

Development of a Restraint System for Rear-Facing Car Seats

Abstract
:1. Introduction
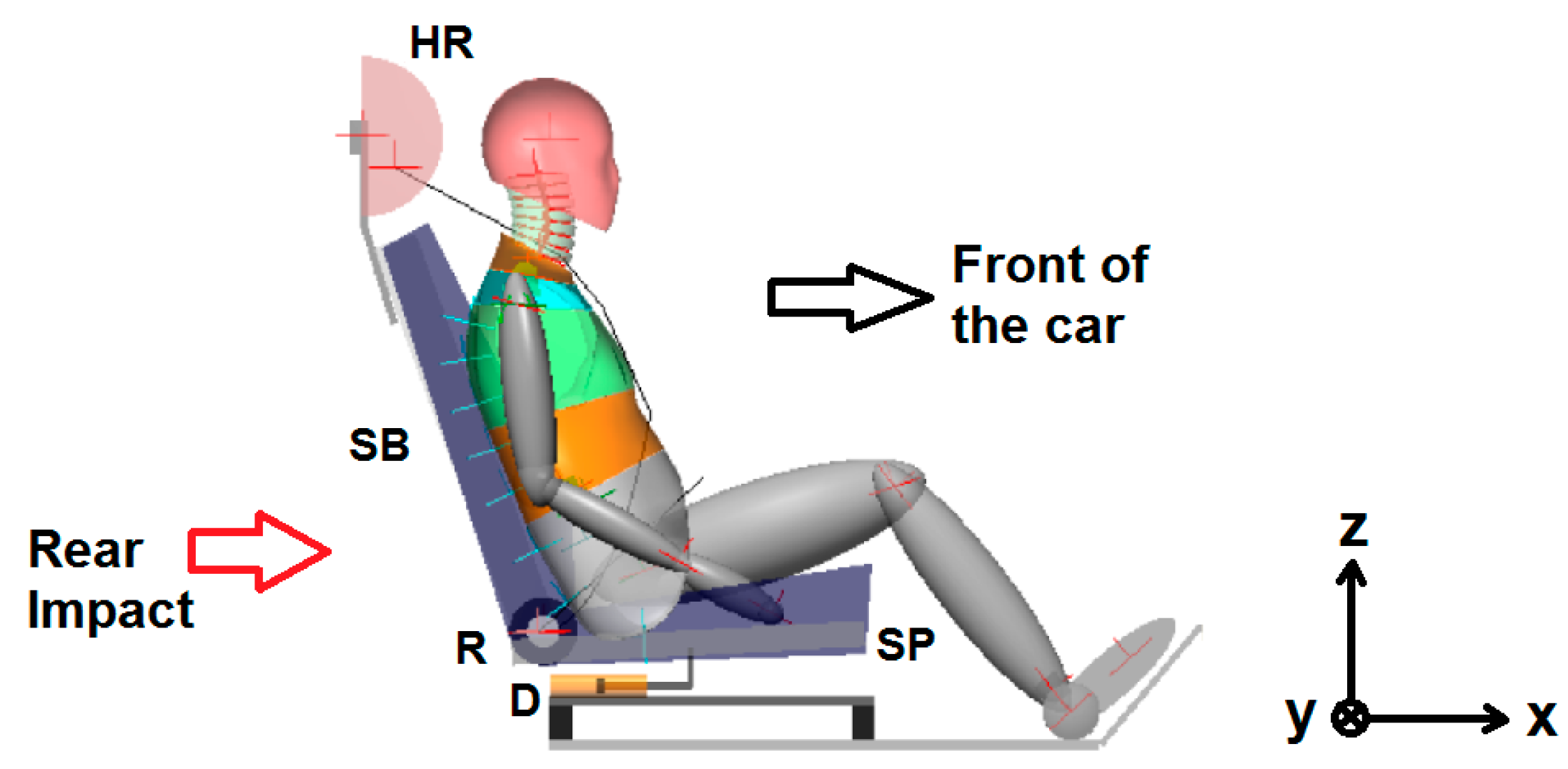
2. Forward-Facing Front Seat for Whiplash Mitigation
2.1. Design Principles and Modelling Details of the Seat
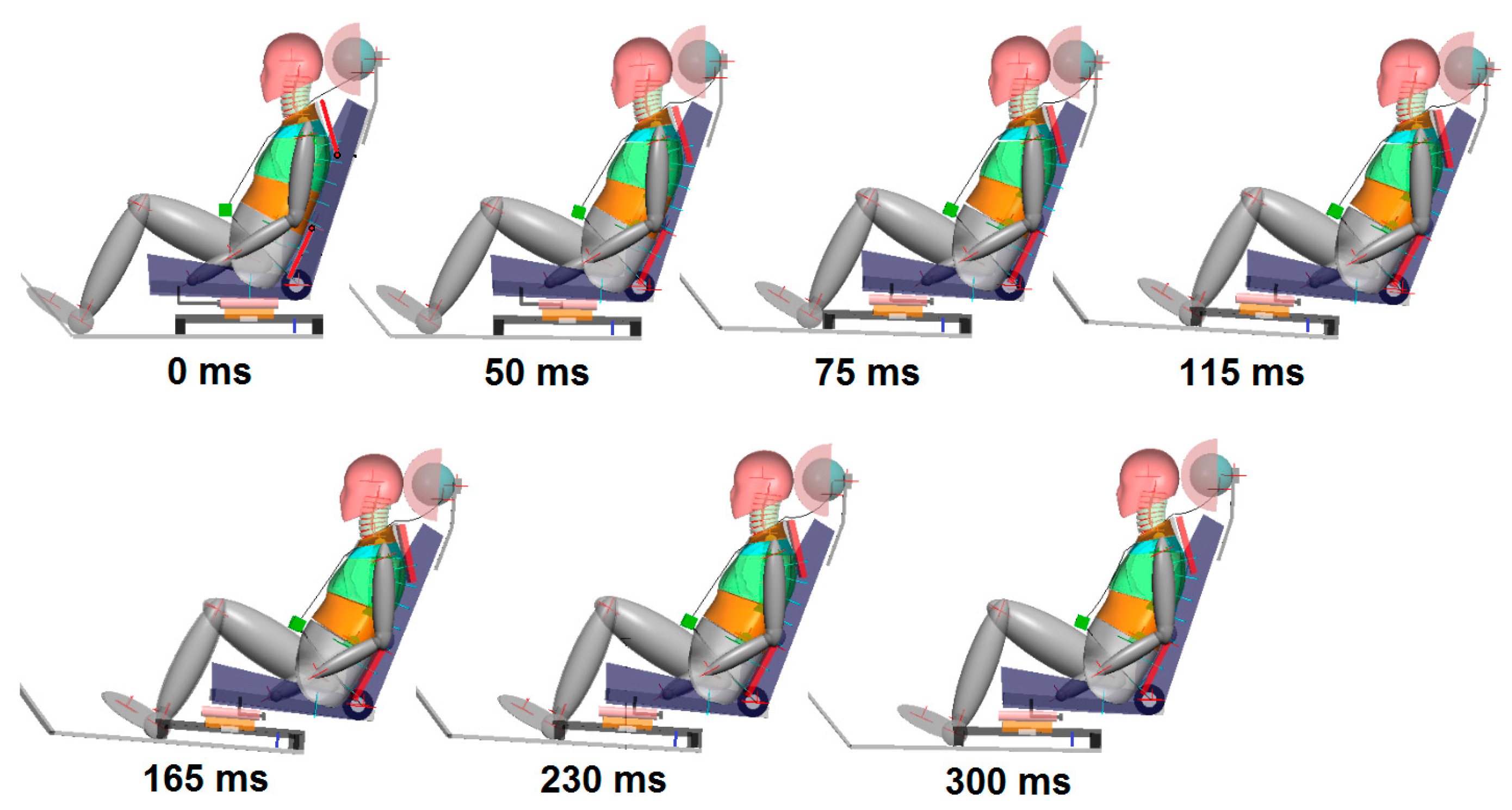
2.2. Assessment of the Performance of the Forward-Facing Front Seat
3. Restraint System Design for Rear-Facing Seats
3.1. Design Principles and Modelling Details of the Rear-Facing Seat
3.2. Performance of the Rear-Facing Seat
3.2.1. Performance of the Rear-Facing Seat at Lower Severities
3.2.2. Performance of the Rear-Facing Seat at Higher Severities
3.2.3. Performance of the Rear-Facing Seat with Out-of-Position Occupant
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pulse | NIC | T1a | HrCt | NDI(−) | NDI(+) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SN(9.4) | 8.83 | 0.19 | 0.48 | 17.7 | 102 | 69 | 3.01 | 96 | 3.42 | 6.79 | 15 | 2.52 | 0.28 |
| SN(13) | 16.8 | 0.28 | 0.42 | 20.0 | 146 | 44 | 4.97 | 139 | 5.00 | 9.07 | 9 | 2.18 | 0.17 |
| SN(16) | 17.2 | 0.31 | 0.43 | 15.0 | 153 | 75 | 4.51 | 135 | 4.63 | 8.83 | 17 | 2.72 | 0.29 |
| SN(20) | 16.4 | 0.28 | 0.39 | 13.9 | 134 | 20 | 5.01 | 108 | 4.05 | 7.95 | 12 | 3.05 | 0.21 |
| TR(24) | 14.5 | 0.28 | 0.39 | 11.9 | 142 | 77 | 4.68 | 119 | 4.76 | 8.59 | 11 | 2.42 | 0.21 |
| Pulse | HIC15 | BrIC |
|---|---|---|
| HS(35) | 7.91 (1.1% IARV) (0% AIS2+) | 0.05 (7% AIS1, 0% AIS2) |
| NC(47) | 35.8 (5.1% IARV) (0% AIS2+) | 0.06 (11% AIS1, 0.1% AIS2) |
| Pulse | ||||||||
|---|---|---|---|---|---|---|---|---|
| HS(35) | 0.31 (31% IARV) | 19 (0.6% IARV) | 172 (5.5% IARV) | 94.3 (2.8% IARV) | 385 (9.6% IARV) | 5.46 (9.5% IARV) | 0.83 (0.4% IARV) | 0.12 (13% AIS2+) (12% IARV) |
| NC(47) | 0.49 (49% IARV) | 15 (0.5% IARV) | 287 (9.2% IARV) | 93 (2.8% IARV) | 653 (16% IARV) | 7.82 (14% IARV) | 1.01 (0.5% IARV) | 0.16 (13% AIS2+) (16% IARV) |
| Pulse | ||||||
|---|---|---|---|---|---|---|
| HS(35) | 41.7 (1.3% IARV) | 142 (4.6% IARV) | 84.9 (2.6% IARV) | 412 (10% IARV) | 3.29 (1.7% IARV) | 5.47 (1.4% IARV) |
| NC(47) | 103 (3.3% IARV) | 157 (5% IARV) | 77 (2.3% IARV) | 739 (18% IARV) | 3.52 (1.8% IARV) | 6.41 (1.7% IARV) |
| Pulse | NIC | NDI(−) | NDI(+) | |
|---|---|---|---|---|
| HS(35) | 0.39 (6.5% IARV) | 21 (78% IARV) | 3.34 | 0.14 |
| NC(47) | 0.54 (9% IARV) | 9.9 (37% IARV) | 5.50 | 0.25 |
| Pulse | Ta3 | cd | VC |
|---|---|---|---|
| HS(35) | 12.3 (20.5% IARV) (37% AIS2+) | 2.3 (5.5% IARV) (14% AIS2+) | 0.0059 (0.59% IARV) (0% AIS2+) |
| NC(47) | 24.8 (41% IARV) (55% AIS2+) | 2.5 (6% IARV) (14% AIS2+) | 0.0054 (0.54% IARV) (0% AIS2+) |
| Pulse | ||
|---|---|---|
| HS(35) | 0 | 2002 (31% IARV) |
| NC(47) | 0 | 2817 (44% IARV) |
| Pulse | TI | |||
|---|---|---|---|---|
| HS(35) | 1.3 (13% IARV) (0% AIS2+) | 0.21 (2.1% IARV) (0% AIS2+) | 43 N (0.54% IARV) (0% AIS2+) | 0.063 (4.8% IARV) (0% AIS2+) |
| NC(47) | 2.18 (21.8% IARV) (0% AIS2+) | 0.42 (4.2% IARV) (0% AIS2+) | 45 N (0.56% IARV) (0% AIS2+) | 0.11 (8.5% IARV) (0% AIS2+) |
| Region | Criterion | % IARV-exp | % IARV-Model |
|---|---|---|---|
| Head | HIC15 | 70–80% | 13% |
| Upper Neck | 1–1.5% | 0.4% | |
| 23–32% | 11% | ||
| 8–13% | 13% | ||
| 25–35% | 18% | ||
| 19–43% | 19% | ||
| 17–18% | 3% | ||
| 18–38% | 19% | ||
| Lower Neck | 36–40% | 10% | |
| 10–15% | 4.8% | ||
| 17–19% | 5.4% | ||
| 20–23% | 21% | ||
| 1–1.5% | 7.2% | ||
| 17–18% | 1.6% | ||
| Thorax | Ta3 | 85–90% | 54% |
| cd | 18–20% | 15% | |
| VC | 2–3% | 0.6% | |
| Lumbar Spine | 7–10% | 0% | |
| 74–91% | 55% |
References
- Himmetoğlu, S. Introduction of a Protection System for Rear-Facing Seats in Autonomous Car Crashes. In Proceedings of the 26th International Scientific Conference Transport Means, Kaunas, Lithuania, 5–7 October 2022; pp. 104–109. [Google Scholar]
- Gutsche, A.J.; Tomasch, E.; Sinz, W.; Levallois, I.; Alonso, S.; Lemmen, P.; Linder, A.; Steffan, H. Improve Assessment and Enhance Safety for the Evaluation of Whiplash Protection Systems Addressing Male and Female Occupants in Different Seat Configurations by Introducing Virtual Methods in Consumer Tests. In Proceedings of the 2013 Ircobi Conference, Göteborg, Sweden, 11–13 September 2013; pp. 77–90. [Google Scholar]
- Jakobsson, L.; Östh, J.; Bohman, K. Rear-end Impact Assessment Expanded with Pre-Impact Posture Variations. In Proceedings of the 2021 Ircobi Conference, Online, 8–10 September 2021. [Google Scholar]
- Parenteau, C.S.; Viano, D.C.; Lau, E.C. Rear-Seat occupant demographics in rear impacts. Traffic Inj. Prev. 2021, 22, 218–223. [Google Scholar] [CrossRef] [PubMed]
- EuroNCAP. European New Car Assessment Programme–The Dynamic Assessment of Car Seats for Neck Injury Protection Testing Protocol; Version 4.1.1; EuroNCAP: Leuven, Belgium, 2021; 54p. [Google Scholar]
- National Highway Traffic Safety Administration (NHTSA). Available online: www.nhtsa.gov/research-data/research-testing-databases#/vehicle (accessed on 11 September 2023).
- Jakobsson, L.; Isaksson-Hellman, I.; Lindman, M. WHIPS (Volvo Cars’ Whiplash Protection System)—The development and real-world performance. Traffic Inj. Prev. 2008, 9, 600–605. [Google Scholar] [CrossRef] [PubMed]
- Mang, D.W.H.; Siegmund, G.P.; Blouin, J.-S. A comparison of anti-whiplash seats during low/moderate speed rear-end collisions. Traffic Inj. Prev. 2020, 21, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Himmetoglu, S.; Acar, M.; Bouazza-Marouf, K.; Taylor, A.J. Car-seat design to improve rear-impact protection. Proc. IMechE Part D J. Automob. Eng. 2011, 225, 441–459. [Google Scholar] [CrossRef]
- Zellmer, H.; Lubbe, N.; Sander, U. Assessing the Injury Risk of Car Occupants on Rearward Facing Seats–An Analysis of GIDAS Cases. In Proceedings of the 8th ESAR Expert Symposium on Accident Research Conference, Hannover, Germany, 19–20 April 2018. [Google Scholar]
- Zellmer, H.; Manneck, F. Assessing Injury Risk of Car Occupants on Rearward Facing Seats in a Full Frontal Impact–Sled Tests in a Generic Test Environment. In Proceedings of the 26th ESV Conference, Eindhoven, The Netherlands, 10–13 June 2019. [Google Scholar]
- Soni, A.; Schilling, S.; Faust, J.; Eickhoff, B. Responses of HIII, THOR, and SAFER-HBM Occupant Models in Rearward-Facing Seat Configuration for High Severity Frontal Impact. In Proceedings of the 2020 Ircobi Conference, Munich, Germany; 2020. [Google Scholar]
- Jin, X.; Hou, H.; Shen, M.; Wu, H.; Yang, K.H. Occupant Kinematics and Biomechanics with Rotatable Seat in Autonomous Vehicle Collision: A Preliminary Concept and Strategy. In Proceedings of the 2018 Ircobi Conference, Athens, Greece, 12–14 September 2018. [Google Scholar]
- Hasija, V.; Kelkar, R.; Takhounts, E.G. Simulation Assessment of Injury Trends for 50th Percentile Males Using Potential Seating Configurations of Future Automated Driving System (ADS) Equipped Vehicles. In Proceedings of the 26th ESV Conference, Eindhoven, The Netherlands, 10–13 June 2019. [Google Scholar]
- Himmetoglu, S.; Acar, M.; Bouazza-Marouf, K.; Taylor, A.J. A multibody human model for rear-impact simulation. Proc. IMechE Part D J. Automob. Eng. 2009, 223, 623–638. [Google Scholar] [CrossRef]
- Himmetoglu, S. Validation of a Multi-Body Human Model for Efficient Rear Impact Simulations. In Proceedings of the 25th International Scientific Conference Transport Means 2021, Online/Kaunas, Lithuania, 6–8 October 2021; pp. 35–40. [Google Scholar]
- Davidsson, J.; Ono, K.; Inami, S.; Svensson, M.Y.; Lövsund, P. A Comparison between Volunteer, BioRID P3 and Hybrid III Performance in Rear Impacts. In Proceedings of the 1999 Ircobi Conference, Sitges, Spain, 23–24 September 1999; pp. 165–178. [Google Scholar]
- Insurance Institute for Highway Safety. Insurance Institute for Highway Safety–Vehicle Seat/Head Restraint Evaluation Protocol–Dynamic Criteria; Version V; IIHS: Ruckersville, VA, USA, 2019; 31p. [Google Scholar]
- Kolich, M. Occupant preferred back angle relative to head restraint regulations. SAE Int. J. Passeng. Cars 2010, 3, 626–632. [Google Scholar] [CrossRef]
- Karabeyoglu, C. Smart Car Seat Design for Safety and Comfort. Master’s Thesis, Hacettepe University, Mechanical Engineering Department, Ankara, Turkey, 2019. [Google Scholar]
- Edwards, M.A.; Brumbelow, M.L.; Trempel, R.E.; Gorjanc, T.C. Seat Design Characteristics Affecting Occupant Safety in Low- and High-Severity Rear-Impact Collisions. In Proceedings of the 2019 Ircobi Conference, Florence, Italy, 11–13 September 2019. [Google Scholar]
- Wietholter, K.; Echemendia, C.; Louden, A.E. Development of a Representative Seat Assembly for FMVSS No. 213. In Proceedings of the 25th ESV Conference, Detroit, MI, USA, 5–8 June 2017. [Google Scholar]
- Genzel, J.; Carlsson, A.; Linder, A.; Pipkorn, B.; Svensson, M. An Open-Source Finite Element Model of a Generic Car Seat: Development and Validation for Low-Severity Rear Impact Evaluations. In Proceedings of the 2022 Ircobi Conference, Porto, Portugal, 14–16 September 2022. [Google Scholar]
- Viano, D.C. Role of the Seat in Rear Crash Safety; Society of Automotive Engineers: Warrendale, PA, USA, 2002. [Google Scholar]
- Netherlands’ Organization for Applied Research (TNO). MADYMO Theory Manual; Version 6.2.2; TNO MADYMO BV: Delft, The Netherlands, 2005. [Google Scholar]
- Park, C.K.; Kan, C.D. Objective Evaluation Method of Vehicle Crash Pulse Severity in Frontal New Car Assessment Program (NCAP) Tests. In Proceedings of the 24th ESV Conference, Gothenburg, Sweden, 8–11 June 2015. [Google Scholar]
- Gabauer, D.J.; Gabler, H.C. Can Delta-V be Adjusted with Structural and Occupant Restraint Performance to Improve Prediction of Chest Acceleration? In Proceedings of the Annals of Advances in Automotive Medicine, 52nd Annual Scientific Conference, San Diego, CA, USA, 6–8 October 2008. [Google Scholar]
- Zuby, D.S.; Farmer, C.M.; Avery, M. The Influence of Crash Pulse Shape on BioRID Response. In Proceedings of the 2003 Ircobi Conference, Lisbon, Portugal, 25–26 September 2003; pp. 327–341. [Google Scholar]
- Wood, D.P.; Adamson, D.; Ydenius, A. Car frontal collisions: Occupant compartment forces, interface forces and stiffnesses. Int. J. Crashworthiness 2004, 9, 311–325. [Google Scholar] [CrossRef]
- EuroNCAP. European New Car Assessment Programme–Assessment Protocol–Adult Occupant Protection; Version 9.1.3; EuroNCAP: Leuven, Belgium, 2021; 49p. [Google Scholar]
- Himmetoglu, S. An Evaluation of Passive Head-Restraints with Different Stiffness and Energy Dissipation Properties for Whiplash Mitigation. In Proceedings of the 7th International Expert Symposium on Accident Research (ESAR 2016), Hannover, Germany, 9–10 June 2016. [Google Scholar]
- Hu, D.Y.; Yang, J.L.; Hu, M.H. Full-scale vertical drop test and numerical simulation of a crashworthy helicopter seat/occupant system. Int. J. Crashworthiness 2009, 14, 565–583. [Google Scholar] [CrossRef]
- Desjardins, S.P. The Evolution of Energy Absorption Systems for Crashworthy Helicopter Seats. In Proceedings of the American Helicopter Society 59th Annual Forum, Phoenix, AZ, USA, 6–8 May 2003. [Google Scholar]
- Zhang, X.; Zhou, Q. An energy-absorbing sliding seat for reducing neck injury risks in rear impact–analysis for prototype built. Traffic Inj. Prev. 2016, 17, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Östling, M.; Lundgren, C.; Lubbe, N.; Pipkorn, B. Reducing lumbar spine vertebra fracture risk with an adaptive seat track load limiter. Front. Future Transp. 2022, 3, 1–10. [Google Scholar] [CrossRef]
- Jazar, R.N. Vehicle Dynamics: Theory and Application; Springer Science + Business Media LLC.: New York, NY, USA, 2008. [Google Scholar]
- Marzougui, D.; Samaha, R.R.; Cui, C.; Kan, C.-D. Working Paper NCAC 2012-W-005; National Crash Analysis Center (NCAC); The George Washington University: Washington, DC, USA, 2012. [Google Scholar]
- Society of Automotive Engineers (SAE). SAE J211-1 (1995): Instrumentation for Impact Test, Part 1, Electronic Instrumentation; SAE: Warrendale, PA, USA, 2007. [Google Scholar]
- Schmitt, K.U.; Niederer, P.F.; Cronin, D.S.; Morrison, B., III; Muser, M.H.; Walz, F. Trauma Biomechanics, 5th ed.; Springer Nature: Cham, Switzerland, 2019. [Google Scholar]
- Takhounts, E.G.; Craig, M.J.; Moorhouse, K.; McFadden, J.; Hasija, V. Development of brain injury criteria (BrIC). Stapp Car Crash J. 2013, 57, 243–266. [Google Scholar] [CrossRef] [PubMed]
- Eppinger, R.; Sun, E.; Bandak, F.; Haffner, M.; Khaewpong, N.; Maltese, M.; Kuppa, S.; Nguyen, T.; Takhounts, E.; Tannous, R.; et al. Development of Improved Injury Criteria for the Assessment of Advanced Automotive Restraint Systems—II; NHTSA: Washington DC, USA, 1999.
- Rupp, J.D.; Flannagan, C.A.C.; Kuppa, A.M. Development of New Injury Risk Curves for the Knee/Distal Femur and the Hip for Use in Frontal Impact Testing; Report No. UMTRI-2009-08; The University of Michigan Transportation Research Institute: Ann Arbor, MI, USA, 2009. [Google Scholar]
- Kuppa, S.; Wang, J.; Haffner, M.; Eppinger, R. Lower Extremity Injuries and Associated Injury Criteria. In Proceedings of the 17th ESV Conference, Amsterdam, The Netherlands, 4–7 June 2001. [Google Scholar]
- Lau, I.V.; Viano, D.C. The Viscous Criterion—Bases and applications of an injury severity index for soft tissues. SAE Trans. 1986, 95, 672–691. [Google Scholar] [CrossRef]
- Bracq, A.; Delille, R.; Marechal, C.; Bourel, B.; Roth, S.; Mauzac, O. Rib fractures prediction method for kinetic energy projectile impact: From blunt ballistic experiments on SEBS gel to impact modeling on a human torso FE model. Forensic Sci. Int. 2019, 297, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Funk, J.R.; Rudd, R.W.; Kerrigan, J.R.; Crandall, J.R. Analysis of Tibial Curvature, Fibular Loading, and the Tibia Index. In Proceedings of the 2003 Ircobi Conference, Lisbon, Portugal, 25–26 September 2003; pp. 135–147. [Google Scholar]
- Yoganandan, N.; Arun, M.W.J.; Stemper, B.D.; Pintar, F.A.; Maiman, D.J. Biomechanics of human thoracolumbar spinal column trauma from vertical impact loading. Ann. Adv. Automot. Med. 2013, 57, 155–166. [Google Scholar] [PubMed]
- Boström, O.; Bohman, K.; Haland, Y.; Kullgren, A.; Krafft, M. New AIS1 Long-Term Neck Injury Criteria Candidates Based on Real Frontal Crash Analysis. In Proceedings of the 2000 IRCOBI Conference, Montpellier, France, 20–22 September 2000; pp. 249–264. [Google Scholar]
- Ejima, S.; Zama, Y.; Satou, F.; Holcombe, S.; Ono, K.; Kaneoka, K.; Shiina, I. Prediction of the Physical Motion of the Human Body Based on Muscle Activity During Pre-Impact Braking. In Proceedings of the 2008 Ircobi Conference, Bern, Switzerland, 17–19 September 2008; pp. 163–175. [Google Scholar]
- Erlinger, N.; Kofler, D.; Heider, E.; Klug, C. Effects of Boundary Conditions and Posture on Simulations with Human Body Models of Braking Events. In Proceedings of the 2022 Ircobi Conference, Porto, Portugal, 14–16 September 2022. [Google Scholar]
- Karemyr, M.; Pettersson, T.; Svensson, M.; Linder, A. Development of Prototype Concepts of the SETs of an Average Female and Male for Low Severity Rear Impact Crash Testing; VTI Report 1147A; Swedish National Road and Transport Research Institute (VTI): Linköping, Sweden, 2022. [Google Scholar]
- Severinsson, Y.; Elisson, L.; Bunketorp, O. Reliability of measuring the cervical sagittal translation mobility with a simple method in a clinical setting. Rehab. Res. Prac. 2012, 2012, 629104. [Google Scholar] [CrossRef] [PubMed]
- Marieswaran, M.; Mansoori, N.; Digge, V.K.; Jhajhria, S.K.; Behera, C.; Lalwani, S.; Kalyanasundaram, D. Effect of preservation methods on tensile properties of human femur-acl-tibial complex (FATC)—A Cadaveric Study on Male Subjects. Acta Bioeng. Biomech. 2018, 20, 31–42. [Google Scholar] [PubMed]
- Graci, V.; Griffith, M.; Seacrist, T.; Brase, D.; Mishra, E.; Pipkorn, B.; Lubbe, N.; Arbogast, K.B. Repositioning forward-leaning vehicle occupants with a pre-pretensioner belt and a startle-based warning in pre-crash scenarios. Traffic Inj. Prev. 2022, 23, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Mishra, E.; Mroz, K.; Lubbe, N. Repositioning forward-leaning passengers by seatbelt pre-pretensioning. Traffic Inj. Prev. 2023, 24, 716–721. [Google Scholar] [CrossRef] [PubMed]












| Crash Pulse | [g] | Delta-V [km/h] | [g] |
|---|---|---|---|
| SN(9.4) | 11.7 | 9.4 | 4.72 |
| SN(13) | 11.2 | 13 | 5.97 |
| SN(16) | 10 | 16 | 7.30 |
| SN(20) | 10.63 | 20 | 7.69 |
| TR(24) | 7.5 | 24 | 7.50 |
| Medium Severity Crash Pulse SN(16) | High Severity Crash Pulse TR(24) | ||||||
|---|---|---|---|---|---|---|---|
| Criterion | Unit | HL | LL | CL | HL | LL | CL |
| NIC | m2/s2 | 11 | 24 | 27 | 13 | 23 | 25.5 |
| - | - | - | 0.69 | - | - | 0.75 | |
| m/s | - | - | 5.2 | - | - | 6 | |
| N | 30 | 190 | 290 | 30 | 210 | 364 | |
| N | - | - | 360 | - | - | 360 | |
| N | 360 | 750 | 900 | 470 | 770 | 1024 | |
| Nm | - | - | 30 | - | - | 30 | |
| N | - | - | 360 | - | - | 360 | |
| Nm | - | - | 30 | - | - | 30 | |
| T1a | g | - | - | 15.55 | - | - | 17.8 |
| HrCt | ms | - | - | 92 | - | - | 92 |
| Pulse | NIC | T1a | HrCt | NDI(−) | NDI(+) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SN(9.4) | 8.14 | 0.11 | 1.35 | 16 | 49 | 110 | 6.57 | 143 | 5.20 | 6.21 | 62 | 0.32 | 1.58 |
| SN(13) | 8.89 | 0.26 | 1.23 | 32 | 98 | 112 | 8.56 | 161 | 4.17 | 7.44 | 47 | 0.63 | 2.18 |
| SN(16) | 11.4 | 0.19 | 1.27 | 24 | 94 | 192 | 7.85 | 161 | 6.31 | 8.32 | 56 | 1.22 | 1.44 |
| SN(20) | 11.9 | 0.32 | 1.35 | 14 | 134 | 178 | 7.10 | 126 | 6.28 | 8.32 | 58 | 1.13 | 0.31 |
| TR(24) | 11.3 | 0.43 | 1.17 | 19 | 151 | 101 | 11.7 | 104 | 5.71 | 7.64 | 51 | 3.37 | 0.30 |
| Crash Pulse | Delta-V | ||
|---|---|---|---|
| HS(35) | 16 g (x) | 35 km/h (x) | 10.54 g (x) |
| NC(47) | −27.3 g (x) | −47.5 km/h (x) | −20.7 g (x) |
| 8.61 g (z) | −1.93 km/h (z) | −1.68 g (z) | |
| 3.72 deg/s2 (y) | −2.36 deg/s (y) | −570 deg/s2 (y) | |
| NC(64) | −46.56 g (x) | −64.2 km/h (x) | −31.92 g (x) |
| 12.89 g (z) | −4.98 km/h (z) | 3.26 g (z) | |
| 13,096 deg/s2 (y) | −12.87 deg/s (y) | 2963 deg/s2 (y) |
| Pulse | NIC | T1a | HrCt | NDI(−) | NDI(+) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SN(9.4) | 7.79 | 0.17 | 0.49 | 17.5 | 88 | 49 | 2.57 | 84 | 4.01 | 7.87 | 14 | 2.29 | 0.28 |
| SN(13) | 11.3 | 0.26 | 0.47 | 17.7 | 135 | 81 | 3.28 | 129 | 3.64 | 12.0 | 8 | 1.21 | 0.17 |
| SN(16) | 13.3 | 0.25 | 0.46 | 15.7 | 130 | 97 | 6.08 | 125 | 3.55 | 8.87 | 16 | 2.57 | 0.29 |
| SN(20) | 9.19 | 0.21 | 0.41 | 12.8 | 115 | 17 | 3.56 | 106 | 3.70 | 7.74 | 11 | 2.79 | 0.22 |
| TR(24) | 15.2 | 0.23 | 0.42 | 9.38 | 128 | 85 | 3.42 | 114 | 3.64 | 8.25 | 11 | 2.14 | 0.21 |
| Region | Criterion | IARV | Reference |
|---|---|---|---|
| Head | HIC15 | 700 | [41] |
| BrIC | - | [40] | |
| Upper Neck | (+shear) | 3100 N | [11,39] |
| (−shear) | 3100 N | [11,39] | |
| (tension) | 3300 N | [39,41] | |
| (compr.) | 4000 N | [39,41] | |
| (extension) | 57 Nm | [39,41] | |
| (flexion) | 190 Nm | [39,41] | |
| Nij | 1 | [39,41] | |
| Lower Neck | (+shear) | 3100 N | [11,39] |
| (−shear) | 3100 N | [11,39] | |
| (tension) | 3300 N | [39,41] | |
| (compr.) | 4000 N | [39,41] | |
| (extension) | 194 Nm | [11] | |
| (flexion) | 380 Nm | [11] | |
| Thorax | Ta3 (thorax acc.) | 60 g | [39,41] |
| cd (chest defl.) | 42 mm | [30,39] | |
| VC | 1 m/s | [39,44,45] | |
| Lumbar Spine | (tension) | 12.2 kN | [11] |
| (compr.) | 6400 N | [11,39] | |
| Hip | (axial compr.) | 10 kN | [39,42] |
| Femur (thigh) | (axial compr.) | 10 kN | [30,42,43] |
| Tibia | (axial compr.) | 8 kN | [30,39,43] |
| Tibia | TI | 1.3 | [30,39,43,46] |
| Pulse | HIC15 | BrIC |
|---|---|---|
| HS(35) | 6.86 (1% IARV) (0% AIS2+) | 0.03 (3% AIS1, 0% AIS2) |
| NC(47) | 39.3 (6% IARV) (0% AIS2+) | 0.04 (4% AIS1, 0% AIS2) |
| NC(64) | 89.6 (13% IARV) (0% AIS2+) | 0.042 (5% AIS1, 0% AIS2) |
| Pulse | ||||||||
|---|---|---|---|---|---|---|---|---|
| HS(35) | 0.29 (29% IARV) | 15.5 (0.5% IARV) | 157 (5% IARV) | 76.2 (2% IARV) | 445 (11% IARV) | 4.74 (8% IARV) | 0.66 (0.3% IARV) | 0.12 (13% AIS2+) (12% IARV) |
| NC(47) | 0.42 (42% IARV) | 13.1 (0.4% IARV) | 219 (7% IARV) | 223 (7% IARV) | 634 (16% IARV) | 7.37 (13% IARV) | 1.54 (0.8% IARV) | 0.15 (13% AIS2+) (15% IARV) |
| NC(64) | 0.67 (67% IARV) | 11.6 (0.4% IARV) | 350 (11% IARV) | 445 (13% IARV) | 729 (18% IARV) | 10.7 (19% IARV) | 5.52 (3% IARV) | 0.19 (14% AIS2+) (19% IARV) |
| Pulse | ||||||
|---|---|---|---|---|---|---|
| HS(35) | 75 (2.4% IARV) | 145 (5% IARV) | 99 (3% IARV) | 420 (11% IARV) | 3.09 (1.6% IARV) | 4.41 (1% IARV) |
| NC(47) | 124 (4% IARV) | 133 (4.3% IARV) | 125 (4% IARV) | 721 (18% IARV) | 5.02 (2.6% IARV) | 5.09 (1.3% IARV) |
| NC(64) | 309 (10% IARV) | 149 (4.8% IARV) | 179 (5.4% IARV) | 837 (21% IARV) | 14.0 (7.2% IARV) | 5.92 (1.6% IARV) |
| Pulse | NIC | NDI(−) | NDI(+) | |
|---|---|---|---|---|
| HS(35) | 0.43 (7% IARV) | 16.8 (62% IARV) | 3.48 | 0.14 |
| NC(47) | 0.54 (9% IARV) | 10.6 (39% IARV) | 3.49 | 0.29 |
| NC(64) | 0.87 (14% IARV) | 19.7 (73% IARV) | 2.74 | 0.96 |
| Pulse | Ta3 | cd | VC |
|---|---|---|---|
| HS(35) | 11.9 (20% IARV) (36% AIS2+) | 2.3 (5.5% IARV) (14% AIS2+) | 0.0072 (0.72% IARV) (0% AIS2+) |
| NC(47) | 25.2 (42% IARV) (55% AIS2+) | 2.6 (6.2% IARV) (14% AIS2+) | 0.005 (0.5% IARV) (0% AIS2+) |
| NC(64) | 32.6 (54% IARV) (65% AIS2+) | 3.2 (7.6% IARV) (15% AIS2+) | 0.006 (0.6% IARV) (0% AIS2+) |
| Pulse | ||
|---|---|---|
| HS(35) | 0 | 2172 (34% IARV) |
| NC(47) | 0 | 2826 (44% IARV) |
| NC(64) | 0 | 3512 (55% IARV) |
| Pulse | TI | |||
|---|---|---|---|---|
| HS(35) | 1.3 (13% IARV) (0% AIS2+) | 0.21 (2.1% IARV) (0% AIS2+) | 43 N (0.54% IARV) (0% AIS2+) | 0.063 (4.8% IARV) (0% AIS2+) |
| NC(47) | 2.18 (21.8% IARV) (0% AIS2+) | 0.42 (4.2% IARV) (0% AIS2+) | 45 N (0.56% IARV) (0% AIS2+) | 0.11 (8.5% IARV) (0% AIS2+) |
| NC(64) | 3.2 (32% IARV) (0% AIS2+) | 0.50 (5% IARV) (0% AIS2+) | 44 N (0.55% IARV) (0% AIS2+) | 0.13 (10% IARV) (0% AIS2+) |
| Region | Criterion | Value | % IARV | % AIS |
|---|---|---|---|---|
| Head | HIC15 | 105 (117) | 15% (17%) | 0% (0%) AIS2+ |
| BrIC | 0.068 (0.070) | - | 18% (19%) AIS1 | |
| Upper Neck | 0.84 (0.83) | 84% (83%) | - | |
| 41 (100) N | 1.3% (3.2%) | - | ||
| 416 (434)N | 13% (14%) | - | ||
| 435 (334) N | 13% (10%) | - | ||
| 782 (760) N | 20% (19%) | - | ||
| 13.5 (17.7) Nm | 23% (31%) | - | ||
| 9.15 (13.5) Nm | 4.8% (7.1%) | - | ||
| 0.20 (0.24) | 20% (24%) | 14% (15%) AIS2+ | ||
| Lower Neck | 265 (194) N | 8.5% (6.3%) | - | |
| 175 (179) N | 5.6% (5.8%) | - | ||
| 205 (217) N | 6.2% (6.6%) | - | ||
| 899 (891) N | 22% (22%) | - | ||
| 11.5 (15.5) Nm | 5.9% (8%) | - | ||
| 9.76 (10.7) Nm | 2.6% (2.8%) | - | ||
| Overall Neck | 0.88 (0.89) m/s | 14.7% (14.8%) | - | |
| NIC | 26 (32) m2/s2 | 96% (118%) | 50% (70%) AIS1 | |
| NDI(−) | 0.27 (2.75) deg | - | - | |
| NDI(+) | 3.88 (0.90) deg | - | - | |
| Thorax | Ta3 | 32.6 (32.6) g | 54% (54%) | 65% (65%) AIS2+ |
| cd | 5.5 (5.5) mm | 13% (13%) | 16% (16%) AIS2+ | |
| VC | 0.01 (0.01) m/s | 1% (1%) | 0% (0%) AIS2+ | |
| Lumbar Spine | 0 (0) kN | 0% (0%) | - | |
| 4034 (4078) N | 63% (64%) | - | ||
| Hip | 2.90 (2.76) kN | 29% (27.6%) | 0% (0%) AIS2+ | |
| Femur (thigh) | 0.91 (0.90) kN | 9.1% (9%) | 0% (0%) AIS2+ | |
| Tibia | 84 (83) N | 1% (1%) | 0% (0%) AIS2+ | |
| Tibia | TI | 0.69 (0.69) | 53% (53%) | 5% (5%) AIS2+ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yavuz, S.; Himmetoglu, S. Development of a Restraint System for Rear-Facing Car Seats. Machines 2023, 11, 1076. https://doi.org/10.3390/machines11121076
Yavuz S, Himmetoglu S. Development of a Restraint System for Rear-Facing Car Seats. Machines. 2023; 11(12):1076. https://doi.org/10.3390/machines11121076
Chicago/Turabian StyleYavuz, Samet, and Selcuk Himmetoglu. 2023. "Development of a Restraint System for Rear-Facing Car Seats" Machines 11, no. 12: 1076. https://doi.org/10.3390/machines11121076
APA StyleYavuz, S., & Himmetoglu, S. (2023). Development of a Restraint System for Rear-Facing Car Seats. Machines, 11(12), 1076. https://doi.org/10.3390/machines11121076