
Progression Risk Score Estimation Based on Immunostaining Data in Oral Cancer Using Unsupervised Hierarchical Clustering Analysis: A Retrospective Study in Taiwan

 , , , and
, , , and
Abstract
:1. Introduction
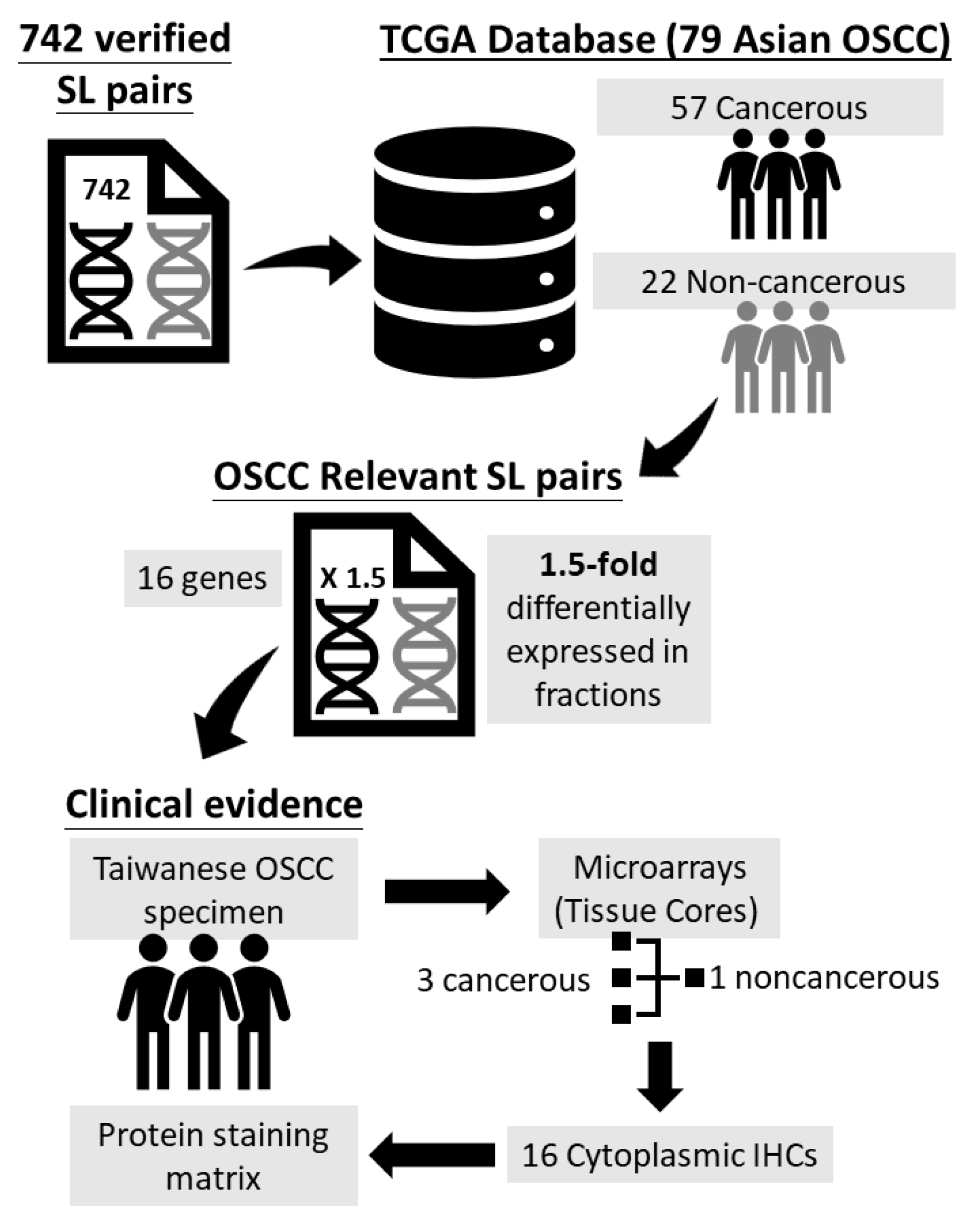
2. Materials and Methods
2.1. Patient Selection
2.2. Tissue Microarrays and Immunostaining
2.3. Data Analysis
3. Results
3.1. Baseline Characteristics
3.2. Unsupervised Hierarchical Clustering Analysis
3.3. Cytoplasmic IHC Stainings and PRS Calculation
3.4. PRS Risk Strata Survival Analysis and Model Comparison
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Adelstein, D.; Gillison, M.L.; Pfister, D.G.; Spencer, S.; Adkins, D.; Brizel, D.M.; Burtness, B.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. NCCN Guidelines Insights: Head and Neck Cancers, Version 2.2017. J. Natl. Compr. Cancer Netw. 2017, 15, 761–770. [Google Scholar] [CrossRef]
- Bernier, J.; Domenge, C.; Ozsahin, M.; Matuszewska, K.; Lefebvre, J.L.; Greiner, R.H.; Giralt, J.; Maingon, P.; Rolland, F.; Bolla, M.; et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N. Engl. J. Med. 2004, 350, 1945–1952. [Google Scholar] [CrossRef] [Green Version]
- Cooper, J.S.; Pajak, T.F.; Forastiere, A.A.; Jacobs, J.; Campbell, B.H.; Saxman, S.B.; Kish, J.A.; Kim, H.E.; Cmelak, A.J.; Rotman, M.; et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2004, 350, 1937–1944. [Google Scholar] [CrossRef] [Green Version]
- Rajthala, S.; Dongre, H.; Parajuli, H.; Min, A.; Nginamau, E.S.; Kvalheim, A.; Lybak, S.; Sapkota, D.; Johannessen, A.C.; Costea, D.E. Combined In Situ Hybridization and Immunohistochemistry on Archival Tissues Reveals Stromal microRNA-204 as Prognostic Biomarker for Oral Squamous Cell Carcinoma. Cancers 2021, 13, 1307. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, L.; Xie, X. RFC4 promotes the progression and growth of Oral Tongue squamous cell carcinoma in vivo and vitro. J. Clin. Lab. Anal. 2021, 35, e23761. [Google Scholar] [CrossRef] [PubMed]
- Galot, R.; Le Tourneau, C.; Guigay, J.; Licitra, L.; Tinhofer, I.; Kong, A.; Caballero, C.; Fortpied, C.; Bogaerts, J.; Govaerts, A.S.; et al. Personalized biomarker-based treatment strategy for patients with squamous cell carcinoma of the head and neck: EORTC position and approach. Ann. Oncol. 2018, 29, 2313–2327. [Google Scholar] [CrossRef] [Green Version]
- Renfro, L.A.; Sargent, D.J. Statistical controversies in clinical research: Basket trials, umbrella trials, and other master protocols: A review and examples. Ann. Oncol. 2017, 28, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Riechelmann, H.; Steinbichler, T.B.; Sprung, S.; Santer, M.; Runge, A.; Ganswindt, U.; Gamerith, G.; Dudas, J. The Epithelial-Mesenchymal Transcription Factor Slug Predicts Survival Benefit of Up-Front Surgery in Head and Neck Cancer. Cancers 2021, 13, 772. [Google Scholar] [CrossRef] [PubMed]
- Au, N.H.; Cheang, M.; Huntsman, D.G.; Yorida, E.; Coldman, A.; Elliott, W.M.; Bebb, G.; Flint, J.; English, J.; Gilks, C.B.; et al. Evaluation of immunohistochemical markers in non-small cell lung cancer by unsupervised hierarchical clustering analysis: A tissue microarray study of 284 cases and 18 markers. J. Pathol. 2004, 204, 101–109. [Google Scholar] [CrossRef]
- Lin, I.H.; Chen, D.T.; Chang, Y.F.; Lee, Y.L.; Su, C.H.; Cheng, C.; Tsai, Y.C.; Ng, S.C.; Chen, H.T.; Lee, M.C.; et al. Hierarchical clustering of breast cancer methylomes revealed differentially methylated and expressed breast cancer genes. PLoS ONE 2015, 10, e0118453. [Google Scholar] [CrossRef]
- Tiong, K.L.; Chang, K.C.; Yeh, K.T.; Liu, T.Y.; Wu, J.H.; Hsieh, P.H.; Lin, S.H.; Lai, W.Y.; Hsu, Y.C.; Chen, J.Y.; et al. CSNK1E/CTNNB1 are synthetic lethal to TP53 in colorectal cancer and are markers for prognosis. Neoplasia 2014, 16, 441–450. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.G.; Chen, C.C.; Wu, Y.Y.; Che, T.F.; Huang, Y.S.; Yeh, K.T.; Shieh, G.S.; Yang, P.C. Uncovering synthetic lethal interactions for therapeutic targets and predictive markers in lung adenocarcinoma. Oncotarget 2016, 7, 73664–73680. [Google Scholar] [CrossRef] [Green Version]
- Edgar, R.; Domrachev, M.; Lash, A.E. Gene Expression Omnibus: NCBI gene expression and hybridization array data repository. Nucleic Acids Res. 2002, 30, 207–210. [Google Scholar] [CrossRef] [Green Version]
- Peng, C.H.; Liao, C.T.; Peng, S.C.; Chen, Y.J.; Cheng, A.J.; Juang, J.L.; Tsai, C.Y.; Chen, T.C.; Chuang, Y.J.; Tang, C.Y.; et al. A novel molecular signature identified by systems genetics approach predicts prognosis in oral squamous cell carcinoma. PLoS ONE 2011, 6, e23452. [Google Scholar] [CrossRef]
- Wang, H.C.; Chiang, C.J.; Liu, T.C.; Wu, C.C.; Chen, Y.T.; Chang, J.G.; Shieh, G.S. Immunohistochemical Expression of Five Protein Combinations Revealed as Prognostic Markers in Asian Oral Cancer. Front. Genet. 2021, 12, 643461. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Fu, J.; Zeng, Z.; Cohen, D.; Li, J.; Chen, Q.; Li, B.; Liu, X.S. TIMER2.0 for analysis of tumor-infiltrating immune cells. Nucleic Acids Res. 2020, 48, W509–W514. [Google Scholar] [CrossRef]
- Fjeldbo, C.S.; Hompland, T.; Hillestad, T.; Aarnes, E.K.; Gunther, C.C.; Kristensen, G.B.; Malinen, E.; Lyng, H. Combining imaging- and gene-based hypoxia biomarkers in cervical cancer improves prediction of chemoradiotherapy failure independent of intratumour heterogeneity. EBioMedicine 2020, 57, 102841. [Google Scholar] [CrossRef]
- Gao, J.; Song, P. Combination of triple biomarkers AFP, AFP-L3, and PIVAKII for early detection of hepatocellular carcinoma in China: Expectation. Drug Discov. Ther. 2017, 11, 168–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.H.; Liu, Y.; Zhang, W.; Liu, C.; He, J.J.; Tang, X.J. Associations between clinical-pathological parameters and biomarkers, HER-2, TYMS, RRMI, and 21-gene recurrence score in breast cancer. Pathol. Res. Pract. 2019, 215, 152644. [Google Scholar] [CrossRef] [PubMed]
- Caponio, V.C.A.; Troiano, G.; Togni, L.; Zhurakivska, K.; Santarelli, A.; Laino, L.; Rubini, C.; Lo Muzio, L.; Mascitti, M. Pattern and localization of perineural invasion predict poor survival in oral tongue carcinoma. Oral Dis. 2021. [Google Scholar] [CrossRef]
- Kim, D.W.; Lee, S.; Kwon, S.; Nam, W.; Cha, I.H.; Kim, H.J. Deep learning-based survival prediction of oral cancer patients. Sci. Rep. 2019, 9, 6994. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, J.G.; Yu, J.W.; Wu, H.B.; Zheng, L.H.; Ni, X.C.; Li, X.Q.; Du, G.Y.; Jiang, B.J. Expressions and clinical significances of c-MET, p-MET and E2f-1 in human gastric carcinoma. BMC Res. Notes 2014, 7, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, J.; Gong, J.; Li, X.; Hu, Z.; Xu, Y.; Shi, H.; Li, D.; Liu, G.; Jie, Y.; Hu, B.; et al. Unsupervised Hierarchical Clustering Identifies Immune Gene Subtypes in Gastric Cancer. Front. Pharmacol. 2021, 12, 692454. [Google Scholar] [CrossRef] [PubMed]
- Opinto, G.; Silvestris, N.; Centonze, M.; Graziano, G.; Pinto, R.; Fucci, L.; Simone, G.; Mangia, A. Hierarchical clustering analysis identifies metastatic colorectal cancers patients with more aggressive phenotype. Oncotarget 2017, 8, 87782–87794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jonckheere, N.; Auwercx, J.; Hadj Bachir, E.; Coppin, L.; Boukrout, N.; Vincent, A.; Neve, B.; Gautier, M.; Trevino, V.; Van Seuningen, I. Unsupervised Hierarchical Clustering of Pancreatic Adenocarcinoma Dataset from TCGA Defines a Mucin Expression Profile that Impacts Overall Survival. Cancers 2020, 12, 3309. [Google Scholar] [CrossRef]
- de Carcer, G. The Mitotic Cancer Target Polo-Like Kinase 1: Oncogene or Tumor Suppressor? Genes 2019, 10, 208. [Google Scholar] [CrossRef] [Green Version]
- Goan, Y.-G.; Liu, P.-F.; Chang, H.-W.; Chen, H.-C.; Chen, W.-C.; Kuo, S.-M.; Lee, C.-H.; Shu, C.-W. Kinome-wide screening with small interfering RNA identified polo-like Kinase 1 as a key regulator of proliferation in oral cancer cells. Cancers 2019, 11, 1117. [Google Scholar] [CrossRef] [Green Version]
- Basnet, R.; Gong, G.Q.; Li, C.; Wang, M.-W. Serum and glucocorticoid inducible protein kinases (SGKs): A potential target for cancer intervention. Acta Pharm. Sin. B 2018, 8, 767–771. [Google Scholar] [CrossRef]
- Ranzuglia, V.; Lorenzon, I.; Pellarin, I.; Sonego, M.; Dall’Acqua, A.; D’Andrea, S.; Lovisa, S.; Segatto, I.; Coan, M.; Polesel, J.; et al. Serum-and glucocorticoid-inducible kinase 2, SGK2, is a novel autophagy regulator and modulates platinum drugs response in cancer cells. Oncogene 2020, 39, 6370–6386. [Google Scholar] [CrossRef]
- Pacini, S.; Pellegrini, M.; Migliaccio, E.; Patrussi, L.; Ulivieri, C.; Ventura, A.; Carraro, F.; Naldini, A.; Lanfrancone, L.; Pelicci, P.; et al. p66SHC promotes apoptosis and antagonizes mitogenic signaling in T cells. Mol. Cell Biol. 2004, 24, 1747–1757. [Google Scholar] [CrossRef] [Green Version]
- Miller, D.R.; Ingersoll, M.A.; Chatterjee, A.; Baker, B.; Shrishrimal, S.; Kosmacek, E.A.; Zhu, Y.; Cheng, P.W.; Oberley-Deegan, R.E.; Lin, M.F. p66Shc protein through a redox mechanism enhances the progression of prostate cancer cells towards castration-resistance. Free Radic. Biol. Med. 2019, 139, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Luan, X.; Zha, J.; Li, Z.; Wu, L.; Yan, Y.; Wang, H.; Hou, D.; Huang, L.; Huang, F.; et al. TNF-alpha inhibits the migration of oral squamous cancer cells mediated by miR-765-EMP3-p66Shc axis. Cell Signal. 2017, 34, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Sun, Z.; Liu, Q.; Ye, D.; Ye, K.; Yang, Z.; Li, D. Role of c-Met in the progression of human oral squamous cell carcinoma and its potential as a therapeutic target. Oncol. Rep. 2018, 39, 209–216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaffer, S.; Bleiweiss, I.J. Beyond hematoxylin and eosin--the role of immunohistochemistry in surgical pathology. Cancer Investig. 2004, 22, 445–465. [Google Scholar] [CrossRef] [PubMed]
- Werner, M.; Chott, A.; Fabiano, A.; Battifora, H. Effect of formalin tissue fixation and processing on immunohistochemistry. Am. J. Surg. Pathol. 2000, 24, 1016–1019. [Google Scholar] [CrossRef]
- Yaziji, H.; Barry, T. Diagnostic Immunohistochemistry: What can go wrong? Adv. Anat. Pathol. 2006, 13, 238–246. [Google Scholar] [CrossRef]
- Hewitt, S.M. Tissue microarrays as a tool in the discovery and validation of predictive biomarkers. Methods Mol. Biol. 2012, 823, 201–214. [Google Scholar] [CrossRef]
- Visser, N.C.M.; van der Wurff, A.A.M.; Pijnenborg, J.M.A.; Massuger, L.; Bulten, J.; Nagtegaal, I.D. Tissue microarray is suitable for scientific biomarkers studies in endometrial cancer. Virchows Arch. 2018, 472, 407–413. [Google Scholar] [CrossRef] [Green Version]
- Nolte, S.; Zlobec, I.; Lugli, A.; Hohenberger, W.; Croner, R.; Merkel, S.; Hartmann, A.; Geppert, C.I.; Rau, T.T. Construction and analysis of tissue microarrays in the era of digital pathology: A pilot study targeting CDX1 and CDX2 in a colon cancer cohort of 612 patients. J. Pathol. Clin. Res. 2017, 3, 58–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Protein Name | Associated Protein Name | Clonality | Source | Catalogue Number | Dilution | Retrieval Buffer |
|---|---|---|---|---|---|---|
| CDH3 | Cadherin 3 | R | Abgent | AP1499B | 1:50 | T-EDTA |
| CDK6 | Cell division protein kinase 6 | R | Abcam Ltd. | ab124821 | 1:100 | T-EDTA |
| CSNK1E | Casein Kinase 1 Epsilon | R | Abgent | AP7403a | 1:50 | T-EDTA |
| EGFR | Epidermal Growth Factor Receptor | R | Zeta Corporation | Z2037 | 1:50 | T-EDTA |
| FEN1 | Flap Structure-Specific Endonuclease 1 | R | Abcam Ltd. | ab70815 | 1:1000 | T-EDTA |
| FLNA | Filamin A | R | Abgent | AP7770a | 1:50 | T-EDTA |
| KRAS | KRAS Proto-Oncogene, GTPase Kirsten rat sarcoma virus protein | R | Abcam Ltd. | ab216890 | 1:200 | C |
| MET a | Mesenchymal epithelial transition factor | R | Abgent | AP3167a | 1:50 | C |
| P16 | p16 (INK4a) tumor suppressor protein | M | BD biosciences | 550834 | 1:100 | T-EDTA |
| PIM1 | Pim-1 Proto-Oncogene, Serine/Threonine Kinase | R | Abgent | AP7932d | 1:50 | T-EDTA |
| PLK1 | Polo-like Kinase 1 | R | Abgent | AP7937a | 1:100 | C |
| POLB | DNA Polymerase Beta | R | Abgent | AP50642 | 1:100 | T-EDTA |
| RB1 | Retinoblastoma 1 | M | Leica Biosystems | NCL-L-RB-358 | 1:50 | T-EDTA |
| SGK2 | Serum/Glucocorticoid Regulated Kinase 2 | R | Abgent | AP7947b | 1:100 | C |
| SHC1 | Src homology 2 domain containing transforming protein 1 | R | Abgent | AP50024 | 1:100 | C |
| STK17A | Serine/threonine-protein kinase 17A | R | Abcam Ltd. | ab97530 | 1:100 | C |
| Characteristics | Progression-Free | Disease-Progressed | p-Value |
|---|---|---|---|
| Cases | 66 | 36 | |
| Age | 0.163 | ||
| <50 years | 25 (37.9%) | 8 (22.2%) | |
| ≧50 years | 41 (62.1%) | 28 (77.8%) | |
| Sex | 1.000 | ||
| Female | 4 (6.1%) | 2 (5.6%) | |
| Male | 62 (93.9%) | 34 (94.4%) | |
| Risk behaviors a | 59 (89.4%) | 33 (91.7%) | 0.984 |
| Site | 0.577 | ||
| Non-buccal | 29 (43.9%) | 13 (36.1%) | |
| Buccal | 37 (56.1%) | 23 (63.9%) | |
| Grade | 0.116 | ||
| 1 | 35 (53.0%) | 13 (36.1%) | |
| 2 | 29 (43.9%) | 23 (63.9%) | |
| 3 | 2 (3.0%) | - | |
| LVI | 5 (7.6%) | 5 (13.9%) | 0.318 |
| PNI | 6 (9.1%) | 7 (19.4%) | 0.212 |
| Margin not free | 3 (4.5%) | 3 (8.3%) | 0.663 |
| ENE | 4 (6.1%) | 5 (13.9%) | 0.273 |
| Tumor stage | 0.055 | ||
| I | 32 (48.5%) | 16 (44.4%) | |
| II | 21 (31.8%) | 6 (16.7%) | |
| III | 5 (7.6%) | 2 (5.6%) | |
| IV | 8 (12.1%) | 12 (33.3%) | |
| Lymph node invasion | 0.878 | ||
| Negative | 50 (75.8%) | 26 (72.2%) | |
| Positive | 16 (24.2%) | 10 (27.8%) | |
| Pathological stage | 0.200 | ||
| I-II | 43 (65.2%) | 18 (50.0%) | |
| III-IV | 23 (34.8%) | 18 (50.0%) | |
| Death | 7 (10.6%) | 19 (52.8%) | 0.001 |
| Protein Clusters | High-Risk | n (%) | Low-Risk | n (%) | p-Value |
|---|---|---|---|---|---|
| 1-factor | |||||
| p16 | 71 | 19 (73.1%) | 31 | 7 (26.9%) | 0.527 |
| STK17A | 77 | 21 (80.8%) | 25 | 5 (19.2%) | 0.677 |
| PIM1 | 71 | 17 (65.4%) | 31 | 9 (34.6%) | 0.708 |
| 2-factor | |||||
| EGFR–CDH3 | 91 | 25 (96.2%) | 11 | 1 (3.8%) | 0.151 |
| KRAS–FLNA | 19 | 19 (73.1%) | 83 | 7 (26.9%) | 0.205 |
| POLB–FEN1 | 66 | 18 (69.2%) | 36 | 8 (30.8%) | 0.279 |
| 3-factor | |||||
| RB1–CDK6–CNSK1E | 73 | 18 (69.2%) | 29 | 8 (30.8%) | 0.745 |
| 4-factor | |||||
| PLK1–PhosphoMet–SGK2–SHC1 | 52 | 16 (61.5%) | 50 | 10 (38.5%) | 0.023 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.-C.; Chan, L.-P.; Wu, C.-C.; Hsiao, H.-H.; Liu, Y.-C.; Cho, S.-F.; Du, J.-S.; Liu, T.-C.; Yang, C.-H.; Pan, M.-R.; et al. Progression Risk Score Estimation Based on Immunostaining Data in Oral Cancer Using Unsupervised Hierarchical Clustering Analysis: A Retrospective Study in Taiwan. J. Pers. Med. 2021, 11, 908. https://doi.org/10.3390/jpm11090908
Wang H-C, Chan L-P, Wu C-C, Hsiao H-H, Liu Y-C, Cho S-F, Du J-S, Liu T-C, Yang C-H, Pan M-R, et al. Progression Risk Score Estimation Based on Immunostaining Data in Oral Cancer Using Unsupervised Hierarchical Clustering Analysis: A Retrospective Study in Taiwan. Journal of Personalized Medicine. 2021; 11(9):908. https://doi.org/10.3390/jpm11090908
Chicago/Turabian StyleWang, Hui-Ching, Leong-Perng Chan, Chun-Chieh Wu, Hui-Hua Hsiao, Yi-Chang Liu, Shih-Feng Cho, Jeng-Shiun Du, Ta-Chih Liu, Cheng-Hong Yang, Mei-Ren Pan, and et al. 2021. "Progression Risk Score Estimation Based on Immunostaining Data in Oral Cancer Using Unsupervised Hierarchical Clustering Analysis: A Retrospective Study in Taiwan" Journal of Personalized Medicine 11, no. 9: 908. https://doi.org/10.3390/jpm11090908