
Usefulness of Magnetic Mallet in Oral Surgery and Implantology: A Systematic Review

 , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. PICO Question
2.2. Search Strategy
2.3. Inclusion and Exclusion Criteria
2.4. Selection of the Studies
2.5. Data Extraction
2.6. Data Analysis
3. Results
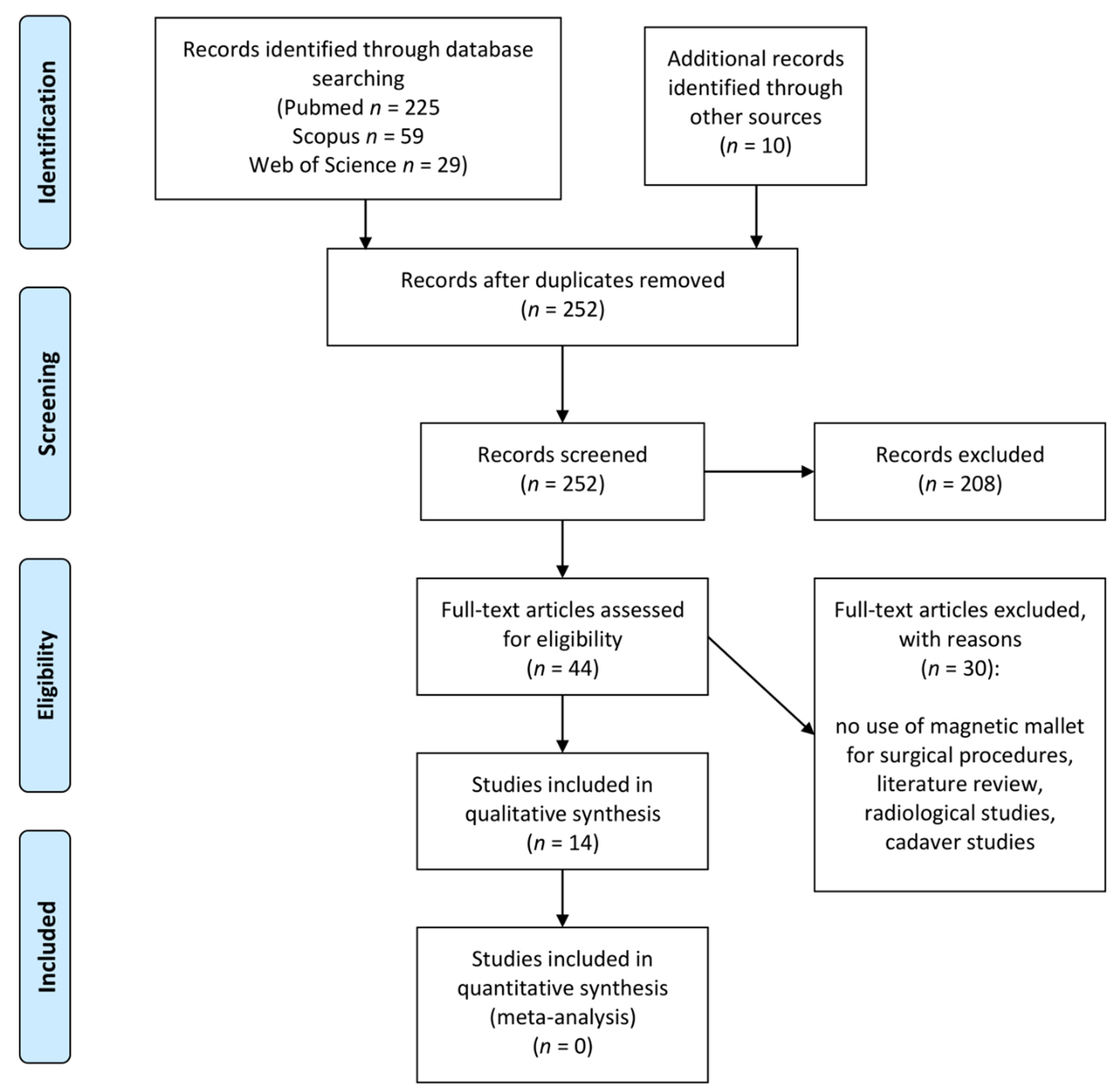
3.1. Study Selection
3.2. Magnetic Mallet in Teeth Extraction
3.3. Magnetic Mallet in Implant Surgery
4. Discussion
4.1. Magnetic Mallet in Teeth Extraction
4.2. Magnetic Mallet in Implant Surgery
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hong, B.; Bulsara, Y.; Gorecki, P.; Dietrich, T. Minimally invasive vertical versus conventional tooth extraction: An interrupted time series study. J. Am. Dent. Assoc. 2018, 149, 688–695. [Google Scholar] [CrossRef] [Green Version]
- Kalk, W.; De Baat, C. Some factors connected with alveolar bone resorption. J. Dent. 1989, 17, 162–165. [Google Scholar] [CrossRef]
- Schmidlin, P.R.; Jung, R.E.; Schug, J. Prevention of alveolar ridge resorption after tooth extraction—A review. Schweiz. Mon. Zahnmed. 2004, 114, 328–336. [Google Scholar]
- Hansson, S.; Halldin, A. Alveolar ridge resorption after tooth extraction: A consequence of a fundamental principle of bone physiology. J. Dent. Biomech. 2012, 3, 1758736012456543. [Google Scholar] [CrossRef]
- Samiksha, G.; Saumyendra, V.S.; Deeksha, A. Residual ridge resorption—A review of etiology. Polymorphism 2019, 2, 107–113. [Google Scholar]
- Atieh, M.A.; Alsabeeha, N.H.M.; Tawse-Smith, A.; Duncan, W.J. Piezoelectric versus conventional implant site preparation: A systematic review and meta-analysis. Clin. Implant. Dent. Relat. Res. 2018, 20, 261–270. [Google Scholar] [CrossRef] [PubMed]
- Saund, D.; Dietrich, T. Minimally-invasive tooth extraction: Doorknobs and strings revisited! Dent. Update 2013, 40, 325–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Attanasio, F.; Antonelli, A.; Brancaccio, Y.; Averta, F.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Primary Stability of Three Different Osteotomy Techniques in Medullary Bone: An in Vitro Study. Dent. J. 2020, 8, 21. [Google Scholar] [CrossRef] [Green Version]
- Giudice, A.; Bennardo, F.; Antonelli, A.; Barone, S.; Wagner, F.; Fortunato, L.; Traxler, H. Influence of clinician’s skill on primary implant stability with conventional and piezoelectric preparation techniques: An ex-vivo study. J. Biol. Regul. Homeost. Agents 2020, 34, 739–745. [Google Scholar] [PubMed]
- Antonelli, A.; Bennardo, F.; Brancaccio, Y.; Barone, S.; Femiano, F.; Nucci, L.; Minervini, G.; Fortunato, L.; Attanasio, F.; Giudice, A. Can Bone Compaction Improve Primary Implant Stability? An In Vitro Comparative Study with Osseodensification Technique. Appl. Sci. 2020, 10, 8623. [Google Scholar] [CrossRef]
- Vercellotti, T.; Troiano, G.; Oreglia, F.; Lombardi, T.; Gregorig, G.; Morella, E.; Rapani, A.; Stacchi, C. Wedge-Shaped Implants for Minimally Invasive Treatment of Narrow Ridges: A Multicenter Prospective Cohort Study. J. Clin. Med. 2020, 9, 3301. [Google Scholar] [CrossRef] [PubMed]
- Palacios, J.A.V.; Garcia, J.J.; Caramês, J.M.M.; Quirynen, M.; da Silva Marques, D.N. Short implants versus bone grafting and standard-length implants placement: A systematic review. Clin. Oral Investig. 2018, 22, 69–80. [Google Scholar] [CrossRef] [PubMed]
- Mokcheh, A.; Jegham, H.; Turki, S. Short implants as an alternative to sinus lift for the rehabilitation of posterior maxillary atrophies: Systematic review and meta-analysis. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Ergina, P.L.; Cook, J.; Blazeby, J.; Boutron, I.; Clavien, P.-A.; Reeves, B.C.; Seiler, C.M. Challenges in evaluating surgical innovation. Lancet 2009, 374, 1097–1104. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://collection.sciencemuseumgroup.org.uk/objects/co100246/bonwill-electromagnetic-mallet-automatic-mallets (accessed on 13 December 2021).
- Visale, K.; Manimala, V.; Vidhyasankari, N.; Shanmugapriya, S.V. Magnetic mallets—A stroke of luck in implantology: A review. J. Acad. Dent. Educ. 2021, 7, 6–9. [Google Scholar] [CrossRef]
- Desai, A.; Patil, S.; Mitra, D.; Shah, R. Magnetic Mallet-Feel the Future. JIDA J. Indian Dent. Assoc. 2020, 14, 26–30. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gherlone, E. Sinus floor elevation by osteotome: Hand mallet versus electric mallet. A prospective clinical study. Int. J. Oral Maxillofac. Implant. 2012, 27, 1144–1150. [Google Scholar]
- Crespi, R.; Capparè, P.; Gherlone, E. A comparison of manual and electrical mallet in maxillary bone condensing for immediately loaded implants: A randomized study. Clin. Implant. Dent. Relat. Res. 2014, 16, 374–382. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gherlone, E.F. Electrical mallet in implants placed in fresh extraction sockets with simultaneous osteotome sinus floor elevation. Int. J. Oral Maxillofac. Implant. 2013, 28, 869–874. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gherlone, E. Electrical Mallet Provides Essential Advantages in Maxillary Bone Condensing. A Prospective Clinical Study. Clin. Implant. Dent. Relat. Res. 2012, 15, 874–882. [Google Scholar] [CrossRef]
- Crespi, R.; Capparé, P.; Gherlone, E. Electrical mallet provides essential advantages in split-crest and immediate implant placement. Oral Maxillofac. Surg. 2013, 18, 59–64. [Google Scholar] [CrossRef]
- Crespi, R.; Bruschi, G.B.; Capparé, P.; Gherlone, E. The utility of the electric mallet. J. Craniofac. Surg. 2014, 25, 793–795. [Google Scholar] [CrossRef]
- Crespi, R.; Bruschi, G.B.; Gastaldi, G.; Capparé, P.; Gherlone, E.F. Immediate Loaded Implants in Split-Crest Procedure. Clin. Implant. Dent. Relat. Res. 2015, 17 (Suppl. 2), e692–e698. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Crespi, G.; Gastaldi, G.; Gherlone, E.F. Delayed Implants Outcome in Maxillary Molar Region. Clin. Implant. Dent. Relat. Res. 2016, 19, 261–267. [Google Scholar] [CrossRef]
- Crespi, R.; Capparé, P.; Crespi, G.; Gastaldi, G.; Gherlone, E. Bone-Level Changes Around Delayed Dental Implants in Previous Large Bone Defects Filled with Reactive Soft Tissue After Extraction: A Cone Beam Computed Tomography Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 1429–1434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crespi, R.; Capparé, P.; Crespi, G.; Gastaldi, G.; Gherlone, E.F. Dimensional Changes of Fresh Sockets with Reactive Soft Tissue Preservation: A Cone Beam CT Study. Implant. Dent. 2017, 26, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Menchini-Fabris, G.B.; Toti, P.; Crespi, G.; Covani, U.; Furlotti, L.; Crespi, R. Effect of Different Timings of Implant Insertion on the Bone Remodeling Volume around Patients’ Maxillary Single Implants: A 2–3 Years Follow-Up. Int. J. Env. Res. Public Health 2020, 17, 6790. [Google Scholar] [CrossRef] [PubMed]
- Menchini-Fabris, G.B.; Toti, P.; Crespi, G.; Covani, U.; Crespi, R. Distal Displacement of Maxillary Sinus Anterior Wall Versus Conventional Sinus Lift with Lateral Access: A 3-Year Retrospective Computerized Tomography Study. Int. J. Environ. Res. Public Health 2020, 17, 7199. [Google Scholar] [CrossRef]
- Crespi, R.; Toti, P.; Covani, U.; Crespi, G.; Menchini-Fabris, G.-B. Clinical and Radiographic Evaluation of Modified Transalveolar Two-Step Osteotome-Mediated Localized Maxillary Sinus Elevation: A Retrospective Computed Tomography Study with a 3-Year Follow-up. Int. J. Oral Maxillofac. Implant. 2021, 36, 553–560. [Google Scholar] [CrossRef]
- Bruschi, G.B.; Bruschi, E.; Papetti, L. Flapless Localised Management of Sinus Floor (LMSF) for trans-crestal sinus floor augmentation and simultaneous implant placement. A retrospective non-randomized study: 5-year of follow-up. Heliyon 2021, 7, e07927. [Google Scholar] [CrossRef]
- Barone, S.; Antonelli, A.; Averta, F.; Diodati, F.; Muraca, D.; Bennardo, F.; Giudice, A. Does Mandibular Gonial Angle Influence the Eruption Pattern of the Lower Third Molar? A Three-Dimensional Study. J. Clin. Med. 2021, 10, 4057. [Google Scholar] [CrossRef]
- Bakkar, M.; Liu, Y.; Fang, D.; Stegen, C.; Su, X.; Ramamoorthi, M.; Lin, L.-C.; Kawasaki, T.; Makhoul, N.; Pham, H.; et al. A Simplified and Systematic Method to Isolate, Culture, and Characterize Multiple Types of Human Dental Stem Cells from a Single Tooth. Methods Mol. Biol. 2017, 1553, 191–207. [Google Scholar] [PubMed]
- Di Vito, A.; Giudice, A.; Chiarella, E.; Malara, N.; Bennardo, F.; Fortunato, L. In Vitro Long-Term Expansion and High Osteogenic Potential of Periodontal Ligament Stem Cells: More Than a Mirage. Cell Transpl. 2019, 28, 129–139. [Google Scholar] [CrossRef] [Green Version]
- Jason, W.; Dan, H.; Nicholas, T. Powertome® Assisted Atraumatic Tooth Extraction. J. Implant. Adv. Clin. Dent. 2009, 1, 35–44. [Google Scholar]
- Available online: https://www.osseotouch.com/en/products/easyroot/ (accessed on 13 December 2021).
- Giudice, A.; Bennardo, F.; Antonelli, A.; Barone, S.; Fortunato, L. COVID-19 is a New Challenge for Dental Practitioners: Advice on Patients’ Management from Prevention of Cross Infections to Telemedicine. Open Dent. J. 2020, 14, 298–304. [Google Scholar] [CrossRef]
- Giudice, A.; Antonelli, A.; Bennardo, F. To test or not to test? An opportunity to restart dentistry sustainably in the ‘COVID-19 era’. Int. Endod. J. 2020, 53, 1020–1021. [Google Scholar] [CrossRef] [PubMed]
- Bennardo, F.; Antonelli, A.; Barone, S.; Figliuzzi, M.M.; Fortunato, L.; Giudice, A. Change of Outpatient Oral Surgery during the COVID-19 Pandemic: Experience of an Italian Center. Int. J. Dent. 2020, 2020, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Chien, A.T.; Stehle, N.E.; Karian, B.K. The Use of Chisels in the Extraction of Mandibular Third Molars: A Technique That May Prevent the Aerosolization of Severe Acute Respiratory Syndrome Coronavirus 2. J. Oral Maxillofac. Surg. 2021, 79, 1199–1206. [Google Scholar] [CrossRef]
- Hong, J.-Y.; Shin, E.-Y.; Herr, Y.; Chung, J.-H.; Lim, H.-C.; Shin, S.-I. Implant survival and risk factor analysis in regenerated bone: Results from a 5-year retrospective study. J. Periodontal Implant. Sci. 2020, 50, 379–391. [Google Scholar] [CrossRef]
- Cha, J.K.; Kim, C.; Pae, H.C.; Lee, J.S.; Jung, U.W.; Choi, S.H. Maxillary sinus augmentation using biphasic calcium phosphate: Dimensional stability results after 3–6 years. J. Periodontal Implant. Sci. 2019, 49, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Toti, P.; Barone, A.; Marconcini, S.; Fabris, G.B.M.; Martuscelli, R.; Covani, U. Pose determination of a blade implant in three dimensions from a single two-dimensional radiograph. Dentomaxillofacial Radiol. 2018, 47, 20170258. [Google Scholar] [CrossRef] [PubMed]
- Feher, B.; Frommlet, F.; Gruber, R.; Hirtler, L.; Ulm, C.; Kuchler, U. Resonance frequency analysis of implants placed in condensed bone. Clin. Oral Implant. Res. 2021, 32, 1200–1208. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Reference | Type of Intervention | Study Design | Number of Patients Treated | Number of Sites (Implants/Teeth) Treated | Follow-Up | Outcomes | Complications |
|---|---|---|---|---|---|---|---|
| Crespi et al., 2012 A [19] | Sinus lift | Prospective | 40 MM 40 CTR | 60 MM 60 CTR | 6, 12, 24 m | Survival rate of 98.33% (both groups) | 2 BPPV in CTR group |
| Crespi et al., 2012 B [20] | Implant site preparation | Prospective | 25 MM 25 CTR | 69 MM 69 CTR | 6, 12, 24 m | Survival rate of 97.1% (MM) and 92.75% (CTR) | 2 BPPV in CTR group |
| Crespi et al., 2013 A [21] | Sinus lift | Prospective | 32 | 70 | 2, 4, 12, 24 m | Survival rate of 98.57% | - |
| Crespi et al., 2013 B [22] | Implant site preparation | Prospective | 18 MM 18 CTR | 25 MM 25 CTR | 6, 12, 24 m | Survival rate of 96% (both groups) | 2 BPPV in CTR group |
| Crespi et al., 2014 A [23] | Ridge expansion | Prospective | 23 MM 23 CTR | 59 MM 59 CTR | 6, 12, 24 m | Survival rate of 100% (MM) and 96.61% (CTR) | 1 BPPV in CTR group |
| Crespi et al., 2014 B [24] | Dental extraction | Retrospective | 156 | 427 | - | No fracture or loss of cortical bone plate | - |
| Crespi et al., 2015 [25] | Ridge expansion | Retrospective | 36 | 93 | 6, 12, 24 m | Survival rate of 98.92% | - |
| Crespi et al., 2016 A [26] | Implant site preparation | Prospective | 40 | 40 | 36 m | Survival rate of 100% | - |
| Crespi et al., 2016 B [27] | Implant site preparation | Prospective | 57 | 84 | 36 m | Survival rate of 100% | - |
| Crespi et al., 2017 [28] * | Dental extraction | Prospective | 53 | 145 | 3 m | No signs of inflamed tissue or exposed bone | - |
| Menchini-Fabris GB, et al. 2020 A [29] * | Dental extraction | Retrospective | 47 | 47 | 24–36 m | No postoperative complications | - |
| Menchini-Fabris GB, et al. 2020 B [30] | Sinus lift | Observational | 29 MM 27 CTR | 29 MM 27 CTR | 36 m | Survival rate of 100% (MM) and 92.6% (CTR) | - |
| Crespi et al. 2021 [31] | Sinus lift | Retrospective | 40 | 40 | 36 m | Survival rate 100% | - |
| Bruschi et al. 2021 [32] | Sinus lift | Retrospective | 52 | 71 | 9–66 m (mean 29.8 m) | Survival rate 98.6% | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bennardo, F.; Barone, S.; Vocaturo, C.; Nucci, L.; Antonelli, A.; Giudice, A. Usefulness of Magnetic Mallet in Oral Surgery and Implantology: A Systematic Review. J. Pers. Med. 2022, 12, 108. https://doi.org/10.3390/jpm12010108
Bennardo F, Barone S, Vocaturo C, Nucci L, Antonelli A, Giudice A. Usefulness of Magnetic Mallet in Oral Surgery and Implantology: A Systematic Review. Journal of Personalized Medicine. 2022; 12(1):108. https://doi.org/10.3390/jpm12010108
Chicago/Turabian StyleBennardo, Francesco, Selene Barone, Camillo Vocaturo, Ludovica Nucci, Alessandro Antonelli, and Amerigo Giudice. 2022. "Usefulness of Magnetic Mallet in Oral Surgery and Implantology: A Systematic Review" Journal of Personalized Medicine 12, no. 1: 108. https://doi.org/10.3390/jpm12010108
APA StyleBennardo, F., Barone, S., Vocaturo, C., Nucci, L., Antonelli, A., & Giudice, A. (2022). Usefulness of Magnetic Mallet in Oral Surgery and Implantology: A Systematic Review. Journal of Personalized Medicine, 12(1), 108. https://doi.org/10.3390/jpm12010108