Digitized ADOS: Social Interactions beyond the Limits of the Naked Eye



Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Materials and Methods
2.1. Ethics Information
2.2. Design
2.3. Sampling Plan and Inclusion/Exclusion Criteria
2.4. Analysis Plan
2.5. Data Types
2.6. Socio-Motor Metrics
3. Results
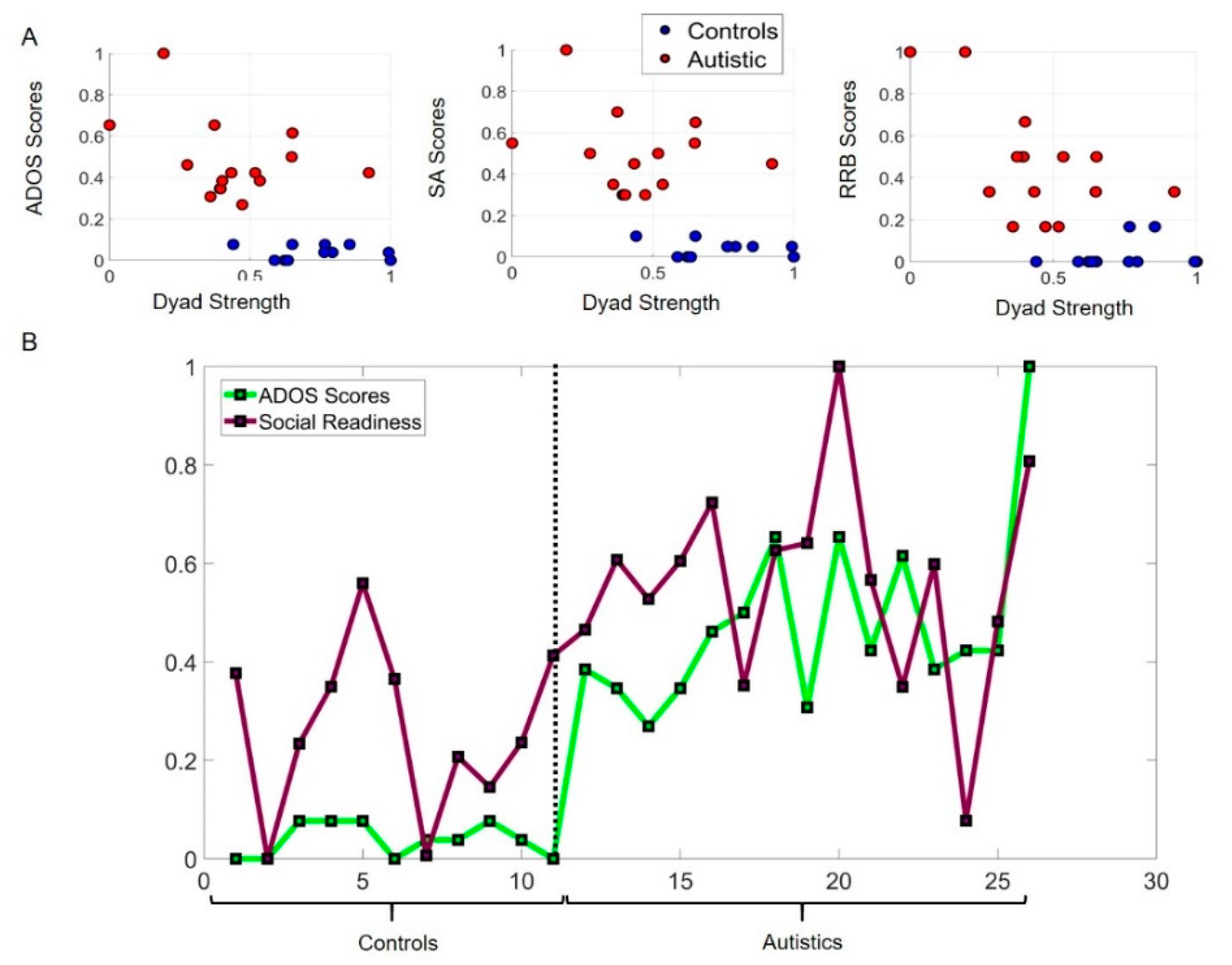
3.1. Potential for Social Readiness Revealed by Micro-Level Socio-Motor Biometrics Is Missed by Macro-Level Criteria
3.2. Mirroring of Social Actions Inevitably Biases the Rater
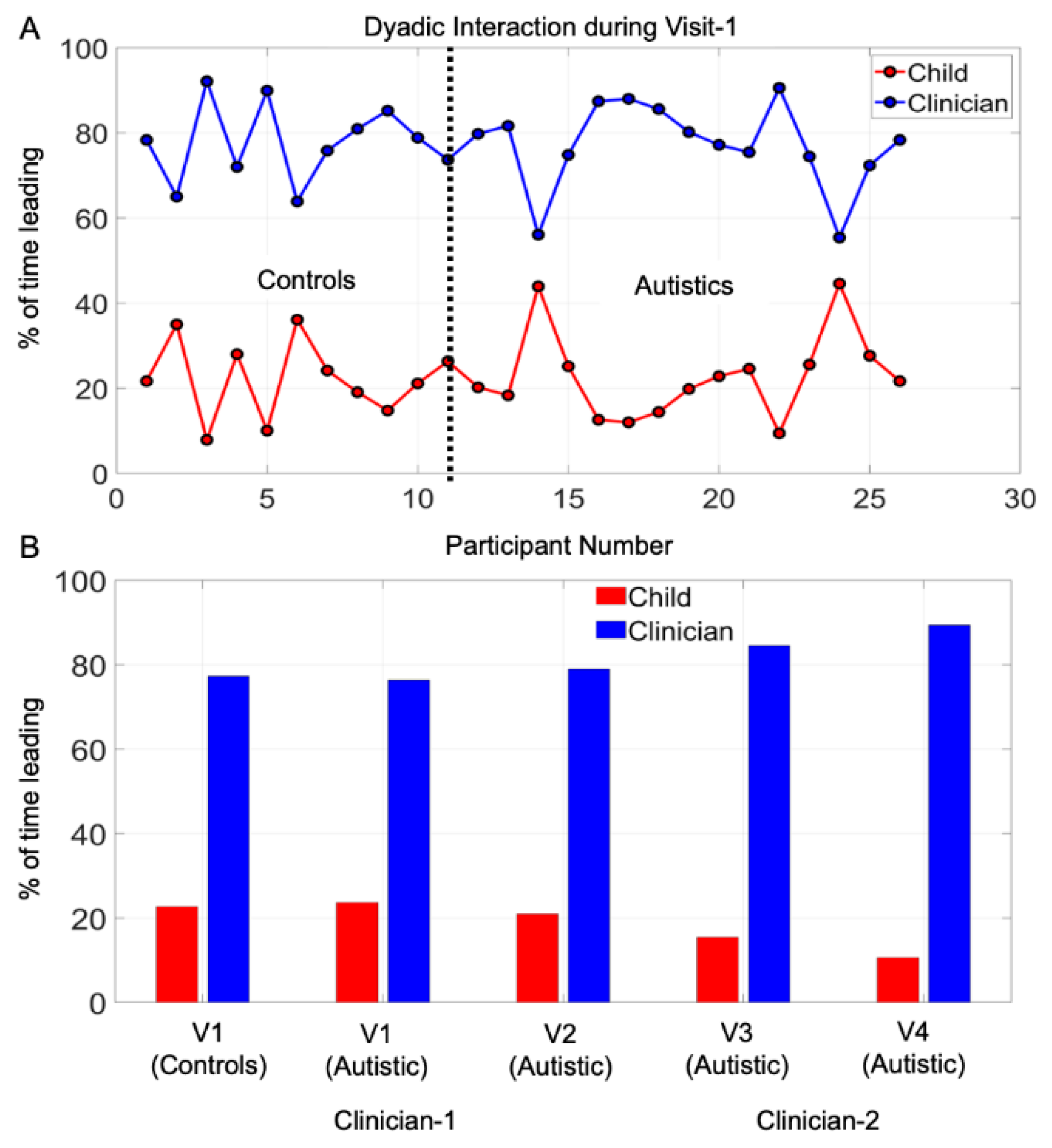
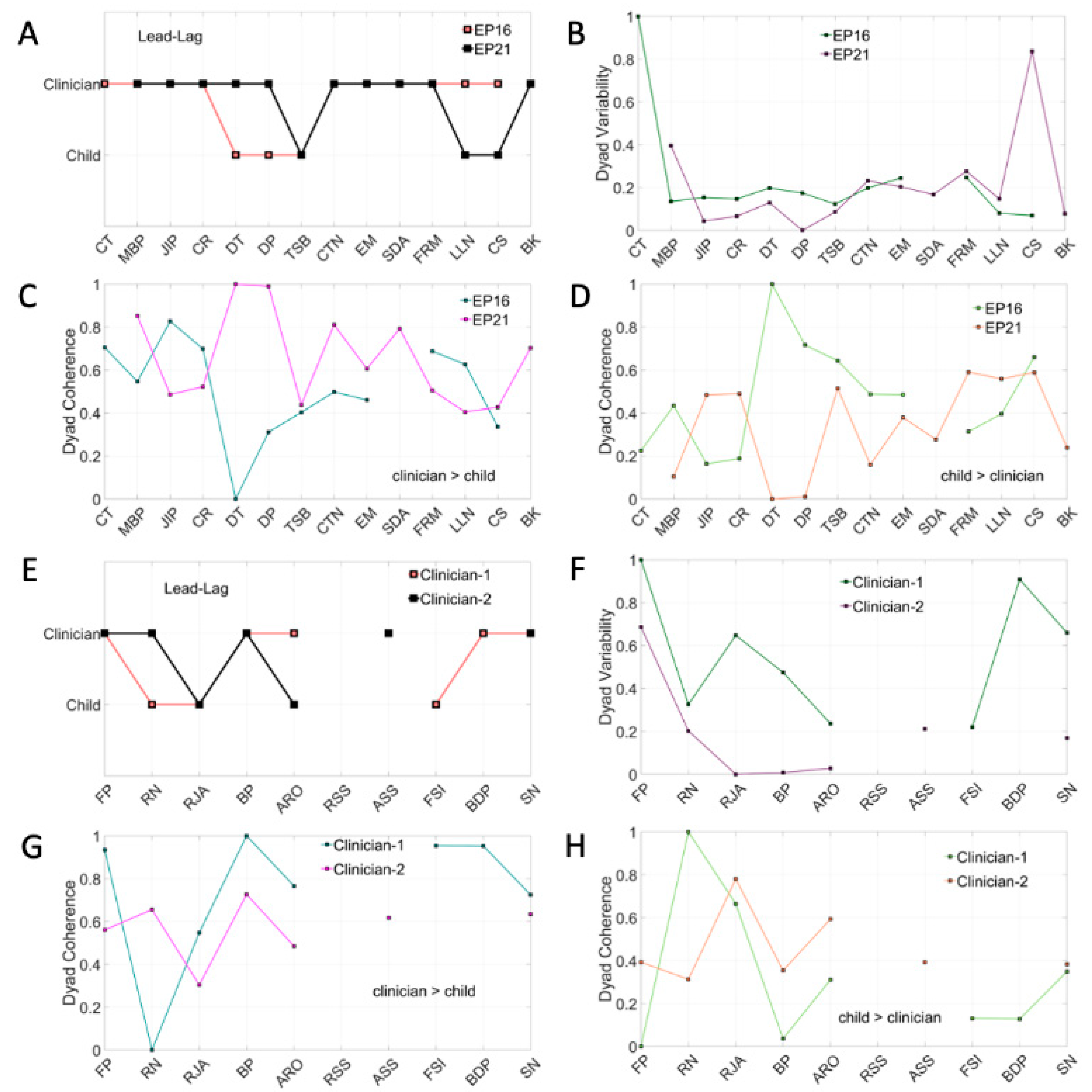
3.3. Systematic Leading Bias of Rater Remains Across ADOS Modules and Familiarity with the Child
3.4. The ADOS Test Probing Appropriateness in Social Interactions Is Administered as a Monologue
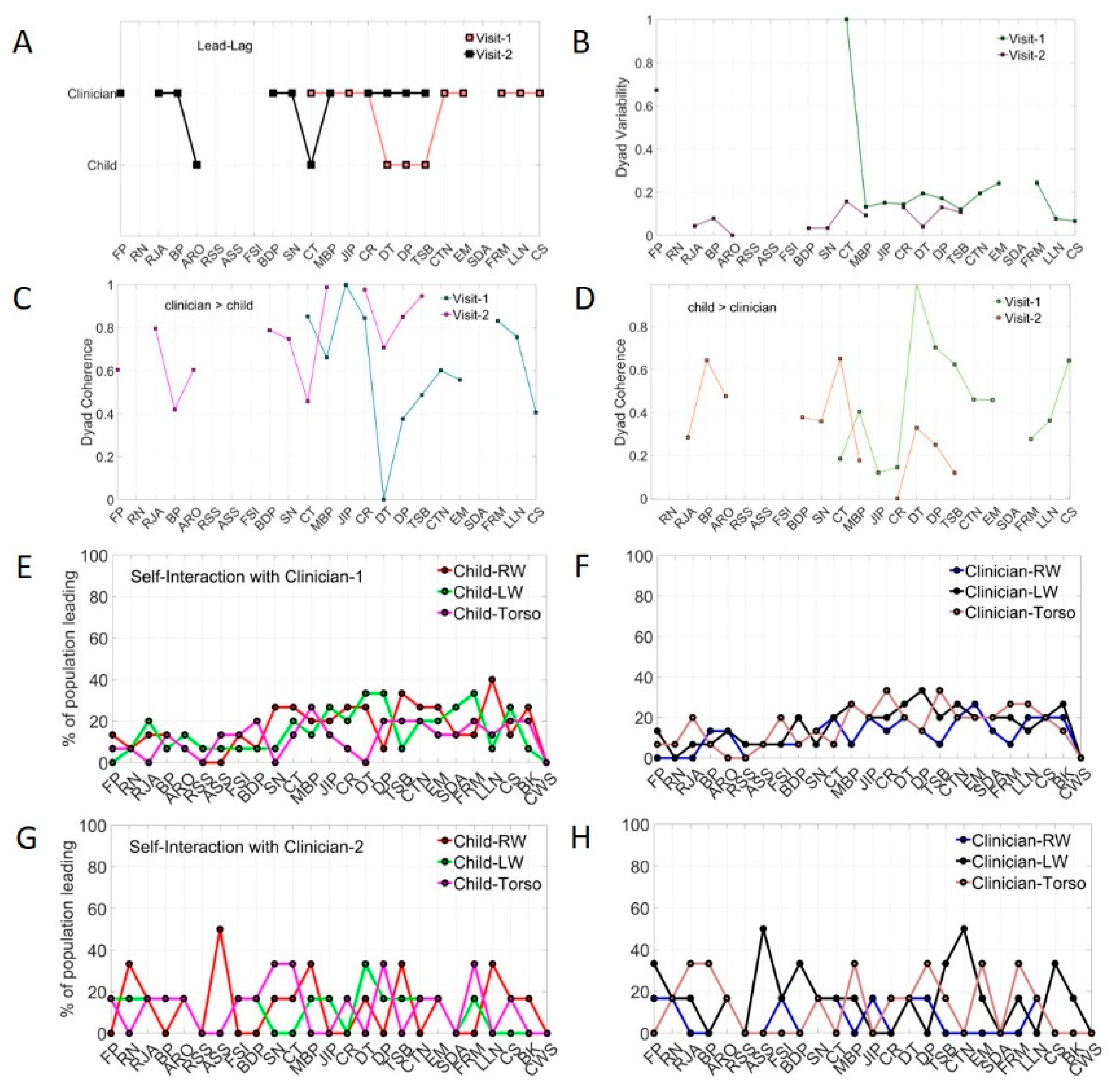
3.5. Micro-Level Analyses Capture Socio-Motor Changes Missed by Macro-Level Scores
3.6. High Sensitivity to Change in Clinician Across All Children of the Cohort
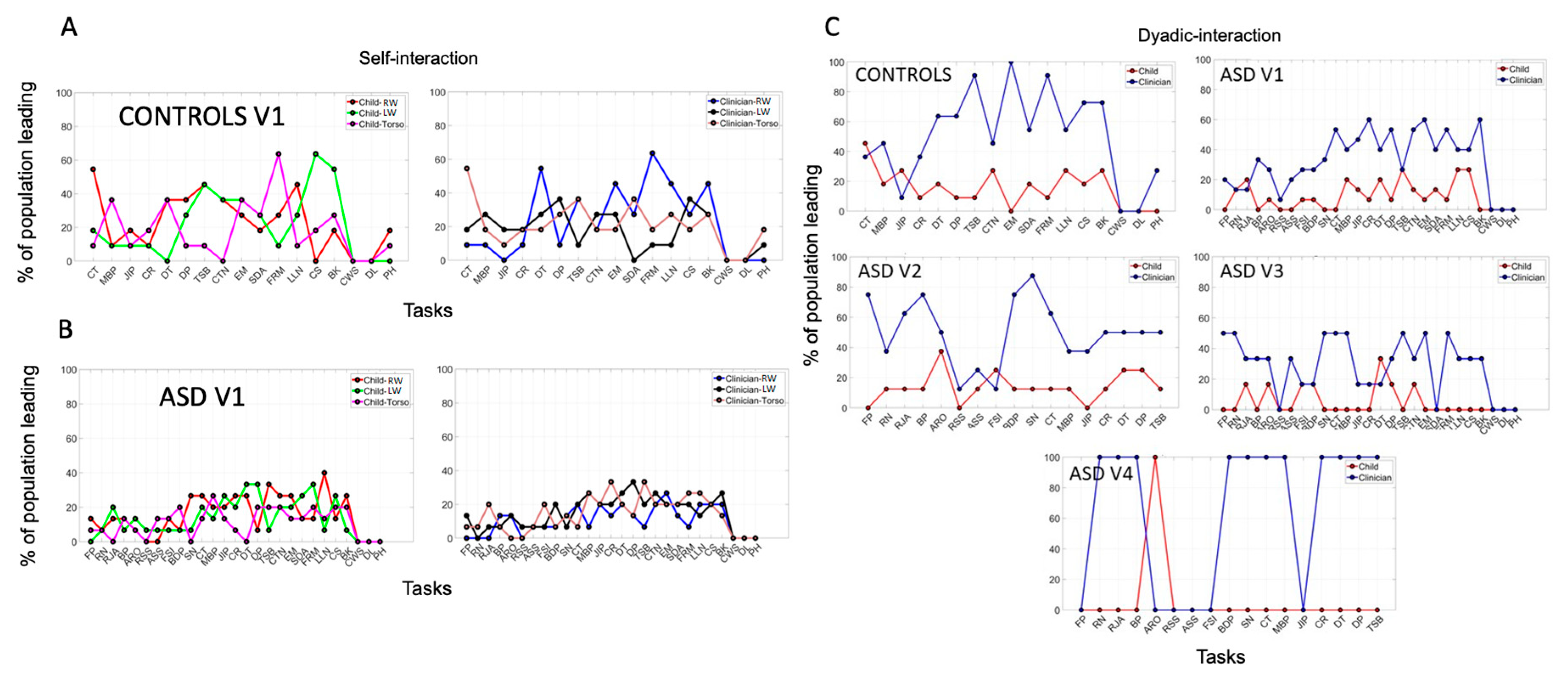
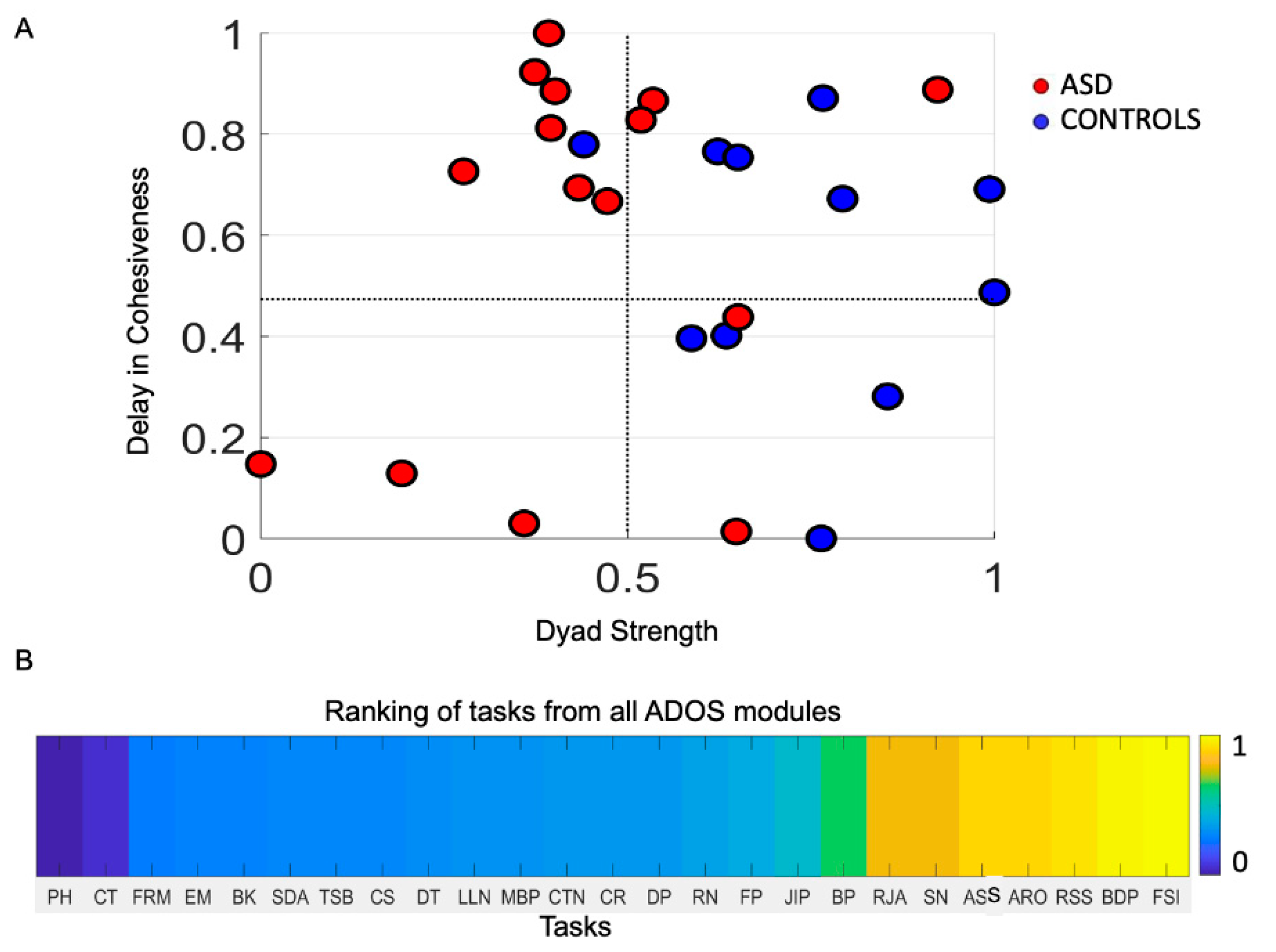
3.7. Stratification of Sub-Types in Autism Is Not Possible Using Macro-Level Criteria Alone
3.8. Two Different Clinicians Perceive the Same Child’s Socio-Motor Patterns Highly Differently
3.9. Task Ranking and Target Treatment
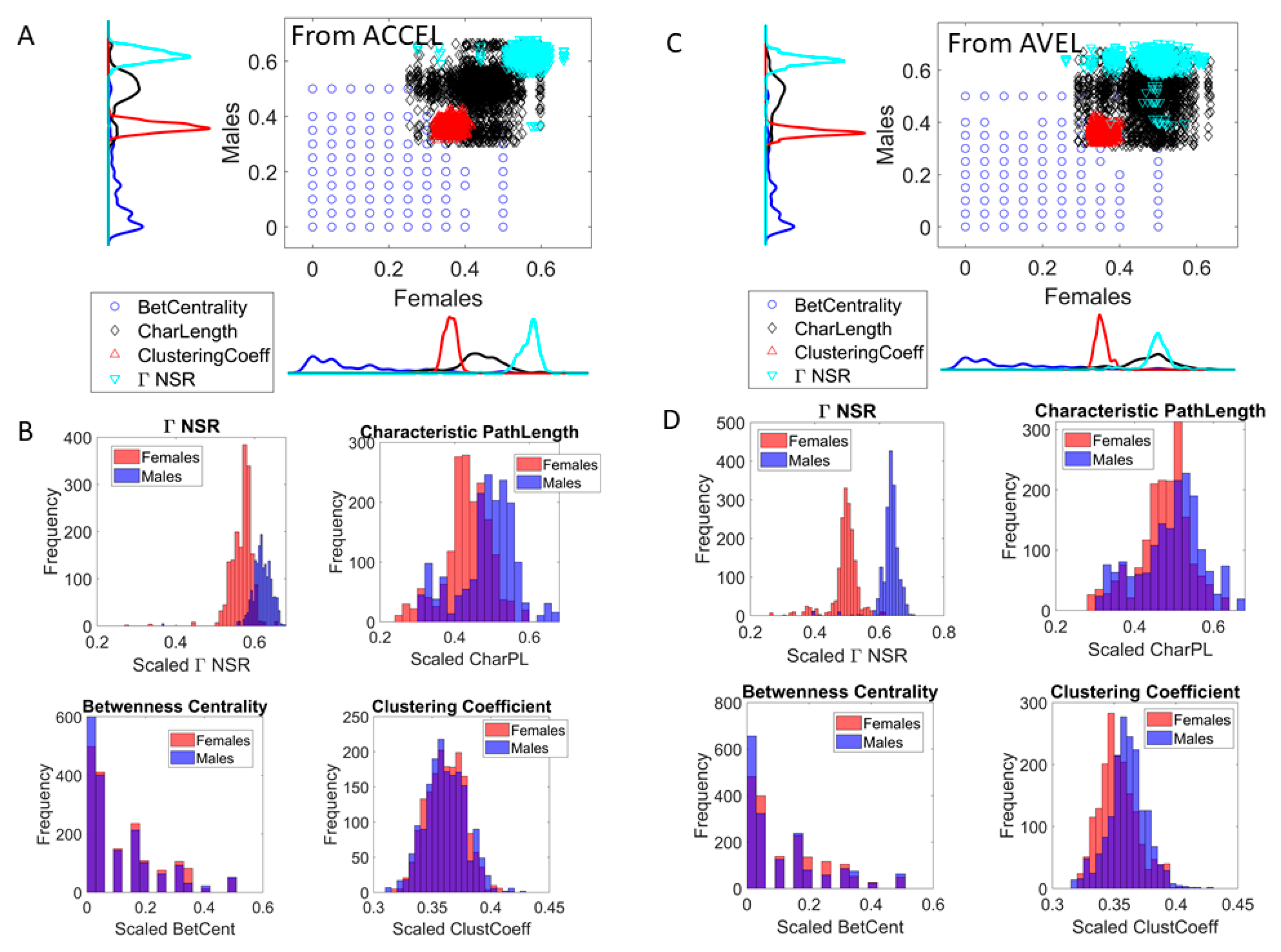
3.10. The Digitazed ADOS Separates Males and Females Using Network Connectivity Metrics and Noise to Signal Ratio (NSR)
4. Discussion
Caveats and Limitations of the Proposed Hybrid Methods
5. Conclusions
6. Patents
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cowlyn, T. Maternal Voice and Communicative Musicality: Sharing the Meaning of Life Before Birth. In Early Vocal Contact and Preterm Infant Brain Development: Bridging the Gap between Research and Practice; Filippa, M., Kuhn, P., Westup, B., Eds.; Springer: Cham, Switzerland, 2017; pp. 3–24. [Google Scholar]
- Moon, C. Prenatal Experience with the Maternal Voice. In Early Vocal Contact and Preterm Infant Brain Development: Bridging the Gap between Research and Practice; Filippa, M., Kuhn, P., Westrup, B., Eds.; Springer: Cham, Switzerland, 2017; pp. 25–38. [Google Scholar]
- Trehub, S.E. The Maternal Voice as a Special Signal for Infants. In Early Vocal Contact and Preterm Infant Brain Development: Bridging the Gap between Research and Practice; Filippa, M., Kuhn, P., Westrup, B., Eds.; Springer: Cham, Switzerland, 2017; pp. 39–55. [Google Scholar]
- Gratier, M.; Devouche, E. The Development of Infant Participation in Communication. In Early Vocal Contact and Preterm Infant Brain Development: Bridging the Gap between Research and Practice; Filippa, M., Kuhn, P., Westrup, B., Eds.; Springer: Cham, Switzerland, 2017; pp. 55–70. [Google Scholar]
- Grandjean, D. Brain Mechanisms in Emotional Voice Production and Perception and Early Life Interactions. In Early Vocal Contact and Preterm Infant Brain Development: Bridging the Gap between Research and Practice; Filippa, M., Kuhn, P., Westrup, B., Eds.; Springer: Cham, Switzerland, 2017; pp. 71–91. [Google Scholar]
- Condon, W.S.; Sander, L.W. Synchrony demonstrated between movements of the neonate and adult speech. Child Dev. 1974, 45, 456–462. [Google Scholar] [CrossRef]
- Condon, W.S.; Sander, L.W. Neonate movement is synchronized with adult speech: Interactional participation and language acquisition. Science 1974, 183, 99–101. [Google Scholar] [CrossRef] [PubMed]
- Brazelton, T.B.; Tronick, E.; Adamson, L.; Als, H.; Wise, S. Early mother-infant reciprocity. Ciba Found. Symp. 1975, 137–154. [Google Scholar] [CrossRef]
- Gusella, J.L.; Muir, D.; Tronick, E.Z. The effect of manipulating maternal behavior during an interaction on three- and six-month-olds’ affect and attention. Child Dev. 1988, 59, 1111–1124. [Google Scholar] [CrossRef] [PubMed]
- Weinberg, M.K.; Tronick, E.Z. Beyond the face: An empirical study of infant affective configurations of facial, vocal, gestural, and regulatory behaviors. Child Dev. 1994, 65, 1503–1515. [Google Scholar] [CrossRef]
- Weinberg, M.K.; Tronick, E.Z. Infant affective reactions to the resumption of maternal interaction after the still-face. Child Dev. 1996, 67, 905–914. [Google Scholar] [CrossRef]
- Bardi, L.; Regolin, L.; Simion, F. Biological motion preference in humans at birth: Role of dynamic and configural properties. Dev. Sci. 2011, 14, 353–359. [Google Scholar] [CrossRef]
- Simion, F.; Regolin, L.; Bulf, H. A predisposition for biological motion in the newborn baby. Proc. Natl. Acad. Sci. USA 2008, 105, 809–813. [Google Scholar] [CrossRef] [Green Version]
- Reid, V.M.; Hoehl, S.; Landt, J.; Striano, T. Human infants dissociate structural and dynamic information in biological motion: Evidence from neural systems. Soc. Cogn. Affect. Neurosci. 2008, 3, 161–167. [Google Scholar] [CrossRef] [Green Version]
- Torres, E.B.; Brincker, M.; Isenhower, R.W.; Yanovich, P.; Stigler, K.A.; Nurnberger, J.I.; Metaxas, D.N.; Jose, J.V. Autism: The micro-movement perspective. Front. Integr. Neurosci. 2013, 7, 32. [Google Scholar] [CrossRef] [Green Version]
- Torres, E.B.; Yanovich, P.; Metaxas, D.N. Give spontaneity and self-discovery a chance in ASD: Spontaneous peripheral limb variability as a proxy to evoke centrally driven intentional acts. Front. Integr. Neurosci. 2013, 7, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konczak, J.; Borutta, M.; Topka, H.; Dichgans, J. The development of goal-directed reaching in infants: Hand trajectory formation and joint torque control. Exp. Brain Res. 1995, 106, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Thelen, E. Dynamic Mechanisms of Change in Early Perceptual-Motor Development. In Mechanisms of Cognitive Development: Behavioral and Neural Perspectives; McClelland, J., Siegler, R.S., Eds.; Lawrence Erlbaum Associates Inc.: Mahwah, NJ, USA; London, UK, 2001; pp. 161–184. [Google Scholar]
- Torres, E.B.; Smith, B.; Mistry, S.; Brincker, M.; Whyatt, C. Neonatal Diagnostics: Toward Dynamic Growth Charts of Neuromotor Control. Front. Pediatr. 2016, 4, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Delafield-Butt, J.T.; Freer, Y.; Perkins, J.; Skulina, D.; Schogler, B.; Lee, D.N. Prospective organization of neonatal arm movements: A motor foundation of embodied agency, disrupted in premature birth. Dev. Sci. 2018, 21, e12693. [Google Scholar] [CrossRef] [PubMed]
- Knoblich, G.; Jordan, J.S. Action coordination in groups and individuals: Learning anticipatory control. J. Exp. Psychol. Learn Mem. Cogn. 2003, 29, 1006–1016. [Google Scholar] [CrossRef] [PubMed]
- Marsh, K.L.; Richardson, M.J.; Schmidt, R.C. Social connection through joint action and interpersonal coordination. Top. Cogn. Sci. 2009, 1, 320–339. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, R.C.; Nie, L.; Franco, A.; Richardson, M.J. Bodily synchronization underlying joke telling. Front. Hum. Neurosci. 2014, 8, 633. [Google Scholar] [CrossRef]
- Whyatt, C.; Torres, E.B. The social-dance: Decomposing Naturalistic dyadic interaction dynamics to the micro-level. In Proceedings of the Movement and Computing, London, UK, 28–30 June 2017. [Google Scholar]
- Amos, P. Rhythm and timing in autism: Learning to dance. Front. Integr. Neurosci. 2013, 7, 27. [Google Scholar] [CrossRef] [Green Version]
- Torres, E.B.; Whyatt, C. Autism: The Movement Sensing Perspective; CRC Press/Taylor & Francis Group: Boca Raton, NJ, USA, 2018; p. xviii. 386p. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Lord, C.; Risi, S.; Lambrecht, L.; Cook, E.H., Jr.; Leventhal, B.L.; DiLavore, P.C.; Pickles, A.; Rutter, M. The autism diagnostic observation schedule-generic: A standard measure of social and communication deficits associated with the spectrum of autism. J. Autism Dev. Disord. 2000, 30, 205–223. [Google Scholar] [CrossRef]
- Torres, E.B.; Rai, R.; Mistry, S.; Gupta, B. Hidden Aspects of the Research ADOS Are Bound to Affect Autism Science. Neural Comput. 2020, 32, 515–561. [Google Scholar] [CrossRef]
- Sporns, O. Networks of the Brain; MIT Press: Cambridge, MA, USA, 2011; p. xi. 412p, 418p. [Google Scholar]
- Sporns, O. Discovering the Human Connectome; MIT Press: Cambridge, MA, USA, 2012; p. xii. 232p. [Google Scholar]
- Torres, E.B.; Denisova, K. Motor noise is rich signal in autism research and pharmacological treatments. Sci. Rep. 2016, 6, 37422. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, D.; Jose, J.V.; Nurnberger, J.I.; Torres, E.B. A Biomarker Characterizing Neurodevelopment with applications in Autism. Sci. Rep. 2018, 8, 614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McClelland, J.; Koslicki, D. EMDUniFrac: Exact linear time computation of the UniFrac metric and identification of differentially abundant organisms. J. Math Biol. 2018, 77, 935–949. [Google Scholar] [CrossRef] [Green Version]
- Lleonart, J.; Salat, J.; Torres, G.J. Removing allometric effects of body size in morphological analysis. J. Theor. Biol. 2000, 205, 85–93. [Google Scholar] [CrossRef] [PubMed]
- Monge, G. Memoire sur la theorie des deblais et des remblais. In Histoire de l’ Academie Royale des Science, avec les Memoired de Mathematique et de Physique; De L’imprimerie Royale: Paris, France, 1781. [Google Scholar]
- Kalampratsidou, V.; Torres, E.B. Peripheral Network Connectivity Analyses for the Real-Time Tracking of Coupled Bodies in Motion. Sensors 2018, 18, 3117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryu, J.; Torres, E.B. The Autonomic Nervous System Differentiates Between Levels of Motor Intent and Hand Dominance. bioRxvi 2020. [Google Scholar] [CrossRef]
- Ryu, J.; Vero, J.; Dobkin, R.D.; Torres, E.B. Dynamic Digital Biomarkers of Motor and Cognitive Function in Parkinson’s Disease. J. Vis. Exp. 2019. [Google Scholar] [CrossRef] [Green Version]
- Ryu, J.; Vero, J.; Torres, E.B. Methods for Tracking Dynamically Coupled Brain-Body Activities during Natural Movement. In Proceedings of the MOCO ‘17: 4th International Conference on Movement Computing, London, UK, 28–30 June 2017; pp. 1–8. [Google Scholar]
- Torres, E.B.; Vero, J.; Rai, R. Statistical Platform for Individualized Behavioral Analyses Using Biophysical Micro-Movement Spikes. Sensors 2018, 18, 1025. [Google Scholar] [CrossRef]
- Torres, E.B.; Mistry, S.; Caballero, C.; Whyatt, C.P. Stochastic Signatures of Involuntary Head Micro-movements Can Be Used to Classify Females of ABIDE into Different Subtypes of Neurodevelopmental Disorders. Front. Integr. Neurosci. 2017, 11, 10. [Google Scholar] [CrossRef]
- Caballero, C.; Mistry, S.; Vero, J.; Torres, E.B. Characterization of Noise Signatures of Involuntary Head Motion in the Autism Brain Imaging Data Exchange Repository. Front. Integr. Neurosci. 2018, 12, 7. [Google Scholar] [CrossRef] [Green Version]
- Torres, E.B.; Isenhower, R.W.; Yanovich, P.; Rehrig, G.; Stigler, K.; Nurnberger, J.; Jose, J.V. Strategies to develop putative biomarkers to characterize the female phenotype with autism spectrum disorders. J. Neurophysiol. 2013, 110, 1646–1662. [Google Scholar] [CrossRef] [PubMed]
- Torres, E.B.; Nguyen, J.; Mistry, S.; Whyatt, C.; Kalampratsidou, V.; Kolevzon, A. Characterization of the Statistical Signatures of Micro-Movements Underlying Natural Gait Patterns in Children with Phelan McDermid Syndrome: Towards Precision-Phenotyping of Behavior in ASD. Front. Integr. Neurosci. 2016, 10, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loomes, R.; Hull, L.; Mandy, W.P.L. What Is the Male-to-Female Ratio in Autism Spectrum Disorder? A Systematic Review and Meta-Analysis. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 466–474. [Google Scholar] [CrossRef] [PubMed]
- Lundstrom, S.; Marland, C.; Kuja-Halkola, R.; Anckarsater, H.; Lichtenstein, P.; Gillberg, C.; Nilsson, T. Assessing autism in females: The importance of a sex-specific comparison. Psychiatry Res. 2019, 282, 112566. [Google Scholar] [CrossRef] [PubMed]









© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bokadia, H.; Rai, R.; Torres, E.B. Digitized ADOS: Social Interactions beyond the Limits of the Naked Eye. J. Pers. Med. 2020, 10, 159. https://doi.org/10.3390/jpm10040159
Bokadia H, Rai R, Torres EB. Digitized ADOS: Social Interactions beyond the Limits of the Naked Eye. Journal of Personalized Medicine. 2020; 10(4):159. https://doi.org/10.3390/jpm10040159
Chicago/Turabian StyleBokadia, Harshit, Richa Rai, and Elizabeth Barbara Torres. 2020. "Digitized ADOS: Social Interactions beyond the Limits of the Naked Eye" Journal of Personalized Medicine 10, no. 4: 159. https://doi.org/10.3390/jpm10040159
APA StyleBokadia, H., Rai, R., & Torres, E. B. (2020). Digitized ADOS: Social Interactions beyond the Limits of the Naked Eye. Journal of Personalized Medicine, 10(4), 159. https://doi.org/10.3390/jpm10040159