
From Genotype to Phenotype—A Review of Kabuki Syndrome †

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Literature Search
3.2. Demographics
3.3. Genotype
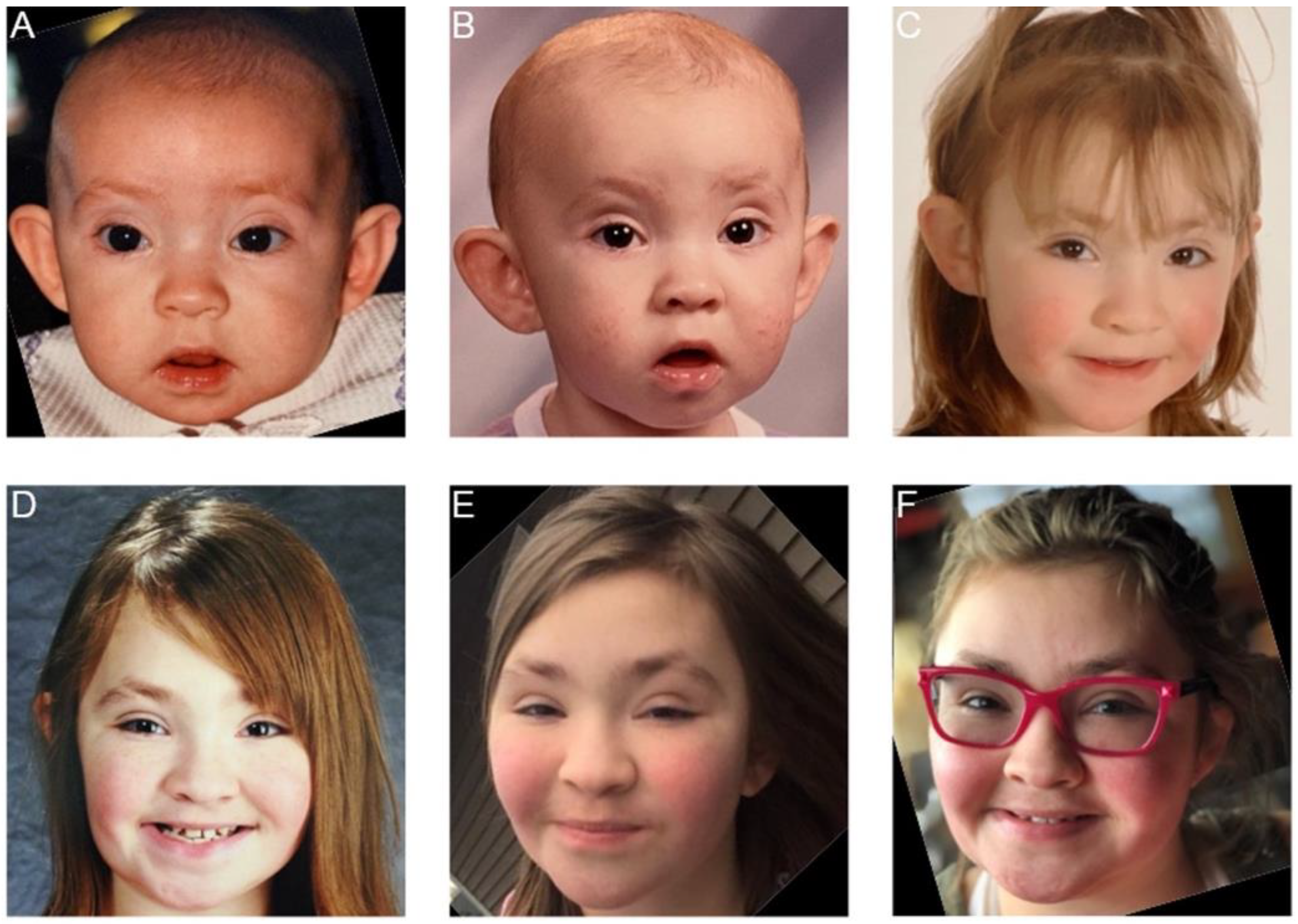
3.4. Facial Gestalt
3.5. Congenital Heart Defects
3.6. Immunologic Profile
3.7. Brain and Neurologic Manifestations
3.8. Cancer
3.9. Endocrinopathies
3.10. Genitourinary Anomalies
3.11. Ophthalmologic Abnormalities
3.12. Gastrointestinal Involvement
3.13. Reproductive Health
3.14. Prenatal and Perinatal History
3.15. Growth and Feeding
3.16. Language and Development
3.17. Cognitive Profile
3.18. Communication, Speech, and Language
3.19. Behavioral Phenotype
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Niikawa, N.; Matsuura, N.; Fukushima, Y.; Ohsawa, T.; Kajii, T. Kabuki make-up syndrome: A syndrome of mental retardation, unusual facies, large and protruding ears, and postnatal growth deficiency. J. Pediatr. 1981, 99, 565–569. [Google Scholar] [CrossRef]
- Kuroki, Y.; Suzuki, Y.; Chyo, H. A new malformation syndrome of long palpebral fissures, large ears, depressed nasal tip, and skeletal anomalies associated with postnatal dwarfism and mental retardation. J. Pediatr. 1981, 99, 570–573. [Google Scholar] [CrossRef]
- Adam, M.P.; Hudgins, L. Kabuki syndrome: A review. Clin. Genet. 2005, 67, 209–219. [Google Scholar] [CrossRef]
- Bogershausen, N.; Gatinois, V.; Riehmer, V.; Kayserili, H.; Becker, J.; Thoenes, M.; Simsek-Kiper, P.O.; Barat-Houari, M.; Elcioglu, N.H.; Wieczorek, D.; et al. Mutation Update for Kabuki Syndrome Genes KMT2D and KDM6A and Further Delineation of X-Linked Kabuki Syndrome Subtype 2. Hum. Mutat. 2016, 37, 847–864. [Google Scholar] [CrossRef] [PubMed]
- Niikawa, N.; Kuroki, Y.; Kajii, T.; Matsuura, N.; Ishikiriyama, S.; Tonoki, H.; Ishikawa, N.; Yamada, Y.; Fujita, M.; Umemoto, H.; et al. Kabuki make-up (Niikawa-Kuroki) syndrome: A study of 62 patients. Am. J. Med. Genet. 1988, 31, 565–589. [Google Scholar] [CrossRef]
- White, S.M.; Thompson, E.M.; Kidd, A.; Savarirayan, R.; Turner, A.; Amor, D.; Delatycki, M.B.; Fahey, M.; Baxendale, A.; White, S.; et al. Growth, behavior, and clinical findings in 27 patients with Kabuki (Niikawa-Kuroki) syndrome. Am. J. Med. Genet. Part A 2004, 127A, 118–127. [Google Scholar] [CrossRef] [PubMed]
- Digilio, M.C.; Gnazzo, M.; Lepri, F.; Dentici, M.L.; Pisaneschi, E.; Baban, A.; Passarelli, C.; Capolino, R.; Angioni, A.; Novelli, A.; et al. Congenital heart defects in molecularly proven Kabuki syndrome patients. Am. J. Med. Genet. Part A 2017, 173, 2912–2922. [Google Scholar] [CrossRef] [PubMed]
- Adam, M.P.; Banka, S.; Bjornsson, H.T.; Bodamer, O.; Chudley, A.E.; Harris, J.; Kawame, H.; Lanpher, B.C.; Lindsley, A.W.; Merla, G.; et al. Kabuki syndrome: International consensus diagnostic criteria. J. Med. Genet. 2019, 56, 89–95. [Google Scholar] [CrossRef]
- Ng, S.B.; Bigham, A.W.; Buckingham, K.J.; Hannibal, M.C.; McMillin, M.J.; Gildersleeve, H.I.; Beck, A.E.; Tabor, H.K.; Cooper, G.M.; Mefford, H.C.; et al. Exome sequencing identifies MLL2 mutations as a cause of Kabuki syndrome. Nat Genet. 2010, 42, 790–793. [Google Scholar] [CrossRef]
- Lederer, D.; Grisart, B.; Digilio, M.C.; Benoit, V.; Crespin, M.; Ghariani, S.C.; Maystadt, I.; Dallapiccola, B.; Verellen-Dumoulin, C. Deletion of KDM6A, a histone demethylase interacting with MLL2, in three patients with kabuki syndrome. Am. J. Hum. Genet. 2012, 90, 119–124. [Google Scholar] [CrossRef]
- Paděrová, J.; Holubová, A.; Simandlová, M.; Puchmajerová, A.; Vlčková, M.; Malíková, M.; Pourová, R.; Vejvalková, S.; Havlovicová, M.; Šenkeříková, M.; et al. Molecular genetic analysis in 14 Czech Kabuki syndrome patients is confirming the utility of phenotypic scoring. Clin. Genet. 2016, 90, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Banka, S.; Lederer, D.; Benoit, V.; Jenkins, E.; Howard, E.; Bunstone, S.; Kerr, B.; McKee, S.; Lloyd, I.C.; Shears, D.; et al. Novel KDM6A (UTX) mutations and a clinical and molecular review of the X-linked Kabuki syndrome (KS2). Clin. Genet. 2015, 87, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Bögershausen, N.; Wollnik, B. Unmasking Kabuki syndrome. Clin. Genet. 2013, 83, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Lange, L.; Pagnamenta, A.T.; Lise, S.; Clasper, S.; Stewart, H.; Akha, E.S.; Quaghebeur, G.; Knight, S.J.L.; Keays, D.A.; Taylor, J.C.; et al. A de novo frameshift in HNRNPK causing a Kabuki-like syndrome with nodular heterotopia. Clin. Genet. 2016, 90, 258–262. [Google Scholar] [CrossRef]
- Bögershausen, N.; Tsai, I.C.; Pohl, E.; Simsek Kiper, P.Ö.; Beleggia, F.; Percin, F.E.; Keupp, K.; Matchan, A.; Milz, E.; Alanay, Y.; et al. Spotlight on the pathogenesis of Kabuki syndrome. Med. Genet. 2015, 27, 84. [Google Scholar]
- Carapito, R.; Ivanova, E.L.; Morlon, A.; Meng, L.; Molitor, A.; Erdmann, E.; Kieffer, B.; Pichot, A.; Naegely, L.; Kolmer, A.; et al. ZMIZ1 Variants Cause a Syndromic Neurodevelopmental Disorder. Am. J. Hum. Genet. 2019, 104, 319–330. [Google Scholar] [CrossRef]
- Caciolo, C.; Alfieri, P.; Piccini, G.; Digilio, M.C.; Lepri, F.R.; Tartaglia, M.; Menghini, D.; Vicari, S. Neurobehavioral features in individuals with Kabuki syndrome. Mol. Genet. Genomic Med. 2018, 6, 322–331. [Google Scholar] [CrossRef]
- Yap, K.L.; Johnson, A.E.K.; Fischer, D.; Kandikatla, P.; Deml, J.; Nelakuditi, V.; Halbach, S.; Jeha, G.S.; Burrage, L.C.; Bodamer, O.; et al. Congenital hyperinsulinism as the presenting feature of Kabuki syndrome: Clinical and molecular characterization of 10 affected individuals. Gen. Med. 2019, 21, 233–242. [Google Scholar] [CrossRef]
- Margot, H.; Geneviève, D.; Gatinois, V.; Arveiler, B.; Moutton, S.; Touitou, I.; Lacombe, D. Typical facial gestalt in X-linked Kabuki syndrome. Am. J. Med. Genet. Part A 2016, 170, 3363–3364. [Google Scholar] [CrossRef]
- Hannibal, M.C.; Buckingham, K.J.; Ng, S.B.; Ming, J.E.; Beck, A.E.; McMillin, M.J.; Gildersleeve, H.I.; Bigham, A.W.; Tabor, H.K.; Mefford, H.C.; et al. Spectrum of MLL2 (ALR) mutations in 110 cases of Kabuki syndrome. Am. J. Med. Genet. Part A 2011, 155, 1511–1516. [Google Scholar] [CrossRef]
- Lederer, D.; Shears, D.; Benoit, V.; Verellen-Dumoulin, C.; Maystadt, I. A three generation X-linked family with Kabuki syndrome phenotype and a frameshift mutation in KDM6A. Am. J. Med. Genet. Part A 2014, 164, 1289–1292. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Lee, C.G. Coinheritance of novel mutations in SCN1A causing gefs+ and in KDM6A causing kabuki syndrome in a family. Ann. Clin. Lab. Sci. 2017, 47, 229–235. [Google Scholar] [PubMed]
- Faundes, V.; Goh, S.; Akilapa, R.; Bezuidenhout, H.; Bjornsson, H.T.; Bradley, L.; Brady, A.F.; Brischoux-Boucher, E.; Brunner, H.; Bulk, S.; et al. Clinical delineation, sex differences, and genotype–phenotype correlation in pathogenic KDM6A variants causing X-linked Kabuki syndrome type 2. Gen. Med. 2021, 23, 1202–1210. [Google Scholar] [CrossRef] [PubMed]
- Murakami, H.; Tsurusaki, Y.; Enomoto, K.; Kuroda, Y.; Yokoi, T.; Furuya, N.; Yoshihashi, H.; Minatogawa, M.; Abe-Hatano, C.; Ohashi, I.; et al. Update of the genotype and phenotype of KMT2D and KDM6A by genetic screening of 100 patients with clinically suspected Kabuki syndrome. Am. J. Med. Genet. Part A 2020, 182, 2333–2344. [Google Scholar] [CrossRef] [PubMed]
- Lepri, F.R.; Cocciadiferro, D.; Augello, B.; Alfieri, P.; Pes, V.; Vancini, A.; Caciolo, C.; Squeo, G.M.; Malerba, N.; Adipietro, I.; et al. Clinical and neurobehavioral features of three novel kabuki syndrome patients with mosaic KMT2D mutations and a review of literature. Int. J. Mol. Sci. 2018, 19, 82. [Google Scholar] [CrossRef]
- Cuvertino, S.; Hartill, V.; Colyer, A.; Garner, T.; Nair, N.; Al-Gazali, L.; Canham, N.; Faundes, V.; Flinter, F.; Hertecant, J.; et al. A restricted spectrum of missense KMT2D variants cause a multiple malformations disorder distinct from Kabuki syndrome. Gen. Med. 2020, 22, 867–877. [Google Scholar] [CrossRef]
- Baldridge, D.; Spillmann, R.C.; Wegner, D.J.; Wambach, J.A.; White, F.V.; Sisco, K.; Toler, T.L.; Dickson, P.I.; Cole, F.S.; Shashi, V.; et al. Phenotypic expansion of KMT2D-related disorder: Beyond Kabuki syndrome. Am. J. Med. Genet. Part A 2020, 182, 1053–1065. [Google Scholar] [CrossRef]
- Tekendo-Ngongang, C.; Kruszka, P.; Martinez, A.F.; Muenke, M. Novel heterozygous variants in KMT2D associated with holoprosencephaly. Clin Genet. 2019, 96, 266–270. [Google Scholar] [CrossRef]
- Sakaria, R.P.; Zaveri, P.G.; Holtrop, S.; Zhang, J.; Brown, C.W.; Pivnick, E.K. Case Report: An Infant With Kabuki Syndrome, Alobar Holoprosencephaly and Truncus Arteriosus: A Case for Whole Exome Sequencing in Neonates With Congenital Anomalies. Front Genet. 2021, 12, 766316. [Google Scholar] [CrossRef]
- Froimchuk, E.; Jang, Y.; Ge, K. Histone H3 lysine 4 methyltransferase KMT2D. Gene 2017, 627, 337–342. [Google Scholar] [CrossRef]
- Aref-Eshghi, E.; Schenkel, L.C.; Lin, H.; Skinner, C.; Ainsworth, P.; Pare, G.; Rodenhiser, D.; Schwartz, C.; Sadikovic, B. The defining DNA methylation signature of Kabuki syndrome enables functional assessment of genetic variants of unknown clinical significance. Epigenetics 2017, 12, 923–933. [Google Scholar] [CrossRef] [PubMed]
- Kokitsu-Nakata, N.M.; Petrin, A.L.; Heard, J.P.; Vendramini-Pittoli, S.; Henkle, L.E.; dos Santos, D.V.C.; Murray, J.C.; Richieri-Costa, A. Analysis of MLL2 gene in the first Brazilian family with Kabuki syndrome. Am. J. Med. Genet. Part A 2012, 158A, 2003–2008. [Google Scholar] [CrossRef] [PubMed]
- Halal, F.; Gledhill, R.; Dudkiewicz, A. Autosomal dominant inheritance of the Kabuki make-up (Niikawa-Kuroki) syndrome. Am. J. Med. Genet. 1989, 33, 376–381. [Google Scholar] [CrossRef]
- Galan-Gomez, E.; Cardesa-Garcia, J.J.; Campo-Sampedro, F.M.; Salamanca-Maesso, C.; Martinez-Frias, M.L.; Frias, J.L. Kabuki make-up (Niikawa-Kuroki) syndrome in five Spanish children. Am. J. Med. Genet. 1995, 59, 276–282. [Google Scholar] [CrossRef] [PubMed]
- Frediani, T.; Lucarelli, S.; Bruni, L. Niikawa-Kuroki (Kabuki) syndrome in two siblings. Minerva Pediatr. 2001, 53, 43–48. [Google Scholar]
- Shotelersuk, V.; Punyashthiti, R.; Srivuthana, S.; Wacharasindhu, S. Kabuki syndrome: Report of six Thai children and further phenotypic and genetic delineation. Am. J. Med. Genet. 2002, 110, 384–390. [Google Scholar] [CrossRef]
- Faundes, V.; Malone, G.; Newman, W.G.; Banka, S. A comparative analysis of KMT2D missense variants in Kabuki syndrome, cancers and the general population. J. Hum. Genet. 2018, 64, 161–170. [Google Scholar] [CrossRef]
- Banka, S.; Veeramachaneni, R.; Reardon, W.; Howard, E.; Bunstone, S.; Ragge, N.; Parker, M.J.; Crow, Y.J.; Kerr, B.; Kingston, H.; et al. How genetically heterogeneous is Kabuki syndrome: MLL2 testing in 116 patients, review and analyses of mutation and phenotypic spectrum. Eur. J. Hum. Genet. 2012, 20, 381–388. [Google Scholar] [CrossRef]
- Yuan, S.M. Congenital heart defects in Kabuki syndrome. Cardiol. J. 2013, 20, 121–124. [Google Scholar] [CrossRef]
- Cheon, C.K.; Ko, J.M. Kabuki syndrome: Clinical and molecular characteristics. Korean J. Pediatr. 2015, 58, 317–324. [Google Scholar] [CrossRef]
- Hughes, H.E.; Davies, S.J. Coarctation of the aorta in kabuki syndrome. Arch. Dis. Child. 1994, 70, 512–514. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.K.; Ahn, K.J.; Kwon, B.S.; Kim, G.B.; Bae, E.J.; Noh, C.I.; Ko, J.M. The strong association of left-side heart anomalies with Kabuki syndrome. Korean J. Pediatr. 2015, 58, 256–262. [Google Scholar] [CrossRef] [PubMed]
- Digilio, M.C.; Baban, A.; Marino, B.; Dallapiccola, B. Hypoplastic left heart syndrome in patients with kabuki syndrome. Pediatr. Cardiol. 2010, 31, 1111–1113. [Google Scholar] [CrossRef] [PubMed]
- Adam, M. Insights into the molecular genetics of Kabuki syndrome. Adv. Genom. Genet. 2015, 5, 121–129. [Google Scholar] [CrossRef]
- Frenk, N.E.; Kim, C.A.; Carneiro-Sampaio, M.; Orii, N.M.; de Moraes Vasconcelos, D. Basic Evaluation of the immunocompetence of Brazilian patients with Kabuki syndrome. Pediatria 2009, 31, 170–177. [Google Scholar]
- Stagi, S.; Gulino, A.V.; Lapi, E.; Rigante, D. Epigenetic control of the immune system: A lesson from Kabuki syndrome. Immunol. Res. 2016, 64, 345–359. [Google Scholar] [CrossRef]
- Hostoffer, R.W.; Bay, C.A.; Wagner, K.; Venglarcik, I.J.; Sahara, H.; Omair, E.; Clark, H.T. Kabuki make-up syndrome associated with an acquired hypogammaglobulinemia and anti-IgA antibodies. Clin. Pediatr. 1996, 35, 273–276. [Google Scholar] [CrossRef]
- Lindsley, A.W.; Saal, H.M.; Burrow, T.A.; Hopkin, R.J.; Shchelochkov, O.; Khandelwal, P.; Xie, C.; Bleesing, J.; Filipovich, L.; Risma, K.; et al. Defects of B-cell terminal differentiation in patients with type-1 Kabuki syndrome. J. Allergy Clin. Immunol. 2016, 137, 179–187.e10. [Google Scholar] [CrossRef] [PubMed]
- Brackmann, F.; Krumbholz, M.; Langer, T.; Rascher, W.; Holter, W.; Metzler, M. Novel MLL2 mutation in Kabuki syndrome with hypogammaglobulinemia and severe chronic thrombopenia. J. Pediatr. Hematol. Oncol. 2013, 35, e314–e316. [Google Scholar] [CrossRef]
- Pham, M.N.; Byun, M.; Cunningham-Rundles, C. Kabuki syndrome another player on the immunodeficiency stage. J. Clin. Immunol. 2018, 38, 379–380. [Google Scholar] [CrossRef]
- Hoffman, J.D.; Ciprero, K.L.; Sullivan, K.E.; Kaplan, P.B.; McDonald-McGinn, D.M.; Zackai, E.H.; Ming, J.E. Immune abnormalities are a frequent manifestation of Kabuki syndrome. Am. J. Med. Genet. 2005, 135A, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Margot, H.; Boursier, G.; Duflos, C.; Sanchez, E.; Amiel, J.; Andrau, J.C.; Arpin, S.; Brischoux-Boucher, E.; Boute, O.; Burglen, L.; et al. Immunopathological manifestations in Kabuki syndrome: A registry study of 177 individuals. Genet. Med. 2020, 22, 181–188. [Google Scholar] [CrossRef] [PubMed]
- Tekin, M.; Fitoz, S.; Arici, S.; Cetinkaya, E.; Incesulu, A. Niikawa-Kuroki (Kabuki) syndrome with congenital sensorineural deafness: Evidence for a wide spectrum of inner ear abnormalities. Int. J. Pediatr. Otorhinolaryngol. 2006, 70, 885–889. [Google Scholar] [CrossRef] [PubMed]
- Ming, J.E.; Russell, K.L.; McDonald-McGinn, D.M.; Zackai, E.H. Autoimmune disorders in Kabuki syndrome. Am. J. Med. Genet. 2005, 132A, 260–262. [Google Scholar] [CrossRef]
- Almecija, A.C.; Perez, V.; Baro, M.; Guerra-Garcia, P.; Vivanco, J.L. Atypical Autoimmune Hematologic Disorders in a Patient With Kabuki Syndrome. J. Pediatr. Hematol. Oncol. 2019, 41, e114–e115. [Google Scholar] [CrossRef]
- Zannolli, R.; Buoni, S.; Macucci, F.; Scarinci, R.; Viviano, M.; Orsi, A.; de Aloe, G.; Fimiani, M.; Volterrani, L.; de Santi, M.M.; et al. Kabuki syndrome with trichrome vitiligo, ectodermal defect and hypogammaglobulinemia A and G. Brain Dev. 2007, 29, 373–376. [Google Scholar] [CrossRef]
- Gurbuz, F.; Ozalp Yuregir, O.; Ceylaner, S.; Topaloglu, A.K.; Yuksel, B. Coexistence of Kabuki Syndrome and Autoimmune Thyroiditis. J. Clin. Res. Pediatr. Endocrinol. 2016, 8, 105–106. [Google Scholar] [CrossRef]
- Wilson, G.N. Thirteen cases of Niikawa-Kuroki syndrome: Report and review with emphasis on medical complications and preventive management. Am. J. Med. Genet. 1998, 79, 112–120. [Google Scholar] [CrossRef]
- Fujishiro, M.; Ogihara, T.; Tsukuda, K.; Shojima, N.; Fukushima, Y.; Kimura, S.; Oka, Y.; Asano, T. A case showing an association between type 1 diabetes mellitus and Kabuki syndrome. Diabetes Res. Clin. Pract. 2003, 60, 25–31. [Google Scholar] [CrossRef]
- Dunn, N.; Katial, R.; Stitt, J. A patient with kabuki (niikawa-kuroki) syndrome, common variable immunodeficiency and immune-mediated neutropenia found to have a novel mutation in the KTM2D Gene. J. Allergy Clin. Immunol. 2016, 137, AB117. [Google Scholar] [CrossRef]
- Nishizaki, N.; Fujinaga, S.; Hirano, D.; Murakami, H.; Kamei, K.; Ohtomo, Y.; Shimizu, T.; Kaneko, K. Membranoproliferative glomerulonephritis Type 3 associated with Kabuki syndrome. Clin. Nephrol. 2014, 81, 369–373. [Google Scholar] [CrossRef]
- Liblau, R.S.; Caillat-Zucman, S.; Fischer, A.M.; Bach, J.F.; Boitard, C. The prevalence of selective IgA deficiency in type 1 diabetes mellitus. J. Pathol. Microbiol. Immunol. 1992, 100, 709–712. [Google Scholar] [CrossRef]
- Smith, W.I., Jr.; Rabin, B.S.; Huellmantel, A.; Thiel, D.H.V.; Drash, A. Immunopathology of juvenile-onset diabetes mellitus: IgA deficiency and juvenile diabetes. Diabetes 1978, 27, 1092–1097. [Google Scholar] [CrossRef] [PubMed]
- Ho, J.; Fox, D.; Innes, A.M.; McLeod, R.; Butzner, D.; Johnson, N.; Trevenen, C.; Kendrick, V.; Cole, D.E.C. Kabuki syndrome and Crohn disease in a child with familial hypocalciuric hypercalcemia. J. Pediatr. Endocrinol. Metab. 2010, 23, 975–979. [Google Scholar] [CrossRef] [PubMed]
- Shah, M.; Bogucki, B.; Mavers, M.; deMello, D.E.; Knutsen, A. Cardiac conduction abnormalities and congenital immunodeficiency in a child with Kabuki syndrome: Case report. BMC Med. Genet. 2005, 6, 28. [Google Scholar] [CrossRef]
- Dentici, M.; Barresi, S.; Niceta, M.; Pantaleoni, F.; Pizzi, S.; Dallapiccola, B.; Tartaglia, M.; Digilio, M. Clinical spectrum of Kabuki-like syndrome caused by HNRNPK haploinsufficiency. Case report and literature review. Eur. J. Hum. Genet. 2019, 26, 477. [Google Scholar] [CrossRef]
- Wright, A.; Hall, A.; Daly, T.; Fontelonga, T.; Potter, S.; Schafer, C.; Lindsley, A.; Hung, C.; Bodamer, O.; Gussoni, E. Lysine methyltransferase 2D regulates muscle fiber size and muscle cell differentiation. FASEB J. 2021, 35, e21955. [Google Scholar] [CrossRef] [PubMed]
- Morgan, A.T.; Mei, C.; Da Costa, A.; Fifer, J.; Lederer, D.; Benoit, V.; McMillin, M.J.; Buckingham, K.J.; Bamshad, M.J.; Pope, K.; et al. Speech and language in a genotyped cohort of individuals with Kabuki syndrome. Am. J. Med. Genet. Part A 2015, 167, 1483–1492. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Raynor, E.M.; Lee, J.W.; Smith, S.L.; Heet, H.; Garrison, D.; Wrigley, J.; Kaylie, D.M.; Riska, K.M. Vestibular dysfunction and gross motor milestone acquisition in children with hearing loss: A systemic review. Otolaryngol.-Head Neck Surg. 2021, 165, 493–506. [Google Scholar] [CrossRef]
- Kurahashi, N.; Miyake, N.; Mizuno, S.; Koshimizu, E.; Kurahashi, H.; Yamada, K.; Natsume, J.; Aoki, Y.; Nakamura, M.; Taniai, H.; et al. Characteristics of epilepsy in patients with Kabuki syndrome with KMT2D mutations. Brain Dev. 2017, 39, 672–677. [Google Scholar] [CrossRef]
- Verrotti, A.; Agostinelli, S.; Cirillo, C.; D’Egidio, C.; Mohn, A.; Boncimino, A.; Coppola, G.; Spalice, A.; Nicita, F.; Pavone, P.; et al. Long-term outcome of epilepsy in Kabuki syndrome. Seizure 2011, 20, 650–654. [Google Scholar] [CrossRef]
- Anzai, M.; Terashima, H.; Kumagai, T.; Takenaka, S.; Kasai, M.; Watanabe, S.; Kubota, M.; Kozaki, R. A Kabuki syndrome patient with late onset West syndrome and intractable epilepsy. No To Hattatsu 2015, 47, S392. (In Japanese) [Google Scholar]
- Grunseich, C.; Fishbein, T.M.; Berkowitz, F.; Shamim, E.A. Tremor and Deep Brain Nuclei Hyperintensities in Kabuki Syndrome. Pediatr. Neurol. 2010, 43, 148–150. [Google Scholar] [CrossRef]
- Di Gennaro, G.; Condoluci, C.; Casali, C.; Ciccarelli, O.; Albertini, G. Epilepsy and polymicrogyria in Kabuki make-up (Niikawa-Kuroki) syndrome. Pediatr. Neurol. 1999, 21, 566–568. [Google Scholar] [CrossRef]
- Yoshioka, S.; Takano, T.; Matsuwake, K.; Sokoda, T.; Takeuchi, Y. A Japanese patient with Kabuki syndrome and unilateral perisylvian cortical dysplasia. Brain Dev. 2011, 33, 174–176. [Google Scholar] [CrossRef]
- Lodi, M.; Chifari, R.; Parazzini, C.; Viri, M.; Beccaria, F.; Lorenzetti, M.E.; Meloni, M.; Capovilla, G.; Romeo, A. Seizures and EEG pattern in Kabuki syndrome. Brain Dev. 2010, 32, 829–834. [Google Scholar] [CrossRef]
- Oksanen, V.E.; Arvio, M.A.; Peippo, M.M.; Valanne, L.K.; Sainio, K.O. Temporo-occipital spikes: A typical EEG finding in Kabuki syndrome. Pediatr. Neurol. 2004, 30, 67–70. [Google Scholar] [CrossRef]
- Topcu, Y.; Bayram, E.; Karaoglu, P.; Yis, U.; Kurul, S.H. Kabuki syndrome and perisylvian cortical dysplasia in a Turkish girl. J. Pediatr. Neurosci. 2013, 8, 259–260. [Google Scholar] [CrossRef] [PubMed]
- Daly, T.; Roberts, A.; Yang, E.; Mochida, G.H.; Bodamer, O. Holoprosencephaly in Kabuki syndrome. Am. J. Med. Genet. Part A 2020, 182, 441–445. [Google Scholar] [CrossRef]
- Dhar, S.S.; Lee, M.G. Cancer-epigenetic function of the histone methyltransferase KMT2D and therapeutic opportunities for the treatment of KMT2D-deficient tumors. Oncotarget 2021, 12, 1296–1308. [Google Scholar] [CrossRef]
- Scala, M.; Morana, G.; Sementa, A.R.; Merla, G.; Piatelli, G.; Capra, V.; Pavanello, M. Aggressive desmoid fibromatosis in Kabuki syndrome: Expanding the tumor spectrum. Pediatr. Blood Cancer 2019, 66, e27831. [Google Scholar] [CrossRef]
- Teranishi, H.; Koga, Y.; Nakashima, K.; Morihana, E.; Ishii, K.; Sakai, Y.; Taguchi, T.; Oda, Y.; Miyake, N.; Matsumoto, N.; et al. Cancer Management in Kabuki Syndrome: The First Case of Wilms Tumor and a Literature Review. J. Pediatr. Hematol. Oncol. 2018, 40, 391–394. [Google Scholar] [CrossRef]
- Tumino, M.; Licciardello, M.; Sorge, G.; Cutrupi, M.C.; Di Benedetto, F.; Amoroso, L.; Catania, R.; Pennisi, M.; D’Amico, S.; Di Cataldo, A. Kabuki syndrome and cancer in two patients. Am. J. Med. Genet. Part A 2010, 152A, 1536–1539. [Google Scholar] [CrossRef] [PubMed]
- Shahdadpuri, R.; O’Meara, A.; O’Sullivan, M.; Reardon, W. Low-grade fibromyxoid sarcoma: Yet another malignancy associated with Kabuki syndrome. Clin. Dysmorphol. 2008, 17, 199–202. [Google Scholar] [CrossRef] [PubMed]
- Casanova, M.; Selicorni, A.; Ferrari, A. Cancer predisposition in children with Kabuki syndrome. Am. J. Med. Genet. Part A 2011, 155, 1504. [Google Scholar] [CrossRef] [PubMed]
- Timothy, L.D.; Lehrke, H.D.; Chandan, V.S.; Kolbe, A.B.; Furuya, K.N. Diffuse Adenomatosis and Hepatocellular Carcinoma Treated with Liver Transplantation in an Adolescent Female with Kabuki Syndrome with a Novel KMT2D Gene Mutation. Case Rep. Pediatr. 2019, 2019, 7983824. [Google Scholar] [CrossRef]
- Karagianni, P.; Lambropoulos, V.; Stergidou, D.; Fryssira, H.; Chatziioannidis, I.; Spyridakis, I. Recurrent giant cell fibroblastoma: Malignancy predisposition in Kabuki syndrome revisited. Am. J. Med. Genet. Part A 2016, 170, 1333–1338. [Google Scholar] [CrossRef]
- Roma, D.; Palma, P.; Capolino, R.; Figà-Talamanca, L.; Diomedi-Camassei, F.; Lepri, F.R.; Digilio, M.C.; Marras, C.E.; Messina, R.; Carai, A.; et al. Spinal ependymoma in a patient with Kabuki syndrome: A case report. BMC Med. Genet. 2015, 16, 80. [Google Scholar] [CrossRef]
- Kaiwar, C.; Kruisselbrink, T.M.; Kudva, Y.C.; Klee, E.W.; Pichurin, P. Exome sequencing confirms diagnosis of kabuki syndrome in an-adult with hodgkin lymphoma and unusually severe multisystem phenotype. Clin. Immunol. 2019, 207, 55–57. [Google Scholar] [CrossRef]
- Scherer, S.; Theile, U.; Beyer, V.; Ferrari, R.; Kreck, C.; Rister, M. Patient with Kabuki syndrome and acute leukemia. Am. J. Med. Genet. 2003, 122A, 76–79. [Google Scholar] [CrossRef]
- Ijichi, O.; Kawakami, K.; Matsuda, Y.; Ikarimoto, N.; Miyata, K.; Takamatsu, H.; Tokunaga, M. A case of kabuki make-up syndrome with EBV + Burkitt’s lymphoma. Acta Paediatr. Jpn. Overs. Ed. 1996, 38, 66–68. [Google Scholar] [CrossRef]
- de Billy, E.; Strocchio, L.; Cacchione, A.; Agolini, E.; Gnazzo, M.; Novelli, A.; De Vito, R.; Capolino, R.; Digilio, M.C.; Caruso, R.; et al. Burkitt lymphoma in a patient with Kabuki syndrome carrying a novel KMT2D mutation. Am. J. Med. Genet. Part A 2019, 179, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Berger, F.; Delecluse, H.J. Lymphomas in immunocompromised hosts. Rev Prat 1993, 43, 1661–1664. [Google Scholar]
- Chrzanowska, K.H.; Krajewska-Walasek, M.; Kuś, J.; Michałkiewicz, J.; Maziarka, D.; Wolski, J.K.; Brecevic, L.; Madaliński, K. Kabuki (Niikawa-Kuroki) syndrome associated with immunodeficiency. Clin. Genet. 1998, 53, 308–312. [Google Scholar] [CrossRef]
- Hamahata, A.; Kamei, W.; Ishikawa, M.; Konoeda, H.; Yamaki, T.; Sakurai, H. Multiple pilomatricomas in Kabuki syndrome. Pediatr. Dermatol. 2013, 30, 253–255. [Google Scholar] [CrossRef]
- Bernier, F.-E.; Schreiber, A.; Coulombe, J.; Hatami, A.; Marcoux, D. Pilomatricoma Associated with Kabuki Syndrome. Pediatr. Dermatol. 2017, 34, e26–e27. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.; El Moneim, A.A.; Aleck, K.; Aughton, D.J.; Baumann, C.; Braddock, S.R.; Gillessen-Kaesbach, G.; Graham, J.M., Jr.; Grebe, T.A.; Gripp, K.W.; et al. Further delineation of Kabuki syndrome in 48 well-defined new individuals. Am. J. Med. Genet. 2005, 132A, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Schrander-Stumpel, C.T.R.M.; Spruyt, L.; Curfs, L.M.G.; Defloor, T.; Schrander, J.J.P. Kabuki syndrome: Clinical data in 20 patients, literature review, and further guidelines for preventive management. Am. J. Med. Genet. 2005, 132A, 234–243. [Google Scholar] [CrossRef]
- Kawame, H.; Hannibal, M.C.; Hudgins, L.; Pagon, R.A. Phenotypic spectrum and management issues in Kabuki syndrome. J. Pediatr. 1999, 134, 480–485. [Google Scholar] [CrossRef]
- Gole, H.; Chuk, R.; Coman, D. Persistent hyperinsulinism in kabuki syndrome 2: Case report and literature review. Clin. Pract. 2016, 6, 68–70. [Google Scholar] [CrossRef]
- Gibson, C.E.; Boodhansingh, K.E.; Li, C.; Conlin, L.; Chen, P.; Becker, S.A.; Bhatti, T.; Bamba, V.; Adzick, N.S.; De Leon, D.D.; et al. Congenital Hyperinsulinism in Infants with Turner Syndrome: Possible Association with Monosomy X and KDM6A Haploinsufficiency. Horm. Res. Paediatr. 2018, 89, 413–422. [Google Scholar] [CrossRef]
- Tawa, R.; Kaino, Y.; Ito, T.; Goto, Y.; Kida, K.; Matsuda, H. A case of Kabuki make-up syndrome with central diabetes insipidus and growth hormone neurosecretory dysfunction. Acta Paediatr. Jpn. Overseas Ed. 1994, 36, 412–415. [Google Scholar] [CrossRef] [PubMed]
- Ito, N.; Ihara, K.; Tsutsumi, Y.; Miyake, N.; Matsumoto, N.; Hara, T. Hypothalamic pituitary complications in Kabuki syndrome. Pituitary 2013, 16, 133–138. [Google Scholar] [CrossRef] [PubMed]
- So, P.L.; Luk, H.M.; Yu, K.P.T.; Cheng, S.S.W.; Hau, E.W.L.; Ho, S.K.L.; Lam, S.T.S.; Lo, I.F.M. Clinical and molecular characterization study of Chinese Kabuki syndrome in Hong Kong. Am. J. Med. Genet. Part A 2020, 185, 675–686. [Google Scholar] [CrossRef]
- Banka, S.; Howard, E.; Bunstone, S.; Chandler, K.E.; Kerr, B.; Lachlan, K.; McKee, S.; Mehta, S.G.; Tavares, A.L.T.; Tolmie, J.; et al. MLL2 mosaic mutations and intragenic deletion-duplications in patients with Kabuki syndrome. Clin. Genet. 2013, 83, 467–471. [Google Scholar] [CrossRef]
- Courcet, J.B.; Faivre, L.; Michot, C.; Burguet, A.; Perez-Martin, S.; Alix, E.; Amiel, J.; Baumann, C.; Cordier, M.P.; Cormier-Daire, V.; et al. Clinical and molecular spectrum of renal malformations in kabuki syndrome. J. Pediatr. 2013, 163, 742–746. [Google Scholar] [CrossRef]
- Çetinkaya, E.; Misirhoǧlu, E.D.; Vidinlisan, S.; Baydar, Z.; Özhan, Z.R. Hypospadias in a patient with Kabuki make-up (Niikawa-Kuroki) syndrome. J. Pediatr. Endocrinol. Metab. 2001, 14, 803–805. [Google Scholar] [CrossRef]
- Shawky, R.M.; Gamal, R.; Mostafa, N. Kabuki make-up syndrome with genitourinary anomalies, ophthalmologic features and hyperpigmentation in an Egyptian child. Egypt. J. Med. Hum. Genet. 2017, 18, 87–92. [Google Scholar] [CrossRef]
- Wang, L.C.; Chiu, I.S.; Wang, P.J.; Wu, M.H.; Wang, J.K.; Hung, Y.B.; Lin, S.J. Kabuki make-up syndrome associated with congenital heart disease. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi 1994, 35, 63–69. [Google Scholar] [PubMed]
- Kerr, B.; Murphy, P.; Quinn, J. Refractory ITP in a patient with Kabuki syndrome: Response to low-dose rituximab. Int. J. Hematol. 2017, 105, 702–703. [Google Scholar] [CrossRef]
- Ewart-Toland, A.; Enns, G.M.; Cox, V.A.; Mohan, G.C.; Rosenthal, P.; Golabi, M. Severe congenital anomalies requiring transplantation in children with Kabuki syndrome. Am. J. Med. Genet. 1998, 80, 362–367. [Google Scholar] [CrossRef]
- Hamdi Kamel, M.; Gilmartin, B.; Mohan, P.; Hickey, D.P. Successful long-term outcome of kidney transplantation in a child with Kabuki syndrome. Pediatr. Transplant. 2006, 10, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Bögershausen, N.; Alanay, Y.; Simsek Kiper, P.O.; Plume, N.; Keupp, K.; Pohl, E.; Pawlik, B.; Rachwalski, M.; Milz, E.; et al. A mutation screen in patients with Kabuki syndrome. Hum. Genet. 2011, 130, 715–724. [Google Scholar] [CrossRef] [PubMed]
- Kluijt, I.; Van Dorp, D.B.; Kwee, M.L.; Toutain, A.; Keppler-Noreuil, K.; Warburg, M.; Bitoun, P. Kabuki syndrome—Report of six cases and review of the literature with emphasis on ocular features. Ophthalmic Genet. 2000, 21, 51–61. [Google Scholar] [CrossRef]
- Cheon, C.K.; Choi, H.Y.; Park, S.H.; Jung, J.H.; Kim, S.J. Ocular manifestations in kabuki syndrome: A report of 10 cases and literature review. Ophthalmic Genet. 2020, 42, 101–104. [Google Scholar] [CrossRef]
- Wessels, M.W.; Brooks, A.S.; Hoogeboom, J.; Niermeijer, M.F.; Willems, P.J. Kabuki syndrome: A review study of three hundred patients. Clin. Dysmorph. 2002, 11, 95–102. [Google Scholar] [CrossRef]
- Rosenberg, C.E.; Daly, T.; Hung, C.; Hsueh, I.; Lindsley, A.W.; Bodamer, O. Prenatal and perinatal history in Kabuki Syndrome. Am. J. Med. Genet. Part A 2020, 182, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Dentici, M.L.; Di Pede, A.; Lepri, F.R.; Gnazzo, M.; Lombardi, M.H.; Auriti, C.; Petrocchi, S.; Pisaneschi, E.; Bellacchio, E.; Capolino, R.; et al. Kabuki syndrome: Clinical and molecular diagnosis in the first year of life. Arch. Dis. Child. 2015, 100, 158–164. [Google Scholar] [CrossRef]
- Vaux, K.K.; Jones, K.L.; Jones, M.C.; Schelley, S.; Hudgins, L. Developmental outcome in Kabuki syndrome. Am. J. Med. Genet. 2005, 132A, 263–264. [Google Scholar] [CrossRef] [PubMed]
- Dorleijn, D.M.; Cohen-Overbeek, T.E.; Groenendaal, F.; Bruinse, H.W.; Stoutenbeek, P. Idiopathic polyhdranmios and postnatal findings. J. Matern. Fetal. Neonatal. Med. 2009, 22, 315–320. [Google Scholar] [CrossRef]
- Magann, E.F.; Chauhan, S.P.; Doherty, D.A.; Lutgendorf, M.A.; Magann, M.I.; Morrison, J.C. A review of idiopathic hydramnios and pregnancy outcomes. Obstet. Gynecol. Surv. 2007, 62, 795–802. [Google Scholar] [CrossRef] [PubMed]
- Schott, D.A.; Blok, M.J.; Gerver, W.J.M.; Devriendt, K.; Zimmermann, L.J.I.; Stumpel, C.T.R.M. Growth pattern in Kabuki syndrome with a KMT2D mutation. Am. J. Med. Genet. Part A 2016, 170, 3172–3179. [Google Scholar] [CrossRef] [PubMed]
- Schott, D.A.; Gerver, W.J.M.; Stumpel, C.T.R.M. Growth Hormone Therapy in Children with Kabuki Syndrome: 1-year Treatment Results. Horm. Res. Paediatr. 2017, 88, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Schott, D.A.; Stumpel, C.T.R.M.; Klaassens, M. Hypermobility in individuals with Kabuki syndrome: The effect of growth hormone treatment. Am. J. Med. Genet. Part A 2019, 179, 219–223. [Google Scholar] [CrossRef] [PubMed]
- van Montfort, L.; Gerver, W.J.M.; Kooger, B.L.S.; Plat, J.; Bierau, J.; Stumpel, C.; Schott, D.A. Follow-Up Study of Growth Hormone Therapy in Children with Kabuki Syndrome: Two-Year Treatment Results. Horm. Res. Paediatr. 2021, 94, 285–296. [Google Scholar] [CrossRef]
- Schott, D.A.; Gerver, W.J.M.; Stumpel, C.T.R.M. Growth Hormone Stimulation Tests in Children with Kabuki Syndrome. Horm. Res. Paediatr. 2016, 86, 319–324. [Google Scholar] [CrossRef] [PubMed]
- Ruault, V.; Corsini, C.; Duflos, C.; Akouete, S.; Georgescu, V.; Abaji, M.; Alembick, Y.; Alix, E.; Amiel, J.; Amouroux, C.; et al. Growth charts in Kabuki syndrome 1. Am. J. Med. Genet. Part A 2020, 182, 446–453. [Google Scholar] [CrossRef] [PubMed]
- Kurosawa, K.; Kawame, H.; Ochiai, Y.; Nakashima, M.; Tohma, T.; Ohashi, H. Patellar dislocation in Kabuki syndrome. Am. J. Med. Genet. 2002, 108, 160–163. [Google Scholar] [CrossRef] [PubMed]
- Weir, R.A.; Alston, A.F.; Ali, M.A. Acute myocardial infarction in Kabuki syndrome: Chance occurrence or a novel risk factor for premature atherosclerosis? Int. J. Cardiol. 2014, 176, e26–e28. [Google Scholar] [CrossRef] [PubMed]
- Mervis, C.B.; Becerra, A.M.; Rowe, M.L.; Hersh, J.H.; Morris, C.A. Intellectual abilities and adaptive behavior of children and adolescents with Kabuki syndrome: A preliminary study. Am. J. Med. Genet. 2005, 132A, 248–255. [Google Scholar] [CrossRef]
- Toutain, A.; Plée, Y.; Ployet, M.J.; Benoit, S.; Perrot, A.; Sembely, C.; Barthez, M.A.; Moraine, C. Deafness and Mondini dysplasia in Kabuki (Niikawa-Kuroki) Syndrome. Report of a case and review of the literature. Genet. Couns. 1997, 8, 99–105. [Google Scholar] [PubMed]
- Van Lierde, K.M.; Van Borsel, J.; Van Cauwenberge, P. Speech patterns in Kabuki make-up syndrome: A case report. J. Commun. Disord. 2000, 33, 447–462. [Google Scholar] [CrossRef]
- Burke, L.W.; Jones, M.C. Kabuki syndrome: Underdiagnosed recognizable pattern in cleft palate patients. Cleft Palate-Craniofac. J. 1995, 32, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Lindgren, A.M.; Hoyos, T.; Talkowski, M.E.; Hanscom, C.; Blumenthal, I.; Chiang, C.; Ernst, C.; Pereira, S.; Ordulu, Z.; Clericuzio, C.; et al. Haploinsufficiency of KDM6A is associated with severe psychomotor retardation, global growth restriction, seizures and cleft palate. Hum. Genet. 2013, 132, 537–552. [Google Scholar] [CrossRef] [PubMed]
- Lu, J.; Mo, G.; Ling, Y.; Ji, L. A novel KMT2D mutation resulting in Kabuki syndrome: A case report. Mol. Med. Rep. 2016, 14, 3641–3645. [Google Scholar] [CrossRef]
- Petzold, D.; Kratzsch, E.; Opitz, C.; Tinschert, S. The Kabuki syndrome: Four patients with oral abnormalities. Eur. J. Orthod. 2003, 25, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Miyake, N.; Mizuno, S.; Okamoto, N.; Ohashi, H.; Shiina, M.; Ogata, K.; Tsurusaki, Y.; Nakashima, M.; Saitsu, H.; Niikawa, N.; et al. KDM6A Point Mutations Cause Kabuki Syndrome. Hum. Mutat. 2013, 34, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.H.; Eaves, L.C. Kabuki make-up (Niikawa-Kuroki) syndrome: Cognitive abilities and autistic features. Dev. Med. Child Neurol. 1997, 39, 487–490. [Google Scholar] [CrossRef] [PubMed]
- Bayar Muluk, N.; Yalçinkaya, F.; Budak, B.; Gündüz, S.; Ayas, K. Evaluation for language and speech development in Kabuki make-up syndrome: A case report. Int. J. Pediatr. Otorhinolaryngol. 2009, 73, 1837–1840. [Google Scholar] [CrossRef]
- Association, A.P. Diagnostic and Statistical Manual of Mental Health Disorders, 5th ed.; American Psychologial Association: Washington, DC, USA, 2013; pp. 33–41. [Google Scholar]
- Lehman, N.; Mazery, A.C.; Visier, A.; Baumann, C.; Lachesnais, D.; Capri, Y.; Toutain, A.; Odent, S.; Mikaty, M.; Goizet, C.; et al. Molecular, clinical and neuropsychological study in 31 patients with Kabuki syndrome and KMT2D mutations. Clin. Genet. 2017, 92, 298–305. [Google Scholar] [CrossRef]
- Paulussen, A.D.C.; Stegmann, A.P.A.; Blok, M.J.; Tserpelis, D.; Posma-Velter, C.; Detisch, Y.; Smeets, E.E.J.G.L.; Wagemans, A.; Schrander, J.J.P.; Van Den Boogaard, M.J.H.; et al. MLL2 mutation spectrum in 45 patients with Kabuki syndrome. Hum. Mutat. 2011, 32, E2018–E2025. [Google Scholar] [CrossRef] [PubMed]
- Kasdon, B.D.; Fox, J.E. Kabuki syndrome: Diagnostic and treatment considerations. Ment. Health Fam. Med. 2012, 9, 171–179. [Google Scholar] [PubMed]
- Porntaveetus, T.; Abid, M.F.; Theerapanon, T.; Srichomthong, C.; Ohazama, A.; Kawasaki, K.; Kawasaki, M.; Suphapeetiporn, K.; Sharpe, P.T.; Shotelersuk, V. Expanding the oro-dental and mutational spectra of Kabuki Syndrome with expression of KMT2D and KDM6A in human tooth germs. Int. J. Biol. Sci. 2018, 14, 381–389. [Google Scholar] [CrossRef]
- Xin, C.; Wang, C.; Wang, Y.; Zhao, J.; Wang, L.; Li, R.; Liu, J. Identification of novel KMT2D mutations in two Chinese children with Kabuki syndrome: A case report and systematic literature review. BMC Med. Genet. 2018, 19, 31. [Google Scholar] [CrossRef] [PubMed]
- Miyake, N.; Koshimizu, E.; Okamoto, N.; Mizuno, S.; Ogata, T.; Nagai, T.; Kosho, T.; Ohashi, H.; Kato, M.; Sasaki, G.; et al. MLL2 and KDM6A mutations in patients with Kabuki syndrome. Am. J. Med. Genet. Part A 2013, 161, 2234–2243. [Google Scholar] [CrossRef]
- van Dongen, L.C.M.; Wingbermuhle, P.A.M.; van der Veld, W.M.; Stumpel, C.; Kleefstra, T.; Egger, J.I.M. Exploring the cognitive phenotype of Kabuki (Niikawa-Kuroki) syndrome. J. Intellect. Disabil. Res. JIDR 2019, 63, 498–506. [Google Scholar] [CrossRef]
- Theodore-Oklota, C.; Hartman, D.S.; Hoffman, D.L.; Björnsson, H.T. A Qualitative Study to Characterize the Humanistic Burden of Kabuki Syndrome in the United States and Canada. Adv. Ther. 2022, 39, 619–631. [Google Scholar] [CrossRef]
- Malik, P.; Sharma, A.; Sakhuja, S.; Munjal, S.; Panda, N.K. Speech and language characteristics in Kabuki Syndrome. Internet J. Allied Health Sci. Pract. 2010, 8, 12. [Google Scholar] [CrossRef]
- Upton, S.; Stadter, C.S.; Landis, P.; Wulfsberg, E.A. Speech characteristics in the Kabuki syndrome. Am. J. Med. Genet. 2003, 116A, 338–341. [Google Scholar] [CrossRef]
- Ilyina, H.; Lurie, I.; Naumtchik, I.; Amoashy, D.; Stephanenko, G.; Fedotov, V.; Kostjuk, A. Kabuki make-up (Niikawa-Kuroki) syndrome in the Byelorussian register of congenital malformations: Ten new observations. Am. J. Med. Genet. 1995, 56, 127–131. [Google Scholar] [CrossRef]
- Defloor, T.; Van Borsel, J.; Schrander-Stumpel, C.T.R.M.; Curfs, L.M.G. Expressive language in children with Kabuki syndrome. Am. J. Med. Genet. 2005, 132A, 256–259. [Google Scholar] [CrossRef]
- Sertçelik, M.; Uğur, Ç.; Şahin Aközel, A.; Gürkan, C.K. A child with kabuki syndrome and autism spectrum disorder. Noropsikiyatr. Ars. 2016, 53, 280–282. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Lai, K.V.; Nussbaum, E.; Do, P.; Chen, J.; Randhawa, I.S.; Chin, T. Congenital lung anomalies in kabuki syndrome. J. Pediatr. Cong. Disord. 2014, 104, 1–5. [Google Scholar]
- Matsumoto, N.; Niikawa, N. Kabuki make-up syndrome: A review. Am. J. Med. Genet. Semin. Med. Genet. 2003, 117C, 57–65. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Search Terms | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
|
|
|
| System 1 | Evaluation | Comment |
|---|---|---|
| Growth | Measurement of height, weight, and head circumference | While infants may have FTT, adolescents and adults may have obesity. KS-specific growth charts available |
| Ophthalmologic | Ophthalmology evaluation | For assessment of strabismus, refractive error, ptosis, and corneal abnormalities |
| Hearing | Baseline audiology evaluation | To assess for conductive and/or sensorineural hearing loss |
| Mouth | Directed evaluation of the palate for palatal anomalies | Consider referral to a craniofacial specialist if palatal anomalies are suspected |
| Consider dental evaluation for those over 3 years of age | ||
| Cardiac | Echocardiogram with visualization of the aortic arch | To assess for congenital heart defects, including coarctation of the aorta |
| Consider EKG | If arrhythmia is suspected | |
| Respiratory | Consider chest radiographs to assess for diaphragmatic eventuation | In those with respiratory issues, chronic cough, or recurrent pneumonia |
| Gastrointestinal/Feeding | Asses nutritional status, feeding, GERD | Consider assessment by a feeding team and/or a VFSS for those with suspected dysphagia |
| Genitourinary | Baseline renal ultrasound | To evaluate for renal anomalies and hydronephrosis |
| Physical examination for hypospadias and/or cryptorchidism in males | ||
| Musculoskeletal | Consider radiographs of the spine in those with scoliosis | To assess for vertebral anomalies |
| Endocrinologic | Assessment for hyperinsulinism | In neonates and infants with persistent hypoglycemia |
| Assessment for hypothyroidism and growth hormone deficiency | In those with an abnormal growth velocity | |
| Immunologic | T cell count, T cell subsets, and serum immunoglobulin levels at the time of diagnosis or at age one year (whichever comes later) | Referral to immunology if immunological studies are abnormal or there is a history of recurrent infections |
| Neurologic | EEG | In those with suspected seizures |
| Brain MRI | To evaluate for a structural brain malformation in those with seizures | |
| To evaluate for Chiari I malformation in those with suggestive symptoms | ||
| Psychiatric/behavioral | Neuropsychiatric evaluation | To include screening for the presence of behavioral problems, including sleep disturbances, ADHD, anxiety, and/or traits suggestive of ASD for individuals age >12 months |
| Miscellaneous/Other | Developmental assessment | To include motor, speech/language evaluation, general cognitive, and vocational skills |
| Consultation with a clinical geneticist and/or genetic counselor | Medical home, care coordination, molecular diagnosis and counseling |
| System 1 | Evaluation | Frequency |
|---|---|---|
| Growth | Measurement of at least height and weight | At each appointment |
| Ophthalmologic | Ophthalmology or optometry to assess vision | At least annually |
| Hearing | Hearing assessment | At least annually |
| Musculoskeletal | Clinical evaluation for scoliosis | At each appointment until skeletal maturity |
| Endocrinologic | Thyroid function tests | Every 2–3 years |
| Immunologic | Assessment of complete blood count, immunoglobulin levels, flow cytometry? | Every 2–3 years |
| Miscellaneous/Other | Monitor developmental progress and educational needs | At each visit during childhood and adolescence |
| Manifestation 1 | Treatment | Considerations/Other |
|---|---|---|
| Strabismus, refractive error, ptosis, lagophthalmos | Standard treatment per Ophthalmology | |
| Hearing loss | Consideration of pressure equalizing tubes in those with conductive hearing loss | Referral to an ENT specialist and audiologist |
| Hearing aids may be considered for those with sensorineural hearing loss | ||
| Cleft lip and/or palate | Standard treatment | Management through a specialized Craniofacial clinic is ideal |
| The palate may be shorter, which can lead to velopharyngeal insufficiency after typical cleft repair | ||
| Dental anomalies | Orthodontic referral if hypodontia or significant malocclusion are noted | |
| Congenital heart defects and/or arrhythmia | Standard treatment per Cardiology | It is unclear whether there is an increased risk for aortic aneurysm; however, if catheterization or angioplasty is being considered, a potential increased risk of aortic aneurysm should be communicated to the treating team |
| Feeding difficulties/GERD | Standard treatment, which may include thickening feeds and appropriate positioning after meals in infants and toddlers | Pharmacologic treatment for GERD may be considered |
| Consideration of gastrostomy tube | In those with severe feeding difficulties and/or poorly coordinated suck and swallow | |
| Chronic diarrhea | Referral to a Gastroenterology specialist | Consider evaluation for malabsorption and/or celiac disease |
| Hypospadias/cryptorchidism | Standard treatment per Urology | |
| Hyperinsulinism and hypothyroidism | Standard treatment per Endocrinology | |
| Short stature | Consideration of growth hormone therapy | |
| Recurrent infections | Intravenous immunoglobulin (IVIG) therapy may be considered in those this documented immunoglobulin deficiency | Referral to Immunology |
| Seizure disorder | Standard antiepileptic treatment per Neurology | |
| Premature thelarche | No treatment is warranted if there are no other signs of premature puberty | |
| Need for anesthesia | Care in positioning during intubation due to joint laxity, which can affect the cervical spine | Education regarding potential structural airway anomalies that could make intubation difficult |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barry, K.K.; Tsaparlis, M.; Hoffman, D.; Hartman, D.; Adam, M.P.; Hung, C.; Bodamer, O.A. From Genotype to Phenotype—A Review of Kabuki Syndrome. Genes 2022, 13, 1761. https://doi.org/10.3390/genes13101761
Barry KK, Tsaparlis M, Hoffman D, Hartman D, Adam MP, Hung C, Bodamer OA. From Genotype to Phenotype—A Review of Kabuki Syndrome. Genes. 2022; 13(10):1761. https://doi.org/10.3390/genes13101761
Chicago/Turabian StyleBarry, Kelly K., Michaelangelo Tsaparlis, Deborah Hoffman, Deborah Hartman, Margaret P. Adam, Christina Hung, and Olaf A. Bodamer. 2022. "From Genotype to Phenotype—A Review of Kabuki Syndrome" Genes 13, no. 10: 1761. https://doi.org/10.3390/genes13101761
APA StyleBarry, K. K., Tsaparlis, M., Hoffman, D., Hartman, D., Adam, M. P., Hung, C., & Bodamer, O. A. (2022). From Genotype to Phenotype—A Review of Kabuki Syndrome. Genes, 13(10), 1761. https://doi.org/10.3390/genes13101761