
Indocyanine Green Angiography for Parathyroid Gland Evaluation during Transoral Endoscopic Thyroidectomy



Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Parathyroid Assessment
2.3. Outcome Evaluation and Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Demographics
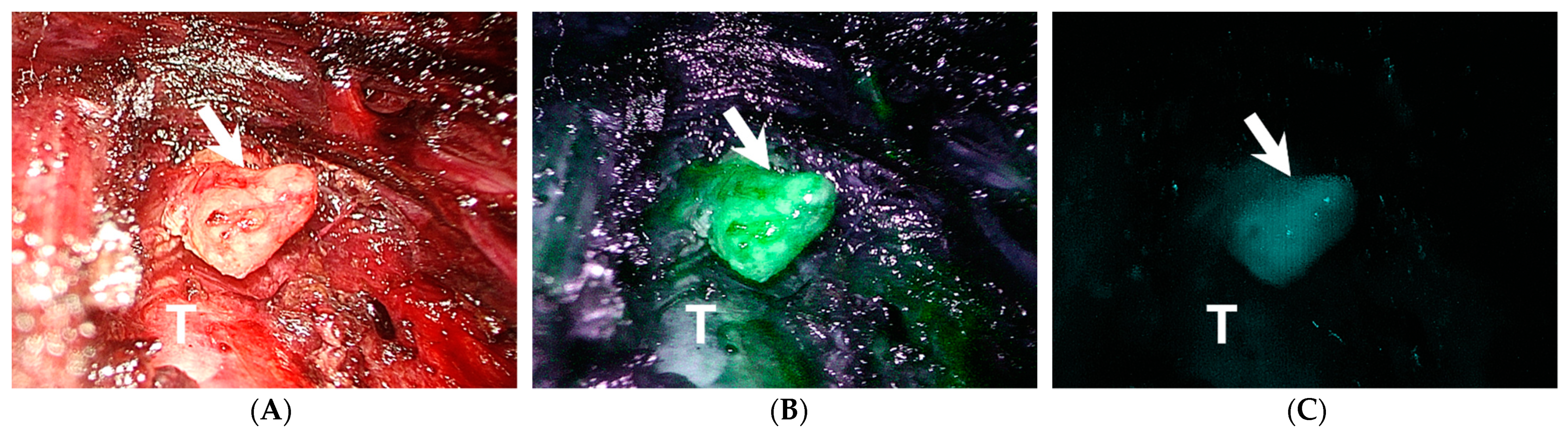
3.2. Parathyroid Gland Identification
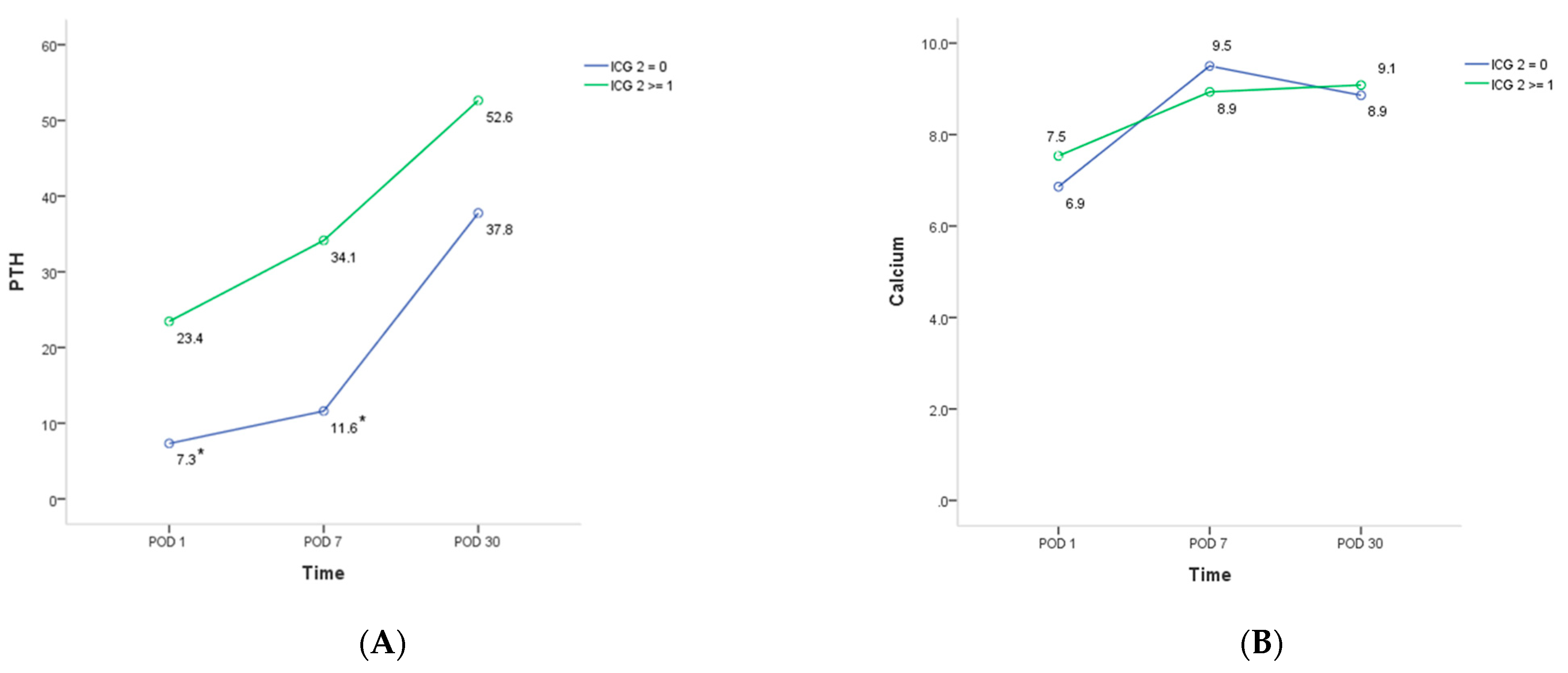
3.3. Parathyroid Glands Perfusion
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Solorzano, C.C.; Thomas, G.; Berber, E.; Wang, T.S.; Randolph, G.W.; Duh, Q.Y.; Triponez, F. Current state of intraoperative use of near infrared fluorescence for parathyroid identification and preservation. Surgery 2021, 169, 868–878. [Google Scholar] [CrossRef] [PubMed]
- Spartalis, E.; Ntokos, G.; Georgiou, K.; Zografos, G.; Tsourouflis, G.; Dimitroulis, D.; Nikiteas, N.I. Intraoperative Indocyanine Green (ICG) Angiography for the Identification of the Parathyroid Glands: Current Evidence and Future Perspectives. In Vivo (Athens, Greece) 2020, 34, 23–32. [Google Scholar] [CrossRef] [PubMed]
- DeLong, J.C.; Ward, E.P.; Lwin, T.M.; Brumund, K.T.; Kelly, K.J.; Horgan, S.; Bouvet, M. Indocyanine green fluorescence-guided parathyroidectomy for primary hyperparathyroidism. Surgery 2018, 163, 388–392. [Google Scholar] [CrossRef]
- Zaidi, N.; Bucak, E.; Yazici, P.; Soundararajan, S.; Okoh, A.; Yigitbas, H.; Dural, C.; Berber, E. The feasibility of indocyanine green fluorescence imaging for identifying and assessing the perfusion of parathyroid glands during total thyroidectomy. J. Surg. Oncol. 2016, 113, 775–778. [Google Scholar] [CrossRef] [PubMed]
- Anuwong, A.; Ketwong, K.; Jitpratoom, P.; Sasanakietkul, T.; Duh, Q.Y. Safety and Outcomes of the Transoral Endoscopic Thyroidectomy Vestibular Approach. JAMA Surg. 2018, 153, 21–27. [Google Scholar] [CrossRef]
- Xing, Z.; Qiu, Y.; Abuduwaili, M.; Xia, B.; Fei, Y.; Zhu, J.; Su, A. Surgical outcomes of different approaches in robotic assisted thyroidectomy for thyroid cancer: A systematic review and Bayesian network meta-analysis. Int. J. Surg. (Lond. Engl.) 2021, 89, 105941. [Google Scholar] [CrossRef] [PubMed]
- Kandil, E.; Hammad, A.Y.; Walvekar, R.R.; Hu, T.; Masoodi, H.; Mohamed, S.E.; Deniwar, A.; Stack, B.C., Jr. Robotic Thyroidectomy Versus Nonrobotic Approaches: A Meta-Analysis Examining Surgical Outcomes. Surg. Innov. 2016, 23, 317–325. [Google Scholar] [CrossRef]
- Wu, Y.J.; Cheng, B.C.; Chiu, C.H.; Huang, S.C.; Li, L.C.; Chung, S.Y.; Den Chen, K.; Pan, C.C.; Li, J.Y.; Lin, H.W.; et al. Successful Modified Transoral Endoscopic Parathyroidectomy Vestibular Approach For Secondary Hyperparathyroidism With Ectopic Mediastinal Glands. Surg. Laparosc. Endosc. Percutaneous Tech. 2019, 29, e88–e93. [Google Scholar] [CrossRef]
- Cohen, O.; Tufano, R.P.; Anuwong, A.; Shaha, A.R.; Olsen, K.D.; Zafereo, M.; Rinaldo, A.; Mäkitie, A.A.; Nixon, I.J.; Russell, J.O.; et al. Transoral endoscopic vestibular approach for thyroidectomy and parathyroidectomy—From promise to practice. Am. J. Otolaryngol. 2021, 42, 103022. [Google Scholar] [CrossRef]
- Yu, H.W.; Chung, J.W.; Yi, J.W.; Song, R.Y.; Lee, J.H.; Kwon, H.; Kim, S.J.; Chai, Y.J.; Choi, J.Y.; Lee, K.E. Intraoperative localization of the parathyroid glands with indocyanine green and Firefly(R) technology during BABA robotic thyroidectomy. Surg. Endosc. 2017, 31, 3020–3027. [Google Scholar] [CrossRef]
- Turan, M.I.; Celik, M.; Erturk, M.S. Indocyanine green fluorescence angiography-guided transoral endoscopic thyroidectomy and parathyroidectomy: First clinical report. Photodiagnosis Photodyn. Ther. 2020, 32, 102028. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, J.G.; Zhang, S.Z.; Chen, G. Comparison of indocyanine green and carbon nanoparticles in endoscopic techniques for central lymph nodes dissection in patients with papillary thyroid cancer. Surg. Endosc. 2020, 34, 5354–5359. [Google Scholar] [CrossRef] [PubMed]
- Anuwong, A.; Sasanakietkul, T.; Jitpratoom, P.; Ketwong, K.; Kim, H.Y.; Dionigi, G.; Richmon, J.D. Transoral endoscopic thyroidectomy vestibular approach (TOETVA): Indications, techniques and results. Surg. Endosc. 2018, 32, 456–465. [Google Scholar] [CrossRef]
- Liang, T.J.; Tsai, C.Y.; Chen, I.S. Foley Balloon Facilitates Creation of Working Space in Transoral Thyroidectomy. World J. Surg. 2020, 44, 1514–1517. [Google Scholar] [CrossRef] [PubMed]
- Liang, T.J.; Wang, N.Y.; Tsai, C.Y.; Liu, S.I.; Chen, I.S. Outcome Comparison between Endoscopic Transoral and Bilateral Axillo-Breast Approach Thyroidectomy Performed by a Single Surgeon. World J. Surg. 2021, 45, 1779–1784. [Google Scholar] [CrossRef]
- Rudin, A.V.; McKenzie, T.J.; Thompson, G.B.; Farley, D.R.; Lyden, M.L. Evaluation of Parathyroid Glands with Indocyanine Green Fluorescence Angiography After Thyroidectomy. World J. Surg. 2019, 43, 1538–1543. [Google Scholar] [CrossRef]
- Vidal Fortuny, J.; Sadowski, S.M.; Belfontali, V.; Guigard, S.; Poncet, A.; Ris, F.; Karenovics, W.; Triponez, F. Randomized clinical trial of intraoperative parathyroid gland angiography with indocyanine green fluorescence predicting parathyroid function after thyroid surgery. Br. J. Surg. 2018, 105, 350–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bliss, R.D.; Gauger, P.G.; Delbridge, L.W. Surgeon’s approach to the thyroid gland: Surgical anatomy and the importance of technique. World J. Surg. 2000, 24, 891–897. [Google Scholar] [CrossRef]
- Solórzano, C.C.; Thomas, G.; Baregamian, N.; Mahadevan-Jansen, A. Detecting the Near Infrared Autofluorescence of the Human Parathyroid: Hype or Opportunity? Ann. Surg. 2020, 272, 973–985. [Google Scholar] [CrossRef]
- De Leeuw, F.; Breuskin, I.; Abbaci, M.; Casiraghi, O.; Mirghani, H.; Ben Lakhdar, A.; Laplace-Builhé, C.; Hartl, D. Intraoperative Near-infrared Imaging for Parathyroid Gland Identification by Auto-fluorescence: A Feasibility Study. World J. Surg. 2016, 40, 2131–2138. [Google Scholar] [CrossRef]
- Moore, E.C.; Rudin, A.; Alameh, A.; Berber, E. Near-infrared imaging in re-operative parathyroid surgery: First description of autofluorescence from cryopreserved parathyroid glands. Gland Surg. 2019, 8, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Abbaci, M.; De Leeuw, F.; Breuskin, I.; Casiraghi, O.; Lakhdar, A.B.; Ghanem, W.; Laplace-Builhé, C.; Hartl, D. Parathyroid gland management using optical technologies during thyroidectomy or parathyroidectomy: A systematic review. Oral Oncol. 2018, 87, 186–196. [Google Scholar] [CrossRef] [PubMed]
- Barrios, L.; Shafqat, I.; Alam, U.; Ali, N.; Patio, C.; Filarski, C.F.; Bankston, H.; Mallen-St. Clair, J.; Luu, M.; Zumsteg, Z.S.; et al. Incidental parathyroidectomy in thyroidectomy and central neck dissection. Surgery 2021, 169, 1145–1151. [Google Scholar] [CrossRef] [PubMed]
- Sakorafas, G.H.; Stafyla, V.; Bramis, C.; Kotsifopoulos, N.; Kolettis, T.; Kassaras, G. Incidental parathyroidectomy during thyroid surgery: An underappreciated complication of thyroidectomy. World J. Surg. 2005, 29, 1539–1543. [Google Scholar] [CrossRef]
- Vidal Fortuny, J.; Belfontali, V.; Sadowski, S.M.; Karenovics, W.; Guigard, S.; Triponez, F. Parathyroid gland angiography with indocyanine green fluorescence to predict parathyroid function after thyroid surgery. Br. J. Surg. 2016, 103, 537–543. [Google Scholar] [CrossRef] [Green Version]
- Lang, B.H.; Wong, C.K.; Hung, H.T.; Wong, K.P.; Mak, K.L.; Au, K.B. Indocyanine green fluorescence angiography for quantitative evaluation of in situ parathyroid gland perfusion and function after total thyroidectomy. Surgery 2017, 161, 87–95. [Google Scholar] [CrossRef]
- Cui, L.; Gao, Y.; Yu, H.; Li, M.; Wang, B.; Zhou, T.; Hu, Q. Intraoperative Parathyroid Localization with Near-Infrared Fluorescence Imaging Using Indocyanine Green during Total Parathyroidectomy for Secondary Hyperparathyroidism. Sci. Rep. 2017, 7, 8193. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Patients (n = 60) | |
|---|---|
| Age (years) | 45.4 ± 12.8 |
| Sex ratio (F:M) | 50:10 |
| Body mass index (kg/m2) | 22.9 ± 3.0 |
| Tumor size (cm) | 2.3 ± 1.0 |
| Surgical Procedure | |
| Lobectomy | 41 (68.3%) |
| Total thyroidectomy | 19 (31.7%) |
| Central neck dissection 1 | 22 (36.7%) |
| Lymph nodes | |
| Retrieved | 3.0 ± 2.7 |
| Involved | 0.9 ± 1.6 |
| Pathology | |
| Benign | 31 (51.7%) |
| malignant | 29 (48.3%) |
| Hospital stay (day) | 3.9 ± 0.5 |
| Lesion Side 1 | Contralateral Side | |||
|---|---|---|---|---|
| Superior Parathyroid (n = 60) | Inferior Parathyroid (n = 60) | Super Parathyroid (n = 19) | Inferior Parathyroid (n = 19) | |
| Visual score | ||||
| 2 | 48 (80.0%) | 41 (68.3%) | 18 (94.7%) | 18 (94.7%) |
| 0 | 1(1.7%) | 0 (0%) | 0 (0%) | 0 (0%) |
| Not identified, initially | 11 (18.3%) | 19 (31.7%) | 1 (5.3%) | 1 (5.3%) |
| Identified after ICG 2 | 1 (1.7%) | 8 (13.3%) | 0 (0%) | 0 (0%) |
| ICG score | ||||
| 2 | 25 (41.7%) | 27 (45.0%) | 5 (26.3%) | 8 (42.1%) |
| 1 | 22 (36.7%) | 21 (35.0%) 3 | 12 (63.2%) | 10 (52.6%) |
| 0 | 3 (5%) | 1 (1.7%) | 1 (5.3%) | 0 (0%) |
| Not identified | 10 (16.7%) | 11 (18.3%) | 1 (5.3%) | 1 (5.3%) |
| Parameter | Value |
|---|---|
| Incidental parathyroidectomy, n | 12 (7.6%) |
| Location | |
| Superior gland | 2 (16.7%) |
| Inferior gland | 10 (83.3%) |
| Cause of parathyroid gland removal | |
| Not identified 1 | 9 (75.0%) |
| Misidentified 2 | 3 (25.0%) |
| Thyroid pathology | |
| Benign | 4 (33.3%) |
| Malignant | 8 (66.7%) |
| Surgical procedure | |
| Lobectomy | 8 (66.7%) |
| Total thyroidectomy | 4 (33.3%) |
| Central neck dissection | 8 (66.7%) |
| ICG 2 = 0 (n = 5) | ICG 2 ≥ 1 1 (n = 14) | p | |
|---|---|---|---|
| PTH < 15 (pg/mL) 2 | |||
| POD 1 | 4 (80%) | 3 (21.4%) | 0.038 |
| POD 7 | 4 (80%) | 0 (0%) | 0.001 |
| POD 30 | 0 (0%) | 0 (0%) | N.A. |
| Calcium < 8.4 (mg/dL) 2 | |||
| POD 1 | 5 (100%) | 11 (78.6%) | 0.376 |
| POD 7 | 0 (0%) | 1 (7.1%) | 0.737 |
| POD 30 | 0 (0%) | 0 (0%) | N.A. |
| Incidental parathyroidectomy, n | 1 (20%) | 3 (21.4%) | 0.728 |
| Duration of calcium supplement, day | 18.2 ± 9.4 | 8.0 ± 6.1 | 0.034 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, T.-J.; Wang, K.-C.; Wang, N.-Y.; Chen, I.-S.; Liu, S.-I. Indocyanine Green Angiography for Parathyroid Gland Evaluation during Transoral Endoscopic Thyroidectomy. J. Pers. Med. 2021, 11, 843. https://doi.org/10.3390/jpm11090843
Liang T-J, Wang K-C, Wang N-Y, Chen I-S, Liu S-I. Indocyanine Green Angiography for Parathyroid Gland Evaluation during Transoral Endoscopic Thyroidectomy. Journal of Personalized Medicine. 2021; 11(9):843. https://doi.org/10.3390/jpm11090843
Chicago/Turabian StyleLiang, Tsung-Jung, Kuo-Chiang Wang, Nai-Yu Wang, I-Shu Chen, and Shiuh-Inn Liu. 2021. "Indocyanine Green Angiography for Parathyroid Gland Evaluation during Transoral Endoscopic Thyroidectomy" Journal of Personalized Medicine 11, no. 9: 843. https://doi.org/10.3390/jpm11090843