
Statin Therapy and the Risk of COVID-19: A Cohort Study of the National Health Insurance Service in South Korea

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Statement
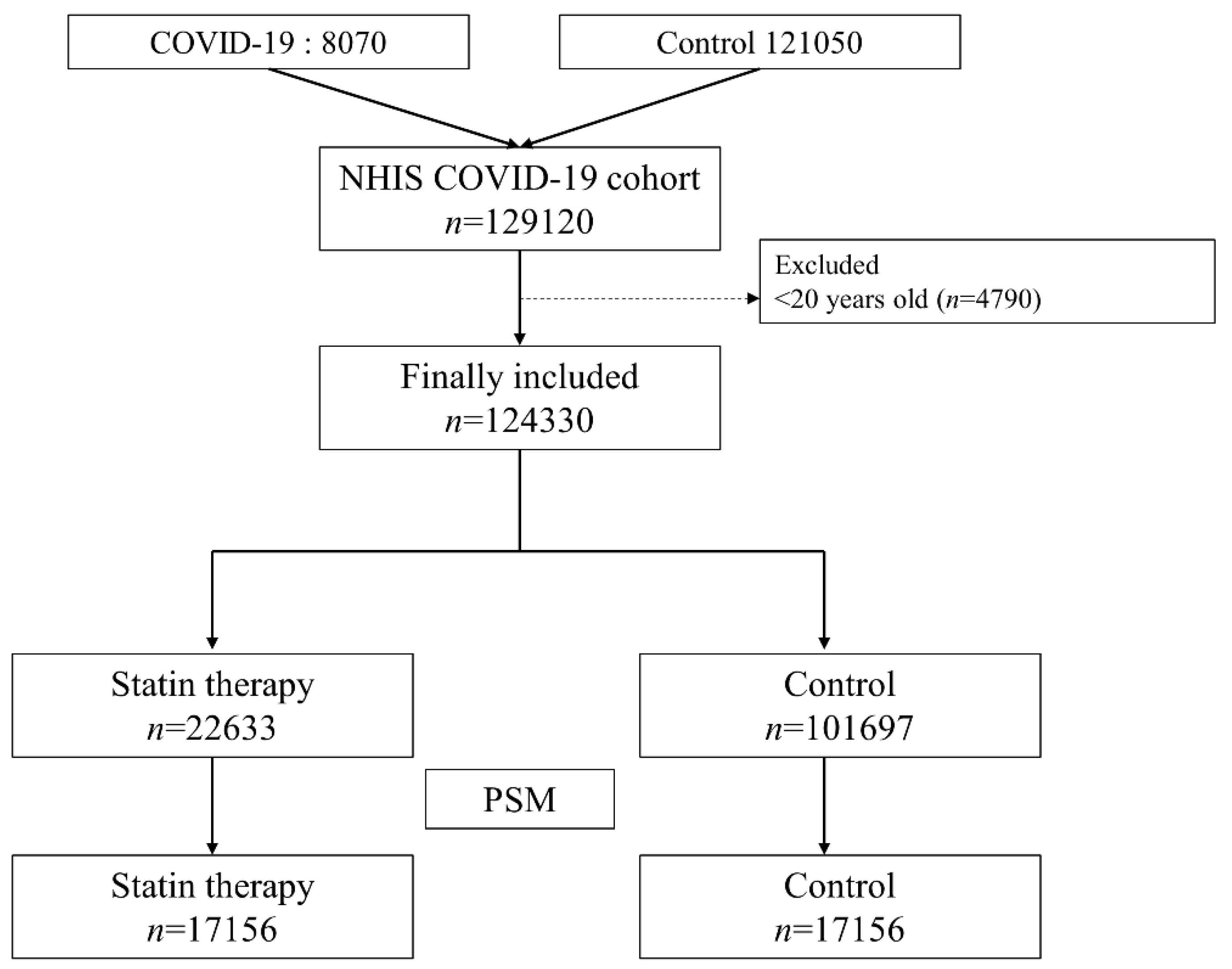
2.2. NHIS-COVID-19 Cohort Database and Study Population
2.3. Statin Users (Exposure Group)
2.4. Endpoints
2.5. Confounders
2.6. Statistical Analyses
3. Results
3.1. Study Population
3.2. Risk of COVID-19 in South Korea
3.3. Hospital Mortality among COVID-19 Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Eggmann, S.; Luder, G.; Verra, M.L.; Irincheeva, I.; Bastiaenen, C.H.G.; Jakob, S.M. Functional ability and quality of life in critical illness survivors with intensive care unit acquired weakness: A secondary analysis of a randomised controlled trial. PLoS ONE 2020, 15, e0229725. [Google Scholar] [CrossRef] [PubMed]
- Zhong, H.; Liu, X.B.; X, Z.Z. The epidemiological characteristics of an outbreak of 2019 novel coronavirus diseases (COVID-19) in China. Lancet 2020, 41, 145–151. [Google Scholar] [CrossRef]
- Bedford, J.; Enria, D.; Giesecke, J.; Heymann, D.L.; Ihekweazu, C.; Kobinger, G.; Lane, H.C.; Memish, Z.; Oh, M.-D.; Schuchat, A.J.T.L. COVID-19: Towards controlling of a pandemic. Lancet 2020, 395, 1015–1018. [Google Scholar] [CrossRef]
- Moore, J.T.; Ricaldi, J.N.; Rose, C.E.; Fuld, J.; Parise, M.; Kang, G.J.; Driscoll, A.K.; Norris, T.; Wilson, N.; Rainisch, G.; et al. Disparities in Incidence of COVID-19 Among Underrepresented Racial/Ethnic Groups in Counties Identified as Hotspots During June 5–18, 2020—22 States, February–June 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1122. [Google Scholar] [CrossRef]
- Moore, J.P.; Klasse, P.J. COVID-19 Vaccines: “Warp Speed” Needs Mind Melds, Not Warped Minds. J. Virol. 2020, 94. [Google Scholar] [CrossRef]
- Santodomingo-Garzon, T.; Cunha, T.M.; Verri, W.A., Jr.; Valerio, D.A.; Parada, C.A.; Poole, S.; Ferreira, S.H.; Cunha, F.Q. Atorvastatin inhibits inflammatory hypernociception. Br. J. Pharm. 2006, 149, 14–22. [Google Scholar] [CrossRef] [Green Version]
- Rosenson, R.S. Low high-density lipoprotein cholesterol and cardiovascular disease: Risk reduction with statin therapy. Am. Heart J. 2006, 151, 556–563. [Google Scholar] [CrossRef]
- Ioannidis, J.P. More than a billion people taking statins? Potential implications of the new cardiovascular guidelines. JAMA 2014, 311, 463–464. [Google Scholar] [CrossRef] [PubMed]
- Zeiser, R. Immune modulatory effects of statins. Immunology 2018, 154, 69–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liao, J.K.; Laufs, U. Pleiotropic effects of statins. Annu. Rev. Pharm. Toxicol. 2005, 45, 89–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pertzov, B.; Eliakim-Raz, N.; Atamna, H.; Trestioreanu, A.Z.; Yahav, D.; Leibovici, L. Hydroxymethylglutaryl-CoA reductase inhibitors (statins) for the treatment of sepsis in adults-A systematic review and meta-analysis. Clin. Microbiol. Infect. 2019, 25, 280–289. [Google Scholar] [CrossRef] [Green Version]
- Fedson, D.S. Treating influenza with statins and other immunomodulatory agents. Antivir. Res. 2013, 99, 417–435. [Google Scholar] [CrossRef] [PubMed]
- Madjid, M.; Safavi-Naeini, P.; Solomon, S.D.; Vardeny, O. Potential Effects of Coronaviruses on the Cardiovascular System: A Review. JAMA Cardiol 2020. [Google Scholar] [CrossRef] [Green Version]
- Fedson, D.S.; Opal, S.M.; Rordam, O.M. Hiding in Plain Sight: An Approach to Treating Patients with Severe COVID-19 Infection. mBio 2020, 11. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.J.; Qin, J.J.; Cheng, X.; Shen, L.; Zhao, Y.C.; Yuan, Y.; Lei, F.; Chen, M.M.; Yang, H.; Bai, L.; et al. In-Hospital Use of Statins Is Associated with a Reduced Risk of Mortality among Individuals with COVID-19. Cell Metab. 2020, 32, 176–187.e174. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; Initiative, S. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2007, 147, 573–577. [Google Scholar] [CrossRef] [Green Version]
- Rosenbaum, P.R.; Rubin, D.B. Reducing bias in observational studies using subclassification on the propensity score. J. Am. Stat. Assoc. 1984, 79, 516–524. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Kurniawan, A. Dyslipidemia is associated with severe coronavirus disease 2019 (COVID-19) infection. Diabetes Metab. Syndr. 2020, 14, 1463–1465. [Google Scholar] [CrossRef] [PubMed]
- Fedson, D.S. Pandemic influenza: A potential role for statins in treatment and prophylaxis. Clin. Infect. Dis. 2006, 43, 199–205. [Google Scholar] [CrossRef] [PubMed]
- de Jong, M.D.; Simmons, C.P.; Thanh, T.T.; Hien, V.M.; Smith, G.J.; Chau, T.N.; Hoang, D.M.; Chau, N.V.; Khanh, T.H.; Dong, V.C.; et al. Fatal outcome of human influenza A (H5N1) is associated with high viral load and hypercytokinemia. Nat. Med. 2006, 12, 1203–1207. [Google Scholar] [CrossRef] [PubMed]
- Haidari, M.; Zhang, W.; Ganjehei, L.; Ali, M.; Chen, Z. Inhibition of MLC phosphorylation restricts replication of influenza virus--a mechanism of action for anti-influenza agents. PLoS ONE 2011, 6, e21444. [Google Scholar] [CrossRef] [PubMed]
- Sun, X.; Whittaker, G.R. Role for influenza virus envelope cholesterol in virus entry and infection. J. Virol. 2003, 77, 12543–12551. [Google Scholar] [CrossRef] [Green Version]
- Fedson, D.S. Confronting the next influenza pandemic with anti-inflammatory and immunomodulatory agents: Why they are needed and how they might work. Influenza Other Respir Viruses 2009, 3, 129–142. [Google Scholar] [CrossRef] [PubMed]
- Bifulco, M.; Gazzerro, P. Statin therapy in COVID-19 infection: Much more than a single pathway. Eur. Heart J. Cardiovasc. Pharm. 2020. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Before Propensity Score Matching (n = 124,330) | After Propensity Score Matching (n = 34,312) | |||||
|---|---|---|---|---|---|---|
| Statin User n = 22,633 | Control Group n = 101,697 | ASD | Statin User n = 17,156 | Control Group n = 17,156 | ASD | |
| Age, year | ||||||
| 20–29 | 146 (0.6) | 32,234 (31.7) | 146 (0.9) | 179 (1.0) | ||
| 30–39 | 331 (1.5) | 12,823 (12.6) | 0.929 | 329 (1.9) | 220 (1.3) | 0.053 |
| 40–49 | 1222 (5.4) | 15,297 (15.0) | 0.427 | 1176 (6.9) | 854 (5.0) | 0.083 |
| 50–59 | 5513 (24.4) | 19,747 (19.4) | 0.115 | 4768 (27.8) | 4786 (27.9) | 0.002 |
| 60–69 | 7640 (33.8) | 12,029 (11.8) | 0.463 | 5503 (32.1) | 5820 (33.9) | 0.039 |
| 70–79 | 4965 (21.9) | 5461 (5.4) | 0.400 | 3232 (18.8) | 3221 (18.8) | 0.002 |
| ≥80 | 2816 (12.4) | 4106 (4.0) | 0.255 | 2002 (11.7) | 2076 (12.1) | 0.013 |
| Sex, male | 8147 (36.0) | 40,579 (39.9) | 0.081 | 6141 (35.8) | 6263 (36.5) | 0.015 |
| Residence | ||||||
| Seoul | 1001 (4.4) | 7055 (6.9) | 788 (4.6) | 778 (4.5) | ||
| Gyeonggi-do | 15,533 (68.6) | 65,960 (64.9) | 0.081 | 11,654 (67.9) | 11,603 (67.6) | 0.006 |
| Daegu | 1111 (4.9) | 5744 (5.6) | 0.034 | 839 (4.9) | 845 (4.9) | 0.002 |
| Gyeongsangbuk-do | 3242 (14.3) | 11,865 (11.7) | 0.076 | 2488 (14.5) | 2551 (14.9) | 0.011 |
| Other area | 1746 (7.7) | 11,073 (10.9) | 0.119 | 1387 (8.1) | 1379 (8.0) | 0.002 |
| Underlying disability | 2687 (11.9) | 4968 (4.9) | 0.216 | 1836 (10.7) | 1913 (11.2) | 0.014 |
| Income level | ||||||
| Q1 (Lowest) | 5999 (26.5) | 26,388 (25.9) | 4490 (26.2) | 4481 (26.1) | ||
| Q2 | 3496 (15.4) | 21,483 (21.1) | 0.157 | 2782 (16.2) | 2773 (16.2) | 0.002 |
| Q3 | 4887 (21.6) | 22,887 (22.5) | 0.022 | 3732 (21.8) | 3694 (21.5) | 0.005 |
| Q4 (Highest) | 7892 (34.9) | 29,177 (28.7) | 0.130 | 5886 (34.3) | 5936 (34.6) | 0.006 |
| Unknown | 359 (1.6) | 1762 (1.7) | 0.012 | 266 (1.6) | 272 (1.6) | 0.003 |
| Charlson comorbidity index 2020 | 3.6 (3.4) | 1.4 (2.6) | 0.640 | 3.2 (3.2) | 3.1 (3.3) | 0.018 |
| Hypertension | 15,826 (69.9) | 16,901 (16.6) | 1.162 | 10,663 (62.2) | 11,185 (65.2) | 0.066 |
| DM without chronic complication | 8099 (35.8) | 5682 (5.6) | 0.630 | 4668 (27.2) | 4403 (25.7) | 0.032 |
| DM with chronic complication | 2944 (13.0) | 1311 (1.3) | 0.348 | 1560 (9.1) | 1171 (6.8) | 0.067 |
| Peripheral vascular disease | 3901 (17.2) | 3297 (3.2) | 0.371 | 2446 (14.3) | 2190 (12.8) | 0.039 |
| Renal disease | 733 (3.2) | 659 (0.6) | 0.146 | 438 (2.6) | 415 (2.4) | 0.008 |
| Rheumatic disease | 1097 (4.8) | 1861 (1.8) | 0.141 | 699 (4.1) | 790 (4.6) | 0.025 |
| Dementia | 1684 (7.4) | 2242 (2.2) | 0.200 | 1168 (6.8) | 1239 (7.2) | 0.016 |
| Peptic ulcer disease | 3331 (14.7) | 6541 (6.4) | 0.233 | 2345 (13.7) | 2334 (13.6) | 0.002 |
| Hemiplegia or paraplegia | 204 (0.9) | 364 (0.4) | 0.058 | 150 (0.9) | 147 (0.9) | 0.002 |
| Moderate or severe liver disease | 43 (0.2) | 103 (0.1) | 0.020 | 34 (0.2) | 35 (0.2) | 0.001 |
| Mild liver disease | 6117 (27.0) | 7495 (7.4) | 0.442 | 3967 (23.1) | 3975 (23.2) | 0.001 |
| Chronic pulmonary disease | 4303 (19.0) | 9813 (9.6) | 0.239 | 3027 (17.6) | 3059 (17.8) | 0.005 |
| Cerebrovascular disease | 3447 (15.2) | 2316 (2.3) | 0.360 | 1971 (11.5) | 1651 (9.6) | 0.052 |
| Congestive heart failure | 2079 (9.2) | 1604 (1.6) | 0.263 | 1241 (7.2) | 1077 (6.3) | 0.033 |
| Myocardial infarction | 722 (3.2) | 465 (0.5) | 0.156 | 329 (1.9) | 232 (1.4) | 0.032 |
| Malignancy | 6157 (27.2) | 15,856 (15.6) | 0.261 | 4355 (25.4) | 4439 (25.9) | 0.011 |
| Metastatic solid tumor | 1350 (6.0) | 2722 (2.7) | 0.139 | 963 (5.6) | 1049 (6.1) | 0.021 |
| AIDS/HIV | 2 (0.0) | 30 (0.0) | 0.022 | 2 (0.0) | 4 (0.0) | 0.012 |
| Other cardiovascular drug use | ||||||
| Aspirin | 4845 (21.4) | 2009 (2.0) | 0.474 | 2468 (14.4) | 1862 (10.9) | 0.086 |
| Clopidogrel | 2874 (12.7) | 823 (0.8) | 0.357 | 1353 (7.9) | 797 (4.6) | 0.097 |
| ACEi | 575 (2.5) | 191 (0.2) | 0.150 | 272 (1.6) | 171 (1.0) | 0.037 |
| ARB | 9836 (43.5) | 8020 (7.9) | 0.718 | 6285 (36.6) | 6390 (37.2) | 0.012 |
| CCB | 4954 (21.9) | 3687 (3.6) | 0.442 | 3094 (18.0) | 2983 (17.4) | 0.016 |
| Beta blocker | 2203 (9.7) | 1206 (1.2) | 0.288 | 1189 (6.9) | 997 (5.8) | 0.038 |
| Variable | Development of COVID-19 | Logistic Regression Analysis | p-Value |
|---|---|---|---|
| OR (95% CI) | |||
| Before PSM | |||
| Control group | 6471/101,697 (6.4) | 1 | |
| Statin user | 1309/22,633 (5.8) | 0.90 (0.85, 0.96) | 0.0011 |
| After PSM | |||
| Control group | 1395/17,156 (8.1) | 1 | |
| Statin user | 938/17,156 (5.5) | 0.65 (0.60 0.71) | <0.001 |
| Variable | Multivariable Model | p-Value |
|---|---|---|
| OR (95% CI) | ||
| Statin users (vs control group) | 0.59 (0.55, 0.64) | <0.001 |
| Age, year | ||
| 20–29 | 1 | |
| 30–39 | 0.91 (0.84, 1.00) | 0.038 |
| 40–49 | 0.86 (0.79, 0.93) | <0.001 |
| 50–59 | 0.77 (0.72, 0.83) | <0.001 |
| 60–69 | 0.63 (0.58, 0.69) | <0.001 |
| 70–79 | 0.46 (0.41, 0.52) | <0.001 |
| ≥80 | 0.35 (0.30, 0.40) | <0.001 |
| Income level | ||
| Q1 | 1 | |
| Q2 | 0.80 (0.75, 0.86) | <0.001 |
| Q3 | 0.78 (0.73, 0.84) | <0.001 |
| Q4 | 0.84 (0.79, 0.90) | <0.001 |
| Unknown | 0.77 (0.63, 0.94) | 0.009 |
| Sex, male | 1.03 (0.98, 1.08) | 0.227 |
| Residence | ||
| Seoul | 1 | |
| Gyeonggi-do | 0.92 (0.83, 1.01) | 0.078 |
| Daegu | 0.98 (0.86, 1.13) | 0.789 |
| Gyeongsangbuk-do | 0.89 (0.80, 1.01) | 0.062 |
| Other area | 0.88 (0.78, 0.99) | 0.031 |
| Underlying disability | 1.04 (0.94, 1.15) | 0.430 |
| Underlying comorbidities | ||
| Hypertension | 1.04 (0.95, 1.13) | 0.406 |
| DM without chronic complication | 1.94 (1.80, 2.09) | <0.001 |
| DM with chronic complication | 0.89 (0.78, 1.02) | 0.101 |
| Peripheral vascular disease | 0.79 (0.71, 0.88) | <0.001 |
| Renal disease | 0.89 (0.72, 1.09) | 0.250 |
| Rheumatic disease | 0.94 (0.82, 1.08) | 0.387 |
| Dementia | 1.83 (1.61, 2.09) | <0.001 |
| Peptic ulcer disease | 1.26 (1.17, 1.36) | <0.001 |
| Hemiplegia or paraplegia | 2.23 (1.72, 2.87) | <0.001 |
| Moderate or severe liver disease | 0.46 (0.25, 0.85) | 0.013 |
| Mild liver disease | 1.99 (1.86, 2.14) | <0.001 |
| Chronic pulmonary disease | 3.63 (3.42, 3.84) | <0.001 |
| Cerebrovascular disease | 1.16 (1.03, 1.32) | 0.017 |
| Congestive heart failure | 2.89 (2.60, 3.23) | <0.001 |
| Myocardial infarction | 6.43 (5.49, 7.54) | <0.001 |
| Malignancy | 1.71 (1.62, 1.81) | <0.001 |
| Metastatic solid tumor | 0.82 (0.73, 0.93) | 0.003 |
| AIDS/HIV | 2.99 (1.27, 7.05) | 0.012 |
| Other cardiovascular drug use | ||
| Aspirin | 0.75 (0.66, 0.86) | <0.001 |
| Clopidogrel | 0.70 (0.59, 0.83) | <0.001 |
| ACEi | 0.80 (0.60, 1.08) | 0.145 |
| ARB | 0.81 (0.74, 0.89) | <0.001 |
| CCB | 0.93 (0.83, 1.04) | 0.225 |
| Beta blocker | 0.59 (0.49, 0.71) | <0.001 |
| Variable | Multivariable Model | p-Value |
|---|---|---|
| OR (95% CI) | ||
| Statin users (vs control group) | 0.74 (0.52, 1.05) | 0.094 |
| Age, 10 year increase | 2.95 (2.48, 3.50) | <0.001 |
| Income level 2020 (Feb) | ||
| Q1 (Lowest) | 1 | |
| Q2 | 0.95 (0.58, 1.55) | 0.834 |
| Q3 | 1.09 (0.71, 1.67) | 0.698 |
| Q4 (highest) | 0.91 (0.63, 1.31) | 0.605 |
| Unknown | 0.54 (0.14, 2.10) | 0.374 |
| Sex, male | 2.23 (1.65, 3.03) | <0.001 |
| Residence at Februrary, 2020 | ||
| Seoul | 1 | |
| Gyeonggi-do | 2.10 (0.68, 6.45) | 0.196 |
| Daegu | 2.96 (0.84, 10.46) | 0.092 |
| Gyeongsangbuk-do | 2.17 (0.68, 6.89) | 0.190 |
| Other area | 1.60 (0.47, 5.52) | 0.455 |
| Underlying disability | 1.25 (0.88, 1.78) | 0.207 |
| Underlying comorbidities | ||
| Hypertension | 1.69 (1.08, 2.63) | 0.021 |
| DM without chronic complication | 1.86 (1.34, 2.57) | <0.001 |
| DM with chronic complication | 1.66 (1.09, 2.54) | 0.019 |
| Peripheral vascular disease | 1.10 (0.74, 1.63) | 0.632 |
| Renal disease | 1.59 (0.95, 2.65) | 0.076 |
| Rheumatic disease | 0.60 (0.31, 1.14) | 0.118 |
| Dementia | 1.55 (1.07, 2.25) | 0.021 |
| Peptic ulcer disease | 1.05 (0.74, 1.51) | 0.773 |
| Hemiplegia or paraplegia | 2.07 (1.11, 3.86) | 0.023 |
| Moderate or severe liver disease | 5.23 (1.32, 20.75) | 0.019 |
| Mild liver disease | 0.79 (0.58, 1.09) | 0.148 |
| Chronic pulmonary disease | 1.81 (1.33, 2.47) | <0.001 |
| Cerebrovascular disease | 0.64 (0.42, 0.98) | 0.042 |
| Congestive heart failure | 1.80 (1.30, 2.51) | <0.001 |
| Myocardial infarction | 0.84 (0.50, 1.41) | 0.506 |
| Malignancy | 0.96 (0.70, 1.32) | 0.816 |
| Metastatic solid tumor | 1.60 1.03 2.47 | 0.035 |
| AIDS/HIV | 1.12 0.08 15.23 | 0.933 |
| Other cardiovascular drug use | ||
| Aspirin | 1.06 (0.70, 1.58) | 0.792 |
| Clopidogrel | 1.36 (0.83, 2.24) | 0.220 |
| ACEi | 1.22 (0.55, 2.73) | 0.620 |
| ARB | 0.82 (0.58, 1.16) | 0.263 |
| CCB | 0.55 (0.36, 0.84) | 0.006 |
| Beta blocker | 1.52 (0.84, 2.76) | 0.170 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, T.K.; Song, I.-A.; Jeon, Y.-T. Statin Therapy and the Risk of COVID-19: A Cohort Study of the National Health Insurance Service in South Korea. J. Pers. Med. 2021, 11, 116. https://doi.org/10.3390/jpm11020116
Oh TK, Song I-A, Jeon Y-T. Statin Therapy and the Risk of COVID-19: A Cohort Study of the National Health Insurance Service in South Korea. Journal of Personalized Medicine. 2021; 11(2):116. https://doi.org/10.3390/jpm11020116
Chicago/Turabian StyleOh, Tak Kyu, In-Ae Song, and Young-Tae Jeon. 2021. "Statin Therapy and the Risk of COVID-19: A Cohort Study of the National Health Insurance Service in South Korea" Journal of Personalized Medicine 11, no. 2: 116. https://doi.org/10.3390/jpm11020116
APA StyleOh, T. K., Song, I. -A., & Jeon, Y. -T. (2021). Statin Therapy and the Risk of COVID-19: A Cohort Study of the National Health Insurance Service in South Korea. Journal of Personalized Medicine, 11(2), 116. https://doi.org/10.3390/jpm11020116