
A Task Allocation Approach of Multi-Heterogeneous Robot System for Elderly Care


Abstract
:1. Introduction
- (1)
- A novel MHRS and its self-organizing architecture covering most nursing scenes of elderly care is proposed, which contributes to a comprehensive smart home for elderly care.
- (2)
- An MRTA algorithm of MHRS is proposed for elderly care, which can achieve safe adaptive cooperation, multi-priority task planning, and emergency task calling.
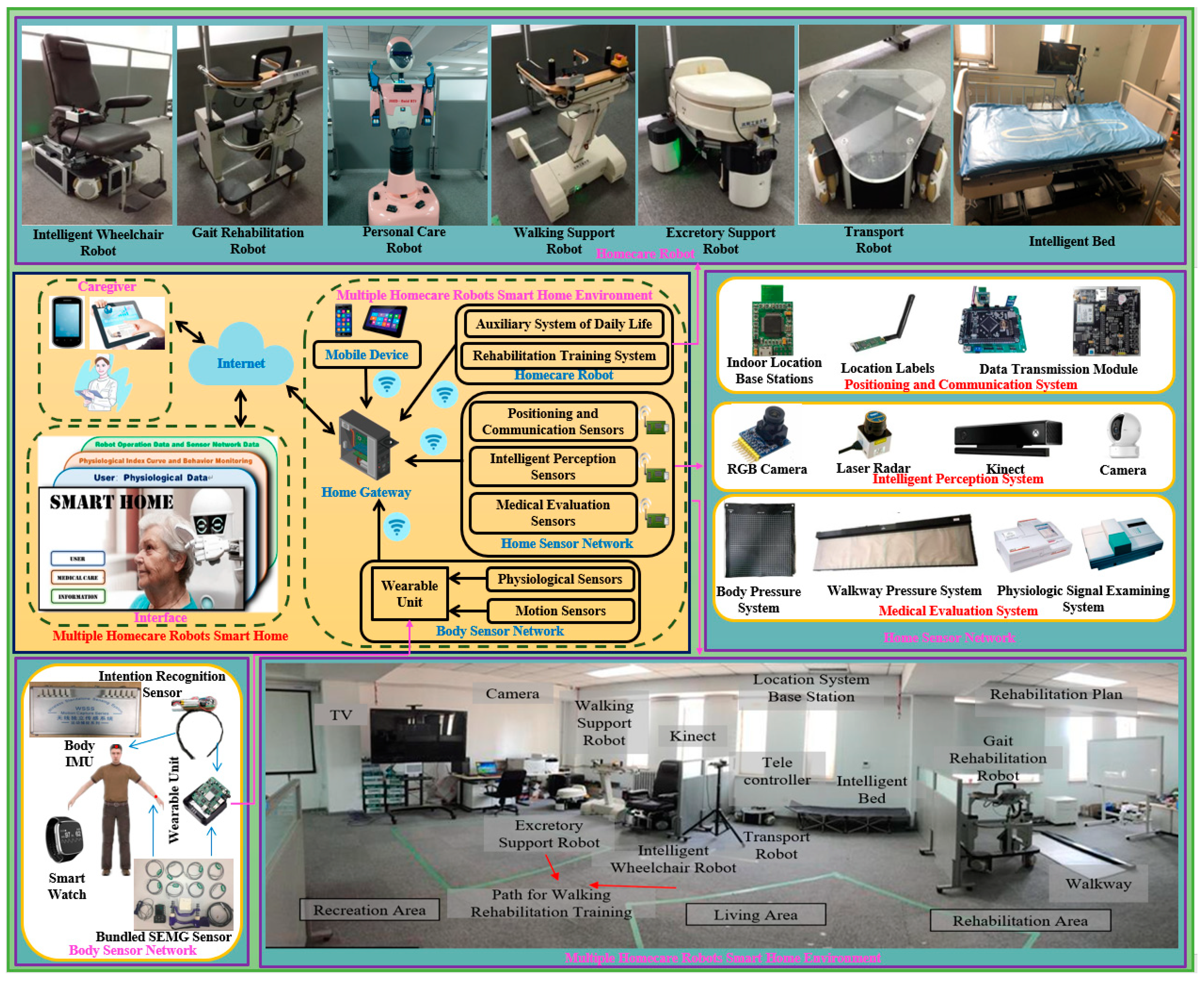
2. Smart Home for Elderly Care
2.1. Heterogeneity of Robots
2.2. The Architecture of MHRS
3. Multi-Robot Task Allocation Algorithm
3.1. Task Model
3.2. Problem Statement
3.3. Communication System and Time Synchronization
3.4. Bid Calculation
3.5. Task Allocation Process
4. Experimental Results
4.1. Performance Comparison of the CBBA and DBPAE in Simulated Environment
- (1)
- The bidding algorithm takes the energy consumption of the system and the waiting time of users as the bidding value. It contributes to the central control center completing the task allocation on the premise of not consuming too much energy.
- (2)
- A dynamic bidding mechanism is established. Each robot needs to bid for the next task combined with the current status. These calculation processes are carried out inside each robot and in parallel with the tasks being performed by the robot. It also contributes to reducing the time of abandoning a current task and re-planning a task. Particularly in DBPAE, if there are no new emergency tasks, new tasks are dynamically added for future allocation. When emergency priority tasks appear, new assignments are forced by deleting the current tasks of robots performing lower priority tasks. However, in CBBA, to assign newly determined tasks, some of which may be emergency tasks, replanning of tasks that must be performed leads to further delay in overall execution.
- (3)
- The high computational requirements of handling many robots can be better satisfied by our proposed DBPAE. Compared with the traditional centralized task planning or multi-objective task allocation methods, it greatly reduces the amount of calculation for centralized task allocation center.
4.2. Simulation of Emergency Task
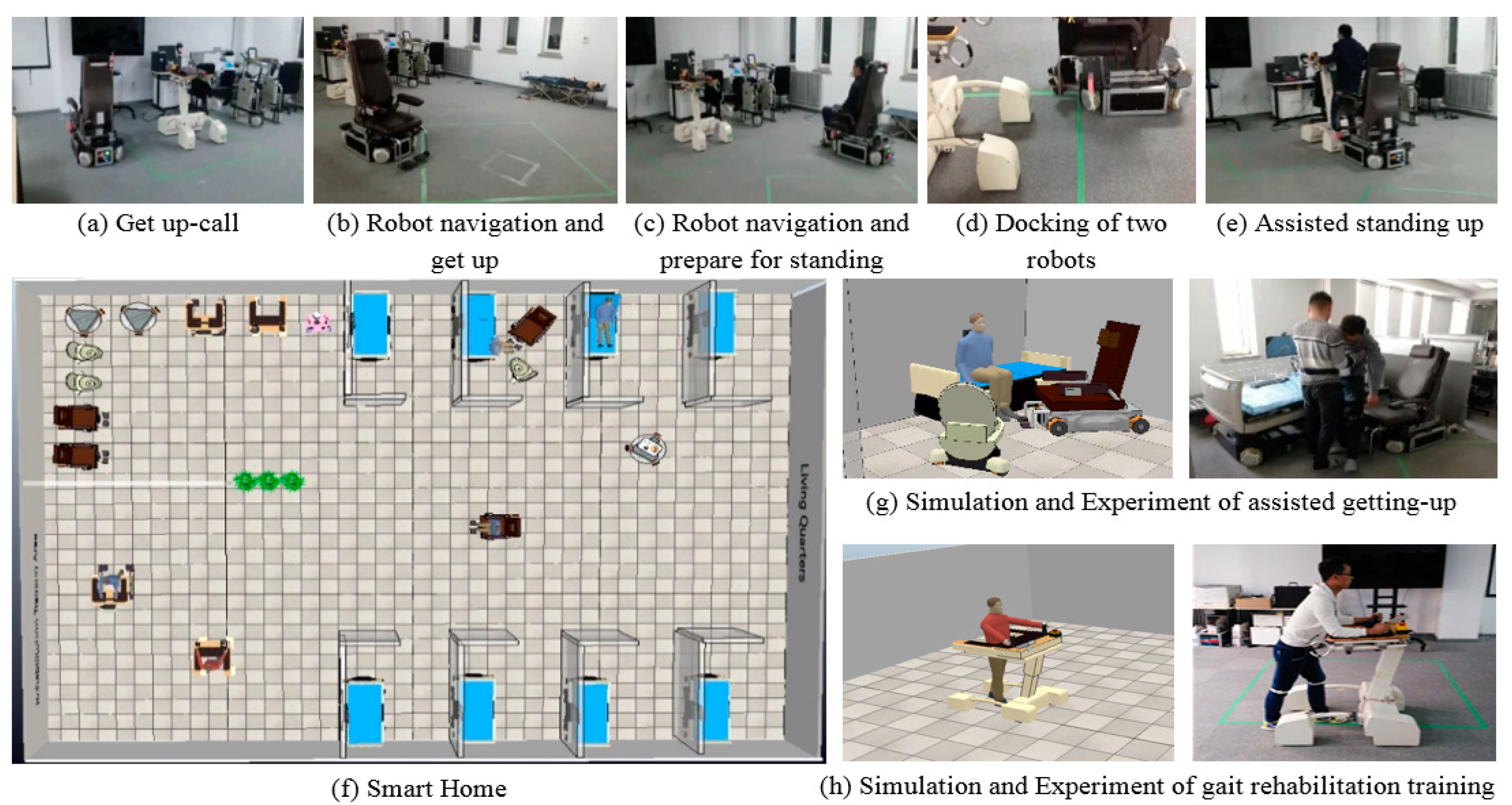
4.3. Experiments on Real Robotics
4.3.1. Continuous Task Assistance by DBPAE
4.3.2. Multi-Robot Cooperative Task in Distributed Execution Layer
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
References
- Monika, N. Aging of population with trends in social development taken into account. In Proceedings of the SHS Web of Conferences, online, 16 December 2021; Volume 129. [Google Scholar] [CrossRef]
- Wang, N.; Gao, W.; Ma, M.; Shan, L.; Fu, X.; Sun, T.; Xia, Q.; Tian, W.; Liu, L.; Yang, H.; et al. The medical insurance system’s weakness to provide economic protection for vulnerable citizens in China: A five-year longitudinal study. Arch. Gerontol. Geriatr. 2020, 92, 104227. [Google Scholar] [CrossRef] [PubMed]
- Chen, L. Population Aging and Health Care Services: What Governments Should Do. Arch. Gerontol. Geriatr. 2021, 92, 104296. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.; Campos, G.; Enríquez, V.; Miranda, A.; Rodriguez, F.; Ponce, H. Nurse-Bot: A robot system applied to medical assistance. In Proceedings of the 2018 International Conference on Mechatronics, Electronics and Automotive Engineering (ICMEAE), Cuernavaca, Mexico, 26–29 November 2018; pp. 56–59. [Google Scholar]
- Ahamed, A.; Ahmed, R.; Hossain, M.I.; Hossain, S.; Alam, S.; Banna, H. Design and implementation of a nursing robot for old or paralyzed person. In Proceedings of the 2020 IEEE Region 10 Symposium (TENSYMP), Dhaka, Bangladesh, 5–7 June 2020; pp. 594–597. [Google Scholar]
- Yanagihara, H.; Kojima, K. Development of transfer assist robot adapted to body sizes of care-recipients. In Proceedings of the 2022 IEEE 4th Global Conference on Life Sciences and Technologies (LifeTech), Osaka, Japan, 7–9 March 2022; pp. 26–27. [Google Scholar]
- Allaban, A.A.; Wang, M.; Padir, T. A systematic review of robotics research in support of in-home care for older adults. Information 2020, 11, 75. [Google Scholar] [CrossRef] [Green Version]
- Sun, Q.; Yu, W.; Kochurov, N.; Hao, Q.; Hu, F. A multi-agent-based intelligent sensor and actuator network design for smart house and home automation. J. Sens. Actuator Netw. 2013, 2, 557–588. [Google Scholar] [CrossRef]
- Mekuria, D.N.; Sernani, P.; Falcionelli, N.; Dragoni, A.F. Reasoning in multi-agent based smart homes: A systematic literature review. In Italian Forum of Ambient Assisted Living 2018; Springer: Cham, Switzerland, 2019; Volume 544, pp. 161–179. [Google Scholar] [CrossRef]
- Roda, C.; Rodríguez, A.; López-Jaquero, V.; González, P.; Navarro, E. A multi-agent system in ambient intelligence for the physical rehabilitation of older people. In Trends in Practical Applications of Agents, Multi-Agent Systems and Sustainability; Springer: Cham, Switzerland, 2015; Volume 372, pp. 113–123. [Google Scholar] [CrossRef]
- Pal, D.; Triyason, T.; Funilkul, S.; Chutimaskul, W. Smart homes and quality of life for the elderly: Perspective of competing models. IEEE Access 2018, 6, 8109–8122. [Google Scholar] [CrossRef]
- Zavalyshyn, I.; Legay, A.; Rath, A.; Riviére, E. Smart home care: Towards supporting elderlies in the comfort and safety of their homes. In Proceedings of the 2021 10th Latin-American Symposium on Dependable Computing (LADC), Florianópolis, Brazil, 22–26 November 2021; pp. 1–6. [Google Scholar]
- Waibel, M.; Beetz, M.; Civera, J.; D’Andrea, R.; Elfring, J.; Gálvez-López, D.; Haussermann, K.; Janssen, D.; Montiel, J.M.M.; Perzylo, A.; et al. RoboEarth. IEEE Robot. Autom. Mag. 2011, 18, 69–82. [Google Scholar] [CrossRef] [Green Version]
- Mohd, N.N.S.; Mizukawa, M. Robotic services at home: An initialization system based on robots’ information and user preferences in unknown environments. Int. J. Adv. Robot. Syst. 2013, 11, 112. [Google Scholar] [CrossRef]
- Park, K.H.; Bien, Z.; Lee, J.J.; Kim, B.K.; Lim, J.T.; Kim, J.D.; Lee, H.; Kim, D.J.; Jung, J.W.; Do, J.H.; et al. Robotic smart house to assist people with movement disabilities. Auton. Robot. 2007, 22, 183–198. [Google Scholar] [CrossRef]
- Zhang, Y.; Tian, G.; Chen, H. Exploring the cognitive process for service task in smart home: A robot service mechanism. Future Gener. Comp. Syst. 2020, 102, 588–602. [Google Scholar] [CrossRef]
- Cavallo, F.; Limosani, R.; Manzi, A.; Bonaccorsi, M.; Esposito, R.; Rocco, M.D.; Pecora, F.; Teti, G.; Saffiotti, A.; Dario, P. Development of a socially believable multi-robot solution from town to home. Cogn. Comput. 2014, 6, 954–967. [Google Scholar] [CrossRef] [Green Version]
- Saffiotti, A.; Broxvall, M.; Gritti, M.; LeBlanc, K.; Lundh, R.; Rashid, J.; Seo, B.S.; Cho, Y.J. The PEIS-Ecology project: Vision and results. In Proceedings of the 2018 IEEE/RSJ International Conference on Intelligent Robots and Systems, Nice, France, 22–26 September 2008; pp. 2329–2335. [Google Scholar]
- Chen, M.; Ma, Y.; Ullah, S.; Cai, W.; Song, E. ROCHAS: Robotics and cloud-assisted healthcare system for empty nester. In Proceedings of the 8th International Conference on Body Area Networks ICST (Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering), Boston, MA, USA, 30 September–2 October 2013; pp. 217–220. [Google Scholar]
- Torta, E.; Werner, F.; Johnson, D.O.; Juola, J.F.; Cuijpers, R.H.; Bazzani, M.; Oberzaucher, J.; Lemberger, J.; Lewy, H.; Bregman, J. Evaluation of a small socially-assistive humanoid robot in intelligent homes for the care of the elderly. J. Intell. Robot. Syst. 2013, 76, 57–71. [Google Scholar] [CrossRef]
- Pyo, Y.; Nakashima, K.; Kuwahata, S.; Kurazume, R.; Tsuji, T.; Morooka, K.; Hasegawa, T. Service robot system with an informationally structured environment. Robot. Auton. Syst. 2015, 74, 148–165. [Google Scholar] [CrossRef] [Green Version]
- Do, H.M.; Pham, M.; Sheng, W.; Yang, D.; Liu, M. RiSH: A robot-integrated smart home for elderly care. Robot. Auton. Syst. 2018, 101, 74–92. [Google Scholar] [CrossRef]
- Tanabe, S.; Saitoh, E.; Koyama, S.; Kiyono, K.; Tatemoto, T.; Kumazawa, N.; Kagaya, H.; Otaka, Y.; Mukaino, M.; Tsuzuki, A.; et al. Designing a robotic smart home for everyone, especially the elderly and people with disabilities. Fujita Med. J. 2019, 5, 31–35. [Google Scholar] [CrossRef]
- Benavidez, P.; Kumar, M.; Agaian, S.; Jamshidi, M. Design of a home multi-robot system for the elderly and disabled. In Proceedings of the 2015 10th System of Systems Engineering Conference (SoSE), San Antonio, TX, USA, 17–20 May 2015; pp. 392–397. [Google Scholar]
- Zhao, D.; Yang, J.; Wang, Y.; Yu, C.; Jiang, Y.; Wang, S.; Fukuda, T. Multiple welfare-robots architecture of smart house for security assistance of daily activities. In Proceedings of the 2018 IEEE International Conference on Intelligence and Safety for Robotics (ISR), Shenyang, China, 24–27 August 2018; pp. 595–601. [Google Scholar]
- Darrah, M.; Niland, W.; Stolarik, B. Multiple UAV Dynamic Task Allocation Using Mixed Integer Linear Programming in a SEAD Mission; Infotech@ Aerospace: Arlington, VA, USA, 2005; pp. 1–11. [Google Scholar]
- Wei, C.; Ji, Z.; Cai, B. Particle swarm optimization for cooperative multi-robot task allocation: A multi-objective approach. IEEE Robot. Autom. Lett. 2020, 5, 2530–2537. [Google Scholar] [CrossRef]
- Tereshchuk, V.; Stewart, J.; Bykov, N.; Pedigo, S.; Devasia, S.; Banerjee, A.G. An efficient scheduling algorithm for multi-robot task allocation in assembling aircraft structures. IEEE Robot. Autom. Lett. 2019, 4, 3844–3851. [Google Scholar] [CrossRef] [Green Version]
- Talebpour, Z.; Martinoli, A. Multi-robot coordination in dynamic environments shared with humans. In Proceedings of the 2018 IEEE International Conference on Robotics and Automation (ICRA), Brisbane, QLD, Australia, 21–25 May 2018; pp. 4593–4600. [Google Scholar]
- Choi, H.-L.; Brunet, L.; How, J.P. Consensus-based decentralized auctions for robust task allocation. IEEE Trans. Robot. 2009, 25, 912–926. [Google Scholar] [CrossRef] [Green Version]
- Ye, F.; Chen, J.; Sun, Q.; Tian, Y.; Jiang, T. Decentralized task allocation for heterogeneous multi-UAV system with task coupling constraints. J. Supercomp. 2021, 77, 111–132. [Google Scholar] [CrossRef]
- Bal, M.; Shen, W.; Hao, Q.; Xue, H. Collaborative smart home technologies for senior independent living: A review. In Proceedings of the 2011 15th International Conference on Computer Supported Cooperative Work in Design (CSCWD), Laussane, Switzerland, 8–10 June 2011; pp. 481–488. [Google Scholar]
- Di Marco, D.; Tenorth, M.; Häussermann, K.; Zweigle, O.; Levi, P. Roboearth action recipe execution. Adv. Intell. Syst. Comp. 2013, 193, 457–466. [Google Scholar] [CrossRef]
- Zhao, D.; Yang, J.; Bai, D.; Jiang, Y. Transfer method of multiple welfare-robots based on minimal fuzzy system. Robot 2019, 41, 813–822. [Google Scholar]
- Zhao, D. Interaction Method of Multiple Welfare-Robots Oriented to Safe Transfer Tasks. Ph.D. Thesis, School of Electrical Engineering, Shenyang University of Technology, Shenyang, China, 2020. [Google Scholar]
- Zhao, D.; Yang, J.; Okoye, M.O.; Wang, S. Walking assist robot: A novel non-contact abnormal gait recognition approach based on extended set membership filter. IEEE Access 2019, 7, 76741–76753. [Google Scholar] [CrossRef]
- Matsumoto, N.; Togo, S.; Yokoi, H. Motion Control of a Walking Support Robot Based on Gait Analysis. In Proceedings of the 2019 IEEE International Conference on Robotics and Biomimetics (ROBIO), Dali, China, 6–8 December 2019; pp. 1881–1885. [Google Scholar]
- Fujimoto, A.; Matsumoto, N.; Jiang, Y. Gait Analysis based Speed Control of Walking Assistive Robot. In Proceedings of the 2018 IEEE International Conference on Intelligence and Safety for Robotics (ISR), Shenyang, China, 24–27 August 2018; pp. 88–92. [Google Scholar]
- Tan, R.; Wang, S.; Jiang, Y. Adaptive control of an omni-directional walker considering the forces caused by user. In Proceedings of the 2013 IEEE International Conference on Mechatronics and Automation (ICMA), Takamatsu, Japan, 4–7 August 2013; pp. 761–766. [Google Scholar]
- Jiang, Y.; Wang, S.; Ishida, K. User directional intention identification for a walking support walker: Adaptation to individual differences with fuzzy learning. In Proceedings of the 6th International Conference on Soft Computing and Intelligent Systems, and the 13th International Symposium on Advanced Intelligence Systems, Kobe, Japan, 20–24 November 2012; pp. 1207–1210. [Google Scholar]
- Khamis, A.; Hussein, A.; Elmogy, A. Multi-robot task allocation: A review of the state-of-the-art. Coop. Robot. Sens. Netw. 2015, 604, 31–51. [Google Scholar] [CrossRef]
- Das, G.P.; McGinnity, T.M.; Coleman, S.A.; Behera, L. A distributed task allocation algorithm for a multi-robot system in healthcare facilities. J. Intell. Robot. Syst. 2015, 80, 33–58. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Index | Robot | Name | Function | Hardware Resources | Software Resources |
|---|---|---|---|---|---|
| R1 |  | (IWR) Intelligent Wheelchair Robot | IWR provides the function of indoor movement for people without walking capability. The height of the chair can rise and fall according to different users’ physical conditions, and the angle of backrest can be adjusted considering the comfort of the user [34,35]. | Joystick; Lidar; Pressure sensor. | Localization; Path planning; Obstacle avoidance. |
| R2 |  | (GRR) Gait Rehabilitation Robot | GRR provides the function of gait rehabilitation training for the elderly, patients with lower extremity dysfunction, and postoperative repairs [36,37,38,39,40]. | Depth sensing camera; Pressure sensor; Human–robot interaction panel. | Localization; Path planning; Obstacle avoidance. |
| R3 |  | (PCR) Personal Care Robot | The personal care robot can provide users with the functions of voice interaction, object grasping and delivery, and emergency rescue. | RGB camera; Depth sensing camera; Microphone; Speakers; Gripper; Pressure sensors in gripper; Human-robot interaction panel. | Localization; Path planning; Obstacle avoidance; Speech recognition. |
| R4 |  | (WSR) Walking Support Robot | WSR provides functions of auxiliary standing and auxiliary walking, which can help people with lower extremity inconveniences to implement indoor moving [34,35,36,37,38,39,40]. | Joystick; Lidar; RGB camera; Depth sensing camera. | Localization; Path planning; Obstacle avoidance. |
| R5 |  | (ESR) Excretory Support Robot | ESR can help bedridden people to complete assisted excretion indoors. Six pressure sensors are installed in the seating part, which can be used to evaluate the seating position and fall risk for ensuring comfort of the whole process [34,35]. | Lidar; Depth sensing camera. | Localization; Path planning; Obstacle avoidance. |
| R6 |  | (TR) Transport Robot | TR can help people to handle different things indoor based on the user’s intention [34,35]. | Lidar; Remote control. | Localization; Path planning; Obstacle avoidance. |
| R7 |  | (IB) Intelligent Bed | IB provides users with the functions of indoor omnidirectional movement, assisted getting up and assisted excretion, height adjustment and tilt angle adjustment based on user comfort analysis. Meanwhile, IB provides users with real-time monitoring function of bed state, including bedsore identification and risk assessment of falling from bed. | Remote control; Touch screen; Pressure sensors. | Localization; Obstacle avoidance. |
| Priority | Activity | Task Type | Required Robot |
|---|---|---|---|
| 0 | Emergency tasks | All robots | |
| 1 | Auxiliary excretion | ESR/WSR/IB | |
| 2 | Grasp/Delivery | PCR/TR | |
| 3 | / | Auxiliary walking/Getting up transfer/Transportation/Stand-to-sit/Sit-to-stand | WSR/IWR/TR/PCR |
| 4 | Gait Rehabilitation Training | GRR |
| Start Bit | Position Coordinate x | Position Coordinate y | |||
|---|---|---|---|---|---|
| $ | temp_x/ Upper8bit | temp_x/ Lower8bit | temp_y/ Upper8bit | temp_y/ Lower8bit | |
| z-axis angular velocity | Angle | Stop bit | |||
| temp_dot/ Upper8bit | temp_dot/ Lower8bit | temp_angle/ Upper8bit | temp_dot/ Upper8bit | temp_dot/ Lower8bit | temp_angle/ Upper8bit |
| Assisted Getting-Up | Assisted Stand-to-Sit | Auxiliary Walking | Transportation | Auxiliary Excretion | |
|---|---|---|---|---|---|
| Market-based Algorithm(s) | 3.45 ± 0.84 | 4.54 ± 1.35 | 2.07 ± 1.25 | 2.47 ± 0.88 | 4.03 ± 1.55 |
| DBPAE(s) | 3.23 ± 0.91 | 4.35 ± 1.52 | 1.86 ± 0.93 | 1.97 ± 0.75 | 3.13 ± 1.32 |
| Get Up-Stand Up-Walk-Drink | Move-Stand Up-Excretion-Come Back to Bed | Stand-Rehabilitation Training-Transportation | Abnormal Behavior | |
|---|---|---|---|---|
| Market-based Algorithm(s) | 7.45 ± 2.05 | 9.47 ± 2.64 | 6.48 ± 1.94 | 4.65 ± 1.64 |
| DBPAE(s) | 5.63 ± 1.74 | 7.83 ± 2.35 | 4.64 ± 2.04 | 2.3 ± 1.04 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, D.; Yang, C.; Zhang, T.; Yang, J.; Hiroshi, Y. A Task Allocation Approach of Multi-Heterogeneous Robot System for Elderly Care. Machines 2022, 10, 622. https://doi.org/10.3390/machines10080622
Zhao D, Yang C, Zhang T, Yang J, Hiroshi Y. A Task Allocation Approach of Multi-Heterogeneous Robot System for Elderly Care. Machines. 2022; 10(8):622. https://doi.org/10.3390/machines10080622
Chicago/Turabian StyleZhao, Donghui, Chenhao Yang, Tianqi Zhang, Junyou Yang, and Yokoi Hiroshi. 2022. "A Task Allocation Approach of Multi-Heterogeneous Robot System for Elderly Care" Machines 10, no. 8: 622. https://doi.org/10.3390/machines10080622
APA StyleZhao, D., Yang, C., Zhang, T., Yang, J., & Hiroshi, Y. (2022). A Task Allocation Approach of Multi-Heterogeneous Robot System for Elderly Care. Machines, 10(8), 622. https://doi.org/10.3390/machines10080622