
Design, Development and Control of a Therapeutic Robot Incorporating Aquatic Therapy for Ankle Rehabilitation

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
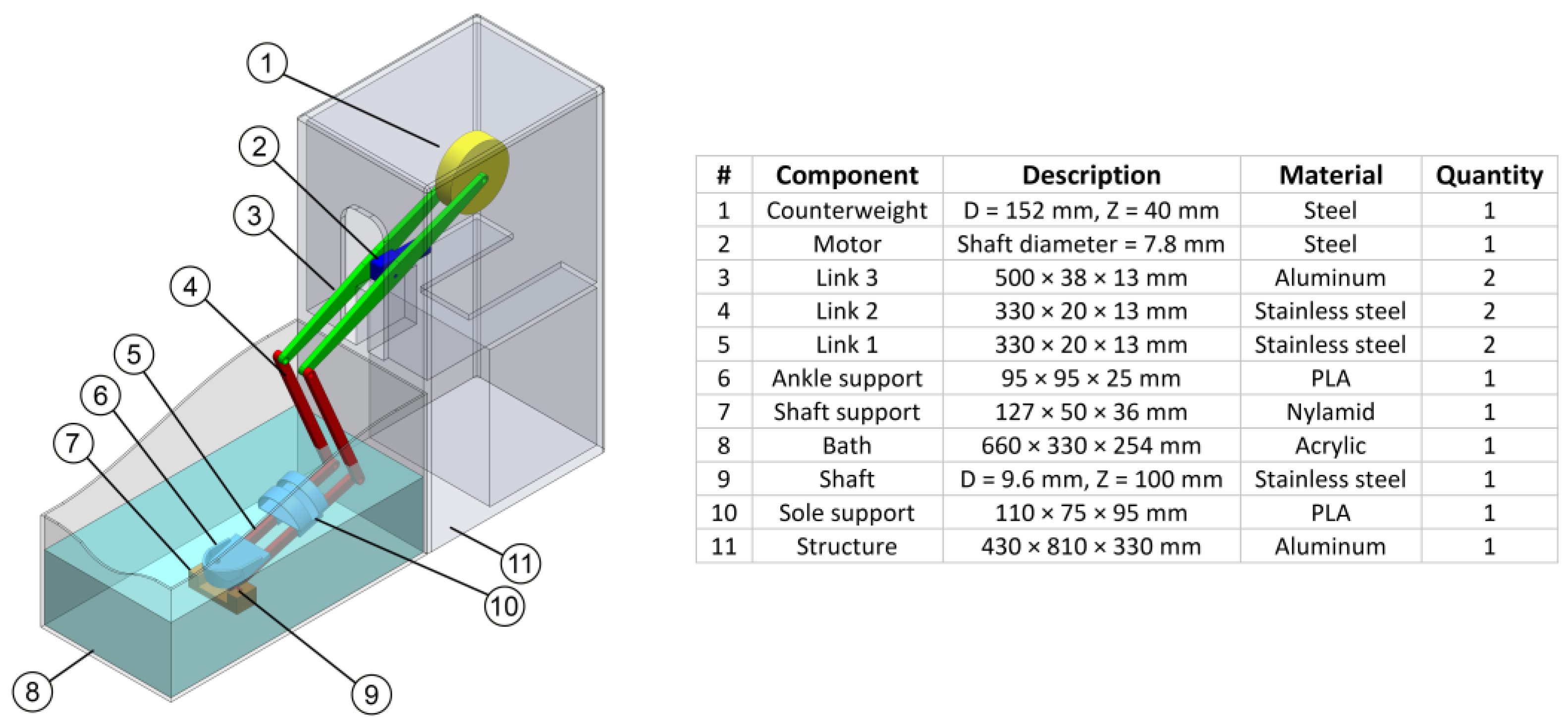
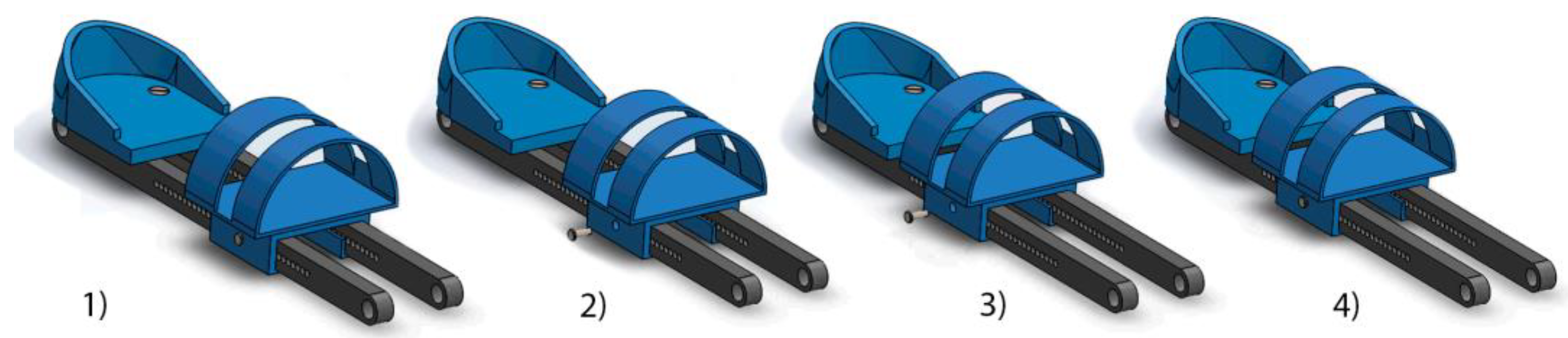
2.1. Robot Design
2.2. Modeling and Control of the Ankle Rehabilitation Robot
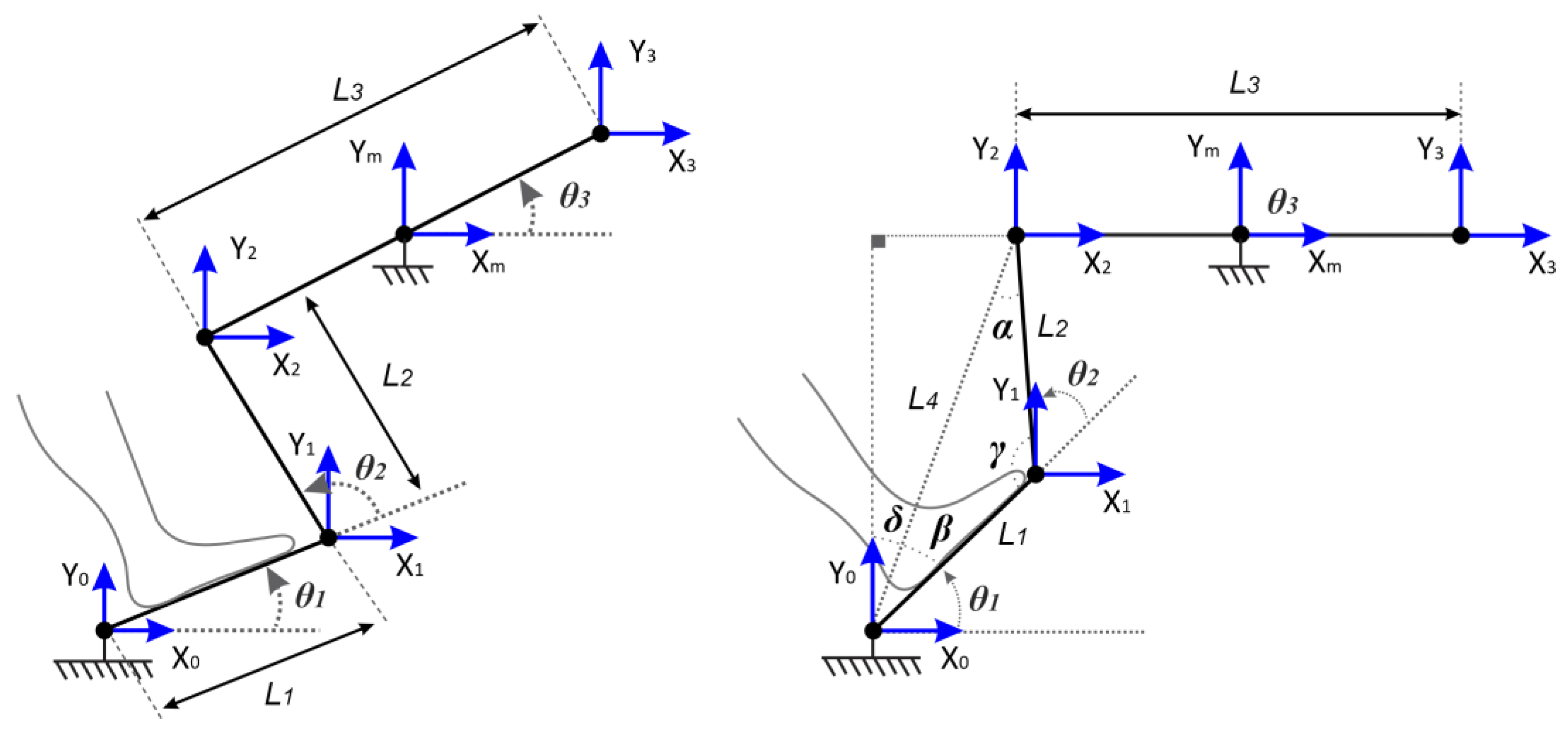
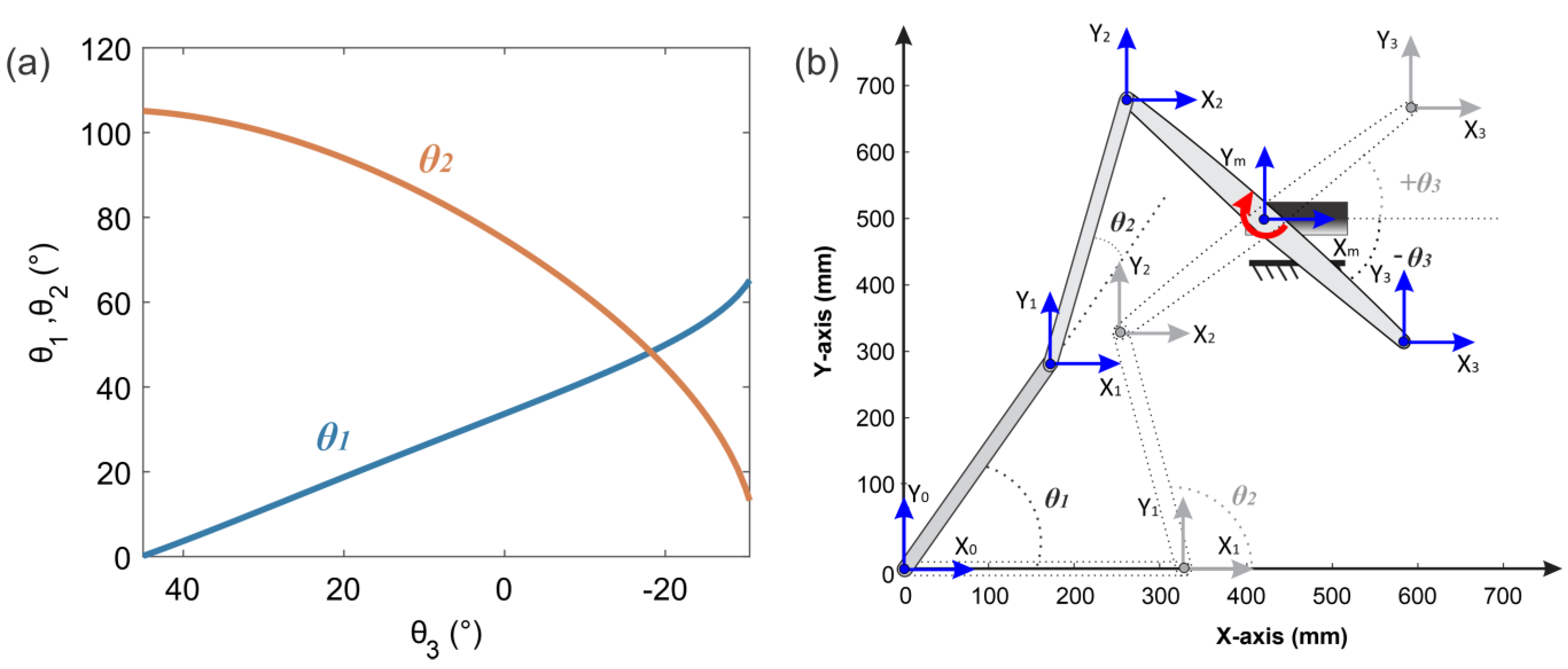
2.2.1. Kinematic Model
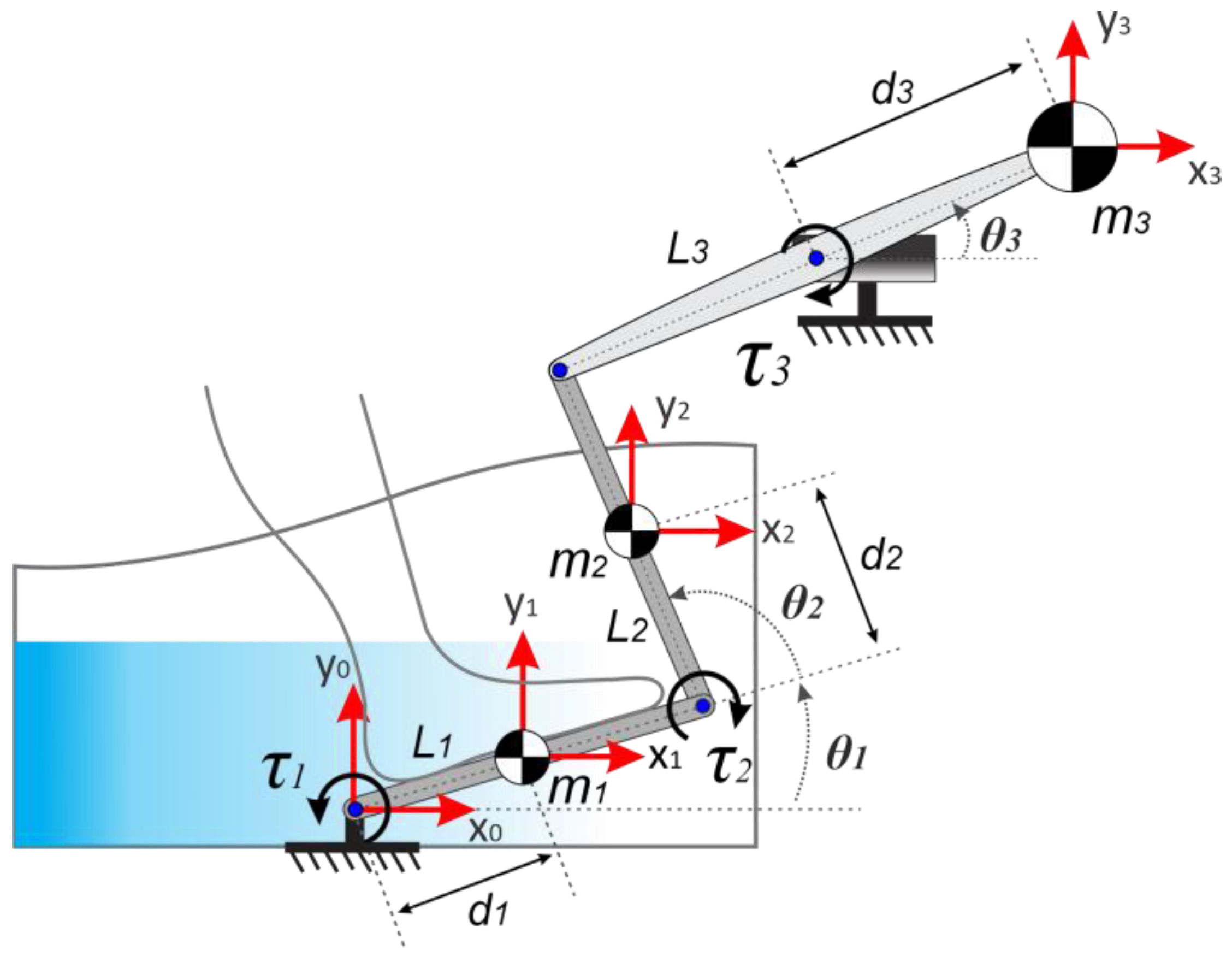
2.2.2. Dynamic Model
2.2.3. Control Strategy of the Ankle Rehabilitation Robot
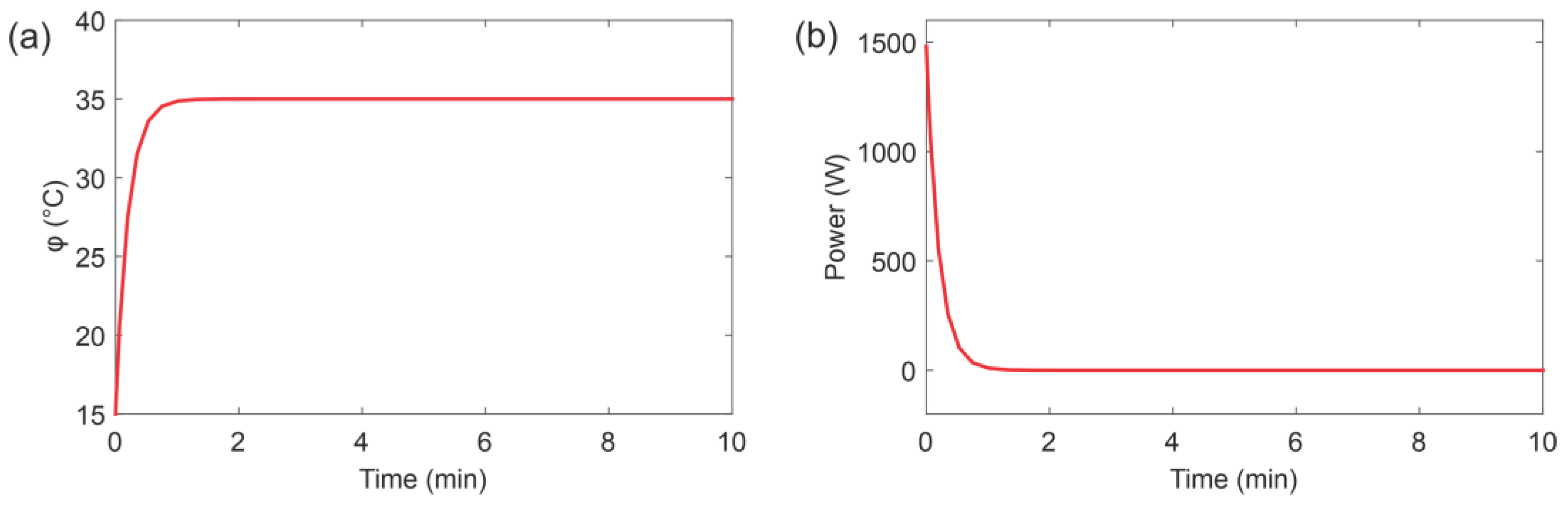
2.3. Modeling and Control of the Hot Water Recirculation System
3. Results
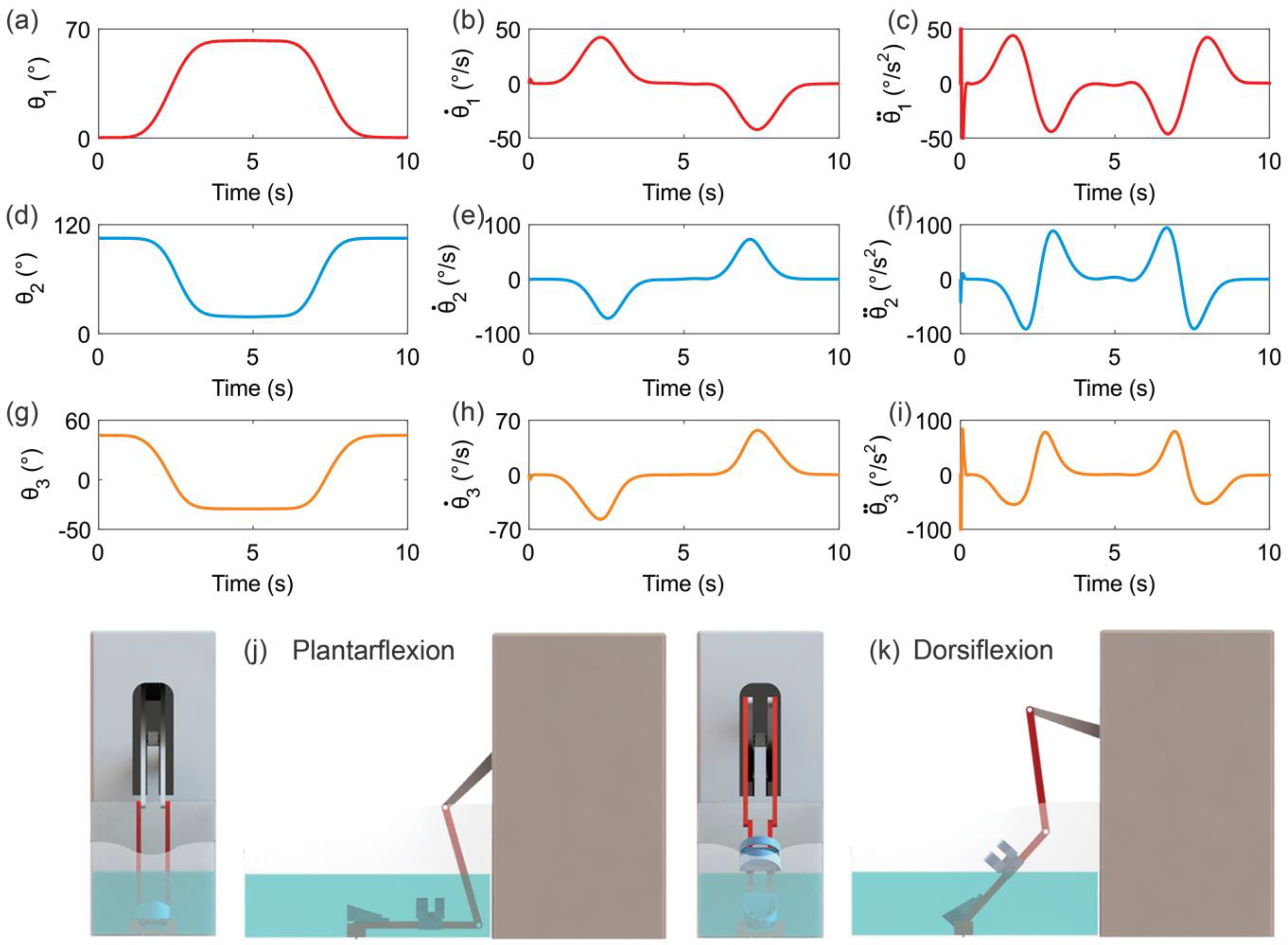
3.1. Kinematic Simulation
3.2. Hot Water Recirculation System Simulation
3.3. Dynamic Simulation
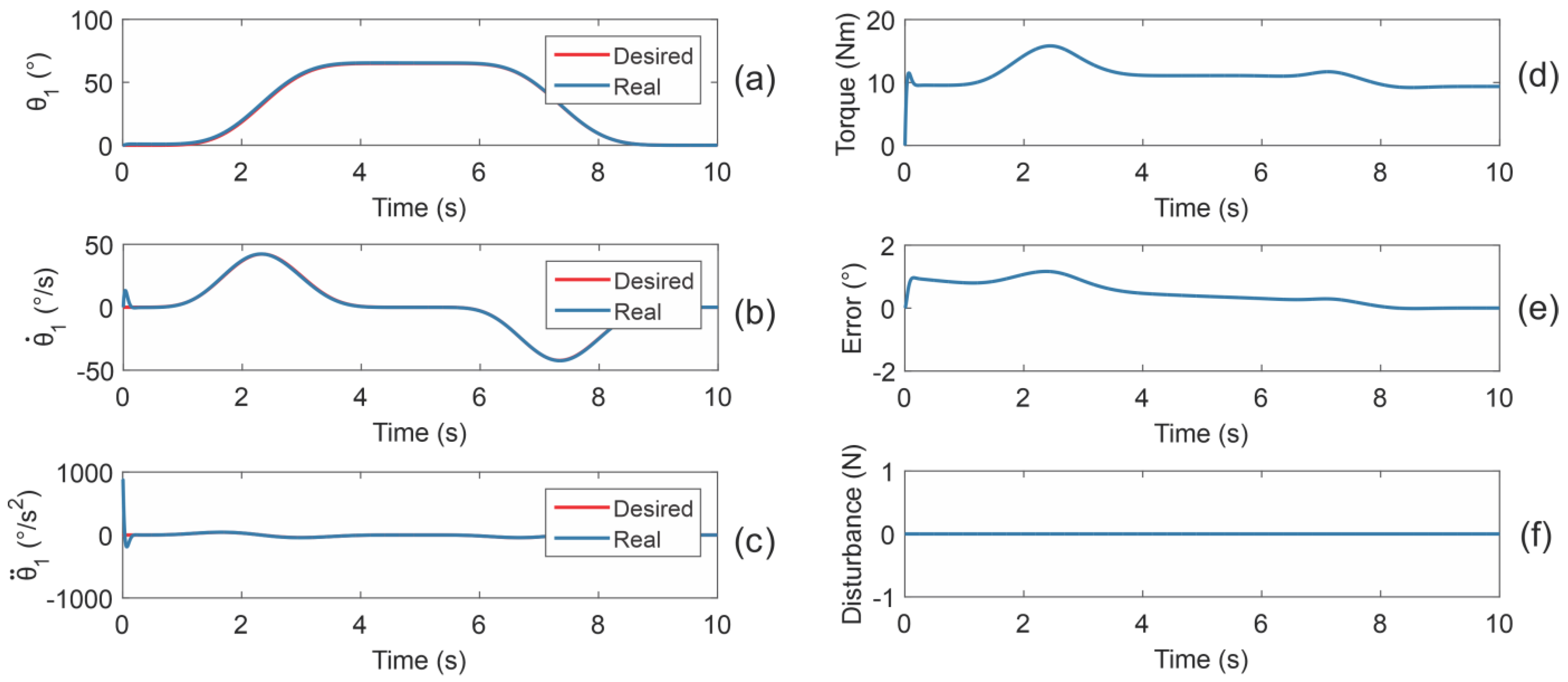
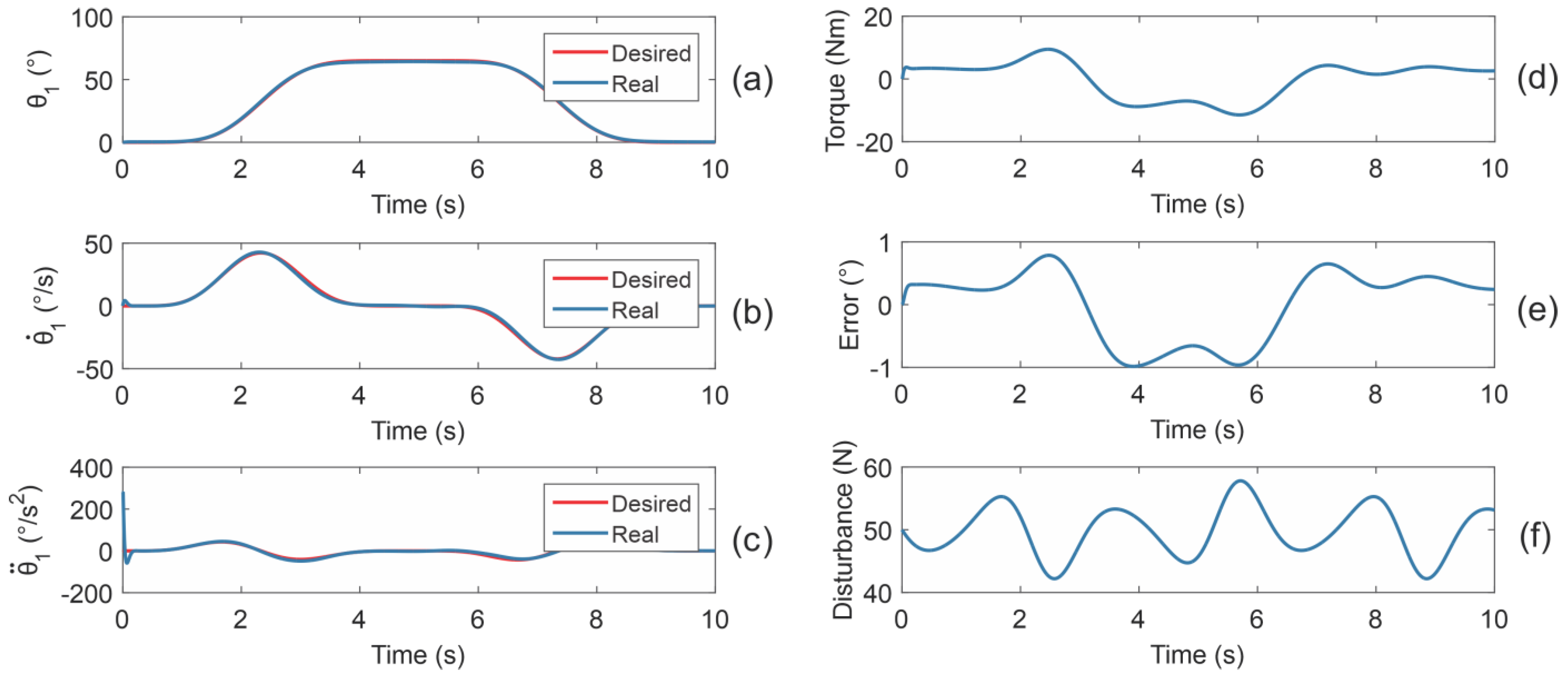
3.3.1. Reference Trajectory Tracking Simulations Using the Dynamic Model
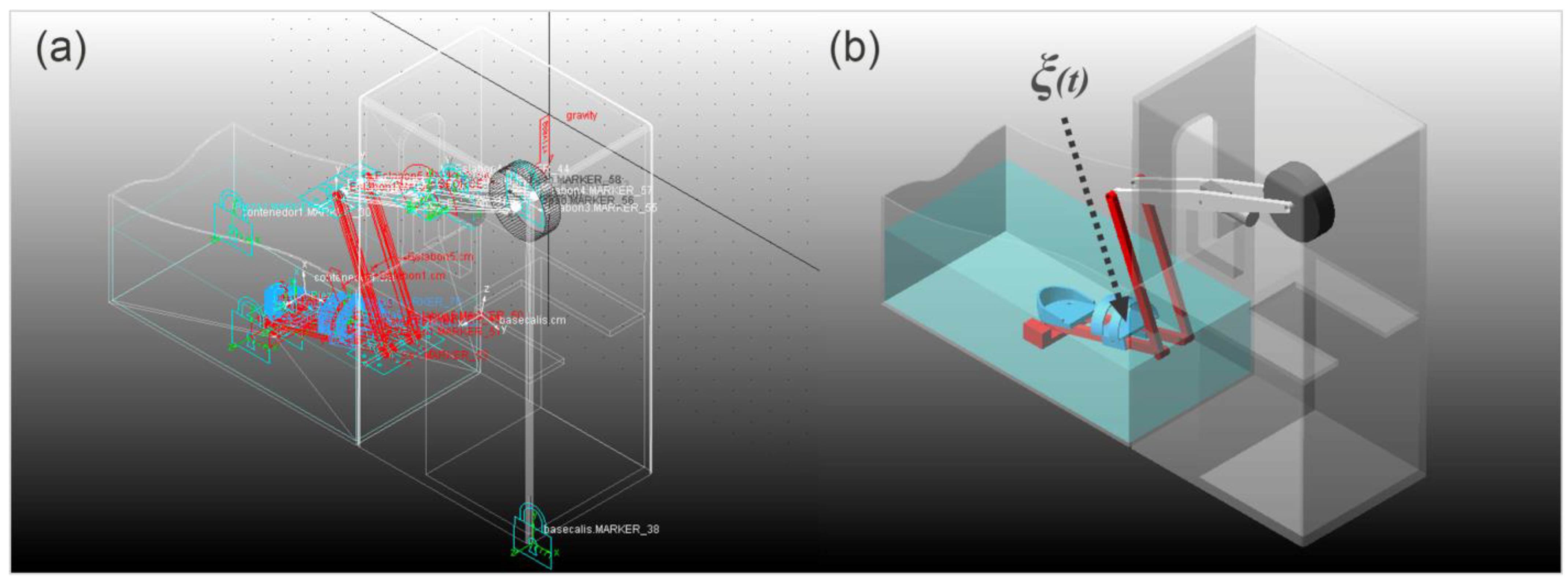
3.3.2. Reference Trajectory Tracking Simulations Using a Virtual Prototype
3.4. Experimental Results
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Delahunt, E.; Remus, A. Risk factors for lateral ankle sprains and chronic ankle instability. J. Athl. Train. 2019, 54, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Kisner, C.; Colby, L.A. Therapeutic Exercise: Foundations and Techniques, 6th ed.; F.A. Davis Company: Philadelphia, PA, USA, 2012; pp. 849–894. [Google Scholar]
- Guzmán Valdivia, C.H.; Carrera Escobedo, J.L.; Blanco Ortega, A.; Oliver Salazar, M.A.; Gómez Becerra, F.A. Diseño y control de un sistema interactivo para la rehabilitación de tobillo: TobiBot. Ing. Mecánica Tecnol. Desarro. 2014, 5, 255–264. [Google Scholar]
- Becker, B.E. Aquatic therapy: Scientific foundations and clinical rehabilitation applications. PM&R 2009, 1, 859–872. [Google Scholar] [CrossRef]
- Baena-Beato, P.Á.; Artero, E.G.; Arroyo-Morales, M.; Robles-Fuentes, A.; Gatto-Cardia, M.C.; Delgado-Fernández, M. Aquatic therapy improves pain, disability, quality of life, body composition and fitness in sedentary adults with chronic low back pain. A controlled clinical trial. Clin. Rehabil. 2014, 28, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Bender, T.; Karagülle, Z.; Bálint, G.P.; Gutenbrunner, C.; Bálint, P.V.; Sukenik, S. Hydrotherapy, balneotherapy, and spa treatment in pain management. Rheumatol. Int. 2005, 25, 220–224. [Google Scholar] [CrossRef] [PubMed]
- Prins, J.; Cutner, D. Aquatic therapy in the rehabilitation of athletic injuries. Clin. Sports Med. 1999, 18, 447–461. [Google Scholar] [CrossRef]
- Levin, S. Aquatic Therapy: A splashing success for arthritis and injury rehabilitation. Physician Sportsmed. 1991, 19, 119–126. [Google Scholar] [CrossRef]
- Broach, E.; Dattilo, J. Aquatic therapy: A viable therapeutic recreation intervention. Ther. Recreat. J. 1996, 30, 213–229. [Google Scholar]
- Konlian, C. Aquatic therapy: Making a wave in the treatment of low back injuries. Orthop. Nurs. 1999, 18, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, M.W.; UHL, T.L.; Mattacola, C.G.; Mccluskey, L.C. Management of Ankle Sprains. Am. Fam. Physician 2001, 63, 93–105. [Google Scholar]
- Pournot, H.; Bieuzen, F.; Duffield, R.; Lepretre, P.M.; Cozzolino, C.; Hausswirth, C. Short term effects of various water immersions on recovery from exhaustive intermittent exercise. Eur. J. Appl. Physiol. 2011, 111, 1287–1295. [Google Scholar] [CrossRef]
- McNeal, R.L. Aquatic therapy for patients with rheumatic disease. Rheum. Dis. Clin. N. Am. 1990, 16, 915–929. [Google Scholar] [CrossRef]
- Thompson, C.; Kelsberg, G.; St Anna, L.; Poddar, S. Clinical inquiries. Heat or ice for acute ankle sprain? J. Fam. Pract. 2003, 52, 642–643. [Google Scholar] [PubMed]
- Nordin, M.; Frankel, V.H. Basic Biomechanics of the Musculoskeletal System, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012; pp. 803–835. [Google Scholar]
- Hinman, R.S.; Heywood, S.E.; Day, A.R. Aquatic physical therapy for hip and knee osteoarthritis: Results of a single-blind randomized controlled trial. Phys. Ther. 2007, 87, 32–43. [Google Scholar] [CrossRef]
- Krebs, H.I.; Dipietro, L.; Levy-Tzedek, S.; Fasoli, S.E.; Rykman-Berland, A.; Zipse, J.; Fawcett, J.A.; Stein, J.; Poizner, H.; Lo, A.C.; et al. A paradigm shift for rehabilitation robotics. IEEE Eng. Med. Biol. Mag. 2008, 27, 61–70. [Google Scholar] [CrossRef]
- Tejima, N. Rehabilitation robotics: A review. Adv. Robot. 2001, 14, 551–564. [Google Scholar] [CrossRef]
- Rodríguez-León, J.F.; Chaparro-Rico, B.D.M.; Russo, M.; Cafolla, D. An Autotuning Cable-Driven Device for Home Rehabilitation. J. Healthc. Eng. 2021, 2021, 6680762. [Google Scholar] [CrossRef]
- Hussain, S.; Jamwal, P.K.; Vliet, P.V.; Brown, N.A.T. Robot Assisted Ankle Neuro-Rehabilitation: State of the art and Future Challenges. Expert Rev. Neurother. 2021, 21, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Guzmán-Valdivia, C.H.; Blanco-Ortega, A.; Oliver-Salazar, M.A.; Gómez-Becerra, F.A.; Carrera-Escobedo, J.L. HipBot–The design, development and control of a therapeutic robot for hip rehabilitation. Mechatronics 2015, 30, 55–64. [Google Scholar] [CrossRef]
- Becerra, F.A.G.; Ortega, A.B.; Beltrán, C.D.G.; Valdivia, C.H.G.; Arcega, R.O.D. Design and control of a new parallel robot for the rehabilitation of the hip-knee. IEEE Lat. Am. Trans. 2018, 16, 1314–1319. [Google Scholar] [CrossRef]
- Azcaray, H.; Blanco, A.; García, C.; Adam, M.; Reyes, J.; Guerrero, G.; Guzmán, C. Robust GPI Control of a New Parallel Rehabilitation Robot of Lower Extremities. Int. J. Control Autom. Syst. 2018, 16, 2384–2392. [Google Scholar] [CrossRef]
- Guzmán, C.H.; Blanco, A.; Brizuela, J.A.; Gómez, F.A. Robust control of a hip–joint rehabilitation robot. Biomed. Signal Process. Control 2017, 35, 100–109. [Google Scholar] [CrossRef]
- Khalid, Y.M.; Gouwanda, D.; Parasuraman, S. A review on the mechanical design elements of ankle rehabilitation robot. Proc. Inst. Mech. Eng. Part H 2015, 229, 452–463. [Google Scholar] [CrossRef]
- Wang, X.; Wang, H.; Hu, X.; Tian, Y.; Lin, M.; Yan, H.; Niu, J.; Sun, L. Adaptive Direct Teaching Control with Variable Load of the Lower Limb Rehabilitation Robot (LLR-II). Machines 2021, 9, 142. [Google Scholar] [CrossRef]
- Díaz, I.; Gil, J.J.; Sánchez, E. Lower-limb robotic rehabilitation: Literature review and challenges. J. Robot. 2011, 2011, 759764. [Google Scholar] [CrossRef]
- Li, J.; Fan, W.; Dong, M.; Rong, X. Research on control strategies for ankle rehabilitation using parallel mechanism. Cogn. Comput. Syst. 2020, 2, 105–111. [Google Scholar] [CrossRef]
- Alcocer, W.; Vela, L.; Blanco, A.; González, J.; Oliver, M. Major trends in the development of ankle rehabilitation devices. Dyna 2012, 176, 45–55. [Google Scholar]
- Blaya, J.A.; Herr, H. Adaptive control of a variable-impedance ankle-foot orthosis to assist drop-foot gait. IEEE Trans. Neural Syst. Rehabil. Eng. 2004, 12, 24–31. [Google Scholar] [CrossRef] [PubMed]
- Ferris, D.P.; Czerniecki, J.M.; Hannaford, B. An ankle-foot orthosis powered by artificial pneumatic muscles. J. Appl. Biomech. 2005, 21, 189–197. [Google Scholar] [CrossRef] [Green Version]
- Hussain, S.; Xie, S.Q.; Jamwal, P.K. Effect of cadence regulation on muscle activation patterns during robot assisted gait: A dynamic simulation study. IEEE J. Biomed. Health Inform. 2013, 17, 442–451. [Google Scholar] [CrossRef]
- Saglia, J.A.; Tsagarakis, N.G.; Dai, J.S.; Caldwell, D.G. A high-performance redundantly actuated parallel mechanism for ankle rehabilitation. Int. J. Robot. Res. 2009, 28, 1216–1227. [Google Scholar] [CrossRef]
- Yoon, J.; Ryu, J.; Lim, K.B. Reconfigurable ankle rehabilitation robot for various exercises. J. Robot. Syst. 2006, 22, 15–33. [Google Scholar] [CrossRef]
- Jamwal, P.K.; Hussain, S.; Mir-Nasiri, N.; Ghayesh, M.H.; Xie, S.Q. Tele-rehabilitation using in-house wearable ankle rehabilitation robot. Assist. Technol. 2018, 30, 24–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, M.; McDaid, A.; Veale, A.J.; Peng, Y.; Xie, S.Q. Adaptive Trajectory tracking control of a parallel ankle rehabilitation robot with joint-space force distribution. IEEE Access 2019, 7, 85812–85820. [Google Scholar] [CrossRef]
- Chang, T.C.; Zhang, X.D. Kinematics and reliable analysis of decoupled parallel mechanism for ankle rehabilitation. Microelectron. Reliab. 2019, 99, 203–212. [Google Scholar] [CrossRef]
- Liu, Q.; Wang, C.; Long, J.J.; Sun, T.; Duan, L.; Zhang, X.; Zhang, B.; Shen, Y.; Shang, W.; Lin, Z.; et al. Development of a New Robotic Ankle Rehabilitation Platform for Hemiplegic Patients after Stroke. J. Healthc. Eng. 2018, 2018, 3867243. [Google Scholar] [CrossRef] [Green Version]
- Ai, Q.; Zhu, C.; Zuo, J.; Meng, W.; Liu, Q.; Xie, S.Q.; Yang, M. Disturbance-Estimated Adaptive Backstepping Sliding Mode Control of a Pneumatic Muscles-Driven Ankle Rehabilitation Robot. Sensors 2018, 18, 66. [Google Scholar] [CrossRef] [Green Version]
- Jamwal, P.K.; Hussain, S.; Ghayesh, M.H.; Rogozina, S.V. Impedance control of an intrinsically compliant parallel ankle rehabilitation robot. IEEE Trans. Ind. Electron. 2016, 63, 3638–3647. [Google Scholar] [CrossRef]
- Ayas, M.S.; Altas, I.H. Fuzzy logic based adaptive admittance control of a redundantly actuated ankle rehabilitation robot. Control Eng. Pract. 2017, 59, 44–54. [Google Scholar] [CrossRef]
- Covaciu, F.; Pisla, A.; Iordan, A.-E. Development of a Virtual Reality Simulator for an Intelligent Robotic System Used in Ankle Rehabilitation. Sensors 2021, 21, 1537. [Google Scholar] [CrossRef]
- Abu-Dakka, F.J.; Valera, A.; Escalera, J.A.; Abderrahim, M.; Page, A.; Mata, V. Passive Exercise Adaptation for Ankle Rehabilitation Based on Learning Control Framework. Sensors 2020, 20, 6215. [Google Scholar] [CrossRef]
- Zuo, S.; Li, J.; Dong, M.; Zhou, X.; Fan, W.; Kong, Y. Design and Performance Evaluation of a Novel Wearable Parallel Mechanism for Ankle Rehabilitation. Front. Neurorobot. 2020, 14, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Liu, C.; Liu, T.; Qi, K.; Niu, J.; Guo, S. Module combination based configuration synthesis and kinematic analysis of generalized spherical parallel mechanism for ankle rehabilitation. Mech. Mach. Theory 2021, 166, 104436. [Google Scholar] [CrossRef]
- Russo, M.; Ceccarelli, M. Analysis of a Wearable Robotic System for Ankle Rehabilitation. Machines 2020, 8, 48. [Google Scholar] [CrossRef]
- Hau, C.T.; Gouwanda, D.; Gopalai, A.A.; Low, C.Y.; Hanapiah, F.A. Gamification and Control of Nitinol Based Ankle Rehabilitation Robot. Biomimetics 2021, 6, 53. [Google Scholar] [CrossRef]
- Alvarez-Perez, M.G.; Garcia-Murillo, M.A.; Cervantes-Sánchez, J.J. Robot-assisted ankle rehabilitation: A review. Disabil. Rehabil. Assist. Technol. 2020, 15, 394–408. [Google Scholar] [CrossRef]
- Blanco, A.; Gómez, F.A.; Olivares, V.H.; Abundez, A.; Colín, J. Design and development of a parallel robot based on an XY table for ankle rehabilitation. Int. J. Autom. Control 2015, 9, 89–106. [Google Scholar] [CrossRef]
- Hollands, K.G.T.; Raithby, G.D.; Konicek, L. Correlation equations for free convection heat transfer in horizontal layers of air and water. Int. J. Heat Mass Transf. 1974, 18, 879–884. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value (mm) |
|---|---|
| 0 | |
| 420 | |
| 496 | |
| 330 | |
| 330 | |
| 500 |
| Parameter | Value |
|---|---|
| 16.97 °C s/kcal | |
| 37 kcal/°C | |
| 0.05890 kg/s | |
| 37 kg | |
| 15 °C | |
| 35 °C | |
| 100 |
| Parameter | Value |
|---|---|
| 330 mm | |
| 500 mm | |
| 165 mm | |
| 250 mm | |
| 0.437 kg | |
| 0.244 kg | |
| 5.783 kg | |
| 0.1 Ns/m |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guzmán-Valdivia, C.H.; Madrigal-López, O.; Désiga-Orenday, O.; Talavera-Otero, J.; Brizuela-Mendoza, J.A.; Chávez-Olivares, C.A.; Cruz-Domínguez, O.; Blanco-Ortega, A.; Berumen-Torres, J.A.; Gómez-Becerra, F.A. Design, Development and Control of a Therapeutic Robot Incorporating Aquatic Therapy for Ankle Rehabilitation. Machines 2021, 9, 254. https://doi.org/10.3390/machines9110254
Guzmán-Valdivia CH, Madrigal-López O, Désiga-Orenday O, Talavera-Otero J, Brizuela-Mendoza JA, Chávez-Olivares CA, Cruz-Domínguez O, Blanco-Ortega A, Berumen-Torres JA, Gómez-Becerra FA. Design, Development and Control of a Therapeutic Robot Incorporating Aquatic Therapy for Ankle Rehabilitation. Machines. 2021; 9(11):254. https://doi.org/10.3390/machines9110254
Chicago/Turabian StyleGuzmán-Valdivia, César H., Oscar Madrigal-López, Omar Désiga-Orenday, Jorge Talavera-Otero, Jorge A. Brizuela-Mendoza, César A. Chávez-Olivares, Oscar Cruz-Domínguez, Andrés Blanco-Ortega, Javier Alejandro Berumen-Torres, and Fabio Abel Gómez-Becerra. 2021. "Design, Development and Control of a Therapeutic Robot Incorporating Aquatic Therapy for Ankle Rehabilitation" Machines 9, no. 11: 254. https://doi.org/10.3390/machines9110254