
Escalation Time to Open Triple Combination Therapy from the Initiation of LAMA versus ICS/LABA in COPD Management: Findings from Comparing the Incidence of Tiotropium and ICS/LABA in Real-World Use in South Korea (CITRUS) Study

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
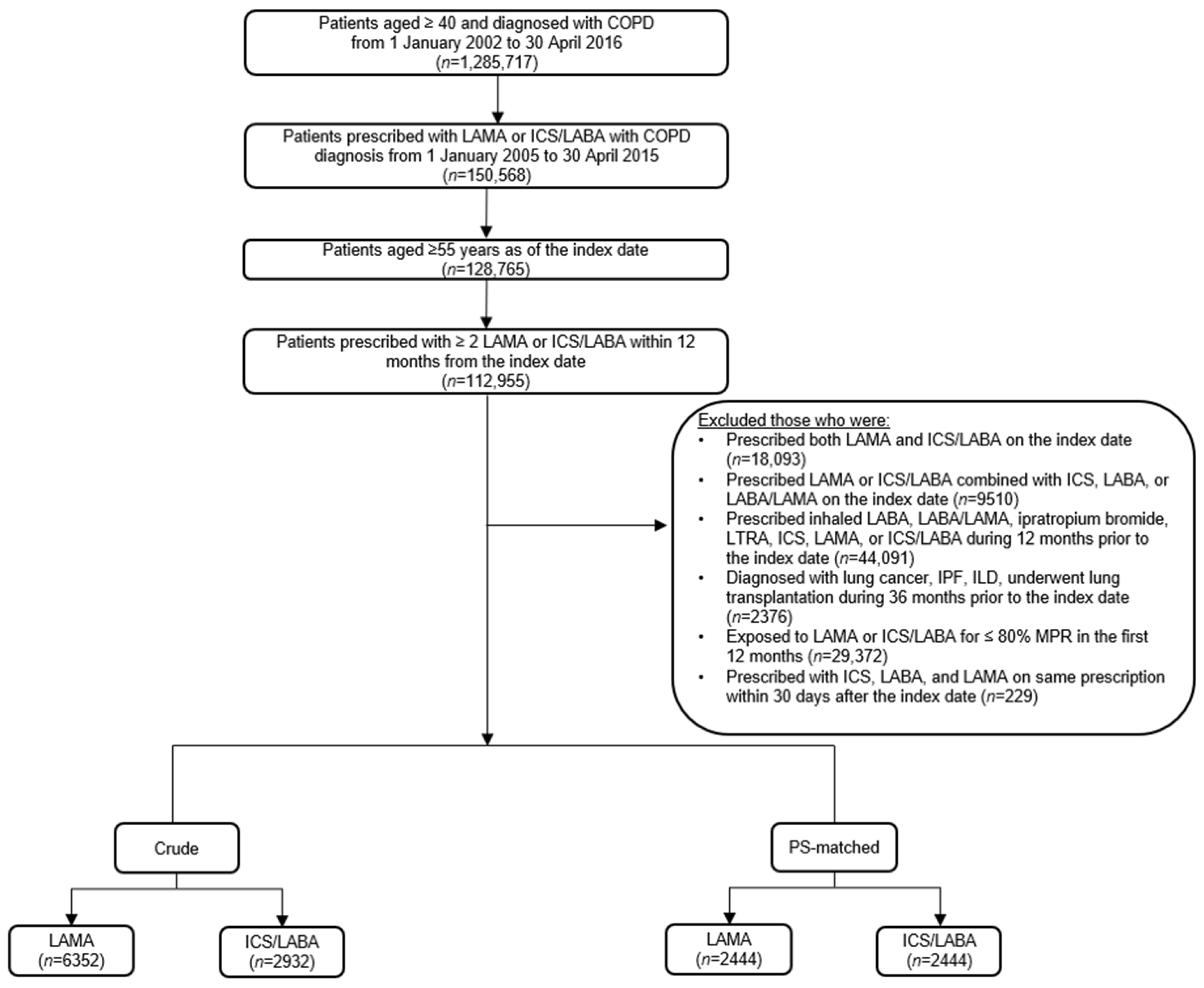
2.1. Study Design and Population
2.2. Covariates
2.3. Outcomes
2.4. Statistical Analysis
2.5. Ethics Approval
3. Results
3.1. Baseline Characteristics
3.2. Time to Triple Combination Therapy
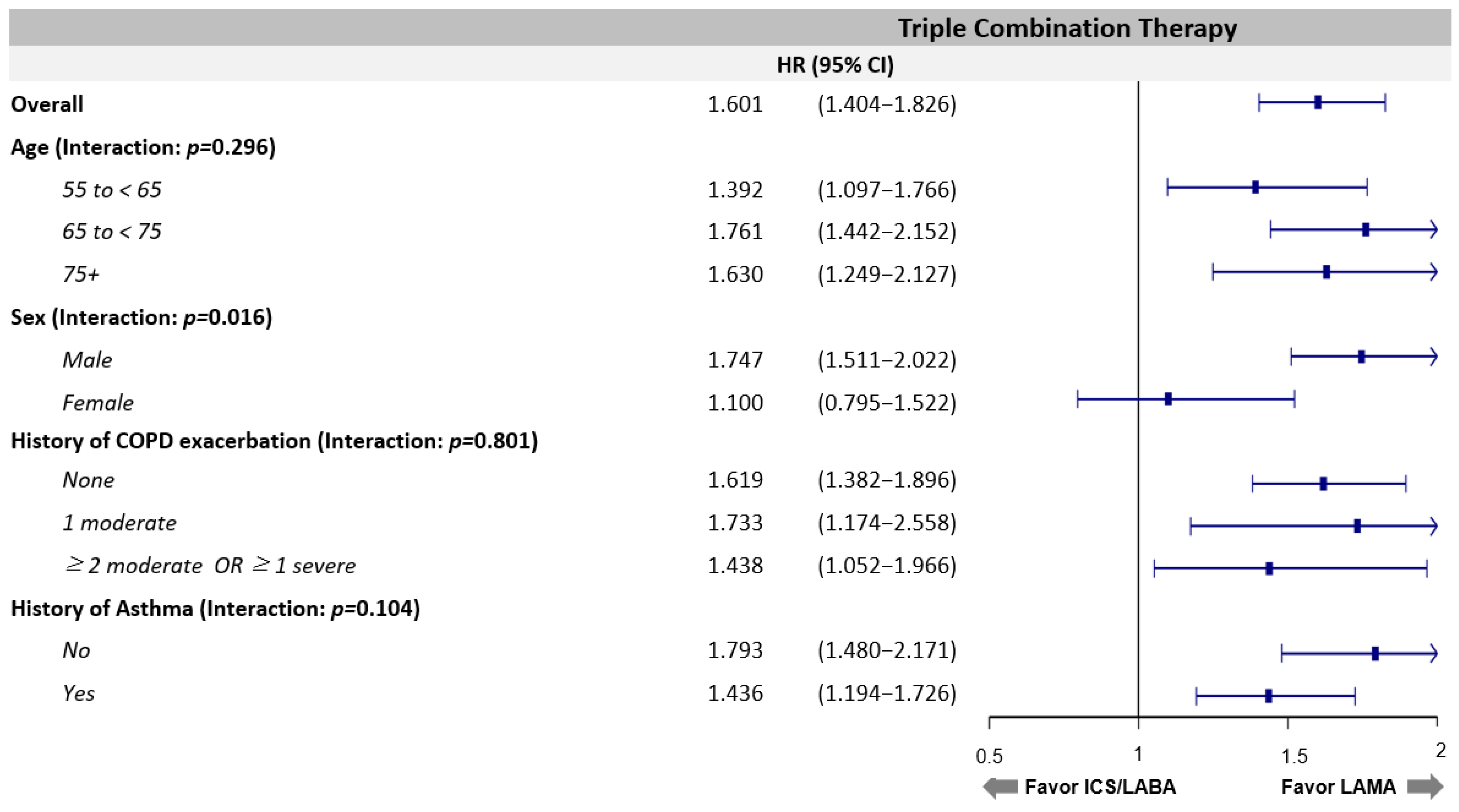
3.3. Risk Factors of Triple Combination Therapy
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Global Initiative for Chronic Obstructive Lung Disease. Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease. 2020 Report. Available online: https://goldcopd.org/wp-content/uploads/2019/12/GOLD-2020-FINAL-ver1.2-03Dec19_WMV.pdf (accessed on 1 July 2021).
- Koarai, A.; Sugiura, H.; Yamada, M.; Ichikawa, T.; Fujino, N.; Kawayama, T.; Ichinose, M. Treatment with LABA versus LAMA for stable COPD: A systematic review and meta-analysis. BMC Pulm. Med. 2020, 20, 111. [Google Scholar] [CrossRef] [PubMed]
- Tavakoli, H.; Johnson, K.M.; FitzGerald, J.M.; Sin, D.D.; Gershon, A.S.; Kendzerska, T.; Sadatsafavi, M. Trends in prescriptions and costs of inhaled medications in chronic obstructive pulmonary disease: A 19-year population-based study from Canada. Int. J. Chron. Obstruct. Pulm. Dis. 2019, 14, 2003–2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dransfield, M.T.; Bourbeau, J.; Jones, P.W.; Hanania, N.A.; Mahler, D.A.; Vestbo, J.; Calverley, P.M. Once-daily inhaled fluticasone furoate and vilanterol versus vilanterol only for prevention of exacerbations of COPD: Two replicate double-blind, parallel-group, randomised controlled trials. Lancet Respir. Med. 2013, 1, 210–223. [Google Scholar] [CrossRef]
- Vestbo, J.; Anderson, J.A.; Brook, R.D.; Calverley, P.M.; Celli, B.R.; Crim, C.; Martinez, F.; Yates, J.; Newby, D.E.; Summit Investigators. Fluticasone furoate and vilanterol and survival in chronic obstructive pulmonary disease with heightened cardiovascular risk (SUMMIT): A double-blind randomised controlled trial. Lancet 2016, 387, 1817–1826. [Google Scholar] [CrossRef]
- Papi, A.; Vestbo, J.; Fabbri, L.; Corradi, M.; Prunier, H.; Cohuet, G.; Guasconi, A.; Montagna, I.; Vezzoli, S.; Petruzzelli, S.; et al. Extrafine inhaled triple therapy versus dual bronchodilator therapy in chronic obstructive pulmonary disease (Tribute): A double-blind, parallel group, randomised controlled trial. Lancet 2018, 391, 1076–1084. [Google Scholar] [CrossRef]
- Lipson, D.A.; Barnhart, F.; Brealey, N.; Brooks, J.; Criner, G.J.; Day, N.C.; Dransfield, M.T.; Halpin, D.M.; Han, M.K.; Jones, C.E.; et al. Once-daily single-inhaler triple versus dual therapy in patients with COPD. N. Engl. J. Med. 2018, 378, 1671–1680. [Google Scholar] [CrossRef]
- Agusti, A.; Fabbri, L.M.; Singh, D.; Vestbo, J.; Celli, B.; Franssen, F.M.; Rabe, K.F.; Papi, A. Inhaled corticosteroids in COPD: Friend or foe? Eur. Respir. J. 2018, 52, 1801219. [Google Scholar] [CrossRef]
- Vestbo, J.; Papi, A.; Corradi, M.; Blazhko, V.; Montagna, I.; Francisco, C.; Cohuet, G.; Vezzoli, S.; Scuri, M.; Singh, D. Single inhaler extrafine triple therapy versus long-acting muscarinic antagonist therapy for chronic obstructive pulmonary disease (Trinity): A double-blind, parallel group, randomised controlled trial. Lancet 2017, 389, 1919–1929. [Google Scholar] [CrossRef] [Green Version]
- Miyazaki, M.; Nakamura, H.; Takahashi, S.; Chubachi, S.; Sasaki, M.; Haraguchi, M.; Terai, H.; Ishii, M.; Fukunaga, K.; Tasaka, S.; et al. The reasons for triple therapy in stable COPD patients in Japanese clinical practice. Int. J. Chron. Obstruct. Pulmon. Dis. 2015, 4, 1053–1059. [Google Scholar]
- Lane, D.C.; Stemkowski, S.; Stanford, R.H.; Tao, Z. Initiation of triple therapy with multiple inhalers in chronic obstructive pulmonary disease: An analysis of treatment patterns from a US retrospective database study. J. Manag. Care Spec. Pharm. 2018, 24, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Celli, B.R.; Wedzicha, J.A. Update on clinical aspects of chronic obstructive pulmonary disease. N. Engl. J. Med. 2019, 381, 1257–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, W.C.; Wu, B.R.; Liao, W.C.; Chen, C.Y.; Chen, W.C.; Hsia, T.C.; Tu, C.Y.; Chen, C.H.; Hsu, W.H. When to Use Initial Triple Therapy in COPD: Adding a LAMA to ICS/LABA by Clinically Important Deterioration Assessment. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 3375–3384. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.R.; Wu, B.; Kern, D.M.; Tunceli, O.; Fox, K.M.; Horton, J.; Legg, R.F.; Trudo, F. Impact of nonadherence to inhaled corticosteroid/LABA therapy on COPD exacerbation rates and healthcare costs in a commercially insured US population. Am. Health Drug Benefits 2017, 10, 92–102. [Google Scholar] [PubMed]
- Khakban, A.; Sin, D.D.; FitzGerald, J.M.; Ng, R.; Zafarí, Z.; McManus, B.; Hollander, Z.; Marra, C.A.; Sadatsafavi, M. Ten-year trends in direct costs of COPD: A population-based study. Chest 2015, 148, 640–646. [Google Scholar] [CrossRef]
- Pasquale, M.K.; Sun, S.X.; Song, F.; Hartnett, H.J.; Stemkowski, S.A. Impact of exacerbations on health care cost and resource utilization in chronic obstructive pulmonary disease patients with chronic bronchitis from a predominantly Medicare population. Int. J. Chron. Obstruct. Pulmon. Dis. 2012, 7, 757–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalon, F.; Roche, N.; Belhassen, M.; Nolin, M.; Pegliasco, H.; Deslée, G.; Housset, B.; Devillier, P.; Van Ganse, E. Dual versus triple therapy in patients hospitalized for COPD in France: A claims data study. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 1839–1854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ritondo, B.L.; Puxeddu, E.; Calzetta, L.; Cazzola, M.; Rogliani, P. Efficacy and safety of triple combination therapy for treating chronic obstructive pulmonary disease: An expert review. Expert Opin. Pharmacother. 2021, 22, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Wedzicha, J.A.; Banerji, D.; Chapman, K.R.; Vestbo, J.; Roche, N.; Ayers, R.T.; Thach, C.; Fogel, R.; Patalano, F.; Vogelmeier, C.F. Indacaterol–Glycopyrronium versus salmeterol–fluticasone for COPD. N. Engl. J. Med. 2016, 374, 2222–2234. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogelmeier, C.; Paggiaro, P.L.; Dorca, J.; Sliwinski, P.; Mallet, M.; Kirsten, A.M.; Beier, J.; Seoane, B.; Segarra, R.M.; Leselbaum, A. Efficacy and safety of aclidinium/formoterol versus salmeterol/fluticasone: A phase 3 COPD study. Eur. Respir. J. 2016, 48, 1030–1039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skolnik, N.S.; Nguyen, T.S.; Shrestha, A.; Ray, R.; Corbridge, T.C.; Brunton, S.A. Current evidence for COPD management with dual long-acting muscarinic antagonist/long-acting β2-agonist bronchodilators. Postgrad. Med. 2020, 132, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Suissa, S.; Dell’Aniello, S.; Ernst, P. Comparative effectiveness of LABA ICS versus LAMA as initial treatment in COPD targeted by blood eosinophils: A population-based cohort study. Lancet Respir. Med. 2018, 6, 855–862. [Google Scholar] [CrossRef]
- Cazzola, M.; Calzetta, L.; Rogliani, P.; Matera, M.G. Triple therapy versus dual bronchodilation and inhaled corticosteroids/long-acting β-agonists in COPD: Accumulating evidence from network meta-analyses. Pulm. Ther. 2019, 5, 117–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quint, J.K.; Montonen, J.; Esposito, D.B.; He, X.; Koerner, L.; Wallace, L.; de la Hoz, A.; Miravitlles, M. COPD maintenance therapy with tiotropium/olodaterol versus LABA/ICS: An assessment of the risk of treatment escalation and adverse outcomes in over 40,000 patients. Am. J. Respir. Crit. Care Med. 2020, 201, A5072. [Google Scholar]
- Di Marco, F.; Santus, P.; Terraneo, S.; Peruzzi, E.; Muscianisi, E.; Ripellino, C.; Pegoraro, V. Characteristics of newly diagnosed COPD patients treated with triple inhaled therapy by general practitioners: A real world Italian study. NPJ Prim. Care Respir. Med. 2017, 27, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müllerová, H.; Shukla, A.; Hawkins, A.; Quint, J. Risk factors for acute exacerbations of COPD in a primary care population: A retrospective observational cohort study. BMJ Open 2014, 4, e006171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Viniol, C.; Vogelmeier, C.F. Exacerbations of COPD. Eur. Respir. Rev. 2018, 27, 170103. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Lee, J.H.; Kim, J.A.; Rhee, C.K. Trend of cost and utilization of COPD medication in Korea. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 27–33. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Jung, H.M.; Kim, S.K.; Yoo, K.H.; Jung, K.S.; Lee, S.H.; Rhee, C.K. Factors associated with chronic obstructive pulmonary disease exacerbation, based on big data analysis. Sci. Rep. 2019, 9, 6679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhee, C.K.; Kim, K.; Yoon, H.K.; Kim, J.A.; Kim, S.H.; Lee, S.H.; Park, Y.B.; Jung, K.S.; Yoo, K.H.; Hwang, Y.I. Natural course of early COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2017, 12, 663–668. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | All (n = 4888) | LAMA (n = 2444) | ICS/LABA (n = 2444) | p Value |
|---|---|---|---|---|
| Observational period, days | 733.92 ± 634.14 | 801.46 ± 698.29 | 666.39 ± 554.84 | <0.001 |
| Age, years | 69.7 ± 7.9 | 69.6 ± 7.9 | 69.7 ± 7.9 | 0.53 |
| 55 to <65 | 1396 (29) | 697 (29) | 699 (29) | |
| 65 to <75 | 2106 (43) | 1068 (44) | 1038 (42) | |
| 75+ | 1386 (28) | 679 (28) | 707 (29) | |
| Sex, male | 3676 (75) | 1854 (76) | 1822 (75) | 0.29 |
| Income level | ||||
| 1st quartile | 768 (16) | 376 (15) | 392 (16) | 0.77 |
| 2nd quartile | 634 (13) | 311 (13) | 323 (13) | |
| 3rd quartile | 935 (19) | 473 (19) | 462 (19) | |
| 4th quartile | 1641 (34) | 838 (34) | 803 (33) | |
| Medical aid | 910 (19) | 446 (18) | 464 (19) | |
| History of COPD exacerbation | ||||
| None | 3648(75) | 1831 (75) | 1817 (74) | 0.88 |
| 1 moderate | 485 (10) | 87 (7) | 247 (10) | |
| ≥2 moderate OR ≥ 1 severe | 755 (15) | 375 (15) | 380 (16) | |
| History of asthma | ||||
| No | 2530 (52) | 1263 (52) | 1267 (52) | 0.91 |
| Yes | 2358 (48) | 1181 (48) | 1177 (48) | |
| History of pneumonia | ||||
| No | 4377 (90) | 2179 (89) | 2198 (90) | 0.37 |
| Yes | 511 (10) | 265 (11) | 246 (10) | |
| mCCI | 2.0 ± 1.8 | 1.9 ± 1.8 | 2.0 ± 1.8 | 0.19 |
| Baseline Characteristics | All (n = 4888) | LAMA (n = 2444) | ICS/LABA (n = 2444) | p Value |
|---|---|---|---|---|
| Incidence rate per 1000 person-years | 106.8 | 81.0 | 139.8 | <0.001 |
| Patients with event | 901 | 383 | 518 | 0.09 |
| Median time to event | 227 | 281 | 207 | 0.03 |
| Age (years) | <0.001 | |||
| 55 to <65 | 435.3 ± 501.6 | 460.0 ± 558.9 | 415.0 ± 449.9 | |
| 65 to <75 | 397.96 ± 461.1 | 479.63 ± 532.2 | 338.8 ± 392.6 | |
| 75+ | 349.41 ± 406.8 | 382.67 ± 381.8 | 327.1 ± 422.7 | |
| Sex | ||||
| Male | 406.0 ± 464.1 | 473.9 ± 514.8 | 358.2 ± 418.9 | <0.001 |
| Female | 353.4 ± 450.0 | 349.1 ± 482.4 | 357.6 ± 420.3 | 0.001 |
| History of COPD exacerbation | ||||
| None | 395.9 ± 458.2 | 444.7 ± 503.6 | 360.0 ± 418.9 | <0.001 |
| 1 moderate | 416.3 ± 502.4 | 513.7 ± 566.9 | 347.61 ± 443.5 | <0.0001 |
| ≥ 2 moderate OR ≥ 1 severe | 391.0 ± 452.1 | 433.9 ± 505.9 | 357.6 ± 405.1 | 0.005 |
| History of asthma | ||||
| No | 395.6 ± 457.4 | 461.6 ± 497.9 | 351.7 ± 423.6 | <0.001 |
| Yes | 399.1 ± 466.8 | 441.0 ± 522.0 | 364.8 ± 414.3 | <0.001 |
| Variables | Univariate HR | Multivariate HR | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | p Value | aHR | 95% CI | p Value | ||
| Index med | LAMA | ref. | - | ref. | - | - | |
| ICS/LABA | 1.601 | 1.402–1.829 | <0.001 | 1.632 | 1.428–1.864 | <0.001 | |
| Age (years) | 55 to <65 | ref. | - | ref. | - | - | |
| 65 to <75 | 0.950 | 0.815–1.107 | 0.511 | 1.046 | 0.814–1.344 | 0.725 | |
| 75+ | 0.824 | 0.691–0.983 | 0.031 | 1.024 | 0.656–1.597 | 0.918 | |
| Sex | Female | ref. | - | ref. | - | - | |
| Male | 1.670 | 1.400–1.992 | <0.001 | 1.699 | 1.422–2.031 | <0.001 | |
| History of COPD exacerbation | None | ref. | - | - | ref. | - | - |
| 1 moderate | 1.225 | 0.996–1.507 | 0.055 | 1.213 | 0.983–1.497 | 0.072 | |
| ≥2 moderate OR ≥1 severe | 1.194 | 1.004–1.420 | 0.045 | 1.191 | 0.996–1.424 | 0.056 | |
| History of asthma | No | ref. | - | - | ref. | - | - |
| Yes | 1.133 | 0.994–1.291 | 0.061 | 1.146 | 0.998–1.317 | 0.053 | |
| History of pneumonia | No | ref. | - | - | - | - | - |
| Yes | 1.029 | 0.831–1.274 | 0.795 | - | - | - | |
| Congestive heart failure | No | ref | - | - | - | - | - |
| Yes | 1.002 | 0.811–1.238 | 0.988 | - | - | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.J.; Rhee, C.K.; Hwang, Y.I.; Yoo, K.H.; Lee, S.E.; Lee, D.; Park, Y.B.; Kim, Y. Escalation Time to Open Triple Combination Therapy from the Initiation of LAMA versus ICS/LABA in COPD Management: Findings from Comparing the Incidence of Tiotropium and ICS/LABA in Real-World Use in South Korea (CITRUS) Study. J. Pers. Med. 2021, 11, 1325. https://doi.org/10.3390/jpm11121325
Lee YJ, Rhee CK, Hwang YI, Yoo KH, Lee SE, Lee D, Park YB, Kim Y. Escalation Time to Open Triple Combination Therapy from the Initiation of LAMA versus ICS/LABA in COPD Management: Findings from Comparing the Incidence of Tiotropium and ICS/LABA in Real-World Use in South Korea (CITRUS) Study. Journal of Personalized Medicine. 2021; 11(12):1325. https://doi.org/10.3390/jpm11121325
Chicago/Turabian StyleLee, Ye Jin, Chin Kook Rhee, Yong Il Hwang, Kwang Ha Yoo, So Eun Lee, Doik Lee, Yong Bum Park, and Youlim Kim. 2021. "Escalation Time to Open Triple Combination Therapy from the Initiation of LAMA versus ICS/LABA in COPD Management: Findings from Comparing the Incidence of Tiotropium and ICS/LABA in Real-World Use in South Korea (CITRUS) Study" Journal of Personalized Medicine 11, no. 12: 1325. https://doi.org/10.3390/jpm11121325