
Plasma Levels of Mid-Regional Proadrenomedullin Accurately Identify H1N1pdm09 Influenza Virus Patients with Risk of Intensive Care Admission and Mortality in the Emergency Department

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
References
- Morens, D.M.; Taubenberger, J.K.; Harvey, H.A.; Memoli, M.J. The 1918 influenza pandemic: Lessons for 2009 and the future. Crit. Care Med. 2010, 38, e10–e20. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Pop-Vicas, A. Clinical review: Primary influenza viral pneumonia. Crit. Care 2009, 13, 235. [Google Scholar] [CrossRef]
- Rello, J.; Rodríguez, A.; Ibañez, P.; Socias, L.; Cebrian, J.; Marques, A.; Guerrero, J.; Ruiz-Santana, S.; Marquez, E.; Del Nogal-Saez, F.; et al. Intensive care adult patients with severe respiratory failure caused by Influenza A (H1N1)v in Spain. Crit. Care 2009, 13, R148. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, N.; Woodhead, M. Predicting the unpredictable: Is it possible clinically to separate H1N1 from non-H1N1 community-acquired pneumonia? Thorax 2011, 66, 187–188. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ruuskanen, O.; Lahti, E.; Jennings, L.C.; Murdoch, D.R. Viral pneumonia. Lancet 2011, 377, 1264–1275. [Google Scholar] [CrossRef]
- Shahpori, R.; Stelfox, H.T.; Doig, C.J.; Boiteau, P.J.E.; Zygun, D.A. Sequential Organ Failure Assessment in H1N1 pandemic planning. Crit. Care Med. 2011, 39, 827–832. [Google Scholar] [CrossRef]
- Pereira, J.M.; Moreno, R.P.; Matos, R.; Rhodes, A.; Martin-Loeches, I.; Cecconi, M.; Lisboa, T.; Rello, J. Severity assessment tools in ICU patients with 2009 Influenza A (H1N1) pneumonia. Clin. Microbiol. Infect. 2012, 18, 1040–1048. [Google Scholar] [CrossRef]
- Minne, L.; Abu-Hanna, A.; De Jonge, E. Evaluation of SOFA-based models for predicting mortality in the ICU: A systematic review. Crit. Care 2009, 12, R161. [Google Scholar] [CrossRef]
- Méndez, R.; Aldás, I.; Menéndez, R. Biomarkers in Community-Acquired Pneumonia (Cardiac and Non-Cardiac). J. Clin. Med. 2020, 9, 549. [Google Scholar] [CrossRef] [PubMed]
- Ingram, P.R.; Inglis, T.; Moxon, D.; Speers, D. Procalcitonin and C-reactive protein in severe 2009 H1N1 influenza infection. Intensive Care Med. 2010, 36, 528–532. [Google Scholar] [CrossRef] [PubMed]
- Lachmann, G.; Knaak, C.; Vorderwülbecke, G.; La Rosée, P.; Balzer, F.; Schenk, T.; Schuster, F.S.; Nyvlt, P.; Janka, G.; Brunkhorst, F.M.; et al. Hyperferritinemia in Critically Ill Patients. Crit. Care Med. 2020, 48, 459–465. [Google Scholar] [CrossRef]
- Eto, T. A review of the biological properties and clinical implications of adrenomedullin and proadrenomedullin N-terminal 20 peptide (PAMP), hypotensive and vasodilating peptides. Peptides 2001, 22, 1693–1711. [Google Scholar] [CrossRef]
- Valenzuela-Sánchez, F.; Valenzuela-Méndez, B.; Rodríguez-Gutiérrez, J.F.; Estella, A.; González-García, M. New role of biomarkers: Mid-regional pro-adrenomedullin, the biomarker of organ failure. Ann. Transl. Med. 2016, 4, 329. [Google Scholar] [CrossRef] [PubMed]
- Akpinar, S.; Rollas, K.; Alagoz, A.; Seğmen, F.; Sipit, T. Performance evaluation of MR-proadrenomedullin and other scoring systems in severe sepsis with pneumonia. J. Thorac. Dis. 2014, 6, 921–929. [Google Scholar] [CrossRef] [PubMed]
- Saeed, K.; Wilson, D.C.; Bloos, F.; Schuetz, P.; van der Does, Y.; Melander, O.; Hausfater, P.; Legramante, J.M.; Claessens, Y.-E.; Amin, D.; et al. The early identification of disease progression in patients with suspected infection presenting to the emergency department: A multi-centre derivation and validation study. Crit. Care 2019, 23, 255. [Google Scholar] [CrossRef]
- Gonzalez del Castillo, J.; Clemente-Callejo, C.; Llopis, F.; Irimia, A.; Oltra-Hostalet, F.; Rechner, C.; Schwabe, A.; Fernandez-Rodriguez, V.; Sánchez-Mora, C.; Giol-Amich, J.; et al. Midregional proadrenomedullin safely reduces hospitalization in a low severity cohort with infections in the ED: A randomized controlled multi-centre interventional pilot study. Eur. J. Intern. Med. 2021, 88, 104–113. [Google Scholar] [CrossRef]
- Kalil, A.C.; Thomas, P.G. Influenza virus-related critical illness: Pathophysiology and epidemiology. Crit. Care 2019, 23, 258. [Google Scholar] [CrossRef]
- Benatti, M.N.; Fabro, A.T.; Miranda, C.H. Endothelial glycocalyx shedding in the acute respiratory distress syndrome after flu syndrome. J. Intensive Care 2020, 8, 72. [Google Scholar] [CrossRef]
- Salgado, D.R.; Ortiz, J.A.; Favory, R.; Creteur, J.; Vincent, J.-L.; De Backer, D. Microcirculatory abnormalities in patients with severe influenza A (H1N1) infection. Can. J. Anesth. 2010, 57, 940–946. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.M.; Fink, M.P.; Marshall, J.C.; Abraham, E.; Angus, D.; Cook, D.; Cohen, J.; Opal, S.M.; Vincent, J.-L.; Ramsay, G. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit. Care Med. 2003, 31, 1250–1256. [Google Scholar] [CrossRef] [PubMed]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M., Jr.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society Consensus Guidelines on the Management of Community-Acquired Pneumonia in Adults. Clin. Infect. Dis. 2007, 44, S27–S72. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Rodriguez, A.; Lisboa, T.; Gallego, M.; Lujan, M.; Wunderink, R. PIRO score for community-acquired pneumonia: A new prediction rule for assessment of severity in intensive care unit patients with community-acquired pneumonia. Crit. Care Med. 2009, 37, 456–462. [Google Scholar] [CrossRef]
- Caruhel, P.; Mazier, C.; Kunde, J.; Morgenthaler, N.G.; Darbouret, B. Homogeneous time-resolved fluoroimmunoassay for the measurement of midregionalproadrenomedullin in plasma on the fully automated system B.R.A.H.M.S KRYPTOR®. Clin. Biochem. 2009, 42, 725–728. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Carrasco, M.; Lagunes, L.; Antón, A.; Gattarello, S.; Laborda, C.; Pumarola, T.; Rello, J. Influenza infection in the intensive care unit: Four years after the 2009 pandemic. Enferm. Infecc. Microbiol. Clín. 2016, 34, 177–183. [Google Scholar] [CrossRef] [PubMed]
- Satterwhite, L.; Mehta, A.; Martin, G.S. Novel findings from the second wave of adult pH1N1 in the United States. Crit. Care Med. 2010, 38, 2059–2061. [Google Scholar] [CrossRef] [PubMed]
- Riera, M.; Payeras-Cifre, A.; A Marcos, M.; Viasus, D.; Farinas, M.C.; Segura, F.; Torre-Cisneros, J.; Martin-Quiros, A.; Rodríguez-Baño, J.; Vila, J.; et al. Clinical presentation and prognosis of the 2009 H1N1 influenza A infection in HIV-1-infected patients: A Spanish multicenter study. AIDS 2010, 24, 2461–2467. [Google Scholar] [CrossRef]
- Valenzuela-Sanchez, F.; Valenzuela-Mendez, B.; Rodriguez-Gutierrez, J.; Bohollo De Austria, R.; Rubio-Quiñones, J.; Puget-Martínez, L.; Valiente Alemán, I.; Angel Estella-García, A. Initial levels of mr-proadrenomedullin: A predictor of severity in patients with influenza a virus pneumonia. Intensive Care Med. Exp. 2015, 3, A832. [Google Scholar] [CrossRef]
- Valenzuela-Sánchez, F.; Valenzuela-Méndez, B.; Rodríguez-Gutiérrez, J.F.; Rello, J. Personalized medicine in severe influenza. Eur. J. Clin. Microbiol. Infect. Dis. 2016, 35, 893–897. [Google Scholar] [CrossRef]
- Andaluz-Ojeda, D.; Nguyen, H.B.; Meunier-Beillard, N.; Cicuéndez, R.; Quenot, J.-P.; Calvo, D.; Dargent, A.; Zarca, E.; Andrés, C.; Nogales, L.; et al. Superior accuracy of mid-regional proadrenomedullin for mortality prediction in sepsis with varying levels of illness severity. Ann. Intensive Care 2017, 7, 15. [Google Scholar] [CrossRef]
- Sega, F.V.D.; Fortini, F.; Spadaro, S.; Ronzoni, L.; Zucchetti, O.; Manfrini, M.; Mikus, E.; Fogagnolo, A.; Torsani, F.; Pavasini, R.; et al. Time course of endothelial dysfunction markers and mortality in COVID-19 patients: A pilot study. Clin. Transl. Med. 2021, 11, e283. [Google Scholar] [CrossRef]
- Nägele, M.P.; Haubner, B.; Tanner, F.C.; Ruschitzka, F.; Flammer, A.J. Endothelial dysfunction in COVID-19: Current findings and therapeutic implications. Atherosclerosis 2020, 314, 58–62. [Google Scholar] [CrossRef]
- Potere, N.; Valeriani, E.; Candeloro, M.; Tana, M.; Porreca, E.; Abbate, A.; Spoto, S.; Rutjes, A.W.S.; Di Nisio, M. Acute complications and mortality in hospitalized patients with coronavirus disease 2019: A systematic review and meta-analysis. Crit. Care 2020, 24, 389. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Rénia, L.; Macary, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Van Lier, D.; Kox, M.; Pickkers, P. Promotion of vascular integrity in sepsis through modulation of bioactive adrenomedullin and dipeptidyl peptidase. J. Intern. Med. 2020, 289, 792–806. [Google Scholar] [CrossRef]
- Gregoriano, C.; Koch, D.; Kutz, A.; Haubitz, S.; Conen, A.; Bernasconi, L.; Hammerer-Lercher, A.; Saeed, K.; Mueller, B.; Schuetz, P. The vasoactive peptide MR-pro-adrenomedullin in COVID-19 patients: An observational study. Clin. Chem. Lab. Med. 2021, 59, 995–1004. [Google Scholar] [CrossRef] [PubMed]
- De Guadiana-Romualdo, L.G.; Martínez, M.M.; Mulero, M.D.R.; Esteban-Torrella, P.; Olivo, M.H.; García, M.J.A.; Campos-Rodríguez, V.; Sancho-Rodríguez, N.; Martínez, M.G.; Alcaraz, A.; et al. Circulating MR-proADM levels, as an indicator of endothelial dysfunction, for early risk stratification of mid-term mortality in COVID-19 patients. Int. J. Infect. Dis. 2021, 111, 211–218. [Google Scholar] [CrossRef]
- Sasso, B.L.; Gambino, C.M.; Scichilone, N.; Giglio, R.V.; Bivona, G.; Scazzone, C.; Muratore, R.; Milano, S.; Barbagallo, M.; Agnello, L.; et al. Clinical Utility of MidregionalProadrenomedullin in Patients with COVID-19. Lab. Med. 2021, 52, 493–498. [Google Scholar] [CrossRef]
- Montrucchio, G.; Sales, G.; Rumbolo, F.; Palmesino, F.; Fanelli, V.; Urbino, R.; Filippini, C.; Mengozzi, G.; Brazzi, L. Effectiveness of mid-regional pro-adrenomedullin (MR-proADM) as prognostic marker in COVID-19 critically ill patients: An observational prospective study. PLoS ONE 2021, 16, e0246771. [Google Scholar] [CrossRef] [PubMed]
- Spoto, S.; Agrò, F.E.; Sambuco, F.; Travaglino, F.; Valeriani, E.; Fogolari, M.; Mangiacapra, F.; Costantino, S.; Ciccozzi, M.; Angeletti, S. High value of mid-regional proadrenomedullin in COVID-19: A marker of widespread endothelial damage, disease severity, and mortality. J. Med. Virol. 2020, 93, 2820–2827. [Google Scholar] [CrossRef] [PubMed]
- Roedl, K.; Jarczak, D.; Fischer, M.; Haddad, M.; Boenisch, O.; de Heer, G.; Burdelski, C.; Frings, D.; Sensen, B.; Karakas, M.; et al. MR-proAdrenomedullin as a predictor of renal replacement therapy in a cohort of critically ill patients with COVID-19. Biomarkers 2021, 26, 417–424. [Google Scholar] [CrossRef]
- Lippi, G.; Henry, B.M. Pooled analysis of mid-regional pro-adrenomedullin values in COVID-19 patients with critical illness. Intern. Emerg. Med. 2021, 16, 1723–1725. [Google Scholar] [CrossRef]
- Saeed, K.; Legramante, J.M.; Angeletti, S.; Curcio, F.; Miguens, I.; Poole, S.; Tascini, C.; Sozio, E.; Del Castillo, J.G. Mid-regional pro-adrenomedullin as a supplementary tool to clinical parameters in cases of suspicion of infection in the emergency department. Expert Rev. Mol. Diagn. 2021, 21, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Zaninotto, M.; Mion, M.M.; Marchioro, L.; Padoan, A.; Plebani, M. Endothelial dysfunction and Mid-Regional proAdrenomedullin: What role in SARS-CoV-2 infected Patients? Clin. Chim. Acta 2021, 523, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Vasileva, D.; Badawi, A. C-reactive protein as a biomarker of severe H1N1 influenza. Inflamm. Res. 2018, 68, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Cuquemelle, E.; Soulis, F.; Villers, D.; Roche-Campo, F.; Somohano, C.A.; Fartoukh, M.; Kouatchet, A.; Mourvillier, B.; Dellamonica, J.; Picard, W.; et al. Can procalcitonin help identify associated bacterial infection in patients with severe influenza pneumonia? A multicentre study. Intensive Care Med. 2011, 37, 796–800. [Google Scholar] [CrossRef]
- Pfister, R.; Kochanek, M.; Leygeber, T.; Brun-Buisson, C.; Cuquemelle, E.; Machado, M.B.P.; Piacentini, E.; E Hammond, N.; Ingram, P.R.; Michels, G. Procalcitonin for diagnosis of bacterial pneumonia in critically ill patients during 2009 H1N1 influenza pandemic: A prospective cohort study, systematic review and individual patient data meta-analysis. Crit. Care 2014, 18, R44. [Google Scholar] [CrossRef]
- Bobbio-Pallavicini, F.; Verde, G.; Spriano, P.; Losi, R.; Bosatra, M.G.; Braschi, A.; Iotti, G.A.; Chiaranda, M.; Villa, S. Body iron status in critically ill patients: Significance of serum ferritin. Intensive Care Med. 1989, 15, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Garcia, P.C.R.; Longhi, F.; Branco, R.G.; Piva, J.P.; Lacks, D.; Tasker, R. Ferritin levels in children with severe sepsis and septic shock. Acta Paediatr. 2007, 96, 1829–1831. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
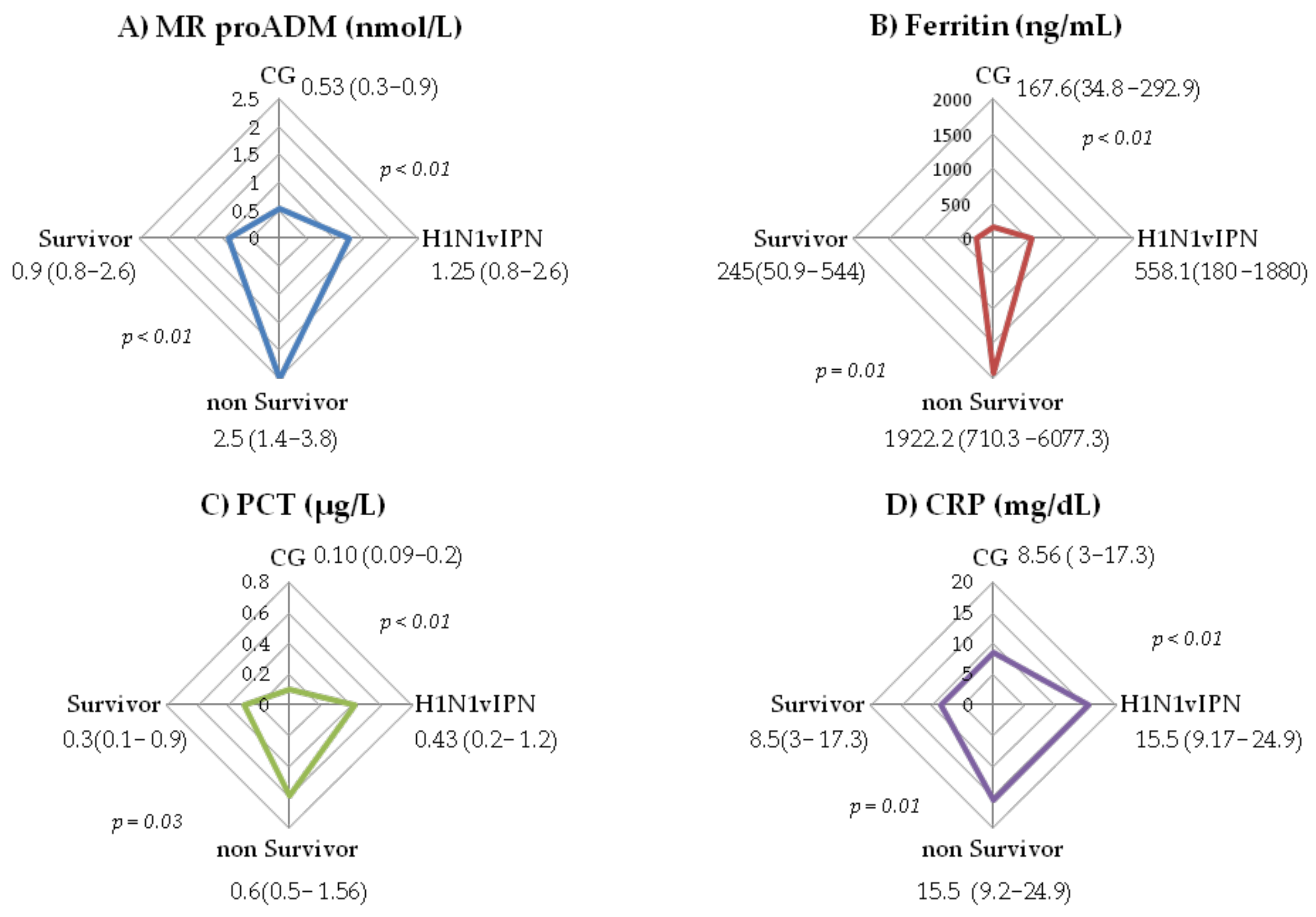
| Variable | H1N1vIPN n = 75 | H1N1vIPN Survivors; n = 53; (70.67%) | H1N1vIPN Non-Survivors; n = 22; (29.33%) |
|---|---|---|---|
| Age median (IQR) | 53 (44–64) | 52 (42.7–64) | 55 (47–70) |
| Men (%) | 49.3% | 49.1% | 50% |
| Women (%) | 50.7% | 50.9% | 50% * |
| BMI median (IQR) | 27 (23–32) | 27 (24–33.3) | 27 (23–30.3) |
| Obesity (BMI > 30) (%) | 31% | 33.3% | 26.3% |
| Smoker/COPD (%) | 32.4% | 34.6% | 27.3% |
| Diabetes Mellitus (%) | 21.3% | 20.8% | 22.7% |
| Immunosuppression (%) | 28% | 30.2% | 22.7% |
| Hematologic malignancy(%) | 6.6% | 5.6 % | 9% |
| Apache II median (IQR) | 17 (12–23) | 15 (12–21.7) | 21 (18–25) * |
| SAPS II median (IQR) | 45 (27–56) | 37 (27–51) | 53.5 (45–60) * |
| SOFA median (IQR) | 8 (8.5–10.7) | 6 (4–9) | 11 (8–12) * |
| Lactic acid (mmol/L) median (IQR) | 1.43 (0.98–1.8) | 6 (4–9) | 1.6 (1–2.5) |
| Stay in ICU median (IQR) | 13 (7–23) | 11 (7–23) | 14.5 (7–26) |
| Mechanical ventilation (%) | 85.3% | 75% | 100% * |
| days in MV median (IQR) | 7.5 (4–17) | 7 (3–16.2) | 12 (5.7–22.5) * |
| PaO2/FiO2 median (IQR) | 90 (60–146) | 107 (72–178) | 55 (46–90) * |
| Prone position (%) | 60.3% | 48.7% | 84.2% * |
| Recruitment maneuvers (%) | 27.6% | 20.5% | 42.1% |
| Septic shock (%) | 56% | 45.3% | 81.8% * |
| Corticosteroids (%) | 33.3% | 45.3% | 31.8% |
| Diuretics (%) | 34.5% | 33.3% | 36.8% |
| Continuous renal replacement therapy (CRRT) (%) | 10.7% | 5.7% | 22.7% * |
| Coinfection and Superinfection in Patients with Influenza A H1N1 Admitted to the ICU | |||
|---|---|---|---|
| COINFECTION | SUPERINFECTION | ||
| MICROORGANISMS | n. isolated cases | MICROORGANISMS | n. isolated cases |
| Streptococcus pneumoniae | 6 | Krebsiella pneumoniae | 4 |
| Staphylococcus epidermidis | 2 | Staphylococcus epidermidis | 3 |
| Krebsiella pneumoniae | 2 | Enterococcus faecium | 3 |
| Candida albicans | 2 | Candida albicans | 2 |
| Staphylococcus aureus | 1 | Acinetobacter baumanii | 2 |
| Pseudomonas aeruginosa | 2 | ||
| Serratia marcescens | 1 | ||
| Total | 13 | Total | 17 |
| Gram+ | 9 | Gram+ | 6 |
| Gram− | 2 | Gram− | 9 |
| Yeast | 2 | Yeast | 2 |
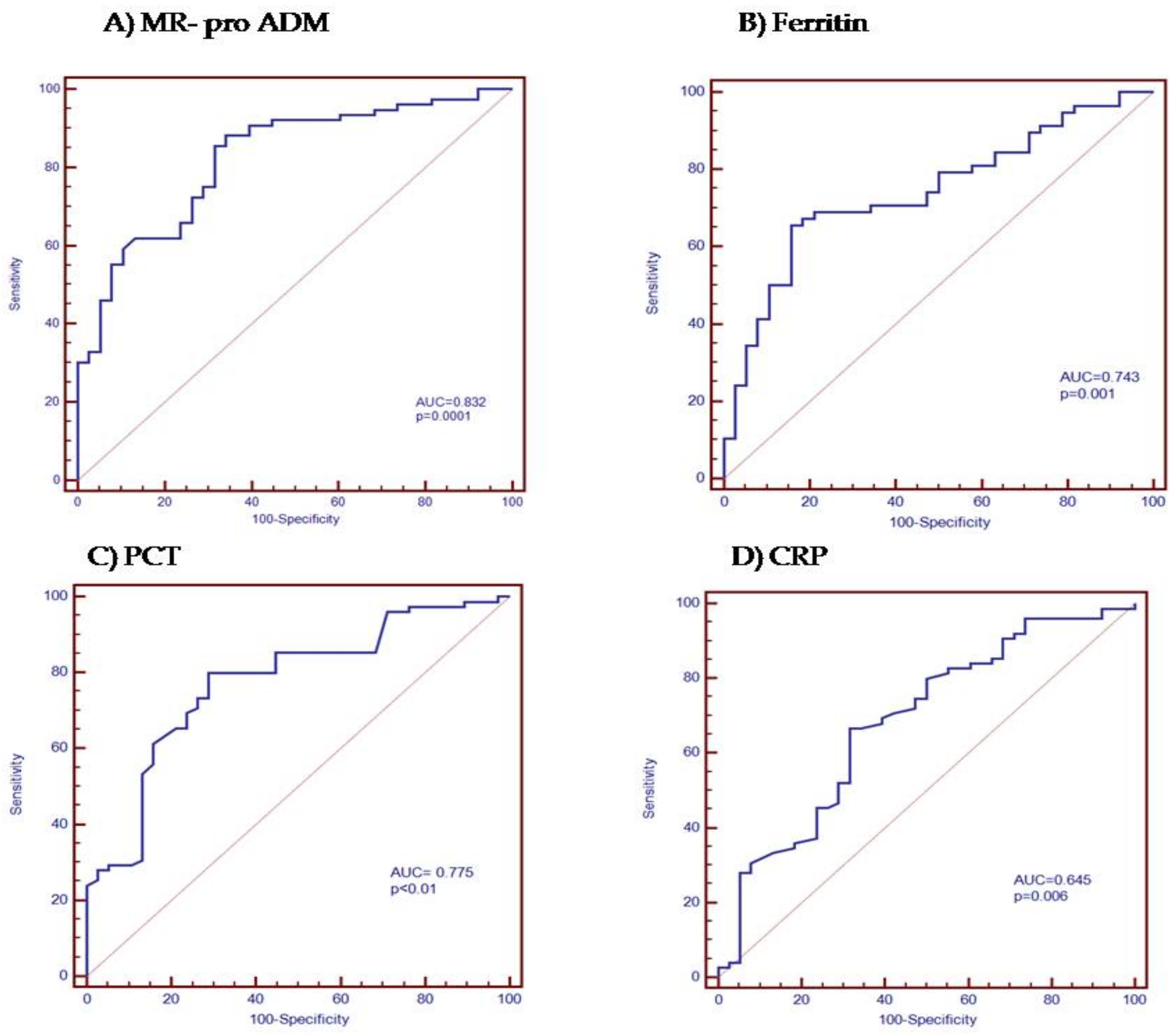
| AUC | Sensitivity | Specificity | PPV | NPV | Criterion | |
|---|---|---|---|---|---|---|
| MR pro ADM | 0.832 | 55% | 90% | 91.5% | 50.7% | >1.1 |
| Ferritin | 0.743 | 65.5% | 84.2% | 85.4% | 62.7% | >325.2 |
| PCT | 0.775 | 80% | 71.05% | 84.5% | 64.3% | >0.20 |
| CRP | 0.645 | 66.7% | 68.42% | 80.6% | 51% | >12 |
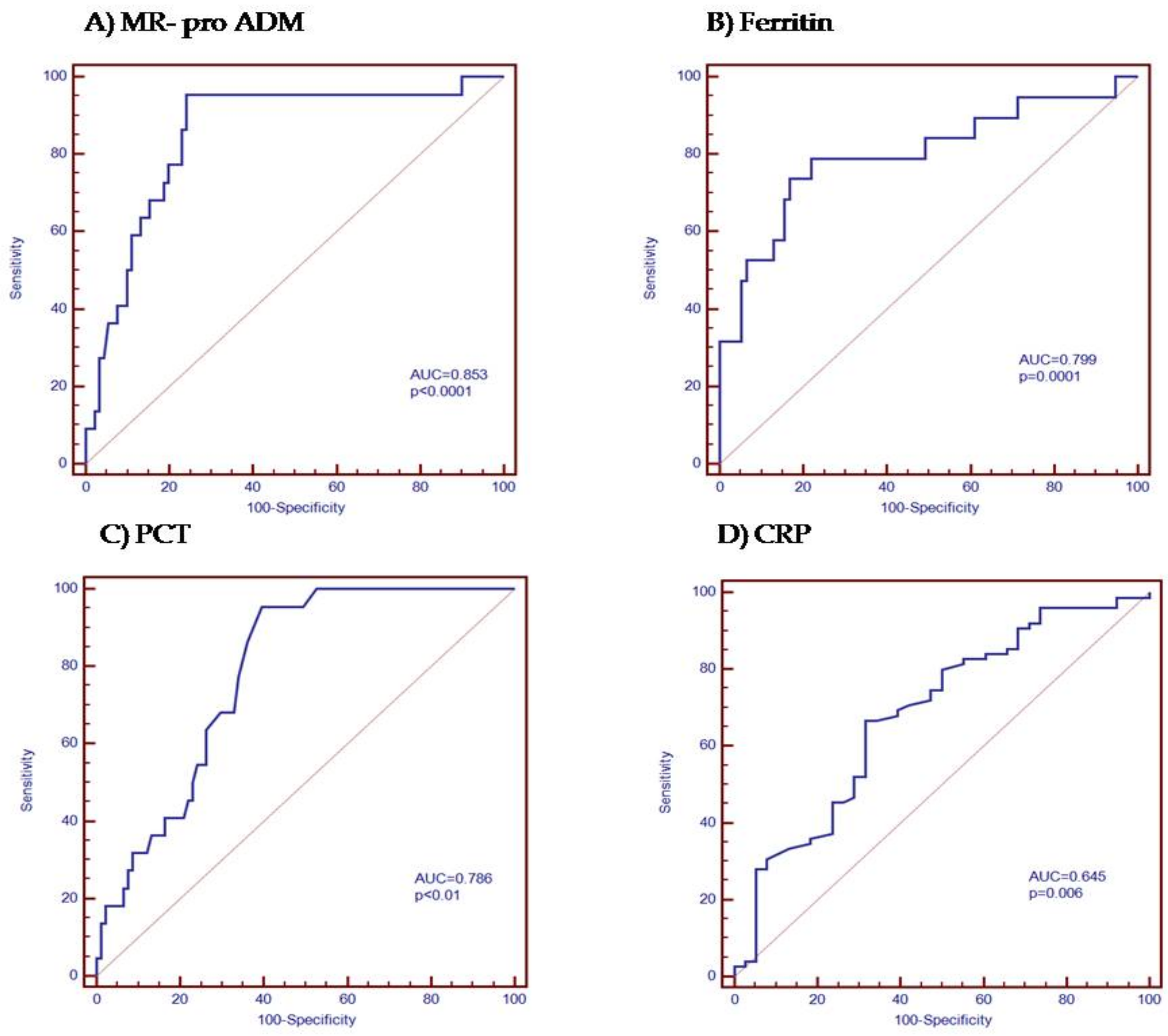
| AUC | Sensitivity | Specificity | PPV | NPV | Criterion | |
|---|---|---|---|---|---|---|
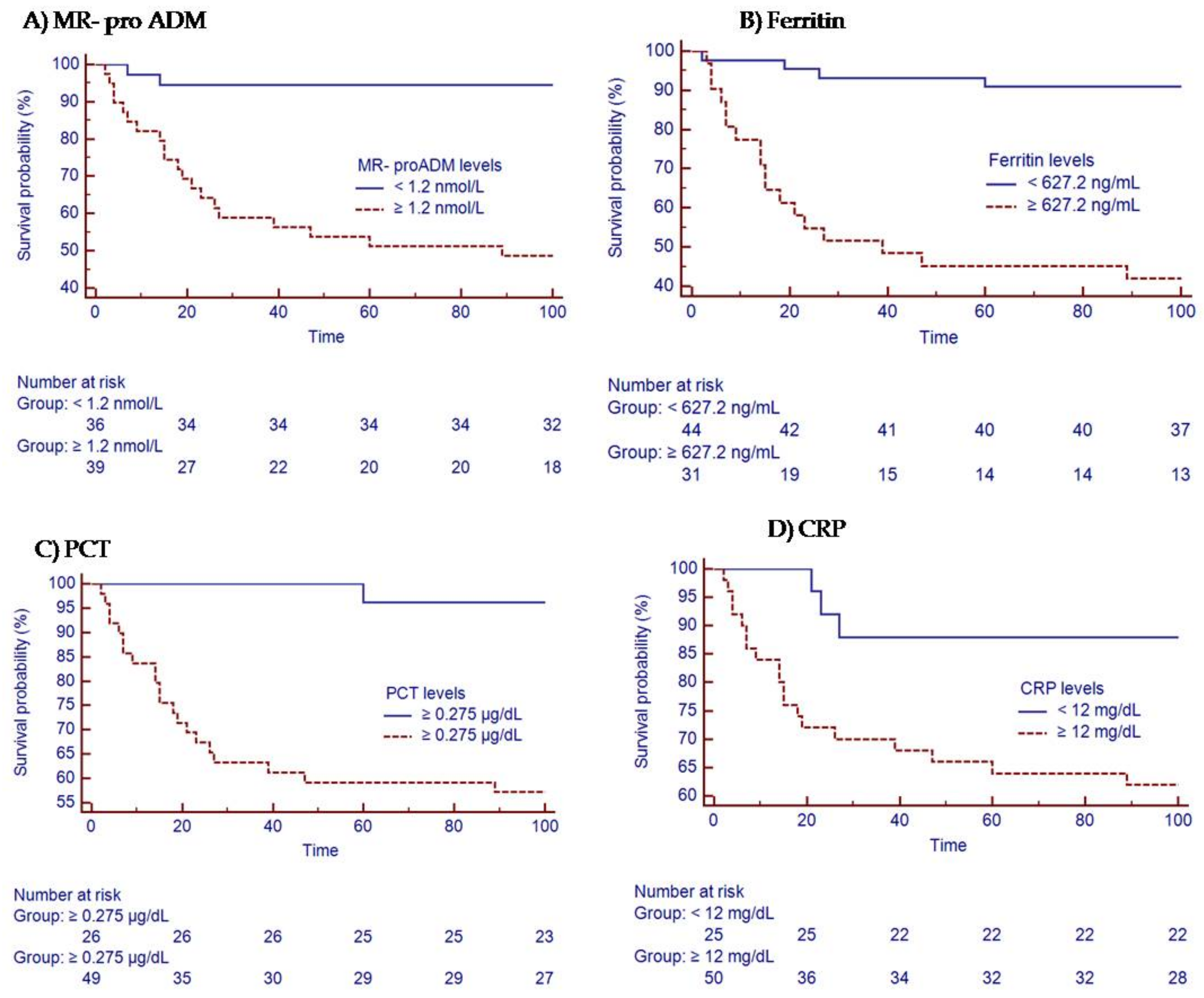
| MR-proADM | 0.853 | 95.45% | 75.82% | 48.8% | 98.6% | >1.2 |
| Ferritin | 0.799 | 78.95% | 77.92% | 46.9% | 93.7% | >627.2 |
| PCT | 0.786 | 95.45% | 60.44% | 36.8% | 98.2% | >0.275 |
| CRP | 0.645 | 86.36% | 52.75% | 30.6% | 94.1% | >12 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valenzuela-Méndez, B.; Valenzuela-Sánchez, F.; Rodríguez-Gutiérrez, J.F.; Bohollo-de-Austria, R.; Estella, Á.; Martínez-García, P.; González-García, M.Á.; Rello, J. Plasma Levels of Mid-Regional Proadrenomedullin Accurately Identify H1N1pdm09 Influenza Virus Patients with Risk of Intensive Care Admission and Mortality in the Emergency Department. J. Pers. Med. 2022, 12, 84. https://doi.org/10.3390/jpm12010084
Valenzuela-Méndez B, Valenzuela-Sánchez F, Rodríguez-Gutiérrez JF, Bohollo-de-Austria R, Estella Á, Martínez-García P, González-García MÁ, Rello J. Plasma Levels of Mid-Regional Proadrenomedullin Accurately Identify H1N1pdm09 Influenza Virus Patients with Risk of Intensive Care Admission and Mortality in the Emergency Department. Journal of Personalized Medicine. 2022; 12(1):84. https://doi.org/10.3390/jpm12010084
Chicago/Turabian StyleValenzuela-Méndez, Blanca, Francisco Valenzuela-Sánchez, Juan Francisco Rodríguez-Gutiérrez, Rafael Bohollo-de-Austria, Ángel Estella, Pilar Martínez-García, María Ángela González-García, and Jordi Rello. 2022. "Plasma Levels of Mid-Regional Proadrenomedullin Accurately Identify H1N1pdm09 Influenza Virus Patients with Risk of Intensive Care Admission and Mortality in the Emergency Department" Journal of Personalized Medicine 12, no. 1: 84. https://doi.org/10.3390/jpm12010084
APA StyleValenzuela-Méndez, B., Valenzuela-Sánchez, F., Rodríguez-Gutiérrez, J. F., Bohollo-de-Austria, R., Estella, Á., Martínez-García, P., González-García, M. Á., & Rello, J. (2022). Plasma Levels of Mid-Regional Proadrenomedullin Accurately Identify H1N1pdm09 Influenza Virus Patients with Risk of Intensive Care Admission and Mortality in the Emergency Department. Journal of Personalized Medicine, 12(1), 84. https://doi.org/10.3390/jpm12010084