
Thermal, Hyperspectral, and Laser Doppler Imaging: Non-Invasive Tools for Detection of The Deep Inferior Epigastric Artery Perforators—A Prospective Comparison Study

 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Detection Devices
2.2. Study Design & Patient Collective
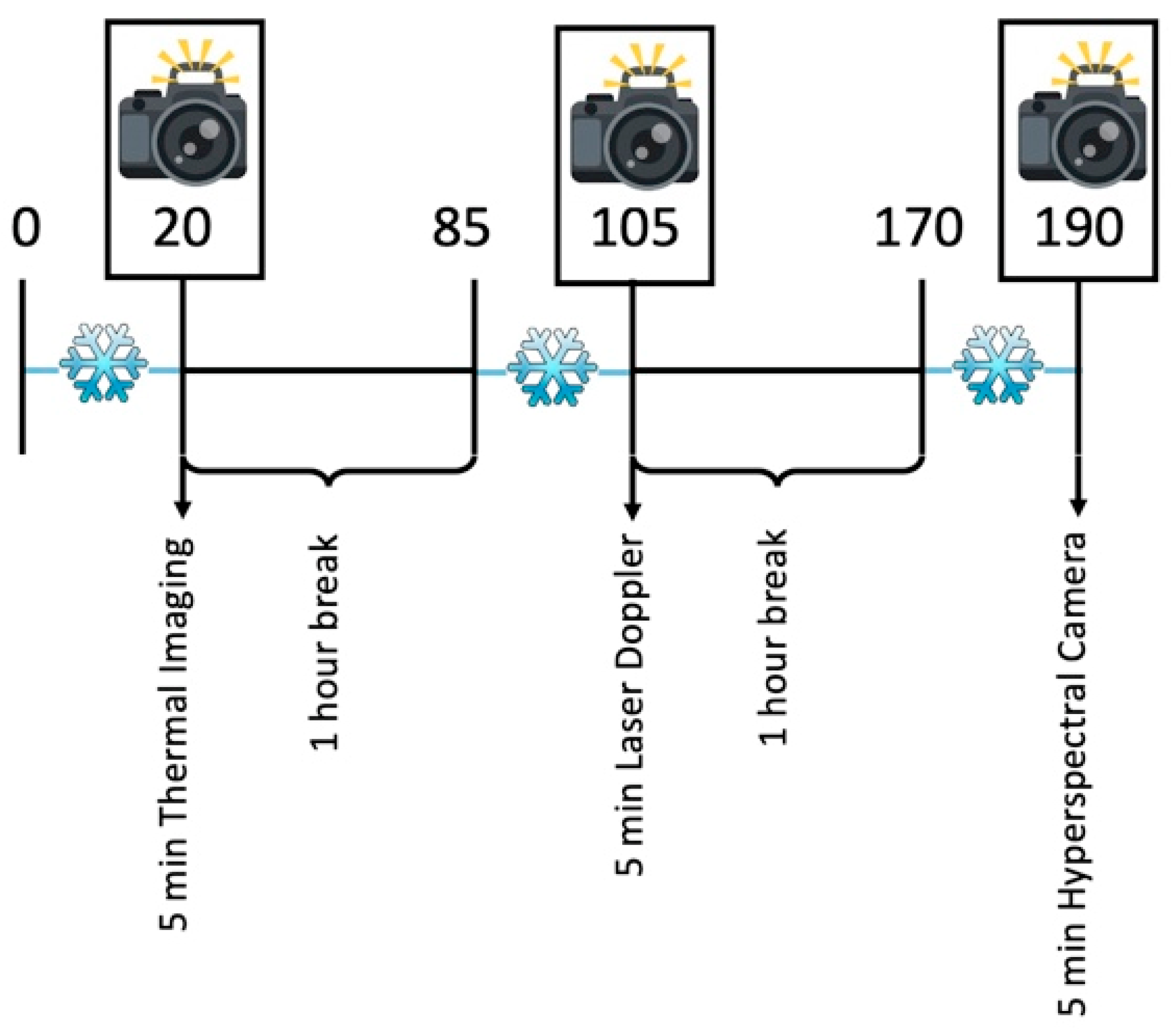
2.3. Study Course
2.4. Image Analysis
2.5. Statistical Analysis
3. Results
3.1. Perforator Detection
3.2. TI Detection
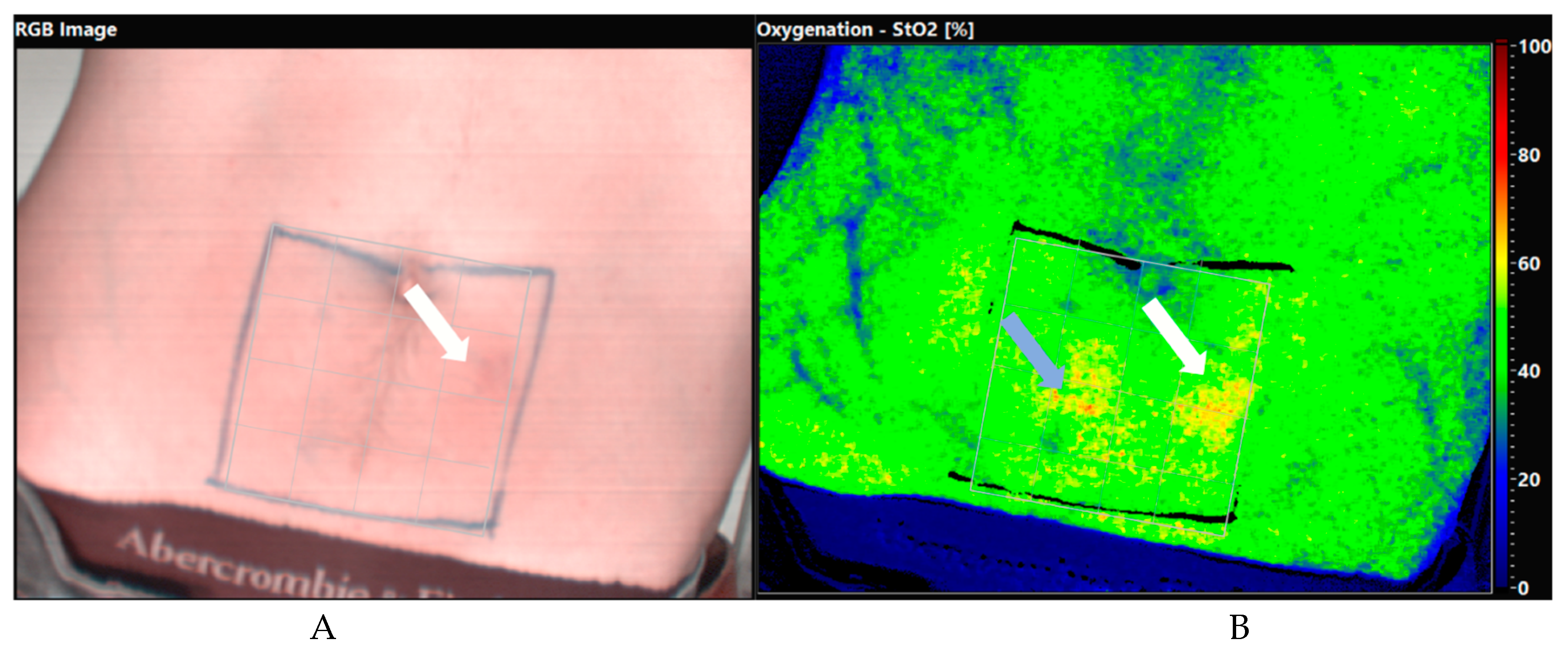
3.3. HS Detection
3.4. LD Detection
4. Discussion
Limitations & Outlook
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, B.T.; Agarwal, J.P.; Ascherman, J.A.; Caterson, S.A.; Gray, D.D.; Hollenbeck, S.T.; Khan, S.A.; Loeding, L.D.; Mahabir, R.C.; Miller, A.S.; et al. Evidence-Based Clinical Practice Guideline: Autologous Breast Reconstruction with DIEP or Pedicled TRAM Abdominal Flaps. Plast. Reconstr. Surg. 2017, 140, 651e–664e. [Google Scholar] [CrossRef]
- Renzulli, M.; Clemente, A.; Brocchi, S.; Gelati, C.; Zanotti, S.; Pizzi, C.; Tassone, D.; Cappabianca, S.; Cipriani, R.; Golfieri, R. Preoperative Computed Tomography Assessment for a Deep Inferior Epigastric Perforator (DIEP) Flap: A New Easy Technique from the Bologna Experience. Acta Radiol. 2020. [Google Scholar] [CrossRef]
- Chaput, B.; Meresse, T.; Bekara, F.; Grolleau, J.; Gangloff, D.; Gandolfi, S.; Herlin, C. Lower Limb Perforator Flaps: Current Concept. Ann. Chir. Plast. Esthet. 2020, 65, 496–516. [Google Scholar] [CrossRef] [PubMed]
- Cina, A.; Barone-Adesi, L.; Rinaldi, P.; Cipriani, A.; Salgarello, M.; Masetti, R.; Bonomo, L. Planning Deep Inferior Epigastric Perforator Flaps for Breast Reconstruction: A Comparison between Multidetector Computed Tomography and Magnetic Resonance Angiography. Eur. Radiol. 2013, 23, 2333–2343. [Google Scholar] [CrossRef] [PubMed]
- Wade, R.G.; Watford, J.; Wormald, J.C.R.; Bramhall, R.J.; Figus, A. Perforator Mapping Reduces the Operative Time of DIEP Flap Breast Reconstruction: A Systematic Review and Meta-Analysis of Preoperative Ultrasound, Computed Tomography and Magnetic Resonance Angiography. J. Plast. Reconstr. Aesthetic Surg. 2018, 71, 468–477. [Google Scholar] [CrossRef] [Green Version]
- D’angelo, A.; Cina, A.; Macrì, G.; Belli, P.; Mercogliano, S.; Barbieri, P.; Grippo, C.; Franceschini, G.; D’archi, S.; Mason, E.J.; et al. Conventional Ct versus Dedicated Ct Angiography in Diep Flap Planning: A Feasibility Study. J. Pers. Med. 2021, 11, 277. [Google Scholar] [CrossRef]
- Rozen, W.M.; Ashton, M.W.; Taylor, G.I. Reviewing the vascular supply of the anterior abdominal wall: Redefining anatomy for increasingly refined surgery. Clin. Anat. 2008, 21, 89–98. [Google Scholar] [CrossRef]
- Kiely, J.; Kumar, M.; Wade, R.G. The Accuracy of Different Modalities of Perforator Mapping for Unilateral DIEP Flap Breast Reconstruction: A Systematic Review and Meta-Analysis. J. Plast. Reconstr. Aesthetic Surg. 2021, 74, 945–956. [Google Scholar] [CrossRef]
- Pereira, N.; Valenzuela, D.; Mangelsdorff, G.; Kufeke, M.; Roa, R. Detection of Perforators for Free Flap Planning Using Smartphone Thermal Imaging: A Concordance Study with Computed Tomographic Angiography in 120 Perforators. Plast. Reconstr. Surg. 2018, 141, 787–792. [Google Scholar] [CrossRef]
- Kagen, A.C.; Hossain, R.; Dayan, E.; Maddula, S.; Samson, W.; Dayan, J.; Smith, M.L. Modern Perforator Flap Imaging with High-Resolution Blood Pool MR Angiography. Radiographics 2015, 35, 901–915. [Google Scholar] [CrossRef] [Green Version]
- Schmauss, D.; Beier, J.P.; Eisenhardt, S.U.; Horch, R.E.; Momeni, A.; Rab, M.; Rieck, B.; Rieger, U.; Schaefer, D.J.; Schmidt, V.J.; et al. The „safe“ Flap—Preoperative Perforator-Mapping and Intraoperative Perfusion Assessment to Reduce Flap-Associated Morbidity Statement of the German Speaking Working Group for Microsurgery of the Peripheral Nerves and Vessels. Handchir. Mikrochir. Plast. Chir. 2019, 51, 410–417. [Google Scholar] [CrossRef]
- Chubb, D.; Rozen, W.M.; Whitaker, I.S.; Ashton, M.W. Images in Plastic Surgery: Digital Thermographic Photography (“thermal Imaging”) for Preoperative Perforator Mapping. Ann. Plast. Surg. 2011, 66, 324–325. [Google Scholar] [CrossRef]
- Daigeler, A.; Schubert, C.; Hirsch, T.; Behr, B.; Lehnhardt, M. Colour Duplex Sonography and “Power-Duplex” in Perforator Surgery—Improvement of Patients Safety by Efficient Planning. Handchir. Mikrochir. Plast. Chir. 2018, 50, 101–110. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.; Ohi, H.; Ogawa, R. Propeller Flaps: Imaging in Propeller Flap Surgery. Semin. Plast. Surg. 2020, 34, 145. [Google Scholar] [CrossRef] [PubMed]
- Khan, U.D.; Miller, J.G. Reliability of Handheld Doppler in Planning Local Perforator–Based Flaps for Extremities. Aesthetic Plast. Surg. 2007, 31, 521–525. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.; Doyle, M.; McCarten, G. The Doppler Probe for Planning Flaps: Anatomical Study and Clinical Applications. Br. J. Plast. Surg. 1990, 43, 1–16. [Google Scholar] [CrossRef]
- Stekelenburg, C.M.; Sonneveld, P.M.D.G.; Bouman, M.B.; van der Wal, M.B.A.; Knol, D.L.; de Vet, H.C.W.; van Zuijlen, P.P.M. The Hand Held Doppler Device for the Detection of Perforators in Reconstructive Surgery: What You Hear Is Not Always What You Get. Burns 2014, 40, 1702–1706. [Google Scholar] [CrossRef]
- Ono, S.; Hayashi, H.; Ohi, H.; Ogawa, R. Imaging Studies for Preoperative Planning of Perforator Flaps: An Overview. Clin. Plast. Surg. 2017, 44, 21–30. [Google Scholar] [CrossRef]
- Unger, M.; Markfort, M.; Halama, D.; Chalopin, C. Automatic Detection of Perforator Vessels Using Infrared Thermography in Reconstructive Surgery. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 501–507. [Google Scholar] [CrossRef]
- Goetze, E.; Thiem, D.G.E.; Gielisch, M.W.; Kämmerer, P.W. Identification of Cutaneous Perforators for Microvascular Surgery Using Hyperspectral Technique—A Feasibility Study on the Antero-Lateral Thigh. J. Cranio-Maxillofac. Surg. 2020, 48, 1066–1073. [Google Scholar] [CrossRef]
- Chaput, B.; Bertheuil, N.; Gandolfi, S.; Grolleau, J.L.; Herlin, C. Perforator Detection with a Hand-Held Doppler Device: Importance of the Learning Curve. Burns 2015, 41, 197. [Google Scholar] [CrossRef]
- Sheena, Y.; Jennison, T.; Hardwicke, J.T.; Titley, O.G. Detection of Perforators Using Thermal Imaging. Plast. Reconstr. Surg. 2013, 132, 1603–1610. [Google Scholar] [CrossRef] [PubMed]
- Tenorio, X.; Mahajan, A.L.; Elias, B.; van Riempst, J.S.; Wettstein, R.; Harder, Y.; Pittet, B. Locating Perforator Vessels by Dynamic Infrared Imaging and Flow Doppler with No Thermal Cold Challenge. Ann. Plast. Surg. 2011, 67, 143–146. [Google Scholar] [CrossRef] [PubMed]
- Holmer, A.; Tetschke, F.; Marotz, J.; Malberg, H.; Markgraf, W.; Thiele, C.; Kulcke, A. Oxygenation and Perfusion Monitoring with a Hyperspectral Camera System for Chemical Based Tissue Analysis of Skin and Organs. Physiol. Meas. 2016, 37, 2064–2078. [Google Scholar] [CrossRef] [PubMed]
- Xiao, W.; Li, K.; Kiu-Huen Ng, S.; Feng, S.; Zhou, H.; Nicoli, F.; Blondeel, P.; Zhang, Y. A Prospective Comparative Study of Color Doppler Ultrasound and Infrared Thermography in the Detection of Perforators for Anterolateral Thigh Flaps. Ann. Plast. Surg. 2020, 84, S190–S195. [Google Scholar] [CrossRef] [PubMed]
- Holmer, A.; Marotz, J.; Wahl, P.; Dau, M.; Kämmerer, P.W. Hyperspectral Imaging in Perfusion and Wound Diagnostics-Methods and Algorithms for the Determination of Tissue Parameters. Biomed. Tech. 2018, 63, 587–594. [Google Scholar] [CrossRef] [PubMed]
- Thiem, D.G.E.; Frick, R.W.; Goetze, E.; Gielisch, M.; Al-Nawas, B.; Kämmerer, P.W. Hyperspectral Analysis for Perioperative Perfusion Monitoring—A Clinical Feasibility Study on Free and Pedicled Flaps. Clin. Oral Investig. 2021, 25, 933–945. [Google Scholar] [CrossRef]
- Shin, J.Y.; Yi, H.S. Diagnostic Accuracy of Laser Doppler Imaging in Burn Depth Assessment: Systematic Review and Meta-Analysis. Burn. J. Int. Soc. Burn. Inj. 2016, 42, 1369–1376. [Google Scholar] [CrossRef]
- Tindholdt, T.; Saidian, S.; Tønseth, K. Microcirculatory Evaluation of Deep Inferior Epigastric Artery Perforator Flaps with Laser Doppler Perfusion Imaging in Breast Reconstruction. J. Plast. Surg. hand Surg. 2011, 45, 143–147. [Google Scholar] [CrossRef]
- FLIR ONE. Pro Thermal Imaging Camera for Smartphones | Teledyne FLIR. Available online: https://www.flir.eu/products/flir-one-pro/ (accessed on 4 July 2021).
- TIVITA®. Wound—Diaspective Vision. Available online: https://diaspective-vision.com/en/produkt/tivita-wound/ (accessed on 24 September 2021).
- Oberg, P. Laser-Doppler Flowmetry. Crit. Rev. Biomed. Eng. 1990, 18, 125–163. [Google Scholar]
- Hallock, G. Acoustic Doppler Sonography, Color Duplex Ultrasound, and Laser Doppler Flowmetry as Tools for Successful Autologous Breast Reconstruction. Clin. Plast. Surg. 2011, 38, 203–211. [Google Scholar] [CrossRef] [PubMed]
- Laser Doppler Line Scanning—MoorLDLS-BI—Moor Instruments. Available online: https://www.moorclinical.com/products/imaging/line-imaging/ (accessed on 24 September 2021).
- Öztuna, D.; Elhan, A.H.; Tüccar, E. Investigation of Four Different Normality Tests in Terms of Type 1 Error Rate and Power under Different Distributions. Turk. J. Med. Sci. 2006, 36, 171–176. [Google Scholar]
- Rabbani, M.; Ilyas, A.; Rabbani, A.; Abidin, Z.; Tarar, M. Accuracy of Thermal Imaging Camera in Identification of Perforators. J. Coll. Physicians Surg. Pak. JCPSP 2020, 30, 512–515. [Google Scholar] [CrossRef] [PubMed]
- Weum, S.; Lott, A.; de Weerd, L. Detection of Perforators Using Smartphone Thermal Imaging. Plast. Reconstr. Surg. 2016, 138, 938e–940e. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muntean, M.V.; Achimas-Cadariu, P.A. Detection of Perforators for Free Flap Planning Using Smartphone Thermal Imaging: A Concordance Study with Computed Tomographic Angiography in 120 Perforators. Plast. Reconstr. Surg. 2018, 142, 604E. [Google Scholar] [CrossRef] [PubMed]
- De Weerd, L.; Weum, S.; Mercer, J.B. The Value of Dynamic Infrared Thermography (DIRT) in Perforator Selection and Planning of Free DIEP Flaps. Ann. Plast. Surg. 2009, 63, 274–279. [Google Scholar] [CrossRef] [PubMed]
- De Weerd, L.; Weum, S.; Mercer, J.B. Locating Perforator Vessels by Dynamic Infrared Imaging and Flow Doppler with No Thermal Cold Challenge. Ann. Plast. Surg. 2014, 72, 261. [Google Scholar] [CrossRef] [PubMed]
- Xue, E.Y.; Chandler, L.K.; Viviano, S.L.; Keith, J.D. Use of FLIR ONE Smartphone Thermography in Burn Wound Assessment. Ann. Plast. Surg. 2018, 80, S236–S238. [Google Scholar] [CrossRef] [PubMed]
- Jaspers, M.E.H.; Carrière, M.E.; Meij-de Vries, A.; Klaessens, J.H.G.M.; van Zuijlen, P.P.M. The FLIR ONE Thermal Imager for the Assessment of Burn Wounds: Reliability and Validity Study. Burns 2017, 43, 1516–1523. [Google Scholar] [CrossRef]
- Ganon, S.; Guédon, A.; Cassier, S.; Atlan, M. Contribution of Thermal Imaging in Determining the Depth of Pediatric Acute Burns. Burns 2020, 46, 1091–1099. [Google Scholar] [CrossRef]
- Romanò, C.L.; Logoluso, N.; Dell’Oro, F.; Elia, A.; Drago, L. Telethermographic Findings after Uncomplicated and Septic Total Knee Replacement. The Knee 2012, 19, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Just, M.; Chalopin, C.; Unger, M.; Halama, D.; Neumuth, T.; Dietz, A.; Fischer, M. Monitoring of Microvascular Free Flaps Following Oropharyngeal Reconstruction Using Infrared Thermography: First Clinical Experiences. Eur. Arch. Oto-Rhino-Laryngol. 2015, 273, 2659–2667. [Google Scholar] [CrossRef] [PubMed]
- Verstockt, J.; Thiessen, F.; Cloostermans, B.; Tjalma, W.; Steenackers, G. DIEP Flap Breast Reconstructions: Thermographic Assistance as a Possibility for Perforator Mapping and Improvement of DIEP Flap Quality. Appl. Opt. 2020, 59, E48. [Google Scholar] [CrossRef]
- Nischwitz, S.P.; Luze, H.; Kamolz, L.P. Thermal Imaging via FLIR One—A Promising Tool in Clinical Burn Care and Research. Burns 2020, 46, 988–989. [Google Scholar] [CrossRef] [PubMed]
- Heimes, D.; Becker, P.; Thiem, D.; Kuchen, R.; Kyyak, S.; Kämmerer, P. Is Hyperspectral Imaging Suitable for Assessing Collateral Circulation Prior Radial Forearm Free Flap Harvesting? Comparison of Hyperspectral Imaging and Conventional Allen’s Test. J. Pers. Med. 2021, 11, 531. [Google Scholar] [CrossRef]
- Schulz, T.; Marotz, J.; Stukenberg, A.; Reumuth, G.; Houschyar, K.; Siemers, F. Hyperspectral Imaging for Postoperative Flap Monitoring of Pedicled Flaps. Handchir. Mikrochir. Plast. Chir. Organ Dtsch. Arb. Handchir. Organ Dtsch. Arb. Mikrochir. Peripher. Nerven Gefasse Organ V 2020, 52, 316–324. [Google Scholar] [CrossRef]
- Kohler, L.H.; Köhler, H.; Kohler, S.; Langer, S.; Nuwayhid, R.; Gockel, I.; Spindler, N.; Osterhoff, G. Hyperspectral Imaging (HSI) as a New Diagnostic Tool in Free Flap Monitoring for Soft Tissue Reconstruction: A Proof of Concept Study. BMC Surgery 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Smit, J.M.; Zeebregts, C.J.; Acosta, R.; Werker, P.M.N. Advancements in Free Flap Monitoring in the Last Decade: A Critical Review. Plast. Reconstr. Surg. 2010, 125, 177–185. [Google Scholar] [CrossRef]
- Tindholdt, T.T.; Saidian, S.; Pripp, A.H.; Tønseth, K.A. Monitoring Microcirculatory Changes in the Deep Inferior Epigastric Artery Perforator Flap with Laser Doppler Perfusion Imaging. Ann. Plast. Surg. 2011, 67, 139–142. [Google Scholar] [CrossRef]
- Van den Heuvel, M.G.W.; Mermans, J.F.; Ambergen, A.W.; van der Hulst, R.R.W.J. Perfusion of the Deep Inferior Epigastric Perforator Flap Measured by Laser Doppler Imager. Ann. Plast. Surg. 2011, 66, 648–653. [Google Scholar] [CrossRef] [Green Version]
- Abdelrahman, M.; Jumabhoy, I.; Qiu, S.S.; Fufa, D.; Hsu, C.-C.; Lin, C.-H.; Lin, Y.-T.; Lin, C.-H. Perfusion Dynamics of the Medial Sural Artery Perforator (MSAP) Flap in Lower Extremity Reconstruction Using Laser Doppler Perfusion Imaging (LDPI): A Clinical Study. J. Plast. Surg. Hand Surg. 2019, 54, 112–119. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject ID | Sex | Age [years] | BMI [kg/m2] | Abdominal Girth [cm] | Perforator Detection |
|---|---|---|---|---|---|
| 01 | Male | 36 | m.d. | m.d. | Left |
| 02 | Male | 30 | 22.86 | 78 | Right |
| 03 | Male | 58 | 29.30 | 111 | Right |
| 04 | Male | 41 | 32.53 | 108 | Left |
| 05 | Male | 65 | m.d. | m.d. | Left |
| 06 | Female | 71 | 27.89 | 92 | Left + Right |
| 07 | Female | 28 | 23.88 | 82 | Left + Right |
| 08 | Female | 22 | 19.13 | 68 | Left |
| 09 | Female | 52 | 23.44 | 70 | Left + Right |
| 10 | Male | 41 | 31.56 | 102 | Left |
| 11 | Male | 61 | 22.21 | 92 | Left + Right |
| 12 | Male | 62 | 23.66 | 93 | Left |
| 13 | Male | 24 | 25.98 | 92 | Left |
| 14 | Female | 24 | 20.44 | 70 | Left |
| 15 | Male | 49 | 32.77 | 132 | Right |
| 16 | Female | 45 | 34.72 | 110 | Left |
| 17 | Male | 60 | 26.47 | 100 | Left + Right |
| 18 | Male | 60 | 25.08 | 98 | Left + Right |
| Total/median (25th, 75th percentile) | 66.6% Male 33.3% Female | 47.00 (29.50, 60.25) | 25.53 (23.01, 31.00) | 92.50 (79.00, 106.50) | 9 Left, 3 Right 6 Left + Right |
| Subject ID | TI | HS | LD |
|---|---|---|---|
| 01 | 6 | 0 | 0 |
| 02 | 6 | 0 | 0 |
| 03 | 6 | 3/6 | 0 |
| 04 | 6 | 2/6 | 0 |
| 05 | 6 | 3/6 | 0 |
| 06 | 4/6 | 0 | 0 |
| 07 | 6 | 0 | 0 |
| 08 | 6 | 0 | 0 |
| 09 | 6 | 0 | 0 |
| 10 | 0 | 0 | 0 |
| 11 | 6 | 0 | 0 |
| 12 | 6 | 6 | 0 |
| 13 | 6 | 2/6 | 0 |
| 14 | 6 | 0 | 0 |
| 15 | 6 | 0 | 0 |
| 16 | 6 | 6 | 0 |
| 17 | 6 | 0 | 0 |
| 18 | 6 | 6 | 0 |
| Total | 100/108 | 28/108 | 0/108 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nischwitz, S.P.; Luze, H.; Schellnegger, M.; Gatterer, S.J.; Tuca, A.-C.; Winter, R.; Kamolz, L.-P. Thermal, Hyperspectral, and Laser Doppler Imaging: Non-Invasive Tools for Detection of The Deep Inferior Epigastric Artery Perforators—A Prospective Comparison Study. J. Pers. Med. 2021, 11, 1005. https://doi.org/10.3390/jpm11101005
Nischwitz SP, Luze H, Schellnegger M, Gatterer SJ, Tuca A-C, Winter R, Kamolz L-P. Thermal, Hyperspectral, and Laser Doppler Imaging: Non-Invasive Tools for Detection of The Deep Inferior Epigastric Artery Perforators—A Prospective Comparison Study. Journal of Personalized Medicine. 2021; 11(10):1005. https://doi.org/10.3390/jpm11101005
Chicago/Turabian StyleNischwitz, Sebastian P., Hanna Luze, Marlies Schellnegger, Simon J. Gatterer, Alexandru-Cristian Tuca, Raimund Winter, and Lars-Peter Kamolz. 2021. "Thermal, Hyperspectral, and Laser Doppler Imaging: Non-Invasive Tools for Detection of The Deep Inferior Epigastric Artery Perforators—A Prospective Comparison Study" Journal of Personalized Medicine 11, no. 10: 1005. https://doi.org/10.3390/jpm11101005
APA StyleNischwitz, S. P., Luze, H., Schellnegger, M., Gatterer, S. J., Tuca, A.-C., Winter, R., & Kamolz, L.-P. (2021). Thermal, Hyperspectral, and Laser Doppler Imaging: Non-Invasive Tools for Detection of The Deep Inferior Epigastric Artery Perforators—A Prospective Comparison Study. Journal of Personalized Medicine, 11(10), 1005. https://doi.org/10.3390/jpm11101005