary, U.; Doumith, M.; Giske, C.G.; Irfan, S.; et al. Emergence of a new antibiotic resistance mechanism in India, Pakistan, and the UK: A molecular, biological, and epidemiological study. Lancet Infect. Dis 2010, 10, 597–602. [Google Scholar] [CrossRef]
- Deshpande, P.; Rodrigues, C.; Shetty, A.; Kapadia, F.; Hedge, A.; Soman, R. New Delhi metallo-β lactamase (NDM-1) in Enterobacteriaceae: Treatment options with carbapenems compromised. J. Assoc. Physicians India 2010, 58, 147–149. [Google Scholar] [PubMed]
- Juhas, M.; van der Meer, J.R.; Gaillard, M.; Harding, R.M.; Hood, D.W.; Crook, D.W. Genomic islands: Tools of bacterial horizontal gene transfer and evolution. FEMS Microbiol. Rev. 2009, 33, 376–393. [Google Scholar] [CrossRef] [PubMed]
- Frost, L.S.; Leplae, R.; Summers, A.O.; Toussaint, A. Mobile genetic elements: The agents of open source evolution. Nat. Rev. Microbiol. 2005, 3, 722–732. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, S.; Datta, S.; Roy, S.; Ramanan, L.; Saha, A.; Viswanathan, R.; Som, T. Carbapenem Resistance in Acinetobacter baumannii and Other Acinetobacter spp. causing neonatal sepsis: Focus on NDM-1 and Its Linkage to ISAba125. Front. Microbiol. 2016, 7, 1126. [Google Scholar] [CrossRef] [PubMed]
- González, L.J.; Bahr, G.; Nakashige, T.G.; Nolan, E.M.; Bonomo, R.A.; Vila, A.J. Membrane anchoring stabilizes and favors secretion of New Delhi metallo-β-lactamase. Nat. Chem. Biol. 2016, 12, 516–522. [Google Scholar] [CrossRef]
- Bahr, G.; Vitor-Horen, L.; Bethel, C.R.; Bonomo, R.A.; González, L.J.; Vila, A.J. Clinical Evolution of New Delhi Metallo-β-Lactamase (NDM) Optimizes resistance under Zn(II) deprivation. Antimicrob. Agents Chemother. 2017, 62, e01849–e01917. [Google Scholar] [CrossRef]
- Fuursted, K.; Schøler, L.; Hansen, F.; Dam, K.; Bojer, M.S.; Hammerum, A.M.; Dagnæs-Hansen, F.; Olsen, A.; Jasemian, Y.; Struve, C. Virulence of a Klebsiella pneumoniae strain carrying the New Delhi metallo-β-lactamase-1 (NDM-1). Microbes Infect. 2012, 14, 155–158. [Google Scholar] [CrossRef]
- Martin, R.M.; Cao, J.; Wu, W.; Zhao, L.; Manthei, D.M.; Pirani, A.; Snitkin, E.; Malani, P.N.; Rao, K.; Bachman, M.A. Identification of pathogenicity-associated loci in Klebsiella pneumoniae from hospitalized patients. Msystems 2018, 3, e00015–e00018. [Google Scholar] [CrossRef]
- Paczosa, M.K.; Mecsas, J. Klebsiella pneumoniae: Going on the offense with a strong defense. Microbiol. Mol. Biol. Rev. 2016, 80, 629–661. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.J.; Lin, T.L.; Chen, C.T.; Chen, Y.Y.; Hsieh, P.F.; Hsu, C.R.; Wu, M.C.; Wang, J.T. Genetic analysis of capsular polysaccharide synthesis gene clusters in 79 capsular types of Klebsiella spp. Sci. Rep. 2015, 5, 15573. [Google Scholar] [CrossRef]
- Walker, K.A.; Miner, T.A.; Palacios, M.; Trzilova, D.; Frederick, D.R.; Broberg, C.A.; Sepúlveda, V.E.; Quinn, J.D.; Miller, V.L. Klebsiella pneumoniae regulatory mutant has reduced capsule expression but retains hypermucoviscosity. MBio 2019, 26, e00089–e00119. [Google Scholar] [CrossRef] [PubMed]
- Wacharotayankun, R.; Arakawa, Y.; Ohta, M.; Tanaka, K.; Akashi, T.; Mori, M.; Kato, N. Enhancement of extracapsular polysaccharide synthesis in Klebsiella pneumoniae by RmpA2, which shows homology to NtrC and FixJ. Infect. Immun. 1993, 61, 3164–3174. [Google Scholar] [CrossRef] [PubMed]
- NCBI Pathogen Detection Reference Gene Catalog. BlaNDM. Available online: http://www.ncbi.nlm.nih.gov/pathogens/isolates#/refgene/blaNDM (accessed on 20 June 2020).
- Baraniak, A.; Izdebski, R.; Fiett, J.; Gawryszewska, I.; Bojarska, K.; Herda, M.; Literacka, E.; Żabicka, D.; Tomczak, H.; Pewińska, N.; et al. NDM-producing Enterobacteriaceae in Poland, 2012-14: Inter-regional outbreak of Klebsiella pneumoniae ST11 and sporadic cases. J. Antimicrob. Chemother. 2016, 71, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Navon-Venezia, S.; Kondratyeva, K.; Carattoli, A. Klebsiella pneumoniae: A major worldwide source and shuttle for antibiotic resistance. FEMS Microbiol. Rev. 2017, 41, 252–275. [Google Scholar] [CrossRef] [PubMed]
- Moubareck, C.A.; Mouftah, S.F.; Pál, T.; Ghazawi, A.; Halat, D.H.; Nabi, A.; AlSharhan, M.A.; AlDeesi, Z.O.; Peters, C.C.; Celiloglu, H.; et al. Clonal emergence of Klebsiella pneumoniae ST14 co-producing OXA-48-type and NDM carbapenemases with high rate of colistin resistance in Dubai, United Arab Emirates. Int. J. Antimicrob. Agents 2018, 52, 90–95. [Google Scholar] [CrossRef]
- Chen, L.; Mathema, B.; Chavda, K.D.; DeLeo, F.R.; Bonomo, R.A.; Kreiswirth, B.N. Carbapenemase-producing Klebsiella pneumoniae: Molecular and genetic decoding. Trends Microbiol. 2014, 22, 686–696. [Google Scholar] [CrossRef] [PubMed]
- Giske, C.G.; Fröding, I.; Hasan, C.M.; Turlej-Rogacka, A.; Toleman, M.; Livermore, D.; Woodford, N.; Walsh, T.R. Diverse sequence types of Klebsiella pneumoniae contribute to the dissemination of blaNDM-1 in India, Sweden, and the United Kingdom. Antimicrob. Agents Chemother. 2012, 56, 2735–2738. [Google Scholar] [CrossRef] [PubMed]
- Baraniak, A.; Machulska, M.; Żabicka, D.; Literacka, E.; Izdebski, R.; Urbanowicz, P.; Bojarska, K.; Herda, M.; Kozińska, A.; Hryniewicz, W.; et al. Towards endemicity: Large-scale expansion of the NDM-1-producing Klebsiella pneumoniae ST11 lineage in Poland, 2015-16. J. Antimicrob. Chemother. 2019, 74, 3199–3204. [Google Scholar] [CrossRef] [PubMed]
- Żabicka, D.; Bojarska, K.; Herda, M.; Literacka, E.; Kozińska, A.; Hryniewicz, W.; Skoczyńska, A.; Baraniak, A.; Machulska, M.; Urbanowicz, P.; et al. Pałeczki Jelitowe Enterobacteriaceae Wytwarzające Karbapenemazy (CPE) w Polsce-Sytuacja w 2016. Krajowy Ośrodek Referencyjny ds. Lekowrażliwości Drobnoustrojów. Available online: http://www.korld.edu.pl/pdf/CPEraport2016.pdf (accessed on 25 November 2017).
- Żabicka, D.; Literacka, E.; Gniadkowski, M.; Hryniewicz, W. Raport Krajowego Ośrod-ka Referencyjnego ds. Lekowrażliwości Drobnoustrojów. Występowanie Entero- bacteriaceae (głównie Klebsiella pneumoniae), wytwarzających karbapenemazę New Delhi (NDM) na terenie Polski w okresie I–III kwartał 2017 roku. KORLD. Available online: http://www.korld.edu.pl/pdf/Raport_NDM_18-12-2017 (accessed on 20 December 2017).
- Karuthu, S.; Blumberg, E.A. Common infections in kidney transplant recipients. Clin. J. Am. Soc. Nephrol. 2012, 7, 2058–2070. [Google Scholar] [CrossRef]
- Ko, K.S.; Cho, D.O.; Ahn, J.H.; Lee, T.W.; Ihm, C.G.; Chang, S.G.; Chai, S.E.; Park, H.C.; Hong, S.H.; Joo, H.Z.; et al. Infections after renal transplantation. Transplant. Proc. 1994, 26, 2072–2074. [Google Scholar] [PubMed]
- Säemann, M.; Hörl, W.H. Urinary tract infection in renal transplant recipients. Eur. J. Clin. Invest 2008, 38 (Suppl. S2), 58–65. [Google Scholar] [CrossRef]
- Vidal, E.; Torre-Cisneros, J.; Blanes, M.; Montejo, M.; Cervera, C.; Aguado, J.M.; Len, O.; Carratalá, J.; Cordero, E.; Bou, G.; et al. Bacterial urinary tract infection after solid organ transplantation in the RESITRA cohort. Transpl. Infect. Dis. 2012, 14, 595–603. [Google Scholar] [CrossRef]
- Izdebski, R.; Sitkiewicz, M.; Urbanowicz, P.; Krawczyk, M.; Brisse, S.; Gniadkowski, M. Genomic background of the Klebsiella pneumoniae NDM-1 outbreak in Poland, 2012–18. J. Antimicrob. Chemother. 2020, 75, 3156–3162. [Google Scholar] [CrossRef] [PubMed]
- Bolger, A.M.; Lohse, M.; Usadel, B. Trimmomatic: A flexible trimmer for Illumina sequence data. Bioinformatics 2014, 30, 2114–2120. [Google Scholar] [CrossRef]
- Nordmann, P.; Poirel, L.; Carrër, A.; Toleman, M.A.; Walsh, T.R. How to detect NDM-1 producers. J. Clin. Microbiol. 2011, 49, 718–721. [Google Scholar] [CrossRef]
- Stojowska, K.; Kałuzewski, S.; Krawczyk, B. Usefulness of PCR melting profile method for genotyping analysis of Klebsiella oxytoca isolates from patients of a single hospital unit. Pol. J. Microbiol. 2009, 58, 247–253. [Google Scholar]
- Gołębiewska, J.E.; Krawczyk, B.; Wysocka, M.; Ewiak, A.; Komarnicka, J.; Bronk, M.; Rutkowski, B.; Dębska-Ślizień, A. Host and pathogen factors in Klebsiella pneumoniae upper urinary tract infections in renal transplant patients. J. Med. Microbiol. 2019, 68, 382–394. [Google Scholar] [CrossRef] [PubMed]
- Nurk, S.; Bankevich, A.; Antipov, D.; Gurevich, A.; Korobeynikov, A.; Lapidus, A.; Prjibelsky, A.; Pyshkin, A.; Sirotkin, A.; Sirotkin, Y.; et al. Assembling genomes and mini-metagenomes from highly chimeric reads. In Research in Computational Molecular Biology. RECOMB 2013. Lecture Notes in Computer Science; Deng, M., Jiang, R., Sun, F., Zhang, X., Eds.; Springer: Berlin/Heidelberg, Germany, 2013; Volume 7821, pp. 158–170. [Google Scholar]
- Mikheenko, A.; Prjibelski, A.; Saveliev, V.; Antipov, D.; Gurevich, A. Versatile genome assembly evaluation with QUAST-LG. Bioinformatics 2018, 34, i142–i150. [Google Scholar] [CrossRef] [PubMed]
- Seemann, T. Prokka: Rapid prokaryotic genome annotation. Bioinformatics 2014, 30, 2068–2069. [Google Scholar] [CrossRef] [PubMed]
- Page, A.J.; Cummins, C.A.; Hunt, M.; Wong, V.K.; Reuter, S.; Holden, M.T.; Fookes, M.; Falush, D.; Keane, J.A.; Parkhill, J. Roary: Rapid large-scale prokaryote pan genome analysis. Bioinformatics 2015, 31, 3691–3693. [Google Scholar] [CrossRef]
- Edgar, R.C. MUSCLE: Multiple sequence alignment with high accuracy and high throughput. Nucleic Acids Res. 2004, 32, 1792–1797. [Google Scholar] [CrossRef]
- Stamatakis, A. RAxML version 8: A tool for phylogenetic analysis and post-analysis of large phylogenies. Bioinformatics 2014, 30, 1312–1313. [Google Scholar] [CrossRef]
- Yu, G.; Smith, D.K.; Zhu, H.; Guan, Y.; Lam, T. Ggtree: An R package for visualization and annotation of phylogenetic trees with their covariates and other associated data. Methods Ecol. Evol. 2017, 8, 28–36. [Google Scholar] [CrossRef]
- Tonkin-Hill, G.; Lees, J.A.; Bentley, S.D.; Frost, S.D.W.; Corander, J. RhierBAPS: An R implementation of the population clustering algorithm hierBAPS. Wellcome Open Res. 2018, 3, 93. [Google Scholar] [CrossRef]
- MLST. Available online: https://github.com/tseemann/mlst (accessed on 25 June 2020).
- Snippy, Rapid Haploid Variant Calling and Core Genome Alignment. Available online: https://github.com/tseemann/snippy (accessed on 25 June 2020).
- SnpEff. Genomic Variant Annotations and Functional Effect Prediction Toolbox. Available online: http://snpeff.sourceforge.net (accessed on 25 June 2020).
- Zankari, E.; Hasman, H.; Cosentino, S.; Vestergaard, M.; Rasmussen, S.; Lund, O.; Aarestrup, F.M.; Larsen, M.V. Identification of acquired antimicrobial resistance genes. J. Antimicrob. Chemother. 2012, 67, 2640–2644. [Google Scholar] [CrossRef]
- Jolley, K.A.; Bray, J.E.; Maiden, M.C.J. Open-access bacterial population genomics: BIGSdb software, the PubMLST.org website and their applications. Wellcome Open Res. 2018, 3, 124. [Google Scholar] [CrossRef]
- Wick, R.R.; Heinz, E.; Holt, K.E.; Wyres, K.L. Kaptive Web: User-friendly capsule and lipopolysaccharide serotype prediction for Klebsiella genomes. BioRxiv 2018, 56, e00197–e00218. [Google Scholar] [CrossRef]
- Carattoli, A.; Zankari, E.; García-Fernández, A.; Voldby Larsen, M.; Lund, O.; Villa, L.; Møller Aarestrup, F.; Hasman, H. In silico detection and typing of plasmids using PlasmidFinder and plasmid multilocus sequence typing. Antimicrob. Agents Chemother. 2014, 58, 3895–3903. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing. 2018. Available online: http://www.R-project.org/ (accessed on 19 July 2021).
- Farzand, R.; Rajakumar, K.; Zamudio, R.; Oggioni, M.R.; Barer, M.R.; O’Hare, H.M. ICEKp2: Description of an integrative and conjugative element in Klebsiella pneumoniae, co-occurring and interacting with ICEKp1. Sci. Rep. 2019, 9, 13892. [Google Scholar] [CrossRef]
- RFPlasmid. Available online: https://github.com/aldertzomer/RFPlasmid (accessed on 25 June 2020).
- Ko, K.S. The contribution of capsule polysaccharide genes to virulence of Klebsiella pneumoniae. Virulence 2017, 8, 485–486. [Google Scholar] [CrossRef]
- Cheng, H.Y.; Chen, Y.S.; Wu, C.Y.; Chang, H.Y.; Lai, Y.C.; Peng, H.L. RmpA regulation of capsular polysaccharide biosynthesis in Klebsiella pneumoniae CG43. J. Bacteriol. 2010, 192, 3144–3158. [Google Scholar] [CrossRef]
- El Fertas-Aissani, R.; Messai, Y.; Alouache, S.; Bakour, R. Virulence profiles and antibiotic susceptibility patterns of Klebsiella pneumoniae strains isolated from different clinical specimens. Pathol. Biol. 2013, 61, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Gołębiewska, J.; Dębska-Ślizień, A.; Komarnicka, J.; Samet, A.; Rutkowski, B. Urinary tract infections in renal transplant recipients. Transplant. Proc. 2011, 43, 2985–2990. [Google Scholar] [CrossRef] [PubMed]
- Munoz-Price, L.S.; Poirel, L.; Bonomo, R.A.; Schwaber, M.J.; Daikos, G.L.; Cormican, M.; Cornaglia, G.; Garau, J.; Gniadkowski, M.; Hayden, M.K.; et al. Clinical epidemiology of the global expansion of Klebsiella pneumoniae carbapenemases. Lancet Infect. Dis. 2013, 13, 785–796. [Google Scholar] [CrossRef]
- Taglietti, F.; Di Bella, S.; Galati, V.; Topino, S.; Iappelli, M.; Petrosillo, N. Carbapenemase-producing Klebsiella pneumoniae-related mortality among solid organ-transplanted patients: Do we know enough? Transpl. Infect. Dis. 2013, 15, E164–E165. [Google Scholar] [CrossRef]
- Wilkowski, P.; Ciszek, M.; Dobrzaniecka, K.; Sańko-Resmer, J.; Łabuś, A.; Grygiel, K.; Grochowiecki, T.; Młynarczyk, G.; Pączek, L. Successful treatment of urinary tract infection in kidney transplant recipients caused by multiresistant Klebsiella pneumoniae producing New Delhi metallo-β-lactamase (NDM-1) with strains genotyping. Transplant. Proc. 2016, 48, 1576–1579. [Google Scholar] [CrossRef]
- Linares, L.; Cervera, C.; Hoyo, I.; Sanclemente, G.; Marco, F.; Cofán, F.; Ricart, M.J.; Navasa, M.; Moreno, A. Klebsiella pneumoniae infection in solid organ transplant recipients: Epidemiology and antibiotic resistance. Transplant. Proc. 2010, 42, 2941–2943. [Google Scholar] [CrossRef]
- Zdziarski, J.; Brzuszkiewicz, E.; Wullt, B.; Liesegang, H.; Biran, D.; Voigt, B.; Grönberg-Hernandez, J.; Ragnarsdottir, B.; Hecker, M.; Ron, E.Z.; et al. Host imprints on bacterial genomes--rapid, divergent evolution in individual patients. PLoS Pathog. 2010, 6, e1001078. [Google Scholar] [CrossRef] [PubMed]
- Stork, C.; Kovács, B.; Rózsai, B.; Putze, J.; Kiel, M.; Dorn, Á.; Kovács, J.; Melegh, S.; Leimbach, A.; Kovács, T.; et al. Characterization of asymptomatic bacteriuria Escherichia coli isolates in search of alternative strains for efficient bacterial interference against uropathogens. Front. Microbiol. 2018, 9, 214. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.; Feng, Y.; Tang, G.; Qiao, F.; McNally, A.; Zong, Z. NDM metallo-β-lactamases and their bacterial producers in Health Care Settings. Clin. Microbiol. Rev. 2019, 32, e00115–e00118. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Liu, Y.; Wang, R.; Wang, Q.; Jin, L.; Wang, H. The transferability and evolution of NDM-1 and KPC-2 co-producing Klebsiella pneumoniae from clinical settings. EBioMedicine 2020, 51, 102599. [Google Scholar] [CrossRef] [PubMed]
- Joseph, L.; Merciecca, T.; Forestier, C.; Balestrino, D.; Miquel, S. From Klebsiella pneumoniae Colonization to Dissemination: An Overview of Studies Implementing Murine Models. Microorganisms 2021, 9, 1282. [Google Scholar] [CrossRef] [PubMed]
- Hammerum, A.M.; Toleman, M.A.; Hansen, F.; Kristensen, B.; Lester, C.H.; Walsh, T.R.; Fuursted, K. Global spread of New Delhi metallo-β-lactamase 1. Lancet Infect. Dis. 2010, 10, 829–830. [Google Scholar] [CrossRef]
- Bonomo, R.A. New Delhi metallo-β-lactamase and multidrug resistance: A global SOS? Clin. Infect. Dis. 2011, 52, 485–487. [Google Scholar] [CrossRef][Green Version]
- Pitout, J.D.; Nordmann, P.; Poirel, L. Carbapenemase-producing Klebsiella pneumoniae, a key pathogen set for global nosocomial dominance. Antimicrob. Agents Chemother. 2015, 59, 5873–5884. [Google Scholar] [CrossRef]
- Ruppé, E.; Armand-Lefèvre, L.; Estellat, C.; El-Mniai, A.; Boussadia, Y.; Consigny, P.H.; Girard, P.M.; Vittecoq, D.; Bouchaud, O.; Pialoux, G.; et al. Acquisition of carbapenemase-producing Enterobacteriaceae by healthy travellers to India, France, February 2012 to March 2013. Eurosurveillance 2014, 19, 20768. [Google Scholar] [CrossRef]
- Fiett, J.; Baraniak, A.; Izdebski, R.; Sitkiewicz, I.; Żabicka, D.; Meler, A.; Filczak, K.; Hryniewicz, W.; Gniadkowski, M. The first NDM metallo-β-lactamase-producing Enterobacteriaceae isolate in Poland: Evolution of IncFII-type plasmids carrying the bla(NDM-1) gene. Antimicrob. Agents Chemother. 2014, 58, 1203–1207. [Google Scholar] [CrossRef]
- Izdebski, R.; Bojarska, K.; Baraniak, A.; Literacka, E.; Herda, M.; Żabicka, D.; Guzek, A.; Półgrabia, M.; Hryniewicz, W.; Gniadkowski, M. NDM-1- or OXA-48-producing Enterobacteriaceae colonising Polish tourists following a terrorist attack in Tunis, March 2015. Eurosurveillance 2015, 20, 21150. [Google Scholar] [CrossRef]
- Clegg, S.; Murphy, C.N. Epidemiology and virulence of Klebsiella pneumoniae. Microbiol. Spectr. 2016, 4. [Google Scholar] [CrossRef]
- Wysocka, M.; Zamudio, R.; Oggioni, M.R.; Gołębiewska, J.; Dudziak, A.; Krawczyk, B. The new Klebsiella pneumoniae ST152 variants with hypermucoviscous phenotype isolated from renal transplant recipients with asymptomatic bacteriuria-genetic characteristics by WGS. Genes 2020, 11, 1189. [Google Scholar] [CrossRef]
- Schroll, C.; Barken, K.B.; Krogfelt, K.A.; Struve, C. Role of type 1 and type 3 fimbriae in Klebsiella pneumoniae biofilm formation. BMC Microbiol. 2010, 10, 179. [Google Scholar] [CrossRef] [PubMed]
- Alcántar-Curiel, M.D.; Blackburn, D.; Saldaña, Z.; Gayosso-Vázquez, C.; Iovine, N.; De la Cruz, M.A.; Girón, J.A. Multi-functional analysis of Klebsiella pneumoniae fimbrial types in adherence and biofilm formation. Virulence 2013, 4, 129–138. [Google Scholar] [CrossRef]
- Phillips, P.L.; Schultz, G.S. Molecular Mechanisms of Biofilm Infection: Biofilm Virulence Factors. Adv. Wound Care 2012, 1, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Lawlor, M.S.; O’connor, C.; Miller, V.L. Yersiniabactin is a virulence factor for Klebsiella pneumoniae during pulmonary infection. Infect. Immun. 2007, 75, 1463–1472. [Google Scholar] [CrossRef] [PubMed]
- Bachman, M.A.; Oyler, J.E.; Burns, S.H.; Caza, M.; Lépine, F.; Dozois, C.M.; Weiser, J.N. Klebsiella pneumoniae yersiniabactin promotes respiratory tract infection through evasion of lipocalin 2. Infect. Immun. 2011, 79, 3309–3316. [Google Scholar] [CrossRef]
- Holt, K.E.; Wertheim, H.; Zadoks, R.N.; Baker, S.; Whitehouse, C.A.; Dance, D.; Jenney, A.; Connor, T.R.; Hsu, L.Y.; Severin, J.; et al. Genomic analysis of diversity, population structure, virulence, and antimicrobial resistance in Klebsiella pneumoniae, an urgent threat to public health. Proc. Natl. Acad. Sci. USA 2015, 112, E3574–E3581. [Google Scholar] [CrossRef] [PubMed]
- Hancock, V.; Klemm, P. Global gene expression profiling of asymptomatic bacteriuria Escherichia coli during biofilm growth in human urine. Infect. Immun. 2007, 75, 966–976. [Google Scholar] [CrossRef] [PubMed]
- Marques, C.; Menezes, J.; Belas, A.; Aboim, C.; Cavaco-Silva, P.; Trigueiro, G.; Gama, L.T.; Pomba, C. Klebsiella pneumoniae causing urinary tract infections in companion animals and humans: Population structure, antimicrobial resistance and virulence genes. J. Antimicrob. Chemother. 2019, 74, 594–602. [Google Scholar] [CrossRef]
- Aguirre-Quiñonero, A.; Martínez-Martínez, L. Non-molecular detection of carbapenemases in Enterobacteriaceae clinical isolates. J. Infect. Chemother. 2017, 23, 1–11. [Google Scholar] [CrossRef][Green Version]
- Xie, L.; Dou, Y.; Zhou, K.; Chen, Y.; Han, L.; Guo, X.; Sun, J. Coexistence of blaOXA-48 and truncated blaNDM-1 on different plasmids in a Klebsiella pneumoniae isolate in China. Front. Microbiol. 2017, 8, 133. [Google Scholar] [CrossRef] [PubMed]
- Sidjabat, H.E.; Townell, N.; Nimmo, G.R.; George, N.M.; Robson, J.; Vohra, R.; Davis, L.; Heney, C.; Paterson, D.L. Dominance of IMP-4-producing Enterobacter cloacae among carbapenemase-producing Enterobacteriaceae in Australia. Antimicrob. Agents Chemother. 2015, 59, 4059–4066. [Google Scholar] [CrossRef]
- Poirel, L.; Dortet, L.; Bernabeu, S.; Nordmann, P. Genetic features of blaNDM-1-positive Enterobacteriaceae. Antimicrob. Agents Chemother. 2011, 55, 5403–5407. [Google Scholar] [CrossRef] [PubMed]
- Rolain, J.M.; Parola, P.; Cornaglia, G. New Delhi metallo-β-lactamase (NDM-1): Towards a new pandemia? Clin. Microbiol. Infect. 2010, 16, 1699–1701. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).