
A New Cloud-Native Tool for Pharmacogenetic Analysis
 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Creating a PGx Database
2.2. Designing a Bioinformatics Pipeline
2.3. Validating Variant Calls and Variant Allele Assignment
3. Results
3.1. System Architecture
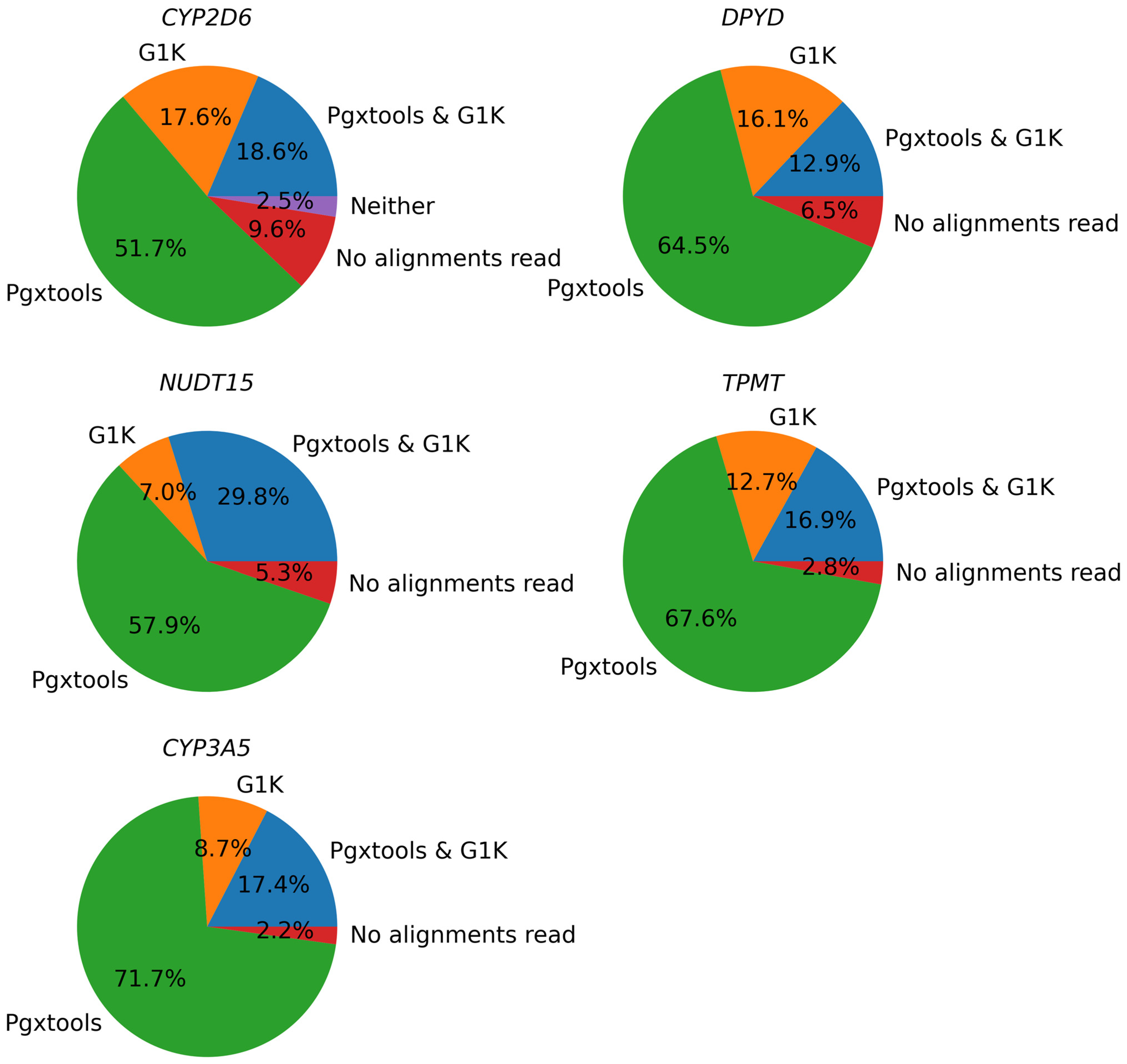
3.2. Accuracy of Variant Calls from Alignments to Variants
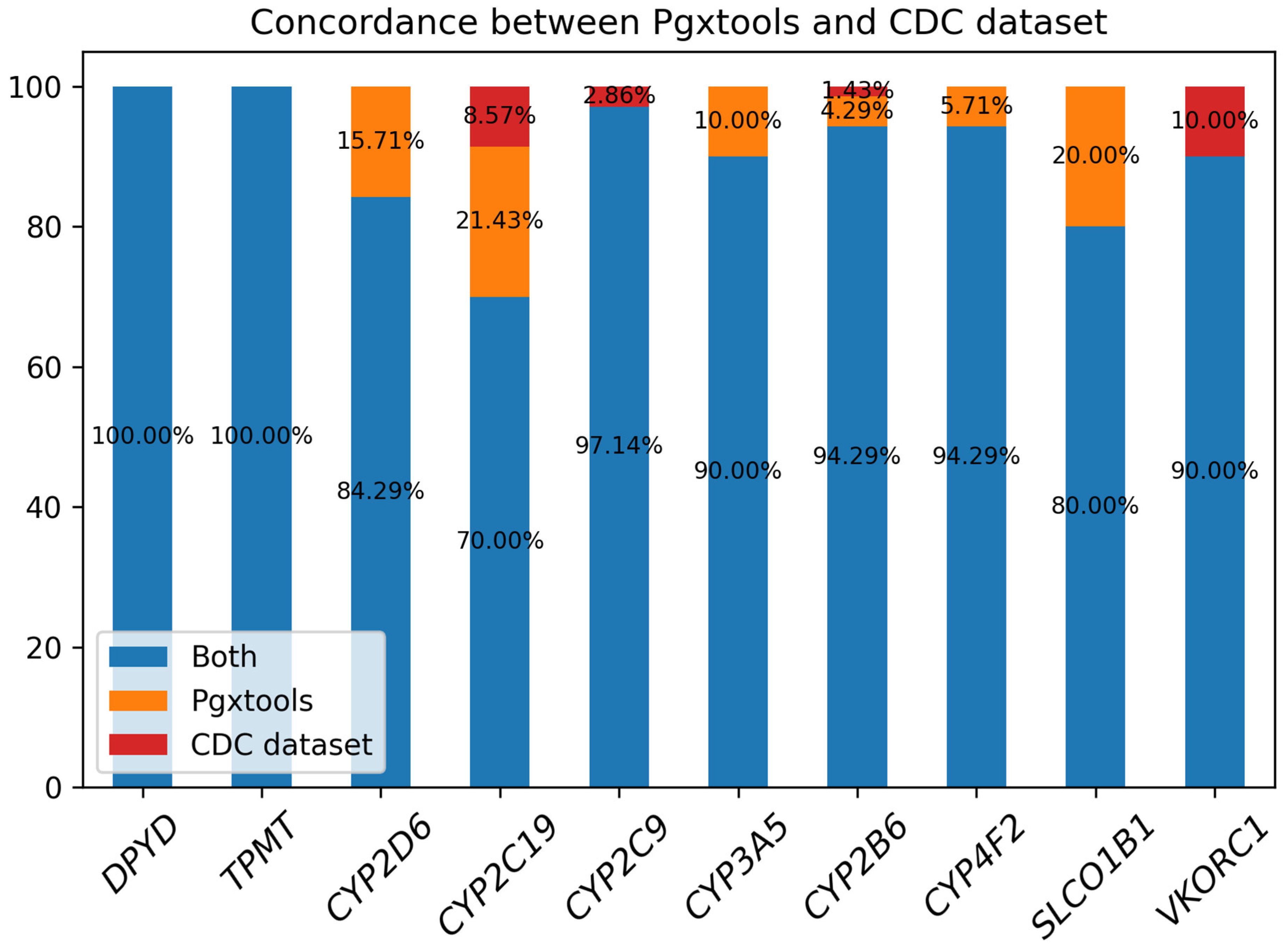
3.3. From Variants to Genotypes
3.4. PGx Interpretation and Reports
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
- The 1000 Genomes Project (G1K) dataset (https://www.internationalgenome.org/1000-genomes-summary/, accessed on 15 January 2023)
- The Reference Materials for Pharmacogenetics|CDC. Consensus Genotypes for 28 PGx Genes Archived on CDC as Part of the Reference Materials for Pharmacogenetics (https://www.cdc.gov/labquality/get-rm/inherited-genetic-diseases-pharmacogenetics/pharmacogenetics.html, accessed on 15 January 2023)
Conflicts of Interest
References
- Pirmohamed, M.; James, S.; Meakin, S.; Green, C.; Scott, A.K.; Walley, T.J.; Farrar, K.; Park, B.K.; Breckenridge, A.M. Adverse drug reactions as cause of admission to hospital: Prospective analysis of 18 820 patients. BMJ 2004, 329, 15–19. [Google Scholar] [CrossRef] [PubMed]
- Lazarou, J.; Pomeranz, B.H.; Corey, P.N. Incidence of adverse drug reactions in hospitalized patients: A meta-analysis of prospective studies. JAMA 1998, 279, 1200–1205. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.; Zhou, Z.; Zhou, J.; Chen, S.Q. Pharmacogenomics of drug metabolizing enzymes and transporters: Relevance to precision medicine. Genom. Proteom. Bioinform. 2016, 14, 298–313. [Google Scholar] [CrossRef] [PubMed]
- Schaeffeler, E.; Fischer, C.; Brockmeier, D.; Wernet, D.; Moerike, K.; Eichelbaum, M.; Zanger, U.M.; Schwab, M. Comprehensive analysis of thiopurine S-methyltransferase phenotype-genotype correlation in a large population of German-Caucasians and identification of novel TPMT variants. Pharmacogenetics 2004, 14, 407–417. [Google Scholar] [CrossRef]
- Mallal, S.; Phillips, E.; Carosi, G.; Molina, J.M.; Workman, C.; Tomazic, J.; Jägel-Guedes, E.; Rugina, S.; Kozyrev, O.; Cid, J.F.; et al. HLA-B*5701 screening for hypersensitivity to abacavir. N. Engl. J. Med. 2008, 358, 568–579. [Google Scholar] [CrossRef] [PubMed]
- Wong, B.Y.L.; Li, Z.; Raphael, M.J.; De Angelis, C.; Hwang, D.M.; Fu, L. Developing DPYD Genotyping Method for Personalized Fluoropyrimidines Therapy. J. Appl. Lab. Med. 2023, 12, jfad092. [Google Scholar] [CrossRef]
- Health C for D and R. Table of Pharmacogenetic Associations. FDA [Internet]. 2022. Available online: https://www.fda.gov/medical-devices/precision-medicine/table-pharmacogenetic-associations (accessed on 15 January 2024).
- Abdullah-Koolmees, H.; van Keulen, A.M.; Nijenhuis, M.; Deneer, V.H.M. Pharmacogenetics Guidelines: Overview and Comparison of the DPWG, CPIC, CPNDS, and RNPGx Guidelines. Front. Pharmacol. 2021, 11, 595219. [Google Scholar] [CrossRef]
- Cavallari, L.H.; Beitelshees, A.L.; Blake, K.V.; Dressler, L.G.; Duarte, J.D.; Elsey, A.; Eichmeyer, J.N.; Empey, P.E.; Franciosi, J.P.; Hicks, J.P.; et al. The IGNITE Pharmacogenetics Working Group: An Opportunity for Building Evidence with Pharmacogenetic Implementation in a Real-World Setting. Clin. Transl. Sci. 2017, 10, 143–146. [Google Scholar] [CrossRef]
- van der Wouden, C.H.; Böhringer, S.; Cecchin, E.; Cheung, K.C.; Dávila-Fajardo, C.L.; Deneer, V.H.M.; Dolžan, V.; Ingelman-Sundberg, M.; Jönsson, S.; Karlsson, M.O.; et al. Generating evidence for precision medicine: Considerations made by the Ubiquitous Pharmacogenomics Consortium when designing and operationalizing the PREPARE study. Pharmacogenetics Genom. 2020, 30, 131–144. [Google Scholar] [CrossRef]
- Swen, J.J.; van der Wouden, C.H.; Manson, L.E.; Abdullah-Koolmees, H.; Blagec, K.; Blagus, T.; Böhringer, S.; Cambon-Thomsen, A.; Cecchin, E.; Cheung, K.; et al. A 12-gene pharmacogenetic panel to prevent adverse drug reactions: An open-label, multicentre, controlled, cluster-randomised crossover implementation study. Lancet 2023, 401, 347–356. [Google Scholar] [CrossRef]
- Keeling, N.J.; Rosenthal, M.M.; West-Strum, D.; Patel, A.S.; Haidar, C.E.; Hoffman, J.M. Preemptive pharmacogenetic testing: Exploring the knowledge and perspectives of US payers. Genet. Med. 2019, 21, 1224–1232. [Google Scholar] [CrossRef] [PubMed]
- Roden, D.M.; McLeod, H.L.; Relling, M.V.; Williams, M.S.; Mensah, G.A.; Peterson, J.F.; Van Driest, S.L. Pharmacogenomics. Lancet 2019, 394, 521–532. [Google Scholar] [CrossRef] [PubMed]
- Sangkuhl, K.; Whirl-Carrillo, M.; Whaley, R.M.; Woon, M.; Lavertu, A.; Altman, R.B.; Carter, L.; Verma, A.; Ritchie, M.D.; Klein, T.E. Pharmacogenomics Clinical Annotation Tool (PharmCAT). Clin. Pharmacol. Ther. 2020, 107, 203–210. [Google Scholar] [CrossRef]
- Yuan, D.Y.; Wildish, T. Bioinformatics Application with Kubeflow for Batch Processing in Clouds. In High Performance Computing; Jagode, H., Anzt, H., Juckeland, G., Ltaief, H., Eds.; Springer International Publishing: Cham, Switzerland, 2020; pp. 355–367. [Google Scholar]
- Pereira, R.; Oliveira, J.; Sousa, M. Bioinformatics and Computational Tools for Next-Generation Sequencing Analysis in Clinical Genetics. J. Clin. Med. 2020, 9, 132. [Google Scholar] [CrossRef] [PubMed]
- Clinical Pharmacogenetics Implementation Consortium Guidelines—CPIC [Internet]. Available online: https://cpicpgx.org/guidelines/ (accessed on 15 January 2024).
- Pratt, V.M.; Everts, R.E.; Aggarwal, P.; Beyer, B.N.; Broeckel, U.; Epstein-Baak, R.; Hujsak, P.; Kornreich, R.; Liao, J.; Lorier, R.; et al. Characterization of 137 Genomic DNA Reference Materials for 28 Pharmacogenetic Genes: A GeT-RM Collaborative Project. J. Mol. Diagn. 2016, 18, 109–123. [Google Scholar] [CrossRef] [PubMed]
- Reference Materials for Pharmacogenetics|CDC. Consensus Genotypes for 28 PGx Genes Archived on CDC as Part of the Reference Materials for Pharmacogenetics [Internet]. 2023. Available online: https://www.cdc.gov/labquality/get-rm/inherited-genetic-diseases-pharmacogenetics/pharmacogenetics.html (accessed on 15 January 2024).
- ENA Browser. The WGS Samples for the Consensus Genotypes for 28 PGx Genes as PRJEB19931 Archived by ENA [Internet]. Available online: https://www.ebi.ac.uk/ena/browser/view/PRJEB19931 (accessed on 15 January 2024).
- What is CrossMap ?—CrossMap 0.6.4 Documentation [Internet]. Available online: https://crossmap.sourceforge.net/ (accessed on 15 January 2024).
- CPIC® Guideline for Thiopurines and TPMT and NUDT15—CPIC [Internet]. Available online: https://cpicpgx.org/guidelines/guideline-for-thiopurines-and-tpmt/ (accessed on 15 January 2024).
- CPIC® Guideline for Tricyclic Antidepressants and CYP2D6 and CYP2C19—CPIC [Internet]. Available online: https://cpicpgx.org/guidelines/guideline-for-tricyclic-antidepressants-and-cyp2d6-and-cyp2c19/ (accessed on 15 January 2024).
- CPIC® Guideline for Clopidogrel and CYP2C19—CPIC [Internet]. Available online: https://cpicpgx.org/guidelines/guideline-for-clopidogrel-and-cyp2c19/ (accessed on 15 January 2024).
- CPIC® Guideline for Proton Pump Inhibitors and CYP2C19—CPIC [Internet]. Available online: https://cpicpgx.org/guidelines/cpic-guideline-for-proton-pump-inhibitors-and-cyp2c19/ (accessed on 15 January 2024).
- CPIC® Guideline for Voriconazole and CYP2C19—CPIC [Internet]. Available online: https://cpicpgx.org/guidelines/guideline-for-voriconazole-and-cyp2c19/ (accessed on 15 January 2024).
- Brouwer, J.M.J.L.; Nijenhuis, M.; Soree, B.; Guchelaar, H.J.; Swen, J.J.; van Schaik, R.H.N.; van der Weide, J.; Rongen, G.; Buunk, A.; de Boer-Veger, N.J.; et al. Dutch Pharmacogenetics Working Group (DPWG) guideline for the gene-drug interaction between CYP2C19 and CYP2D6 and SSRIs. Eur. J. Hum. Genet. 2022, 30, 1114–1120. [Google Scholar] [CrossRef]
- Hicks, J.K.; Bishop, J.R.; Sangkuhl, K.; Müller, D.J.; Ji, Y.; Leckband, S.G.; Leeder, J.S.; Graham, R.L.; Chiulli, D.L.; Llerena, A.; et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2D6 and CYP2C19 Genotypes and Dosing of Selective Serotonin Reuptake Inhibitors. Clin. Pharmacol. Ther. 2015, 98, 127–134. [Google Scholar] [CrossRef]
- CPIC® Guideline for Ondansetron and Tropisetron Based on CYP2D6 Genotype—CPIC [Internet]. Available online: https://cpicpgx.org/guidelines/guideline-for-ondansetron-and-tropisetron-and-cyp2d6-genotype/ (accessed on 15 January 2024).
- CPIC® Guideline for Tamoxifen Based on CYP2D6 Genotype—CPIC [Internet]. Available online: https://cpicpgx.org/guidelines/cpic-guideline-for-tamoxifen-based-on-cyp2d6-genotype/ (accessed on 15 January 2024).
- Brown, J.T.; Bishop, J.R.; Sangkuhl, K.; Nurmi, E.L.; Mueller, D.J.; Dinh, J.C.; Gaedigk, A.; Klein, T.E.; Caudle, K.E.; McCracken, J.T.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for Cytochrome P450 (CYP)2D6 Genotype and Atomoxetine Therapy. Clin. Pharmacol. Ther. 2019, 106, 94–102. [Google Scholar] [CrossRef]
- CPIC® Guideline for Opioids and CYP2D6, OPRM1, and COMT—CPIC [Internet]. Available online: https://cpicpgx.org/guidelines/guideline-for-codeine-and-cyp2d6/ (accessed on 15 January 2024).
- Caudle, K.E.; Sangkuhl, K.; Whirl-Carrillo, M.; Swen, J.J.; Haidar, C.E.; Klein, T.E.; Gammal, R.S.; Relling, R.V.; Scott, S.A.; Hertz, D.L.; et al. Standardizing CYP2D6 Genotype to Phenotype Translation: Consensus Recommendations from the Clinical Pharmacogenetics Implementation Consortium and Dutch Pharmacogenetics Working Group. Clin. Transl. Sci. 2020, 13, 116–124. [Google Scholar] [CrossRef]
- Pratt, V.M.; Cavallari, L.H.; Del Tredici, A.L.; Gaedigk, A.; Hachad, H.; Ji, Y.; Kalman, L.V.; Ly, R.C.; Moyer, A.M.; Scott, S.A.; et al. Recommendations for Clinical CYP2D6 Genotyping Allele Selection: A Joint Consensus Recommendation of the Association for Molecular Pathology, College of American Pathologists, Dutch Pharmacogenetics Working Group of the Royal Dutch Pharmacists Association, and the European Society for Pharmacogenomics and Personalized Therapy. J. Mol. Diagn. 2021, 23, 1047–1064. [Google Scholar]
- Auton, A.; Abecasis, G.R.; Altshuler, D.M.; Durbin, R.M.; Abecasis, G.R.; Bentley, D.R.; Chakravarti, A.; Clark, A.G.; Donnelly, P.; Eichler, E.E.; et al. A global reference for human genetic variation. Nature 2015, 526, 68–74. [Google Scholar]
- Numanagić, I.; Malikić, S.; Ford, M.; Qin Twesigomwe, D.; Wright, G.E.B.; Drögemöller, B.I.; da Rocha, J.; Lombard, Z.; Hazelhurst, S. Allelic decomposition and exact genotyping of highly polymorphic and structurally variant genes. Nat. Commun. 2018, 9, 828. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Wheeler, M.M.; Thummel, K.E.; Nickerson, D.A. Calling Star Alleles With Stargazer in 28 Pharmacogenes With Whole Genome Sequences. Clin. Pharmacol. Ther. 2019, 106, 1328–1337. [Google Scholar] [CrossRef]
- Chen, X.; Shen, F.; Gonzaludo, N.; Malhotra, A.; Rogert, C.; Taft, R.J.; Bentley, D.R.; Eberle, M.A. Cyrius: Accurate CYP2D6 genotyping using whole-genome sequencing data. Pharmacogenomics J. 2021, 21, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Twesigomwe, D.; Drögemöller, B.I.; Wright, G.E.; Siddiqui, A.; da Rocha, J.; Lombard, Z.; Hazelhurst, S. StellarPGx: A Nextflow Pipeline for Calling Star Alleles in Cytochrome P450 Genes. Clin. Pharmacol. Ther. 2021, 110, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Twesigomwe, D.; Wright, G.E.B.; Drögemöller, B.I.; da Rocha, J.; Lombard, Z.; Hazelhurst, S. A systematic comparison of pharmacogene star allele calling bioinformatics algorithms: A focus on CYP2D6 genotyping. npj Genom. Med. 2020, 5, 30. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gene | Drug(s) |
|---|---|
| COMT | Opioid |
| CYP2B6 | Efavirenz |
| CYP2C9 | Warfarin |
| CYP2C19 | Clopidogrel, Proton Pump Inhibitors (Omeprazole, Lansoprazole, Pantoprazole, and Dexlansoprazole), Selective Serotonin Reuptake Inhibitors (Citalopram, Escitalopram, and Sertraline), Tricyclic Antidepressants (Tertiary Amines Amitriptyline, Clomipramine, Doxepin, Imipramine, and Trimipramine), Voriconazole |
| CYP2D6 | Ondansetron and Tropisetron, Selective Serotonin Reuptake Inhibitors (Paroxetine and Fluvoxamine), Opioid (Codeine, Tramadol, and Hydrocodone), Atomoxetine, Tricyclic Antidepressants, Tamoxifen |
| CYP3A5 | Tacrolimus |
| CYP4F2 | Warfarin |
| DPYD | Fluoropyrimidines 5-fluorouracil |
| IL28B | PEG Interferon-α-Based Regimens |
| NUDT15 | Thiopurine |
| SLCO1B1 | Simvastatin |
| TPMT | Thiopurine (thioguanine, mercaptopurine, and azathioprine) |
| VKORC1 | Warfarin |
| CYP2D6 | CYP3A5 | DPYD | NUDT15 | TPMT | |
|---|---|---|---|---|---|
| GRCh37 | 68.17% | 92.69% | 98.80% | 97.72% | 97.40% |
| GRCh38 | 98.59% | 100% | 100% | 100% | 100% |
| GRCh38 to GRCh37 backported | 97.84% | 100% | 99.84% | 99.81% | 99.56% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yuan, D.Y.; Park, J.H.; Li, Z.; Thomas, R.; Hwang, D.M.; Fu, L. A New Cloud-Native Tool for Pharmacogenetic Analysis. Genes 2024, 15, 352. https://doi.org/10.3390/genes15030352
Yuan DY, Park JH, Li Z, Thomas R, Hwang DM, Fu L. A New Cloud-Native Tool for Pharmacogenetic Analysis. Genes. 2024; 15(3):352. https://doi.org/10.3390/genes15030352
Chicago/Turabian StyleYuan, David Yu, Jun Hyuk Park, Zhenyu Li, Rohan Thomas, David M. Hwang, and Lei Fu. 2024. "A New Cloud-Native Tool for Pharmacogenetic Analysis" Genes 15, no. 3: 352. https://doi.org/10.3390/genes15030352