
The Potential Health Costs of PM10 Impacts on a Gold Mine Village, during Company Liquidation: An Analysis of 2013–2017



Abstract
:1. Introduction
1.1. Wind Erosion of Tailings Storage Facilities Material (Wind-Blown Dust)
1.2. Particulate Matter and Ambient Air Quality Standards
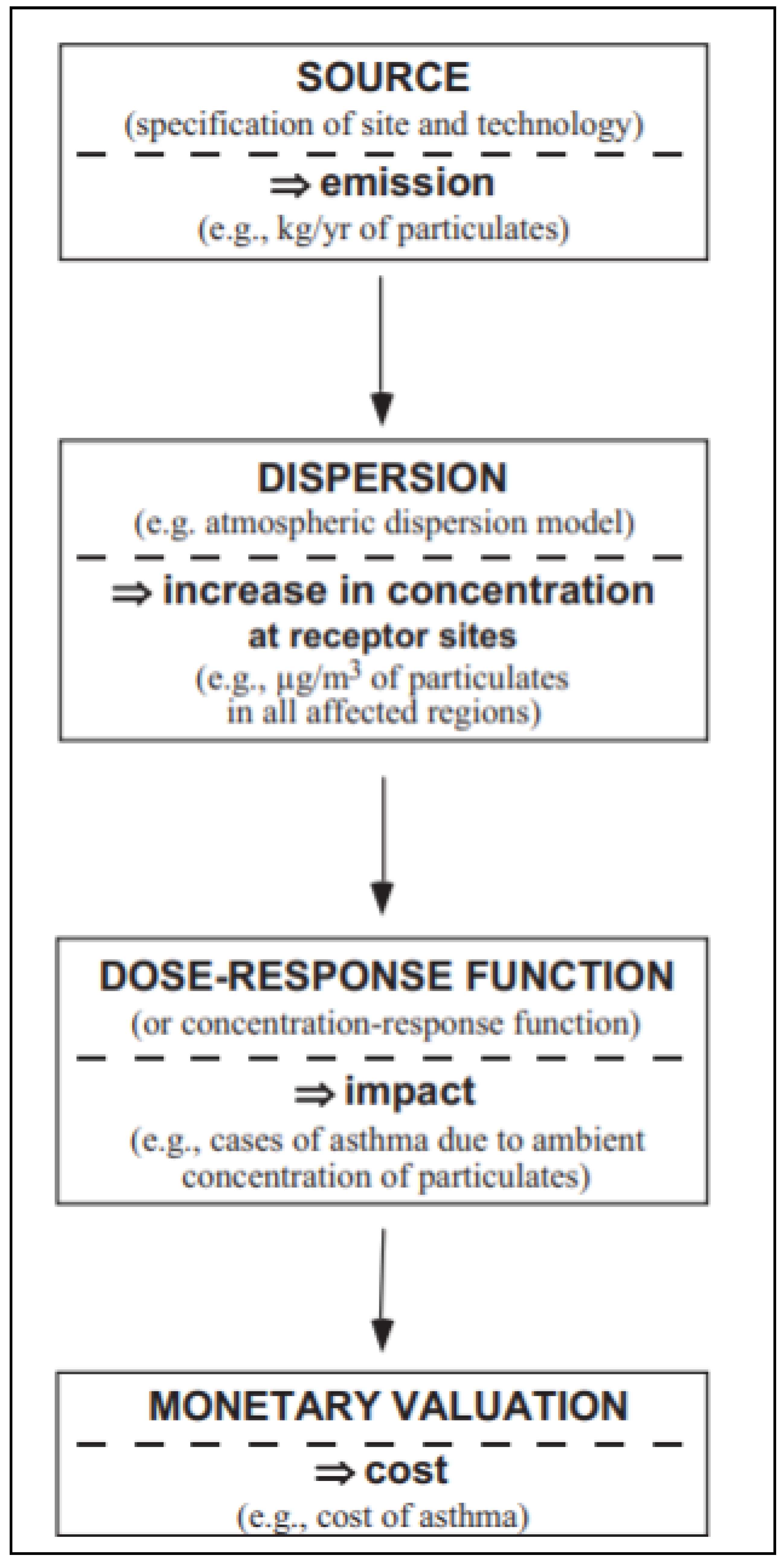
1.3. External Costs in Mining
2. Materials and Methods
- ExternE’s first principle is to employ quantitative figures and procedures in the assessment or weighting of impacts. Only quantitative algorithms can guarantee transparency and reproducibility.
- Secondly, monetary units are used to convert impacts into money. To internalize external effects with taxes, it is also important to express these effects in monetary terms.
- Impacts are evaluated based on (measured) preferences of the affected population.
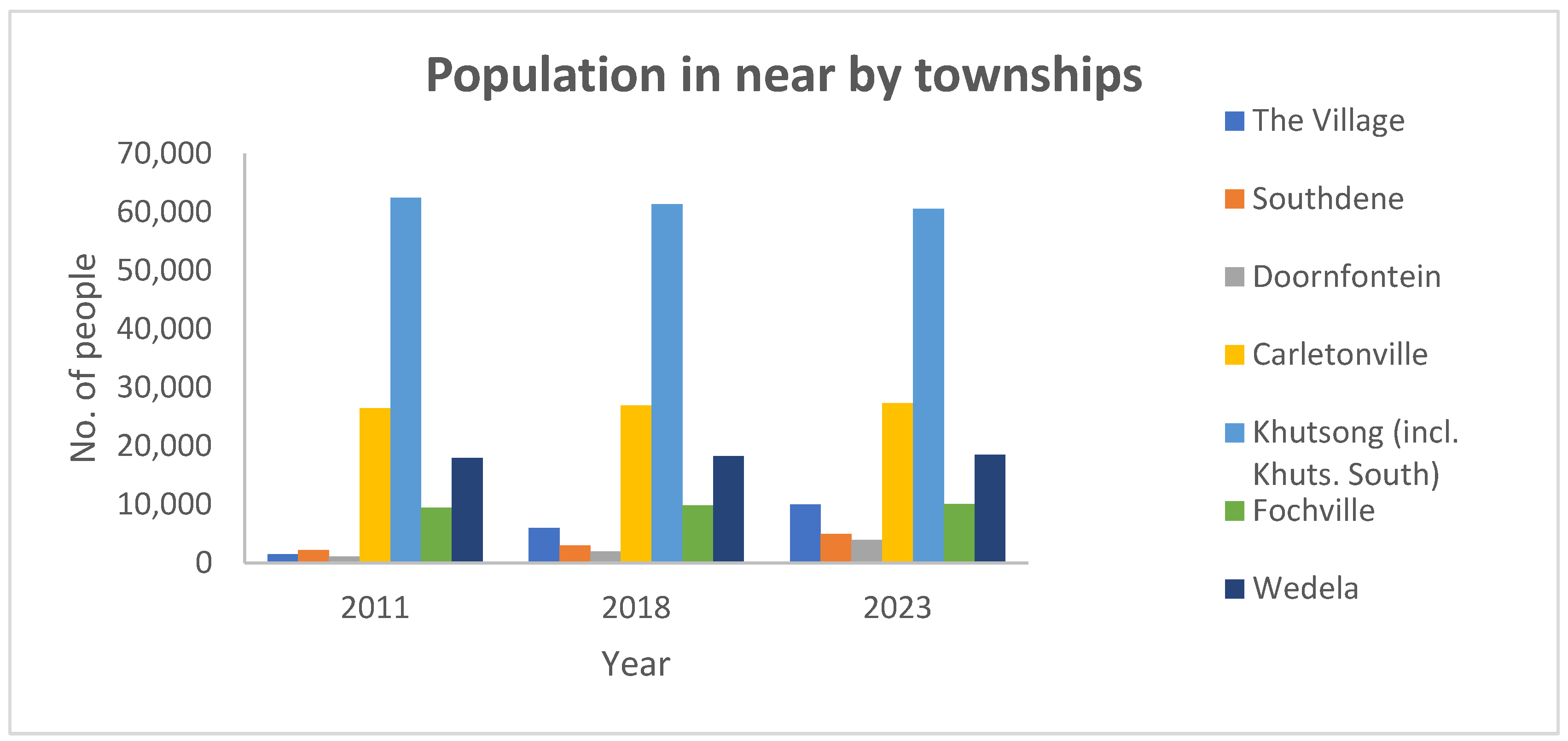
- To get meaningful results, the affected population must be interviewed. People interviewed must understand the change in utility that occurs as a result of the impact being assessed. It is important to value a damage, not a pressure or effect. In this study, the population was interviewed in 2017 to investigate their perception of the dust impacts in the area. The population size details were also verified and confirmed during the household survey process.
- The methodology should therefore be able to calculate site- and time-dependent external costs. To fully appreciate site, time, and technology dependence, a detailed bottom-up calculation is required. Calculating average or aggregate external costs can then be determined depending on the question at hand [62]. In this study, the period considered was 2013 to 2017 which coincides with the mining company liquidation period. The external costs calculated were the aggregate external costs of this period.
- AERMOD model simulations were run, and the assessment of ambient exposure of the population to particulate matter was based on these simulations.
- An assessment of the exposure to background PM concentration was conducted (below which there is thought to be no harmful health effects).
- An estimate was made of the number of people exposed to particulate matter.
- An estimate of the health effect is based on its incidence (for example, the potential underlying morbidity of the population).
- The exposure-response functions related to PM10 of the selected health effects were analyzed and used. A population is exposed to an air pollutant and the resulting health effect is determined by epidemiological studies (European Environmental Agency).
- The calculations of the health impacts for each health outcome were conducted (based on the exposed population).
- The burden of disease was calculated using the cost of illness algorithms.
2.1. Dispersion Modeling
- assuming emissions to be constant and uniform,
- the wind direction and speed to be constant,
- downwind diffusion to be negligible compared to vertical and crosswind diffusion,
- the terrain is relatively flat i.e., no crosswind barriers, no deposition or absorption of the pollutant,
- the vertical and crosswind diffusion of the pollutant follow a Gaussian distribution, while the shape of the plume can be represented by an expanding cone, and the turbulence of the plume is homogeneous.
2.1.1. Data Acquisition
2.1.2. Data Analysis
2.1.3. Model Validation
2.2. Health Impact Assessment
2.2.1. Dose-Response Function
2.2.2. Cost Analysis
3. Results and Discussions
Uncertaities in the Estimates
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Naicker, K.; Cukrowska, E.; McCarthy, T.S. Acid Mine drainage arising from gold mining activity in Johannesburg, South Africa and environs. Environ. Pollut. 2003, 122, 29–40. [Google Scholar] [CrossRef]
- Saldarriaga-Isaza, A.; Villegas-Palacio, C.; Arango, S. The public good dilemma of a non-renewable common resource: A look at the facts of artisanal gold mining Resour. Policy 2013, 38, 224–232. [Google Scholar] [CrossRef]
- Freeman, M. The Measurement of Environment and Resource Values: Theory and Methods, 2nd ed.; Resources for the Future: Washington, DC, USA, 2003. [Google Scholar]
- Ostro, B. Estimating the Health Effects of Air Pollution: A Method with an Application to Jakarta, Policy Research Working Paper 1301; World Bank Policy Research Department: Washington, DC, USA, 1994. [Google Scholar]
- Ostro, B. Outdoor Air Pollution: Assessing the Environmental Burden of Disease at National and Local Levels. In Environmental Burden of Disease Series No. 5; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Hohmeyer, O. Social Costs of Energy Consumption; Springer: Berlin, Germany, 1988. [Google Scholar]
- Hohmeyer, O. The social costs of electricity-renewables versus fossil and nuclear energy. Int. J. Sol. Energy 1992, 11, 231–250. [Google Scholar] [CrossRef]
- Ottinger, R.L.; Wooley, D.R.; Robinsson, N.A.; Hodas, D.R.; Babb, S.E. Environmental Costs of Electricity; Oceana Publications, Inc.: New York, NY, USA, 1991. [Google Scholar]
- Pearce, D.; Bann, C.; Georgiou, S. The Social Cost of Fuel Cycles, Report to the UK Department of Trade and Industry; HMSO: London, UK, 1992. [Google Scholar]
- Friedrich, R.; Voss, A. External costs of electricity generation. Energy Policy 1993, 21, 114–122. [Google Scholar] [CrossRef] [Green Version]
- McGraw-Hill Utility Data Institute. Oak Ridge National Laboratory (ORNL) and Resources for the Future (RfR) External Costs and Benefits of Fuel Cycle, Reports 2–8; McGraw-Hill Utility Data Institute: Washington, DC, USA, 1994–1998. [Google Scholar]
- Kovacevic, T.; Tomsic, Z.; Debrecin, Z. External costs of electricity: From air emissions to health damage. In Proceedings of the 12th Regional Central European Conference IUPPA and Fourth International Conference on Environmental Impact Assessment, Prague, Czech Republic, 11–14 September 2000; Section C. pp. 317–573. [Google Scholar]
- Fouquet, R.; Slade, R.; Karakoussis, V.; Gross, R.; Bauen, A.; Anderson, D. External Costs and Environmental Policy in the United Kingdom and the European Union, Occasional Paper 3; Imperial College Centre for Energy Policy and Technology: London, UK, 2001. [Google Scholar]
- Commission of the European Communities (CEC), The European Commission, 1995–2000. Luxembourg: Office for Official Publications of the European Communities, 1995. Available online: https://www.referenceforbusiness.com/encyclopedia/Clo-Con/Commission-of-the-European-Communities.html#ixzz76jOj7RXN (accessed on 6 May 2021).
- Commission of the European Communities (CEC). The European Commission. Brussels: Commission of the European Communities, 1999. Available online: https://www.referenceforbusiness.com/encyclopedia/Clo-Con/Commission-of-the-European-Communities.html#ixzz76jPXae4P (accessed on 6 May 2021).
- Office of Technology Assessment (OTA), Annual Report to the Congress: Fiscal Year 1993. Federation of American Scientists. Available online: https://ota.fas.org/otareports/year/1994a/ (accessed on 2 June 2021).
- Lee, R. Externalities Studies: Why Are the Numbers Different. In Social Costs and Sustainability: Valuation and implementation in the Energy and Transport Sector, Proceeding of the International Conference, Ladenburg, Germany, 27–30 May 1995; Hohmeyer, O., Ottinger, R.L., Rennings, K., Eds.; Springer: Berlin, Germany, 1997. [Google Scholar]
- Stirling, A. Valuing the environmental impacts of electricity production: A critical review of some “first-generation” studies. Energy Source 1998, 20, 267–300. [Google Scholar] [CrossRef]
- Schleisner, L. Comparison of methodologies for externality assessment. Energy Policy 2000, 28, 1127–1136. [Google Scholar] [CrossRef]
- Sundqvist, T. Electricity Externality Studies-Do the Numbers Make Sense? Licentiate Thesis, Lulea University of Technology, Lulea, Sweden, 2000. [Google Scholar]
- Sundqvist, T. Regulating Externalities in the Power Sector: Some Lessons from Previous Valuation Studies. Miner. Energy-Raw Mater. Rep. 2001, 16, 14–31. [Google Scholar] [CrossRef]
- Sundqvist, T.; Söderholm, P. Valuing the environmental impacts of electricity generation: A critical survey. J. Energy Lit. 2002, 2, 3–41. [Google Scholar]
- Krewitt, W. External costs of energy—Do the answers match the questions? Looking back at 10 Years of ExternE. Energy Policy 2002, 30, 839–848. [Google Scholar] [CrossRef]
- Kim, S.H. Evaluation of negative environmental impacts of electricity generation: Neoclassical and institutional approaches. Energy Policy 2006, 35, 413–423. [Google Scholar] [CrossRef]
- Burtraw, D.; Krupnick, A. The True Cost of Electric Power: An Inventory of Methodologies to Support Future Decision-making in Comparing the Cost and Competitiveness of Electricity Generation Technologies; Summary of Policymakers; Resources for the Future: Washington, DC, USA, 2012. [Google Scholar]
- Graaf Zivin, J.S.; Neidell, M.J. Environment, health and human capita. J. Econ. Lit. 2013, 51, 689–730. [Google Scholar] [CrossRef]
- Currie, I.; De Waal, J. The Bill of Rights Handbook. In Environment, 5th ed.; Juta & Company Ltd.: Cape Town, South Africa, 2005; pp. 521–530. [Google Scholar]
- Maseki, J.H. Risk Assessment of Inhaled and Ingested Airborne Particles in the Vicinity of Gold Mine Tailings: Case Study of the Witwatersrand Basin. Master’s Thesis, University of Johannesburg, Johannesburg, South Africa, 2013. [Google Scholar]
- Farmer, A.M. The effects of dust on vegetation—A review. Environ. Pollut. 1993, 79, 63–75. [Google Scholar] [CrossRef]
- Grantz, D.A.; Garner, J.H.B.; Johnson, D.W. Ecological effects of particulate matter. Environ. Int. 2003, 29, 213–239. [Google Scholar] [CrossRef]
- Martinez-Ramirez, S.; Thompson, G.E. Dry and wet deposition studies of the degradation of cement mortars. Mater. Constr. 1998, 48, 15–31. [Google Scholar]
- Petavratzi, E.; Kingman, L.; Lowndes, S. Particulates from mining operations: A review of sources, effects and regulations. Miner. Eng. 2005, 18, 1183–1199. [Google Scholar] [CrossRef]
- Mergler, D.; Anderson, H.A.; Chan, I.H.M.; Mhaffey, K.R.; Murray, M.; Sakamoto, M.; Stern, A.H. Methylmercury exposure and health effects in humans: A worldwide concern. AMBIO 2007, 36, 3–11. [Google Scholar] [CrossRef]
- Annegarn, H.J.; Surridge, A.D.; Hlapolosa, H.S.P.; Swanepoel, D.J.D.E.V.; Horne, A.R. Review of 10 years of environmental dust monitoring at Crown Mines. J. Mine Vent. Soc. S. Afr. 1991, 44, 46–50. [Google Scholar]
- Coetzee, H. Radiometric Surveying in the Vicinity of Witwatersrand Gold Mine. In Mine Closure 2008; Fourie, A.B., Tibbet, M., Weiersbye, I.M., Dye, P.J., Eds.; Australian Centre for Geomachanics: Perth, Australia, 2008; pp. 617–629. [Google Scholar]
- Amegbey, N.A.; Adimado, A.A. Incidents of cyanide spillage in Ghana. Miner. Process. Ext. Metall. 2003, 112, 126–130. [Google Scholar] [CrossRef]
- Adei, D.; Addei, I.; Kwadjosse, H.A. Study of the effects of mining activities on the health status of people: A case study. Res. J. Appl. Sci. Eng.Technol. 2011, 3, 99–104. [Google Scholar]
- Annegarn, H.J.; Grant, M.R. Direct Source Apportionment of Particulate Pollution within a Township, Final Report submitted to the Department of Minerals and Energy, Low Smoke Coal Programme; University of Witwatersrand: Johannesburg, South Africa, 1999. [Google Scholar]
- Annegarn, H.J.; Grant, M.R.; Kneen, M.A.; Scorgie, Y. Direct Source Apportionment of Particulate Pollution within a Township, Report for the Department of Minerals and Energy, Low Smoke Coal Programme; Report No. DME/2/DME-99; University of Witwatersrand: Johannesburg, South Africa, 1999. [Google Scholar]
- Bickel, P.; Friedrich, R. (Eds.) ExternE-Externalities of Energy: Methodology Update. EUR 21951; European Commission, Directorate–General for Research Sustainable Energy Systems: Luxembourg, 2005. [Google Scholar]
- Hnizdo, E.; Murray, J. Risk of pulmonary tuberculosis relative to silicosis and exposure to silica dust in South African gold miners. Occup. Environ. Med. 1998, 55, 496–502. [Google Scholar] [CrossRef] [Green Version]
- Dockery, D.W.; Pope, C.A. Acute Respiratory Effects of Particulate Air Pollution. Annu. Rev. Public Health 1994, 15, 107–132. [Google Scholar] [CrossRef]
- American Thoracic Society (ATS). Adverse effects of crystalline silica exposure: American Thoracic Society Committee of the Scientific Assembly on Environmental Occupational Health. Am. J. Res. Critic. Care Med. 1997, 155, 761–765. [Google Scholar] [CrossRef]
- Makgae, M. Key Areas in Waste Management: A South African Perspective; INTECH Open Access Publisher: London, UK, 2011. [Google Scholar]
- Wright, C.; Oosthuizen, R. PM2.5 as an Emerging Priority Pollutant in South Africa-Impacts on Human Health; Department of Environmental Affairs Directorate Information Management: Pretoria, South Africa, 2010.
- Kok, J.F.; Parteli, E.J.R.; Michaels, T.I.; Bou Karam, D. The physics of wind-blown sand and dust. Rep. Prog. Phys. 2012, 75, 106901. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Guidelines for Air Quality; World Health Organisation: Geneva, Switzerland, 2000. [Google Scholar]
- Jeong, S.J. The Impact of Air Pollution on Human Health in Suwon City. Asian J. Atmos. Environ. 2013, 7, 227–233. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Health Risks of Air Pollution in Europe—HRAPIE Project Recommendations for Concentration–Response Functions for Cost–Benefit Analysis of Particulate Matter, Ozone and Nitrogen Dioxide; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2013. [Google Scholar]
- Happo, M.; Markkanen, A.; Markkanen, P.; Jalava, P.; Kuuspalo, K.; Leskinen, A.; Sippula, O.; Lehtinen, K.; Jokiniemi, J.; Hirvonen, M.R. Seasonal variation in the toxicological properties of size-segregated indoor and outdoor air particulate matter. Toxicol. In Vitro 2013, 27, 1550–1561. [Google Scholar] [CrossRef]
- Laden, F.; Schwartz, J.; Speizer, F.E.; Dockery, D.W. Reduction in fine particulate air pollution and mortality—Extended follow-up of the Harvard six cities study. Am. J. Respir. Crit. Care Med. 2006, 173, 667–672. [Google Scholar] [CrossRef]
- Dockery, D.W.C.A.; Pope, X.; Xiping, J.; Spengler, J.; Ware, M.F.; Ferris, B.; Speizer, F. An Association between Air Pollution and Mortality in Six US Cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [Green Version]
- Pope, C.A.; Thun, M.J.; Namboodiri, M.M.; Dockery, D.W.; Evans, J.S.; Speizer, F.E.; Heath, C.W., Jr. Particulate air pollution as a predictor of mortality in a prospective study of US adults. Am. J. Respir. Crit. Care Med. 1995, 151, 669–674. [Google Scholar] [CrossRef]
- Maseki, J.; Annegarn, H. Health risk posed by enriched heavy metals (As, Cd, and Cr) in airborne particles from Witwatersrand gold tailings. J. S. Afr. Inst. Min. Met. 2017, 117, 663–669. [Google Scholar] [CrossRef]
- Ojelede, M.E.; Annegarn, H.J.; Kneen, M.A. Evaluation of aeolian emissions from gold mine tailings on the Witwatersrand. Aeol. Res. 2012, 3, 477–486. [Google Scholar] [CrossRef]
- Oguntoke, O.; Ojelede, E.M.; Annegarn, J.H. Frequency of mine dust episodes and the influence of meteorological parameters in the Witwatersrand area, South Africa. Int. J. Atmos. Sci. 2013, 2013, 128463. [Google Scholar] [CrossRef] [Green Version]
- Kneen, M.A.; Ojelede, M.E.; Annegarn, J.H. Housing and population sprawl near tailings storage facilities in the Witwatersrand: 1952 to current. S. Afr. J. Sci. 2015, 111, 11–12. [Google Scholar] [CrossRef]
- Statistics South Africa, Mid-Year Population Estimates. Statistical Release P0302, 2014. Available online: https://www.statssa.gov.za/publications/P0302/P03022014.pdf (accessed on 10 June 2021).
- Republic of South Africa. National Environmental Management: Air Quality Act No. 39 of 2004: Draft National Dust Control Regulations, Government Gazette No.35931; Republic of South Africa: Cape Town, South Africa, 7 December 2012. [Google Scholar]
- Republic of South Africa. National Environmental Management: Air Quality Act No. 39 of 2004: National Ambient Air Quality Standard, Government Gazette Vol 486 No.35463; Republic of South Africa: Cape Town, South Africa, 24 December 2009. [Google Scholar]
- FRIDGE. Bentley West Management Consultants (Pty) Ltd. and Airshed Planning Professionals (Pty) Ltd. 2004: Study to Examine the Potential Socio-Economic Impact of Measures to Reduce Air Pollution from Combustion; Final Report 2004 for the Fund for Research into Industrial; Development Growth and Equity (FRIDGE), NEDLAC Trade and Industry Chamber: Johannesburg, South Africa, 2004. [Google Scholar]
- Papagiannis, A.; Roussos, D.; Menegaki, M.; Damigos, D. Externalities from lignite mining-related dust emissions. Energy Policy 2014, 74, 414–442. [Google Scholar] [CrossRef]
- Pizzol, M.; Weidema, B.; Brandão, M.; Osset, P. Monetary valuation in life cycle assessment: A review. J. Clean. Prod. 2015, 86, 170–179. [Google Scholar] [CrossRef]
- Othman, J.; Sahani, M.; Mahmud, M.; Sheikh Ahmad, M.K. Transboundary smoke haze pollution in Malaysia: Inpatient health impacts and economic valuation. Environ. Pollut. 2014, 189, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Tian, H.; Cheng, K.; Lu, L.; Zheng, M.; Wang, S.; Hao, J.; Wang, K.; Hua, S.; Zhu, C. The variation of chemical characteristics of PM2.5 and PM10 and formation causes during two haze pollution events in urban Beijing, China. Atmos. Environ. 2015, 107, 1–8. [Google Scholar] [CrossRef]
- Hou, Q.; An, X.; Wang, Y.; Tao, Y.; Sun, Z. An assessment of China’s PM10-related health economic losses in 2009. Sci. Total Environ. 2012, 435–436, 61–65. [Google Scholar] [CrossRef]
- Kan, H.; Chen, B. Particulate air pollution in urban areas of Shanghai, China: Health-based economic assessment. Sci. Total Environ. 2004, 322, 71–79. [Google Scholar] [CrossRef]
- Zhang, D.; Aunan, K.; Martin Seip, H.; Larssen, S.; Liu, J.; Zhang, D. The assessment of health damage caused by air pollution and its implication for policy making in Taiyuan, Shanxi, China. Energy Policy 2010, 38, 491–502. [Google Scholar] [CrossRef] [Green Version]
- Van Horen, C. Counting the Social Costs: Electricity and Externalities in South Africa; Juta Academic: Cape Town, South Africa, 1997. [Google Scholar]
- Kunzli, N.; Kaiser, R.; Medina, S. Public Health impact of outdoor and traffic-related air pollution: A European assessment. Lancet 2001, 356, 795–801. [Google Scholar] [CrossRef]
- Nelson, C.D. The Public Health Impacts of Particulate Emissions from Coal-fired Power Plants in Minnesota. Master’s Thesis, Faculty of the Graduate School, University of Minnesota, Saint Anthony Falls, MN, USA, October 2000. [Google Scholar]
- Holland, M.; Watkiss, P. BeTa-Benefits Table Database: Estimates of the Marginal External Costs of Air Pollution in Europe. Created for European Commission DG Environment by Netcen; European Commission DG Environment: Copenhagen, Denmark, 2002. [Google Scholar]
- World Bank and International Finance Corporation, It’s Not over When it’s Over: Mine Closure around the World. 2002. Available online: http://siteresources.worldbank.org/INTOGMC/Resources/notoverwhenover.pdf (accessed on 10 May 2020).
- Wang, X.; Mauzerall, D.L. Evaluating impacts of air pollution in China on public health: Implications for future air pollution and energy policies. Atmos. Environ. 2006, 40, 1706–1721. [Google Scholar] [CrossRef]
- Willis, K.G.; Garrod, G.D. Externalities from extraction of aggregates regulation by tax or land-use controls. Resour. Policy 1999, 25, 77–86. [Google Scholar] [CrossRef]
- Bui, L.T.; Nguyen, P.H.; Nguyen, D.C.M. Model for assessing health damage from air pollution in quarrying area e case study at Tan Uyen quarry. Ho Chi Minh megapolis, Vietnam. Heliyon 2020, 6, e05045. [Google Scholar] [CrossRef]
- Mpanza, M.; Adam, E.; Moolla, R. Dust Deposition Impacts at a Liquidated Gold Mine Village: Gauteng Province in South Africa. Int. J. Environ. Res. Public Health 2020, 17, 4929. [Google Scholar] [CrossRef]
- Quah, E.; Boon, T.L. The economic cost of particulate air pollution on health in Singapore. J. Asian Econ. 2003, 14, 73–90. [Google Scholar] [CrossRef]
- Blyvoor Gold Capital. Environmental Management Programme Report for the Blyvooruitzicht and Doornfontein Mine. EMP Rep. 2018, unpublished. [Google Scholar]
- Mpanza, M.; Adam, E.; Moolla, R. Perceptions of external costs of dust fallout from gold mine tailings: West Wits Basin. Clean Air J. 2020, 30, 52–63. [Google Scholar] [CrossRef]
- Lawyers for Human Rights (LHR). Blyvooruitzicht Mine Village: The Human Toll of State and Corporate Abdication of Responsibility in South Africa. 2017. Available online: http://www.lhr.org.za/ (accessed on 3 April 2021).
- Maddison, D.A. Meta-Analysis of Air Pollution Epidemiological Studies; Centre for Social and Economic Research on the Global Environment: London, UK; University College London: London, UK; University of East Anglia: Norwich, UK, 1997. [Google Scholar]
- World Health Organization (WHO). Review of Evidence on Health of Air Pollution-REVIHAAP Project Technical Report; World Health Organization: Bonn, Germany, 2013; Available online: www.euro.eho.int/_data/assets/pdf_file/0004/193108/REVIHAAP-Final-technical-report-final-version.pdf (accessed on 10 June 2021).
- Rowe, R.D.; Lang, C.M.; Chesnut, L.G.; Latimer, D.A.; Rae, D.; Bernow, S.M.; White, D.E. New York State Environmental Externalities Cost Study; Empire State Electric Energy Research Corporation: New York, NY, USA, 1996. [Google Scholar]
- Schwartz, J.; Slater, D.; Larson, T.; Pierson, W.; Koening, J. Particulate air pollution and hospital emergency room visits for asthma in Seattle. Am. Rev. Respir. Dis. 1993, 174, 826–883. [Google Scholar] [CrossRef]
- Schwartz, J.; Zanobette, A.; Bateson, T. Revised Analysis of the National Morbidity, Mortality and Air Pollution Study: Morbidity and Mortality among Elderly Residents of Cities with Daily PM Measurements; Health Effects Institute: Baltimore, MD, USA, 2005. [Google Scholar]
- Xu, Z.; Yu, D.; Jing, L.; Xu, X. Air pollution and daily mortality in Shenyang, China. Arch. Environ. Health Int. J. 2000, 55, 115–120. [Google Scholar] [CrossRef]
- Pope, C.A. Synoptic weather modeling and estimates of the exposure-response relationship between daily mortality and particulate air pollution. Environ. Health Perspect. 1996, 104, 414–420. [Google Scholar] [CrossRef]
- Dixon, J.A.; Scura, L.F.; Carpenter, R.A.; Sherman, P.B. Economic Analysis of Environmental Impacts, New Edition; Earthscan Publications Ltd.: London, UK, 2013. [Google Scholar]
- University of Cape Town. Socio-Economic Impact of Air pollution Reduction Meausres Task 5b, Socio-economic Impacts Associated with Prioritised Options, Report Compiled in Collaboration with Bentley West Management Consultants on Behalf of National Economic Development and Labour Council (NEDLAC) under the Fund for Research into Industrial Growth and Equity (FRIDGE); University of Cape Town: Cape Town, South Africa, 2004. [Google Scholar]
- Scorgie, Y.; Burger, L.W.; Annegarn, H.J. Socio-Economic Impact of Air Pollution Reduction Measures—Task 2: Establishment of Source Inventories, and Task 3: Identification and Prioritisation of Technology Options; Report compiled on behalf of NEDLAC under the Fund for Research into Industrial Growth and Equity; Airshed Planning Professionals: Midrand, South Africa, 25 June 2003. [Google Scholar]
- Western Cape Government: Department of Health. Western Cape Government Hospital Tariffs: UPFS Fee Schedule for Full Paying Patients (Externally Funded, Foreigners, RGP and Patients with Private Doctor Incl). Available online: https://www.westerncape.gov.za/assets/departments/health/annexure_a3_externally_funded_april_2014.pdf (accessed on 10 June 2021).
- Yin, H.; Xu, L.; Cai, Y. Monetary Valuation of PM10-Related Health Risks in Beijing China: The Necessity for PM10 Pollution Indemnity. Int. J. Environ. Res. Public Health 2015, 12, 1660–4601. [Google Scholar] [CrossRef] [Green Version]
- Zhou, M.; Liu, Y.; Wang, I.; Kuang, X.; Xu, X.; Kan, H. Particulate air pollution and mortality in a cohort of Chinese men. Environ. Pollut. 2014, 186, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Khaniabadi, Y.O.; Daryanoosh, S.M.; Amrane, A.; Polosa, R.; Hopke, P.K.; Goudarzi, G.; Mohammadi, M.J.; Sicard, P.; Armin, H. Impact of Middle Eastern Dust storms on human health. Atmos. Poll. Res. 2017, 8, 606–613. [Google Scholar] [CrossRef]
- Nurmagambetov, T.; Kuwahara, R.; Garbe, P. The Economic Burden of Asthma in the United States, 2008–2013; Division of Environmental Hazards and Health Effects, National Center for Environmental Health, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2013. Available online: https://pubmed.ncbi.nlm.nih.gov/29323930/ (accessed on 21 July 2021). [CrossRef]
- Krewski, D.; Burnett, R.T.; Goldberg, M.S.; Hoover, K.; Siemiatycki, J.; Abrahamowicz, M.; White, W.H. Health Effects Institute Reanalysis of the Havard Six Cities Study and the American Cancer Society Study of Particulate Air Pollution and Mortality; A special Report of the Institute’s Particle Epidemiology Reanalysis Project; Health Effects Institute: Cambridge, MA, USA; North Andover, MA, USA, 2000. [Google Scholar]
- Scorgie, Y.; Paterson, G.; Burger, L.W.; Annergarn, H.J.; Kneen, M.A. Socio-Economic Impact of Air Pollution Reduction Measures-Task 4a Supplementary Report: Quantification of Health Report: Quantification of Health Risks and Associated Costs Due to Fuel Burning Source Groups, Report Compiled on behalf of National Economic Development and Labour Council (NEDLAC) under the Fund For Research into Industrial Growth and Equity (FRIDGE); Airshed Planning Professionals Pty Ltd.: Midrand, South Africa, 2004. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
| Source | Daily Average (µg/m3) | Annual Average (%) |
|---|---|---|
| South Africa | 75 | 40 |
| WHO | 50 | 20 |
| FRIDGE | 25 | 15 |
| Health Effect | Function | Population Sector | Source |
|---|---|---|---|
| Respiratory hospital admissions-daily exposures | 1.2 × 10−5 1.39 × 10−5 | All persons | Ostro [4] FRIDGE [61] |
| Respiratory symptoms | 1.83 × 10−1 | All persons | Ostro [4] |
| Restricted activity days (RAD)-annual average | 5.75 × 10−2 | Adults | Ostro [4] |
| Restricted activity days (RAD)-daily exposures | 1.60 × 10−4 | Adults | Rowe et al. [3] |
| Asthma attacks | 6.5 × 10−3 | Asthmatics | Maddison [82] |
| Cardiovascular hospital admissions-daily exposures | 1.01 × 10−7 | All persons | Dockery et al. [2] |
| Health End Point | Period | Health Impact Wedela | Health Impact Gold Mine Village |
|---|---|---|---|
| Respiratory hospital admin | Short-term | 5.47 | 0.36 |
| Cardiovascular hospital admin | Short-term | 0.046 | 0.0030 |
| Restricted activity days (RAD) | Short-term | 73 | 4.8 |
| Asthma attacks | Short-term | 296 | 19.5 |
| Respiratory symptoms | Short-term | 83,470 | 549 |
| Health Endpoint | Gold Mine Village | Gold Mine Village | Wedela | Wedela |
|---|---|---|---|---|
| Cost (R) and ($) with impact daily 75 µg/m3 (NAAQS) | Cost (R) and ($) with impact daily 25 µg/m3 (FRIDGE) | Cost (R) and ($) with impact daily 75 µg/m3 (NAAQS) | Cost (R) and ($) with impact 25 µg/m3 (FRIDGE) | |
| Asthma treatment | R 75,804 $939,534 1,195,909.753 | R 833,847 $10,334,917 | R 1,152,541 $14,284,893 | R 3,457,624 $4,285,469 |
| Respiratory illness private inpatient clients | R 9012 $111,697 | R 99,130 $1,228,643 | R 137,017 $1,698,224 | R 411,051 $5,094,673 |
| Respiratory illness public inpatient clients | R 6309 $78,195 | R 69,395 $860,100 | R 95,918 $1,188,833 | R 287,753 $3,566,485 |
| Respiratory illness private outpatient clients | R 954 $11,824 | R 10,492 $130,041 | R 14,502 $179,742 | R 43,507 $539,237 |
| Respiratory illness public outpatient clients | R 668 $8279 | R 7349 $91,085 | R 10,157 $125,888 | R 30,472 $377,678 |
| Restricted activity days (RAD) | R 3742 $46,379 | R 41,159 $510,135 | R 4,053,399 $50,238,881 | R 60,800,982 $753,583,179 |
| Total (R) | 96,488 | 1,061,372 | 5,463,534 | 65,031,388 |
| Health End Point | Costs (R) and ($) Estimated for 2013 | Cost ($) from Other Countries | Source |
|---|---|---|---|
| Hospital admission (average length stay 4.37 days) private | R 23,740 $245,384 | Beijing, China [89] 2705.81 (2011) 2761.04 (2012) USA [89] 7600 (2012) | FRIDGE, [61] |
| Asthma treatment cost per annum (average length stay 6.9 days) | R 1900 $19,638 | Beijing, China [93] 346.13 (2011) 372.36 (2012) USA [89] 3266 (2013) | FRIDGE, [61] |
| Respiratory illness Private inpatients | R 12,235 $126,462 | USA [89] 393 (2013) | FRIDGE, [61] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mpanza, M.; Adam, E.; Moolla, R. The Potential Health Costs of PM10 Impacts on a Gold Mine Village, during Company Liquidation: An Analysis of 2013–2017. Minerals 2022, 12, 169. https://doi.org/10.3390/min12020169
Mpanza M, Adam E, Moolla R. The Potential Health Costs of PM10 Impacts on a Gold Mine Village, during Company Liquidation: An Analysis of 2013–2017. Minerals. 2022; 12(2):169. https://doi.org/10.3390/min12020169
Chicago/Turabian StyleMpanza, Mbalenhle, Elhadi Adam, and Raeesa Moolla. 2022. "The Potential Health Costs of PM10 Impacts on a Gold Mine Village, during Company Liquidation: An Analysis of 2013–2017" Minerals 12, no. 2: 169. https://doi.org/10.3390/min12020169