
Association of CYP3A4-392A/G, CYP3A5-6986A/G, and ABCB1-3435C/T Polymorphisms with Tacrolimus Dose, Serum Concentration, and Biochemical Parameters in Mexican Patients with Kidney Transplant

 ,
,  ,
,  , ,
, ,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Polymorphisms Genotyping
2.3. TAC Quantification and Biochemical Parameter Determination
2.4. Pharmacogenetic Analysis
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Features of the Study Population
3.2. Analysis of the SNPs: CYP3A4-392A/G, CYP3A5-6986A/G, and ABCB1-3435C/T Polymorphisms
3.3. CYP3A4-392A/G, CYP3A5-6986A/G, and ABCB1-3435C/T Genotypes, TAC Concentration, and Dose
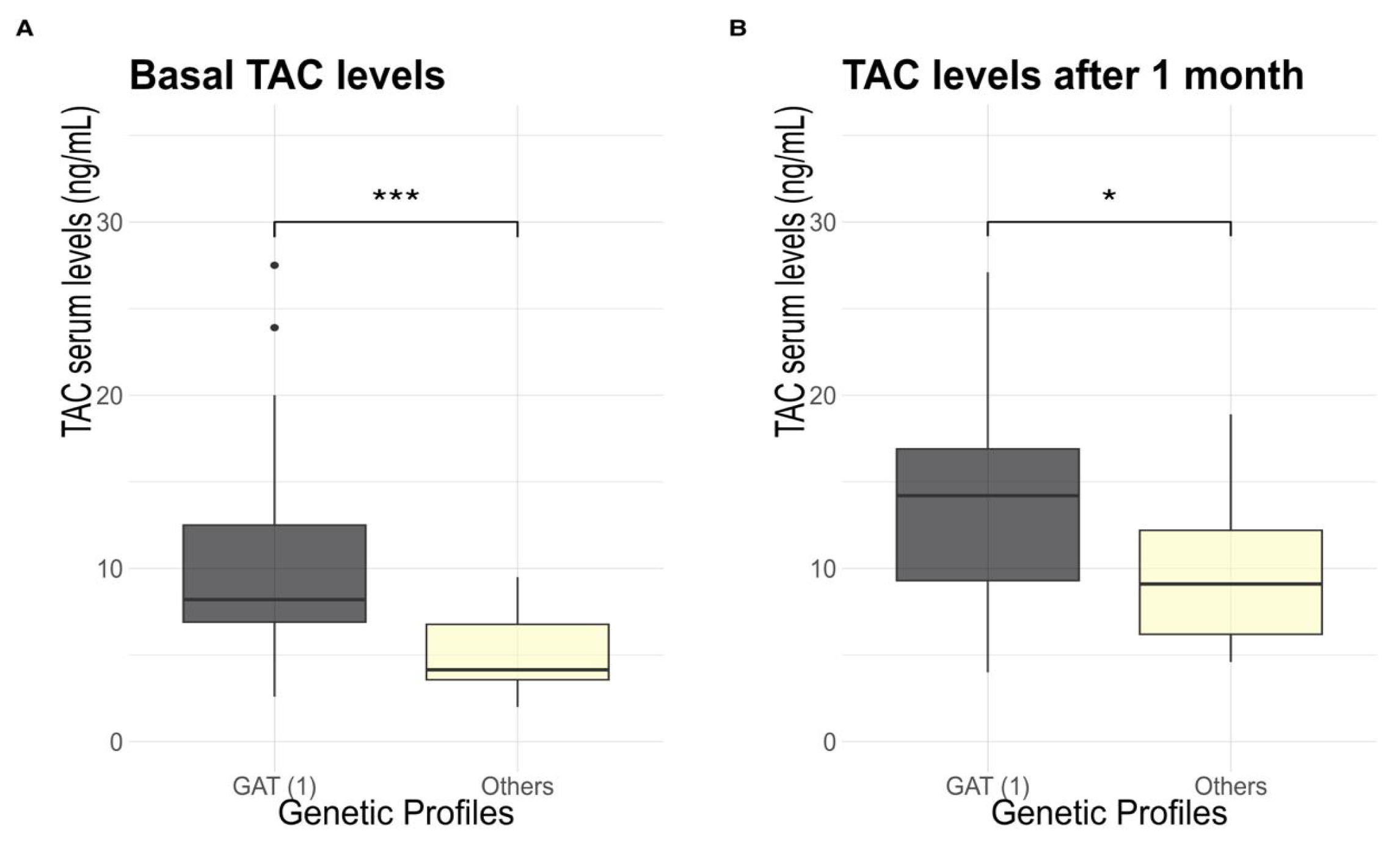
3.4. TAC Concentration and Genetic Profile
3.5. Comparison of TAC Concentration TAC Dose, Biochemical Parameters, and Concurrent Drugs at Baseline and One Month after Evolution
3.6. Assessment of the Association of Genetic and Biochemical Parameters with TAC Concentration
4. Discussion
Study Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Couser, W.; Remuzzi, G.; Mendis, S.; Tonelli, M. The contribution of chronic kidney disease to the global burden of major noncommunicable diseases. Kidney Int. 2011, 80, 1258–1270. [Google Scholar] [CrossRef] [PubMed]
- Robles-Osorio, M.L.; Sabath-Silva, E.; Sabath, E. Arsenic-mediated nephrotoxicity. Ren. Fail. 2015, 37, 542–547. [Google Scholar] [CrossRef] [PubMed]
- United States Renal Data System. Annual Data Report [Internet]. USRDS. 2022 Annual Data Report: Atlas of Chronic Kidney Disease and End Stage Renal Disease in the US, NIH, NIDDKD. Available online: https://usrds-adr.niddk.nih.gov/2022 (accessed on 24 February 2024).
- Pecoits, R.; Rosa, G.; Gonzalez, M.; Marinovich, S.; Fernandez, S.; Lugon, J.; Poblete, H.; Elgueta, S.; Gomez, R.; Cerdas, M.; et al. Renal replacement therapy in CKD: An update from the Latin American Registry of Dialysis and Transplantation. J. Bras. Nefrol. 2015, 37, 9–13, (In English/Portuguese). [Google Scholar]
- Flagg, A. Chronic Renal Therapy. Nurs. Clin. N. Am. 2018, 53, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Camilleri, B.; Pararajasingam, R.; Buttigieg, J.; Halawa, A. Immunosuppression strategies in elderly renal transplant recipients. Transplant. Rev. 2020, 34, 100529. [Google Scholar] [CrossRef]
- Szumilas, K.; Wilk, A.; Wiśniewski, P.; Gimpel, A.; Dziedziejko, V.; Kipp, M.; Pawlik, A. Current Status Regarding Immunosuppressive Treatment in Patients after Renal Transplantation. Int. J. Mol. Sci. 2023, 24, 10301. [Google Scholar] [CrossRef]
- Kapturczak, M.; Meier, H.; Kaplan, B. Pharmacology of calcineurin antagonists. Transplant. Proc. 2004, 36 (Suppl. 2), 25S–32S. [Google Scholar] [CrossRef]
- McKeon, F. When worlds collide: Immunosuppressants meet protein phosphatases. Cell 1991, 66, 823–826. [Google Scholar] [CrossRef] [PubMed]
- Hsiao, C.; Ho, M.; Ho, C.; Wu, Y.; Lee, P.; Hu, R. Long-Term Tacrolimus Blood Trough Level and Patient Survival in Adult Liver Transplantation. J. Pers. Med. 2021, 11, 90. [Google Scholar] [CrossRef]
- Wallemacq, P.; Verbeeck, R. Comparative clinical pharmacokinetics of tacrolimus in paediatric and adult patients. Clin. Pharmacokinet. 2001, 40, 283–295. [Google Scholar] [CrossRef]
- Christians, U.; Braun, F.; Schmidt, M.; Kosian, N.; Schiebel, H.; Ernst, L.; Winkler, M.; Kruse, C.; Linck, A.; Sewing, K.F. Specific and sensitive measurement of FK506 and its metabolites in blood and urine of liver-graft recipients. Clin. Chem. 1992, 38, 2025–2032. [Google Scholar] [CrossRef] [PubMed]
- Van, T.; Etsouli, O.; Moes, J.; Swen, J. Comparison of the impact of pharmacogenetic variability on the PK of slow release and immediate release tacrolimus formulations. Genes 2020, 11, 1205. [Google Scholar] [CrossRef] [PubMed]
- Cheng, F.; Li, Q.; Wang, J.; Hu, M.; Zeng, F.; Wang, Z.; Zhang, Y. Genetic polymorphisms affecting tacrolimus metabolism and the relationship to post-transplant outcomes in kidney transplant recipients. Pharmgenomics Pers. Med. 2021, 14, 1463–1474. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Huan, G.; Wang, M. Influence of CYP3A and ABCB1 Single Nucleotide Polymorphisms on the Pharmacokinetics/Pharmacodynamics of Tacrolimus in Pediatric Patients. Curr. Drug Metab. 2018, 19, 1141–1151. [Google Scholar] [CrossRef] [PubMed]
- Ebid, A.; Ismail, A.; Lotfy, N.; Mahmoud, M.; ELSharkawy, M. Influence of CYP3A4*22 and CYP3A5*3 combined genotypes on tacrolimus dose requirements in Egyptian renal transplant patients. J. Clin. Pharm. Ther. 2022, 47, 2255–2263. [Google Scholar] [CrossRef] [PubMed]
- Janssens, A.C.; Moonesinghe, R.; Yang, Q.; Steyerberg, E.W.; van Duijn, C.M.; Khoury, M.J. The impact of genotype frequencies on the clinical validity of genomic profiling for predicting common chronic diseases. Genet. Med. 2007, 9, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Favela, A.; Rangel, H.; Fricke, I.; Ortega, A.; Martínez, G.; López, M. Genetic variability among Mexican Mestizo and Amerindian populations based on three ABCB1 polymorphisms. Mol. Biol. Rep. 2018, 45, 2525–2533. [Google Scholar] [CrossRef]
- García, P.; Medeiros, M.; Reyes, H.; Rodríguez, B.; Alber, J.; Ortiz, L.; Vásquez, M.; Elizondo, G.; Morales, L.; Mancilla, E.; et al. CYP3A5 polymorphism in Mexican renal transplant recipients and its association with tacrolimus dosing. Arch. Med. Res. 2012, 43, 283–287. [Google Scholar] [CrossRef]
- MacPhee, I. Pharmacogenetic biomarkers: Cytochrome P450 3A5. Clin. Chim. Acta 2012, 413, 1312–1317. [Google Scholar] [CrossRef]
- Velickovic, R.; Mikov, M.; Catic, A.; Stefanovic, N.; Stojanovic, M.; Jokanovic, M.; Cvetkovic, T. Tacrolimus as a part of immunosuppressive treatment in kidney transplantation patients: Sex differences. Gend. Med. 2012, 9, 471–480. [Google Scholar] [CrossRef]
- Evans, E.; McLeod, H. Pharmacogenomics—Drug disposition, drug targets, and side effects. N. Engl. J. Med. 2003, 348, 538–549. [Google Scholar] [CrossRef] [PubMed]
- Hamadeh, I.; Zhang, Q.; Steuerwald, N.; Hamilton, A.; Druhan, L.; McSwain, M.; Diez, Y.; Rusin, S.; Han, Y.; Symanowski, J.; et al. Effect of CYP3A4, CYP3A5, and ABCB1 Polymorphisms on Intravenous Tacrolimus Exposure and Adverse Events in Adult Allogeneic Stem Cell Transplant Patients. Biol. Blood Marrow Transplant. 2019, 25, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Marsh, S.; King, C.R.; Van Booven, D.J.; Revollo, J.Y.; Gilman, R.H.; McLeod, H.L. Pharmacogenomic assessment of Mexican and Peruvian populations. Pharmacogenomics 2015, 16, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Miedziaszczyk, M.; Idasiak, I. Safety analysis of co-administering tacrolimus and omeprazole in renal transplant recipients—A review. Biomed. Pharmacother. 2023, 166, 115149. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.; Dykes, D.; Polesky, H. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids Res. 1988, 16, 1215. [Google Scholar] [CrossRef] [PubMed]
- Anglicheau, D.; Flamant, M.; Schlageter, M.; Martinez, F.; Cassinat, B. Pharmacokinetic interaction between corticosteroids and tacrolimus after renal transplantation. Nephrol. Dial. Transplant. 2003, 18, 2409–2414. [Google Scholar] [CrossRef] [PubMed]
- Schiff, J.; Cole, E.; Cantarovich, M. Therapeutic monitoring of calcineurin inhibitors for the nephrologist. Clin. J. Am. Soc. Nephrol. 2007, 2, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Jouve, T.; Noble, J.; Rostaing, L.; Malvezzi, P. An update on the safety of tacrolimus in kidney transplant recipients, with a focus on tacrolimus minimization. Expert Opin. Drug Saf. 2019, 18, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Cavalli, S.; Hirata, M.; Hirata, R. Detection of MboII polymorphism at the 5′ promoter region of CYP3A4. Clin. Chem. 2001, 47, 348–351. [Google Scholar] [CrossRef]
- van Schaik, R.H.N.; van der Heiden, I.P.; van den Anker, J.N.; Lindemans, J. CYP3A5 variant allele frequencies in Dutch Caucasians. Clin. Chem. 2002, 48, 1668–1671. [Google Scholar] [CrossRef]
- Sy, S.; Singh, P.; Shilbayeh, S.; Zmeili, R.; Conrado, D.; Derendorf, H. Influence of CYP3A5 6986A>G and ABCB1 3435C >T Polymorphisms on Adverse Events Associated with Tacrolimus in Jordanian Pediatric Renal Transplant Patients. Clin. Pharmacol. Drug Dev. 2013, 2, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Chen, Y.; Zhang, L.; Chen, B.; Yang, D.; Chen, W.; Zhu, P.; Fang, Z.; Chen, Z. Influence of CYP3A5, IL-10 polymorphisms and metabolism rate on tacrolimus exposure in renal post-transplant recipients. Pharmacogenomics 2022, 23, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Fathy, M.; Kamal, M.; Mohy, A.; Nabil, A. Impact of CYP3A5 and MDR-1 gene polymorphisms on the dose and level of tacrolimus among living-donor liver transplanted patients: Single center experience. Biomarkers 2016, 21, 335–341. [Google Scholar] [CrossRef] [PubMed]
- Macphee, I.; Fredericks, S.; Mohamed, M.; Moreton, M.; Carter, N.; Johnston, A.; Goldberg, L.; Holt, D. Tacrolimus pharmacogenetics: The CYP3A5*1 allele predicts low dose-normalized tacrolimus blood concentrations in whites and South Asians. Transplantation 2005, 79, 499–502. [Google Scholar] [CrossRef] [PubMed]
- Hesselink, D.A.; van Schaik, R.H.; Van Der Heiden, I.P.; van der Werf, M.; Gregoor, P.J.H.S.; Lindemans, J.; Weimar, W.; van Gelder, T. Genetic polymorphisms of the CYP3A4, CYP3A5, and MDR-1 genes and pharmacokinetics of the calcineurin inhibitors cyclosporine and tacrolimus. Clin. Pharmacol. Ther. 2003, 74, 245–254. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.; Barama, A.; Poirier, C.; Vinet, B.; Roger, M. Cyp3A4, Cyp3A5, and MDR-1 genetic influences on tacrolimus pharmacokinetics in renal transplant recipients. Pharmacogenet. Genom. 2006, 16, 659–665. [Google Scholar] [CrossRef]
- Marín, A.; Gómez, J.; Mendoza, N.; Figuera, L. Association between the Polymorphisms rs2070744, 4b/a and rs1799983 of the NOS3 Gene with Chronic Kidney Disease of Uncertain or Non-Traditional Etiology in Mexican Patients. Medicina 2023, 59, 829. [Google Scholar] [CrossRef] [PubMed]
- Wesseling, C.; Crowe, J.; Hogstedt, C.; Jakobsson, K.; Lucas, R.; Wegman, D. The epidemic of chronic kidney disease of unknown etiology in Mesoamerica: A call for interdisciplinary research and action; García, C. Importance of Pharmacogenetics and Drug-Drug Interactions in a Kidney Transplanted Patient. Am. Public Health 2013, 103, 1927–1930. [Google Scholar] [CrossRef] [PubMed]
- Staatz, C.; Tett, S. Clinical pharmacokinetics and pharmacodynamics of tacrolimus in solid organ transplantation. Clin. Pharmacokinet. 2004, 43, 623–653. [Google Scholar] [CrossRef]
- Sapir, R.; Wang, Y.; Famure, O.; Li, Y.; Kim, S. Time-dependent variability in tacrolimus trough blood levels is a risk factor for late kidney transplant failure. Kidney Int. 2014, 85, 1404–1411. [Google Scholar] [CrossRef]
- Størset, E.; Holford, N.; Midtvedt, K.; Bremer, S.; Bergan, S.; Åsberg, A. Importance of hematocrit for a tacrolimus target concentration strategy. Eur. J. Clin. Pharmacol. 2014, 70, 65–77. [Google Scholar] [CrossRef] [PubMed]
- Mourad, M.; Wallemac, P.; De Meyer, M.; Malaise, J.; De Pauw, L.; Eddour, D.; Goffin, E.; Lerut, J.; Haufroid, V. Biotransformation enzymes and drug transporters pharmacogenetics in relation to immunosuppressive drugs: Impact on pharmacokinetics and clinical outcome. Transplantation. 2008, 85 (Suppl. 7), S19–S24. [Google Scholar] [CrossRef] [PubMed]
- Katsakiori, P.; Papapetrou, E.; Goumenos, D.; Nikiforidis, G.; Flordellis, C. Investigation of clinical interaction between omeprazole and tacrolimus in CYP3A5 non-expressors, renal transplant recipients. Ther. Clin. Risk Manag. 2010, 6, 265–269. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Concha, J.; Sangüesa, E.; Saez, A.; Aznar, I.; Berenguer, N.; Saez, L.; Ribate, M. Importance of Pharmacogenetics and Drug–Drug Interactions in a Kidney Transplanted Patient. Life 2023, 13, 1627. [Google Scholar] [CrossRef] [PubMed]
- Williams, P.; Cosme, J.; Ward, A.; Angove, H.; Matak, D.; Jhoti, H. Crystal structure of human cytochrome P450 2C9 with bound warfarin. Nature 2003, 424, 464–468. [Google Scholar] [CrossRef]
- Zhao, W.; Baudouin, V.; Fakhoury, M.; Storme, T.; Deschênes, G.; Jacqz-Aigrain, E. Pharmacokinetic interaction between tacrolimus and amlodipine in a renal transplant child. Transplantation 2012, 93, e29–e30. [Google Scholar] [CrossRef]


{kind=link}
| Variables | n = 46 |
|---|---|
| Age (years) * | 29.8 ± 5.3 |
| Sex ** | |
| 36 (80) 10 (20) |
| BMI (kg/m2) * | 24.7 ± 4.1 |
| Evolution time of CKD (years) *** | 4 (2–10) |
| Etiology of CKD ** | |
| 43 (93.5) 2 (4.3) 1 (2.2) |
| RRT pre-KT ** | |
| 19 (41.3) 22 (47.8) 5 (10.9) |
| Other comorbidities ** | |
| 38 (82.6) 8 (17.4) |
| KT number ** | |
| 45 (97.8) 1 (2.2) |
| Donor type ** | |
| 34 (73.9) 6 (13.04) 6 (13.04) |
| Type of immune induction pre-KT ** | |
| 31 (67.4) 15 (32.60) |
| Maintenance immunosuppression ** | |
| 46 (100) |
| Other drugs | |
| 11 (23.9) |
| 27 (58.7) |
| SNPs | Genotype | n (%) | Allele | n (%) | n | ||||
|---|---|---|---|---|---|---|---|---|---|
| CYP3A4-392A/G | AA | 37 (82) | A | 82 (91) | 45 | ||||
| AG | 8 (18) | G | 8 (9) | ||||||
| GG | 0 | - | - | ||||||
| CYP3A5-6986A/G | AA | 0 | A | 17 (18) | 46 | ||||
| AG | 17 (37) | G | 75 (82) | ||||||
| GG | 29 (63) | - | - | ||||||
| ABCB1-3435C/T | CC | 3 (7) | C | 35 (40) | 44 | ||||
| CT | 29 (65) | T | 53 (60) | ||||||
| TT | 12 (27) | - | - | ||||||
| Genetic profile | |||||||||
| CYP3A4392 A/G | CYP3A5-6986 A/G | ABCB1-3435 C/T | n (%) | ||||||
| 1 | G | A | T | 46 (50) | |||||
| 2 | G | A | C | 24 (26) | |||||
| 3 | A | A | T | 4 (4) | |||||
| 4 | A | A | C | 9 (9) | |||||
| Others | – | – | – | 9 (9) | |||||
| Baseline Determination | One Month Later Determination | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Gene SNPs | Genotype | TAC Doses *** | p-Value | TAC Concentration *** | p-Value | TAC Doses *** | p-Value | TAC Concentration *** | p-Value |
| CYP3A4 392A/G | AA | 0.12 (0.10–0.12) | 0.98 | 8.8 (5.9–12.5) | 0.30 | 0.11 (0.06–0.17) | 0.98 | 13.90 (4.0–27.10) | 0.77 |
| AG | 0.12 (0.6–0.12) | 7.45 (4.8–10.32) | 0.12 (0.05–0.15) | 12.25 (4.60–19.10) | |||||
| GG | - | - | - | - | |||||
| CYP3A5 6986A/G | AA | - | 0.71 | - | 0.30 | - | 0.34 | - | 0.006 |
| AG | 0.12 (0.10–0.12) | 6.9 (5.0–9.5) | 0.11 (0.08–0.17) | 9.20 (4.00–27.10) | |||||
| GG | 0.12 (0.6–0.12) | 9 (7.1–12.5) | 0.11 (0.05–0.17) | 14.60 (4.60–23.90) | |||||
| ABCB1 3435C/T | CC | 0.12 (0.12–0.12) | 0.35 | 8.2 (6.6–10.7) | 0.99 | 0.10 (0.08–0.15) | 0.45 | 14.20 (6.20–15.10) | 0.79 |
| CT | 0.12 (0.6–0.12) | 8.2 (6.6–10.7) | 0.11 (0.05–0.17) | 13.90 (4.00–27.10) | |||||
| TT | 0.12 (0.10–0.12) | 9.9 (6.45–11.7) | 0.12 (0.06–0.15) | 13.75 (7.70–18.90) | |||||
| Baseline | One Month Follow-Up | p-Value | |
|---|---|---|---|
| TAC concentration (ng/dL) *** | 8.1(5.0–11.8) | 13.5 (9.0–16.8) | <0.001 |
| TAC dose (mg/kg/day) *** | 0.12(0.12–0.12) | 0.11 (0.10–0.13) | 0.619 |
| Hematocrit (%) * | 32.9 ± 6.7 | 39.5 ± 4.4 | <0.001 |
| Albumin (g/dL) * | 4.11 ± 0.5 | 4.42 ± 0.4 | 0.074 |
| Creatinine (mg/dL) * | 1.3 (1.1–1.4) | 1.01 (0.82–1.3) | <0.001 |
| Drug interaction ** | No = 16 (35) Yes = 30 (65) | No = 28 (61) Yes = 18 (39) | 0.019 |
| TAC Concentration | |||
|---|---|---|---|
| Variables | Group 1: <15 ng/dL | Group 2: >15 ng/dL | p-Value |
| CYP3A4-392A/G ** | |||
| AA | 31 (68.9) | 6 (13.3) | 0.578 a |
| AG | 8 (17.8) | 0 (0) | |
| CYP3A5-6986A/G ** | |||
| AG | 15 (32.6) | 2 (4.3) | >0.99 a |
| GG | 25 (54.3) | 4 (8.7) | |
| ABCB1-3435C/T ** | |||
| CC | 3 (6.8) | 0 (0) | 0.239 a |
| CT | 23 (52.3) | 6 (13.6) | |
| TT | 12 (27.3) | 0 (0) | |
| TAC serum (ng/dL) * concentration ** | 7.35 (5.0–10.32) | 21.95 (17.6–26.6) | <0.001 b |
| TAC dose (mg/kg/day) *** | 0.12 (0.12–0.12) | 0.12 (0.12–0.12) | 0.869 b |
| Serum creatinine (mg/dL) *** | 1.32 (1.0975–1.43) | 1.195 (1.10–1.39) | 0.935 b |
| Hematocrit (%) *** | 31.95 (27.60–36.27) | 40.75 (37.75–43.82) | 0.005 b |
| Serum albumin (g/L) *** | 4.0 (3.7–4.5) | 4.20 (4.2–4.4) | 0.371 b |
| Hypoalbuminemia ** | |||
| Yes | 3 (10) | 0 (0) | >0.99 a |
| No | 22 (73.3) | 5 (16.7) | |
| Use of drugs that elevate serum TAC concentration ** | 25 (54.3) | 5 (10.9) | 0.649 a |
| Yes | 15 (32.6) | 1 (2.2) | |
| No | |||
| One-month follow-up | |||
| CYP3A4-392A/G ** | |||
| AA | 24 (53.3) | 13 (28.9) | 0.452 a |
| AG | 4 (8.9) | 4 (8.9) | |
| CYP3A5-6986A/G ** | |||
| AG | 14 (30.4) | 3 (6.5) | 0.05 a |
| GG | 15 (32.6) | 14 (30.4) | |
| ABCB1-3435C/T ** | |||
| CC | 2 (4.5) | 1 (2.3) | >0.99 a |
| CT | 18 (40.9) | 11 (25.0) | |
| TT | 7 (15.9) | 5 (11.4) | |
| TAC serum (ng/dL concentration) *** | 8.10 (4.00–11.90) | 16.48 (12.00–27.10) | <0.001 b |
| TAC dose (mg/kg/day) *** | 0.11 (0.05–0.17) | 0.12 (0.07–0.15) | 0.598 b |
| Serum creatinine (mg/dL) * | 0.98 (±0.23) | 1.16 (±0.36) | 0.039 c |
| Hematocrit (%) * | 38.9 (±4.11) | 40.5 (±4.78) | 0.237 c |
| Serum albumin (g/L) * | 4.21 (±0.31) | 4.59 (±0.32) | 0.034 c |
| Hypoalbuminemia: | |||
| Yes | 0 (0) | 0 (0) | --- |
| No | 7 (43.75) | 9 (56.25) | |
| Use of drugs that elevate serum TAC concentration: | |||
| Yes | 8 (17.4) | 10 (21.7) | 0.060 a |
| No | 21 (45.7) | 8 (15.2) | |
| Characteristics One Month Later | Odds Ratio (OR) | 95% CI | p-Value |
|---|---|---|---|
| CYP3A5-6986A/G PM * | 4.35 | 1.13–21.90 | 0.0458 |
| CYP3A5-6986A/G PM ** | 9.32 | 1.54–93.08 | 0.028 |
| Serum creatinine (mg/dL) | 7.05 | 0.45–177.12 | 0.191 |
| Hematocrit | 1.07 | 0.90–1.28 | 0.439 |
| Drug use that increases TAC concentration ‡ | 9.53 | 1.79–88.23 | 0.018 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alatorre-Moreno, E.V.; Saldaña-Cruz, A.M.; Pérez-Guerrero, E.E.; Morán-Moguel, M.C.; Contreras-Haro, B.; López-de La Mora, D.A.; Dávalos-Rodríguez, I.P.; Marín-Medina, A.; Rivera-Cameras, A.; Balderas-Peña, L.-M.A.; et al. Association of CYP3A4-392A/G, CYP3A5-6986A/G, and ABCB1-3435C/T Polymorphisms with Tacrolimus Dose, Serum Concentration, and Biochemical Parameters in Mexican Patients with Kidney Transplant. Genes 2024, 15, 497. https://doi.org/10.3390/genes15040497
Alatorre-Moreno EV, Saldaña-Cruz AM, Pérez-Guerrero EE, Morán-Moguel MC, Contreras-Haro B, López-de La Mora DA, Dávalos-Rodríguez IP, Marín-Medina A, Rivera-Cameras A, Balderas-Peña L-MA, et al. Association of CYP3A4-392A/G, CYP3A5-6986A/G, and ABCB1-3435C/T Polymorphisms with Tacrolimus Dose, Serum Concentration, and Biochemical Parameters in Mexican Patients with Kidney Transplant. Genes. 2024; 15(4):497. https://doi.org/10.3390/genes15040497
Chicago/Turabian StyleAlatorre-Moreno, Edith Viridiana, Ana Miriam Saldaña-Cruz, Edsaúl Emilio Pérez-Guerrero, María Cristina Morán-Moguel, Betsabé Contreras-Haro, David Alejandro López-de La Mora, Ingrid Patricia Dávalos-Rodríguez, Alejandro Marín-Medina, Alicia Rivera-Cameras, Luz-Ma Adriana Balderas-Peña, and et al. 2024. "Association of CYP3A4-392A/G, CYP3A5-6986A/G, and ABCB1-3435C/T Polymorphisms with Tacrolimus Dose, Serum Concentration, and Biochemical Parameters in Mexican Patients with Kidney Transplant" Genes 15, no. 4: 497. https://doi.org/10.3390/genes15040497
APA StyleAlatorre-Moreno, E. V., Saldaña-Cruz, A. M., Pérez-Guerrero, E. E., Morán-Moguel, M. C., Contreras-Haro, B., López-de La Mora, D. A., Dávalos-Rodríguez, I. P., Marín-Medina, A., Rivera-Cameras, A., Balderas-Peña, L.-M. A., Gómez-Ramos, J. J., Cortés-Sanabria, L., & Salazar-Páramo, M. (2024). Association of CYP3A4-392A/G, CYP3A5-6986A/G, and ABCB1-3435C/T Polymorphisms with Tacrolimus Dose, Serum Concentration, and Biochemical Parameters in Mexican Patients with Kidney Transplant. Genes, 15(4), 497. https://doi.org/10.3390/genes15040497