Abstract
Background: Neuroendocrine neoplasms (NEN) originate from neuroendocrine cells ubiquitously spread throughout the body. Hypercalcemia associated with cancer is the most common life-threatening metabolic disorder in patients with advanced stage cancer. Paraneoplastic hypercalcemia is more commonly associated with hematological malignancies, renal and breast carcinomas, and squamous cell carcinomas, but it has also been described in patients with well-differentiated NEN, where it often remains undiagnosed. Among its causes, systemic secretion of parathyroid hormone-related protein (PTHrP) and ectopic production of 1,25-dihydroxyvitamin D and parathyroid hormone (PTH) may be considered paraneoplastic causes of hypercalcemia. In order to clarify the diagnostic work up of paraneoplastic hypercalcemia in patients with NEN, we perform a systematic review, which is lacking in the literature. Methods: We performed a data search using MEDLINE and SCOPUS including papers from 1961 to 2021. We selected articles on paraneoplastic hypercalcemia associated with well-differentiated NEN. Results: The search led to the selection of 78 publications for a total of 114 patients. Pooled data showed that the most frequent primary tumor site associated with paraneoplastic hypercalcemia was pancreatic NEN, followed by Pheochromocytoma. In most cases, paraneoplastic hypercalcemia was caused by PTHrP production and secretion. In more than two thirds of cases, paraneoplastic hypercalcemia was present at the time of NEN diagnosis and, in metachronous cases, was related to local recurrence, distant metastasis development, or tumor progression. In most patients, a combination of therapeutic approaches was employed, and reduction of the tumor burden was essential to control the paraneoplastic syndrome. Discussion: The onset of hypercalcemia associated with cancer in patients with well-differentiated NEN represents a major clinical challenge. The complex clinical and therapeutical management of paraneoplastic hypercalcemia implies the need for a multidisciplinary approach, aimed at controlling the clinical syndrome and tumor growth.
1. Introduction
Neuroendocrine neoplasms (NEN) originate from neuroendocrine cells which are distributed throughout the body. These tumors can synthesize and release biologically active substances such as hormones, peptides, or cytokines, causing distinct clinical syndromes [1] and differently impacting health-related quality of life [2,3,4]. Diagnostic and therapeutic management of functioning NEN is complex due to the high heterogeneity of these neoplasms in terms of clinical aggressiveness and the control of secretions. From the perspective of the precision medicine approach to NEN [5], the onset of paraneoplastic syndromes (PNS) should not be overlooked.
PNS are a heterogeneous group of clinical conditions, involving various systems, characterized by signs and symptoms occurring in association with malignancies. PNS are due to tumor-mediated production and release of different bioactive substances, or alternatively, by immune-mediated processes, and are not related to the specific organ or tissue from which they originate. PNS may occur before tumor diagnosis, concomitantly, or late in the course of clinical history and may influence therapeutic management. Consequently, PNS may impact prognosis and patients’ quality of life [6,7].
Hypercalcemia associated with cancer is the most common life-threatening metabolic disorder in patients with advanced-stage cancer. Hypercalcemia is associated with different neoplasms, may occur in up to 20–30% of all cancer patients, and is related to a poor prognosis. Thus, early diagnosis and intervention are of utmost importance in patients’ management. Hypercalcemia is more commonly associated with hematological malignancies, renal and breast carcinomas, and squamous cell carcinomas, but it has been also described in patients with well-differentiated NEN [8].
Hypercalcemia associated with cancer may be caused by: (i) systemic secretion of parathyroid hormone-related protein (PTHrP), a peptide produced by tumors with close homology in the N-terminal sequence to parathyroid hormone (PTH); (ii) osteolytic metastases, or, more rarely, by (iii) ectopic production of 1,25-dihydroxyvitamin D, which leads to intestinal hyperabsorption of calcium and increased osteoclastic bone reabsorption, and (iv) ectopic hyperparathyroidism [9].
Clinical presentation of hypercalcemia is influenced by its rapidity of onset and by its severity. Typical symptoms do not differ from benign hypercalcemia and may be nonspecific and develop gradually, leading to a delayed diagnosis. Signs and symptoms comprise gastrointestinal complaints such as nausea, vomiting, constipation, abdominal pain, and even anorexia, weight loss, bone pain, polyuria, weakness, and fatigue. Cardiovascular complications and arrythmias may also occur, as well as neurologic symptoms, especially in severe hypercalcemia (>14 mg/dl) [10].
Currently, data about NEN-related hypercalcemia come from case reports or case series. Most NEN-related hypercalcemia is secondary to the ectopic secretion of PTHrP, the so-called humoral hypercalcemia of malignancy, and it is more commonly described in association with pancreatic NEN (p-NEN). Different clinical presentations have been reported in association with different tumor stages, grades, and patient outcomes, as well as various therapeutic management strategies [11].
To provide a core of data about the epidemiology, clinical presentation, treatment, and impact on prognosis in patients with well-differentiated NEN-related hypercalcemia, we performed a systematic review [12].
2. Materials and Methods
We performed a systematic review of the literature according to the Cochrane Collaboration and PRISMA statement [13]. We searched for English-language articles in MEDLINE and SCOPUS, no timeframe restrictions were applied, including papers from 1961 to 2021. We searched for potentially relevant studies through these keywords: PTHrP AND NET/NEN; PTH AND NET/NEN; paraneoplastic hypercalcemia AND NET/NEN; and hypercalcemia AND NET/NEN. Eligibility criteria for study selection included studies on humans with any of the following designs: randomized clinical trials, prospective non-randomized trials, retrospective studies, case series, case reports, brief communications, and letters to the editor. We selected articles on paraneoplastic hypercalcemia associated with well-differentiated NEN, including paragangliomas, pheochromocytomas, medullary thyroid cancer, thymic and mediastinal, ovarian, uterine, cervical, gastroentheropancreatic, lung, and rectal NEN. For each paper, we analyzed patients’ age, sex, signs, symptoms, time presentation of hypercalcemia and hypercalcemia inducing molecules (PTH, PTHrP, 1,25(OH) vitamin D) or other peptide secretion. We furthermore evaluated the primary NEN’s site, grade, staging (with ENETS classification), type of metastasis at diagnosis of paraneoplastic hypercalcemia, NEN and hypercalcemia therapy, and patients’ survival from the onset of hypercalcemia. Each study was screened by abstract and title, and potentially eligible studies were further assessed in detail by retrieving full-length articles. Each full-length article was independently reviewed by three separate authors (AR, IZ, and FS) following the inclusion criteria. Three authors (AR, IZ, and FS) independently extracted data from the articles that met the inclusion criteria. A standardized form was used to extract relevant data.
Data are expressed as mean and standard deviation (SD) or median and 25–75% interquartile range (IQR), as appropriate. Normally distributed variables were assessed using the Shapiro–Wilk test. Homoscedasticity and homogeneity of variances were assessed by visual inspection and with Levene’s test. Differences between independent groups were evaluated using the t test for normally distributed variables and using the nonparametric Mann–Whitney test for non-normally distributed variables. Differences between the binomial proportions of independent groups of a dichotomous-dependent variable were assessed for homogeneity using the chi-square test or Fisher’s exact test, as appropriate. All statistical analyses were performed with SPSS Statistics version 27.0 (IBM SPSS Statistics Inc., Chicago, IL, USA).
3. Results
From the original number of 1281 studies, we excluded 1192 articles after title and abstract screening; reasons for exclusion included duplicates and studies in which hypercalcemia was due to primary hyperparathyroidism associated to genetic syndromes. We furthermore completed our research by analyzing the references of the selected papers (see Figure 1). We finally assessed 78 papers for a total of 114 patients for eligibility (see Table 1) [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91]. The main clinical features of the gathered cases are summarized in Table 2.
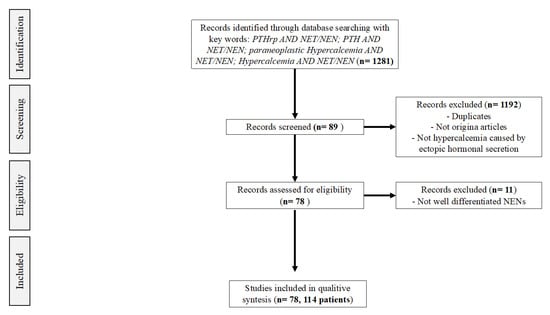
Figure 1.
Flowchart of the literature search for the systematic review study. From: Liberati A, Altman DG, Tetzlaff J, Mulrow C, et al. (2009) The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med 6(7): e1000100. doi:10.1371/journal.pmed.1000100.

Table 1.
Summary of cases of paraneoplastic hypercalcemia in well-differentiated NEN reported in the literature.
Table 2.
Demographic, pathological, and clinical characteristics of well-differentiated NEN patients with paraneoplastic hypercalcemia reported in the literature.
The mean age of the patients was 46.3 ± 15.8 years and a slight majority of them was male (54.9%). The most frequent histological origin, with more than two thirds of the reported cases (72.8%), was p-NEN, followed by Pheochromocytoma (15.8%). All other NEN types were present only in a few patients. At the time of paraneoplastic hypercalcemia onset, most patients had a metastatic NEN disease (57.9%); in particular, the most common metastatic site by far was the liver, followed by the lymph nodes, bone, and lungs. Only 13.3% of patients with p-NEN (11/83) had a localized disease at paraneoplastic hypercalcemia onset, while the great majority of Pheochromocytoma cases (94.4%; 17/18) showed no sign of metastatic involvement at paraneoplastic hypercalcemia onset, although the adrenal tumors were, in the reports with available data, on average, quite large (mean size 5.5 × 6.6 cm).
3.1. Clinical Presentation
In 69.3% of cases, paraneoplastic hypercalcemia was present at the time of NEN diagnosis; this finding was especially true for those patients with Pheochromocytoma, among which 88.9% presented with paraneoplastic hypercalcemia at the time of tumor diagnosis. In the remaining cases, paraneoplastic hypercalcemia arose later in the course of the neoplastic disease, with a mean time from NEN diagnosis of 83.4 ± 56.3 months. The metachronous onset of paraneoplastic hypercalcemia was associated with the development of local recurrence or distant metastases and tumor progression in 43.8% and 50% of cases, respectively.
Among all cases, mean calcemic levels at paraneoplastic hypercalcemia onset were 14 ± 2.7 mg/dl. Calcemic levels in patients with p-NEN were higher than those in patients with a Pheochromocytoma, and this difference was found to be statistically significant (p < 0.001). No significant difference in the degree of hypercalcemia was found when comparing patients based on paraneoplastic hypercalcemia-producing molecules or paraneoplastic hypercalcemia onset (at NEN diagnosis vs. metachronous onset).
Data regarding the humoral factors responsible for paraneoplastic hypercalcemia were available only for 80 patients. In most cases (85%), PTHrP was considered the peptide implicated in paraneoplastic hypercalcemia onset and progression; PTH was elevated in 11.3% of patients with paraneoplastic hypercalcemia, while paraneoplastic hypercalcemia was driven by 1,25(OH) vitamin D in only three patients [14,17,26].
Besides hypercalcemia-producing molecules, 28.1% of the patients (mostly p-NEN) showed cosecretion of other peptides: the most frequent was calcitonin, followed by vasoactive intestinal peptide (VIP), pancreatic polypeptide, gastrin, somatostatin, and glucagon; there was a cosecretion of adrenocorticotropic hormone (ACTH) in only one case [88]. Interestingly, in seven cases, cosecretion of multiple peptides was reported [18,29,42,45,80].
3.2. Symptomatology
In 25.4% of cases, the clinical presentation of paraneoplastic hypercalcemia was not described; in the other 85 patients (74.6%), multiple signs and symptoms associated with paraneoplastic hypercalcemia were reported. Symptoms can develop gradually and become clinically evident only when blood calcium levels are very high. The severity of the onset depends not only on the age and the comorbidities of the patients, but also on the site of onset of the malignancy and on the grading of the primary NEN. It is very interesting to underline that the symptomatology of hypercalcemia could be synchronous with the diagnosis of the tumor or metachronous, and often correlated, with the progression of disease, even after many years.
The most recurring symptoms are anorexia and fatigue, which are described, respectively, in 37.6% and 31.8% of patients. For both symptoms, a progressive onset, often associated with other gastrointestinal symptoms, was reported. Anorexia is characterized by a typical gradual and involuntary weight loss, suggestive of neoplastic pathology. Among the typical symptoms of hypercalcemia, vomiting and nausea are described, respectively, in 24.7% and 21.2% of patients. Abdominal pain is another common clinical manifestation (21.2%) of paraneoplastic hypercalcemia, and it is depicted as an “indigestion pain” [20], an “abdominal discomfort” [34,55], and is associated with abdominal cramps without a well-defined localization. Constipation is the least frequent gastrointestinal symptom, complained about by only 9.4% of patients. This clinical picture is often evident at the diagnosis of NEN; however, it is difficult to discern with certainty whether it is caused by the neoplasm itself or by hypercalcemia. Regarding genitourinary manifestations of paraneoplastic hypercalcemia, synchronous polyuria and polydipsia are described, respectively, in 14.1% and 11.8% of patients and were linked to the onset of nephrogenic diabetes insipidus disease in one patient [74]. Paraneoplastic hypercalcemia, moreover, rarely causes dehydration up to the development of acute renal failure (2.4%); dehydration is often caused by diarrhea triggered by vasoactive hormones such as VIP [80,90]. The synchronous diagnosis of nephrolithiasis associated with NEN is mentioned in only four patients [32,45,63,81]. Neuropsychiatric symptoms are outlined in 7.1% of patients by the progressive development of cognitive dysfunction. Mental confusion at the diagnosis of NEN with an inability to maintain concentration and, in some cases, with an impaired short-term memory are described in 8.2% of patients. Hypercalcemia could, moreover, cause unexpected changes in patients’ behavior, anxiety, and depression up to the development of drowsiness, lethargy, and coma. Musculoskeletal symptoms are poorly described in the literature; however, muscle weakness is the most prevalent one (10.6%), followed by cramps, myopathy, and osteopenia and/or osteoporosis. With regard to bone pain (3.5%), Ataallah et al. and Rasbach er al. described two cases of arthralgia associated with hypercalcemia [16,78]. Cardiovascular manifestations are typically synchronous with the NEN diagnosis and include arrhythmias and hypertension, which are complained about by 14.1% of patients; however, in 10 of these patients, paraneoplastic hypercalcemia was caused by a Pheochromocytoma [35,61,73,76,77,81,89], thus is difficult to define if hypertension was caused by the effect of catecholamines or by paraneoplastic hypercalcemia. Lastly, Abraham et al. described a case report of paraneoplastic hypercalcemia correlated with diagnosis of p-NEN in a pregnant woman at 29 weeks’ gestation, which caused a symptomatology comparable with pre-eclampsia characterized by consciousness, headache, hypertension, and proteinuria [43].
3.3. Treatment Approach for Paraneoplastic Hypercalcemia
Only 85 cases had available data about the treatment used for the management of paraneoplastic hypercalcemia.
In most patients, a combination of therapeutic approaches was employed, mostly intravenous hydration, loop diuretics, and bisphosphonates (mainly pamidronate and zoledronate). In fewer cases, calcitonin and glucocorticoid were also employed, while the use of denosumab and cinacalcet was reported in only six and four cases, respectively. See Table 1.
Regarding antineoplastic therapy, data were available for 95 patients. In most cases, a combination of antineoplastic approaches was used. A total of 60 (63.2%) patients underwent surgery, both at the primary site and for metastatic or recurrent disease. Local techniques (embolization or radiofrequency ablation) were used in 17.9% patients for treating their liver metastases. Regarding medical therapy, somatostatin analogues (SSAs) were used in 37.9% of patients, chemotherapy was employed in 32.6% of patients, peptide receptor radionuclide therapy (PRRT) was administered in 10.5% patients, and target therapy with sunitinib and everolimus were both employed in five cases. See Table 1.
Data regarding paraneoplastic hypercalcemia response to therapy (both medical and antineoplastic) were available for 84 cases. Disease burden-reducing techniques (surgery, embolization) were able to control paraneoplastic hypercalcemia in 39.3% of cases, mainly in patients with localized, operable disease. Medical therapy alone could control paraneoplastic hypercalcemia in only 13.1% of patients, primarily through the utilization of bisphosphonates; in particular, intravenous hydration alone determined normalization of calcemic levels in only two patients and, when associated with other treatments, in three more cases. Medical antineoplastic treatments alone controlled paraneoplastic hypercalcemia in 20.2% of patients. In the remaining cases (27.4%), different combinations of therapies, including medical therapy for paraneoplastic hypercalcemia and antineoplastic (both surgical and medical), were used together to achieve paraneoplastic hypercalcemia control.
Survival data were available for 74 patients; median overall survival was 18 months (IQR range, 7–37). Among patients with p-NEN, median survival was 23.5 months (IQR range, 9.8–48).
4. Discussion
Nowadays, paraneoplastic hypercalcemia is a well-established paraneoplastic syndrome that is associated with many malignancies, even if the relationship between NEN and hypercalcemia is still little considered. Systematically reviewing the literature, we extracted that this rare condition was described in a total of 114 cases of patients with well-differentiated NEN.
The pancreas represents the most frequent localization of NEN associated with paraneoplastic hypercalcemia (72.8%), followed by Pheochromocytoma (15.8%). This observation is particularly interesting if we consider that, in an animal study, it has been demonstrated that PTHrP acts as a growth factor for pancreatic beta-cells [92] and that, in chronic pancreatitis, PTHrP functions as a mediator of proinflammatory and profibrotic cytokines, which in turn regulate PTHrP expression [93]. As in other malignancies, paraneoplastic hypercalcemia may also occur in NEN through several different mechanisms, including PTHrP secretion, PTH secretion, and calcitriol overproduction. In NEN, as in all other types of solid cancers, the most common cause of paraneoplastic hypercalcemia is the tumor production and release of PTHrP (85% of cases). PTHrP carries out a physiologic role in embryologic development and in mammary gland function, but it has no other known functional role in the adult metabolism [94]. PTHrP shares its amino acid sequence homology with PTH at its N-terminus and activates the type 1 PTH receptor, but it is encoded by a different gene [95]. Like PTH, PTHrP also increases calcium reabsorption in the kidney and stimulates osteoblasts to secrete receptor activators of nuclear factor-B ligands (RANKL), which bind to the RANK receptor on osteoclasts [96,97]. This interaction mediates the differentiation of osteoclast precursors into mature osteoclasts and increases bone resorption by osteoclasts. Since the most frequent cause of paraneoplastic hypercalcemia in NEN is PTHrP secretion, PTHrP levels should be checked in all patients with this clinical and biochemical suspect. The accuracy and reliability of laboratory assays for PTHrP have improved because of newer double-antibody techniques. Furthermore, when elevated at tumor diagnosis, PTHrP can be used as a biomarker to assess treatment response to therapy.
A less common cause of paraneoplastic hypercalcemia is the paraneoplastic ectopic secretion of PTH by tumors, which has been described in association with several malignancies, most of which are of the lung [98,99,100]. Only three cases of well-differentiated NEN associated with paraneoplastic hypercalcemia secondary to tumor-mediated overproduction of calcitriol are described in the literature [14,17,26]. Over production of calcitriol is a typical cause of paraneoplastic hypercalcemia in lymphomas [101,102], in which tumor cells or surrounding lymphocytes overexpress 1α-hydroxylase, which causes ectopic conversion of 25 hydroxyvitamin D to 1,25-dihydroxyvitamin D [103,104]. Calcitriol-related hypercalcemia derives from both increased intestinal and bone reabsorption of calcium.
This review showed the timing of paraneoplastic hypercalcemia occurrence during the “natural history” of well-differentiated NEN disease. In most cases, hypercalcemia is already present at diagnosis (69.3% of cases); in others, it develops during the disease (mean time from NEN diagnosis of 83.4 ± 56.3 months). In most cases, the metachronous occurrence of hypercalcemia is associated with disease progression/relapse. In the case of Pheochromocytoma, hypercalcemia was already present at diagnosis in 88.9% of cases, while in two cases, hypercalcemia was observed at the recurrence of the disease 94 and 204 months after the first surgical treatment, respectively. Hypercalcemia is almost always associated with the presence of distant metastases, except in 10.5% of cases, in which there were no metastases or there were only metastases to the local regional lymph nodes. Therefore, it seems that the tumor burden at diagnosis or during disease progression determines the capacity of hormone secretion by the neoplasm, which is different to what is described in the literature for Pheochromocytoma.
Paraneoplastic hypercalcemia is typically associated with severe clinical signs and symptoms and is often an oncologic emergency [9], while the paraneoplastic hypercalcemia of the NEN as a whole seems to give more moderate symptoms, similar to those of primary hyperparathyroidism. The most frequent symptoms are asthenia, gastrointestinal, and genitourinary disturbances. Severe symptoms such as pre-eclampsia, coma, lethargy, and arrhythmia have been described in extremely rare cases.
The management of paraneoplastic hypercalcemia in well-differentiated NEN is challenging. In fact, in our review, we observed that, in 27.4% of cases, the combination of multiple treatments (medical therapy for paraneoplastic hypercalcemia and different antineoplastic (both surgical and medical) treatments, variously combined) was required to obtain control of hypercalcemia. Disease burden-reducing techniques (surgery, embolization) were able to control paraneoplastic hypercalcemia, mainly in patients with localized, operable disease. Medical therapy alone could control paraneoplastic hypercalcemia in selected patients, primarily through the employment of bisphosphonates; in particular, intravenous hydration alone determined calcemic normalization in only two patients and, when associated with other treatments, the improvement is measured in very few cases. Medical antineoplastic treatments alone controlled paraneoplastic hypercalcemia in less than a quarter of reported patients. Therefore, the pooled data from our systematic review show that tumor debulking plays a key role in controlling paraneoplastic hypercalcemia in patients with well-differentiated NEN, so surgical treatment should be indicated whenever feasible. PRRT was administered in a limited number of cases; however, given its capability to control functioning tumors [105] and its potential role as a neoadjuvant therapy [106,107,108], PRRT could be prescribed either before surgery or in patients with progressive metastatic inoperable disease to reduce tumor secretion and tumor burden.
The onset of hypercalcemia associated with cancer in patients with well-differentiated NEN represents a major clinical challenge. Prior to the diagnosis of paraneoplastic hypercalcemia, physicians should rule out multiple endocrine neoplasia (MEN) 1 and 2 [109,110], in which the hypercalcemia could be due to primary hyperparathyroidism. Paraneoplastic hypercalcemia caused by ectopic production of PTH, although uncommon, should be considered in patients with p-NET when PTH levels are significantly elevated and there is no evidence of a parathyroid-related cause. Recognizing the association between elevated PTH levels and paraneoplastic hypercalcemia can prevent unnecessary parathyroid or exploratory neck surgery. Since paraneoplastic hypercalcemia must be recognized and framed promptly, and as it often remains undiagnosed, the complex clinical and therapeutical management of paraneoplastic hypercalcemia implies the need for a multidisciplinary approach, aimed at controlling the clinical syndrome and tumor growth. With the present review we have shown how paraneoplastic hypercalcemia in well-differentiated NEN was diagnosed and managed over the years and how important it is to conduct a personalized diagnostic and therapeutic process that provides an overview of the patient and his status.
In summary, compared with paraneoplastic hypercalcemia of solid and hematological tumors, paraneoplastic hypercalcemia in NEN shares PTHrP as the most common causal agent with solid tumors, while paraneoplastic hypercalcemia in lymphomas is more frequently caused by 1,25(OH) vitamin D. Furthermore, paraneoplastic hypercalcemia in NEN seems to be less severe than in solid and hematological tumors. Finally, the prognosis of paraneoplastic hypercalcemia of solid and hematological tumors seems to be worse than in NEN; this could be related to the milder symptomatology of NEN patients and to their better oncological prognosis.
A limitation of this review is represented by the difficulty of bibliographic research and data extraction. Since paraneoplastic hypercalcemia in NEN is a rare condition, we decided not to place timeframe restrictions in the selection of the articles; this allowed us to include a considerable number of cases in the review. However, it led to a lot of missing data, especially from the oldest articles. Indeed, relevant information such as grading, staging, and the paraneoplastic hypercalcemia-inducing molecule were not reported in some older case reports; interestingly, in cases from 1961 to 1991, an unspecified PTH-like substance was considered responsible for paraneoplastic hypercalcemia. Given that PTHrP was first isolated in 1987, we could speculate that, in those patients, PTHrP was the paraneoplastic hypercalcemia-driving molecule. See Table 1.
Author Contributions
Conceptualization, E.G., A.C. and A.F.; methodology, F.S., A.R. and I.Z.; validation, F.S., A.R., I.Z. and E.G.; formal analysis, E.M.G.; investigation, F.S., A.R. and I.Z.; resources, F.S., A.R. and I.Z.; data curation, E.G., A.C. and A.F.; writing—original draft preparation, E.G., F.S., R.M., A.R. and I.Z.; writing—review and editing, E.G., F.S., R.M. and A.F.; visualization, E.G., F.S. and A.F.; supervision, A.C. All authors have read and agreed to the published version of the manuscript.
Funding
Ministerial research project PRIN2017Z3N3YC.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
This review is part of the ‘NIKE’ project (Neuroendocrine tumors Innovation Knowledge and Education) led by Annamaria Anita Livia Colao and Antongiulio Faggiano, which aims to increase knowledge of NETs. We would like to acknowledge the project coordinators, Diego Ferone (Genoa), Andrea M. Isidori (Rome), and Maria Chiara Zatelli (Ferrara), and all those who contributed: Manuela Albertelli (Genoa), Barbara Altieri (Würzburg, Germany), Filomena Bottiglieri (Naples), Roberta Centello (Rome), Federica de Cicco (Naples), Alessandra Dicitore (Milan), Valentina Di Vito (Rome), Giuseppe Fanciulli (Sassari), Tiziana Feola (Rome), Francesco Ferraù (Messina), Marco Gallo (Turin), Federica Grillo (Genova), Andrea Lania (Rozzano), Fabio Lo Calzo (Naples), Erika Messina (Messina), Giovanna Muscogiuri (Naples), Luca Pes (Cagliari), Genoveffa Pizza (Naples), Riccardo Pofi (Rome), Giulia Puliani (Rome), Carmen Rainone (Naples), Paola Razzore (Turin), Manila Rubino (Milan), Rosaria Maddalena Ruggeri (Messina), Emilia Sbardella (Rome), Franz Sesti (Rome), Giovanni Vitale (Milan). We wish to thank the NETTARE Unit—NeuroEndocrine Tumor TAsk foRcE of “Sapienza” University of Rome, Italy, led by Andrea Lenzi, Andrea M. Isidori, Antongiulio Faggiano, and Elisa Giannetta, for integrating the patients’ multidisciplinary clinical, diagnostic, and therapeutic management and follow-up.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Yao, J.C.; Hassan, M.; Phan, A.; Dagohoy, C.; Leary, C.; Mares, J.E.; Evans, D.B. One hundred years after “carcinoid”: Epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J. Clin. Oncol. 2008, 26, 3063–3072. [Google Scholar] [CrossRef]
- Zamponi, V.; La Salvia, A.; Tarsitano, M.G.; Mikovic, N.; Rinzivillo, M.; Panzuto, F.; Giannetta, E.; Faggiano, A.; Mazzilli, R. Effect of Neuroendocrine Neoplasm Treatment on Human Reproductive Health and Sexual Function. J. Clin. Med. 2022, 11, 3983. [Google Scholar] [CrossRef] [PubMed]
- Modica, R.; Scandurra, C.; Maldonato, N.M.; Dolce, P.; Dipietrangelo, G.G.; Centello, R.; Di Vito, V.; Giannetta, E.; Isidori, A.M.; Lenzi, A.; et al. Health-related quality of life in patients with neuroendocrine neoplasms: A two-wave longitudinal study. J. Endocrinol. Investig. 2022, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Scandurra, C.; Modica, R.; Maldonato, N.M.; Dolce, P.; Dipietrangelo, G.G.; Centello, R.; Di Vito, V.; Bottiglieri, F.; de Cicco, F.; Giannetta, E.; et al. Quality of Life in Patients with Neuroendocrine Neoplasms: The Role of Severity, Clinical Heterogeneity, and Resilience. J. Clin. Endocrinol. Metab. 2021, 106, e316–e327. [Google Scholar] [CrossRef] [PubMed]
- Gaudenzi, G.; Dicitore, A.; Carra, S.; Saronni, D.; Pozza, C.; Giannetta, E.; Persani, L.; Vitale, G. MANAGEMENT of ENDOCRINE DISEASE: Precision medicine in neuroendocrine neoplasms: An update on current management and future perspectives. Eur. J. Endocrinol. 2019, 181, R1–R10. [Google Scholar] [CrossRef]
- Kaltsas, G.; Androulakis, I.I.; de Herder, W.W.; Grossman, A.B. Paraneoplastic syndromes secondary to neuroendocrine tumours. Endocr. Relat. Cancer 2010, 17, R173–R193. [Google Scholar] [CrossRef] [PubMed]
- Dimitriadis, G.K.; Angelousi, A.; Weickert, M.O.; Randeva, H.S.; Kaltsas, G.; Grossman, A. Paraneoplastic endocrine syndromes. Endocr. Relat. Cancer 2017, 24, R173–R190. [Google Scholar] [CrossRef]
- Asonitis, N.; Angelousi, A.; Zafeiris, C.; Lambrou, G.I.; Dontas, I.; Kassi, E. Diagnosis, Pathophysiology and Management of Hypercalcemia in Malignancy: A Review of the Literature. Horm. Metab. Res. 2019, 51, 770–778. [Google Scholar] [CrossRef]
- Stewart, A.F. Clinical practice. Hypercalcemia associated with cancer. New Engl. J. Med. 2005, 352, 373–379. [Google Scholar] [CrossRef]
- Rosner, M.H.; Dalkin, A.C. Onco-nephrology: The pathophysiology and treatment of malignancy-associated hypercalcemia. Clin. J. Am. Soc. Nephrol. 2012, 7, 1722–1729. [Google Scholar] [CrossRef]
- Tsoli, M.; Dimitriadis, G.K.; Androulakis, I.I.; Kaltsas, G.; Grossman, A. Paraneoplastic Syndromes Related to Neuroendocrine Tumors. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Faggiano, A.; Colao, A. Editorial-Special Issue: Foreword to the Special Issue on NIKE: Neuroendocrine Tumors, Innovation in Knowledge and Education. Front. Endocrinol. 2021, 12, 722145. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef]
- Giannetta, E.; Sesti, F.; Modica, R.; Grossrubatscher, E.M.; Guarnotta, V.; Ragni, A.; Zanata, I.; Colao, A.; Faggiano, A. Case Report: Unmasking Hypercalcemia in Patients With Neuroendocrine Neoplasms. Experience From Six Italian Referral Centers. Front. Endocrinol. 2021, 12, 665698. [Google Scholar] [CrossRef]
- Copur, M.S.; Vargas, L.; Wedel, W.; Merani, S.; Cushman-Vokoun, A.; Drincic, A. Pancreatic Neuroendocrine Tumor With Humoral Hypercalcemia and High Tumor PD-L1 Score. Oncology 2020, 34, 548–552. [Google Scholar] [CrossRef]
- Ataallah, B.; Buttar, B.S.; Kulina, G.; Kaell, A. Hypercalcemia in a Patient Diagnosed with a Vasoactive Intestinal Peptide Tumor. Cureus 2020, 12, e6882. [Google Scholar] [CrossRef]
- van Lierop, A.H.; Bisschop, P.H.; Boelen, A.; van Eeden, S.; Engelman, A.F.; van Dijkum, E.J.N.; Klümpen, H.-J. Hypercalcaemia due to a calcitriol-producing neuroendocrine tumour. J. Surg. Case Rep. 2019, 2019, rjz346. [Google Scholar] [CrossRef]
- Gild, M.L.; Tsang, V.; Samra, J.; Clifton-Bligh, R.J.; Tacon, L.; Gill, A.J. Hypercalcemia in Glucagon Cell Hyperplasia and Neoplasia (Mahvash Syndrome): A New Association. J. Clin. Endocrinol. Metab. 2018, 103, 3119–3123. [Google Scholar] [CrossRef]
- Daskalakis, K.; Chatzelis, E.; Tsoli, M.; Papadopoulou-Marketou, N.; Dimitriadis, G.K.; Tsolakis, A.V.; Kaltsas, G. Endocrine paraneoplastic syndromes in patients with neuroendocrine neoplasms. Endocrine 2019, 64, 384–392. [Google Scholar] [CrossRef]
- Symington, M.; Davies, L.; Kaltsas, G.; Weickert, M.O. Malignant hypercalcaemia related to parathyroid hormone-related peptide (PTHrP) secretion from a metastatic pancreatic neuroendocrine tumour (NET). BMJ Case Rep. 2017, 2017, bcr2017219692. [Google Scholar] [CrossRef]
- Lu, C.; Wang, Z.; Wang, G.; Wang, X.; Liu, X. Superior mediastinal typical carcinoid detected by 99mTc-MIBI SPECT/CT imaging: A case report. Medicine 2017, 96, e9457. [Google Scholar] [CrossRef]
- Ranade, R.; Basu, S. Metabolic Bone Disease in the Context of Metastatic Neuroendocrine Tumor: Differentiation from Skeletal Metastasis, the Molecular PET-CT Imaging Features, and Exploring the Possible Etiopathologies Including Parathyroid Adenoma (MEN1) and Paraneoplastic Humoral Hypercalcemia of Malignancy Due to PTHrP Hypersecretion. World J. Nucl. Med. 2017, 16, 62–67. [Google Scholar] [PubMed]
- Valdes-Socin, H.; Almanza, M.R.; Fernández-Ladreda, M.T.; Van Daele, D.; Polus, M.; Chavez, M.; Beckers, A. Use of cinacalcet and sunitinib to treat hypercalcaemia due to a pancreatic neuroendocrine tumor. Arch. Endocrinol. Metab. 2017, 61, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Iliuta, I.A.; Beauregard, J.M.; Couture, F.; Douville, P.; Mac-Way, F. Reversal of Severe and Refractory Humoral Hypercalcemia With 177Lu-Octreotate Peptide Receptor Radionuclide Therapy for Neuroendocrine Tumor of the Pancreas. Clin. Nucl. Med. 2015, 40, e448–e450. [Google Scholar] [CrossRef] [PubMed]
- Teng, J.; Abell, S.; Hicks, R.J.; Hofman, M.S.; Sachithanandan, N.; McKelvie, P.; MacIsaac, R.J. Protracted hypocalcaemia following a single dose of denosumab in humoral hypercalcaemia of malignancy due to PTHrP-secreting neuroendocrine tumour. Clin. Endocrinol. 2014, 81, 940–942. [Google Scholar] [CrossRef]
- Zhu, V.; de Las Morenas, A.; Janicek, M.; Hartshorn, K. Hypercalcemia from metastatic pancreatic neuroendocrine tumor secreting 1,25-dihydroxyvitamin D. J. Gastrointest. Oncol. 2014, 5, E84–E87. [Google Scholar]
- Kamp, K.; Feelders, R.A.; van Adrichem, R.C.S.; de Rijke, Y.B.; van Nederveen, F.H.; Kwekkeboom, D.J.; de Herder, W.W. Parathyroid hormone-related peptide (PTHrP) secretion by gastroenteropancreatic neuroendocrine tumors (GEP-NETs): Clinical features, diagnosis, management, and follow-up. J. Clin. Endocrinol. Metab. 2014, 99, 3060–3069. [Google Scholar] [CrossRef]
- Rossi, R.E.; Naik, K.; Navalkissoor, S.; Imber, C.; O’Beirne, J.; Toumpanakis, C.; Caplin, M.E. Case report of multimodality treatment for metastatic parathyroid hormone-related peptide-secreting pancreatic neuroendocrine tumour. Tumori 2014, 100, 153e–156e. [Google Scholar] [CrossRef]
- Milanesi, A.; Yu, R.; Wolin, E.M. Humoral hypercalcemia of malignancy caused by parathyroid hormone-related peptide-secreting neuroendocrine tumors. Report of six cases. Pancreatology 2013, 13, 324–326. [Google Scholar] [CrossRef]
- Shah, R.H.; Martinez, D. Pancreatic neuroendocrine tumor associated with humoral hypercalcemia of malignancy and carcinoid tumor: A case report and review of the literature. Pancreas 2013, 42, 549–551. [Google Scholar] [CrossRef]
- Kanakis, G.; Kaltsas, G.; Granberg, D.; Grimelius, L.; Papaioannou, D.; Tsolakis, A.V.; Öberg, K. Unusual complication of a pancreatic neuroendocrine tumor presenting with malignant hypercalcemia. J. Clin. Endocrinol. Metab. 2012, 97, E627–E631. [Google Scholar] [CrossRef]
- Kandil, E.; Noureldine, S.; Khalek, M.A.; Daroca, P.; Friedlander, P. Ectopic secretion of parathyroid hormone in a neuroendocrine tumor: A case report and review of the literature. Int. J. Clin. Exp. Med. 2011, 4, 234–240. [Google Scholar]
- Ghazi, A.A.; Boustani, I.; Amouzegar, A.; Attarian, H.; Pourafkari, M.; Gashti, H.N.; Sabetian, T.; Tirgari, F.; Ghazi, S.; Kovacs, K. Postpartum hypercalcemia secondary to a neuroendocrine tumor of pancreas; a case report and review of literature. Iran. J. Med. Sci. 2011, 36, 217–221. [Google Scholar]
- Shirai, K.; Inoue, I.; Kato, J.; Maeda, H.; Moribata, K.; Shingaki, N.; Ueda, K.; Deguchi, H.; Maekita, T.; Iguchi, M.; et al. A case of a giant glucagonoma with parathyroid hormone-related peptide secretion showing an inconsistent postsurgical endocrine status. Intern. Med. 2011, 50, 1689–1694. [Google Scholar] [CrossRef]
- Takeda, K.; Hara, N.; Kawaguchi, M.; Nishiyama, T.; Takahashi, K. Parathyroid hormone-related peptide-producing non-familial pheochromocytoma in a child. Int. J. Urol. 2010, 17, 673–676. [Google Scholar] [CrossRef]
- Morita, Y.; Suzuki, S.; Sakaguchi, T.; Oishi, K.; Suzuki, A.; Fukumoto, K.; Inaba, K.; Baba, S.; Takehara, Y.; Konno, H. Pancreatic neuroendocrine cell tumor secreting parathyroid hormone-related protein and gastrin: Report of a case. Surg. Today 2010, 40, 1192–1196. [Google Scholar] [CrossRef]
- Demura, M.; Yoneda, T.; Wang, F.; Zen, Y.; Karashima, S.; Zhu, A.; Cheng, Y.; Yamagishi, M.; Takeda, Y. Ectopic production of parathyroid hormone in a patient with sporadic medullary thyroid cancer. Endocr. J. 2010, 57, 161–170. [Google Scholar] [CrossRef]
- Srirajaskanthan, R.; McStay, M.; Toumpanakis, C.; Meyer, T.; Caplin, M.E. Parathyroid hormone-related peptide-secreting pancreatic neuroendocrine tumours: Case series and literature review. Neuroendocrinology 2009, 89, 48–55. [Google Scholar] [CrossRef]
- Brzozowska, M.M.; Wolmarans, L.; Conaglen, J.V. Hypercalcaemia caused by a carcinoid tumour. Intern. Med. J. 2009, 39, 415–418. [Google Scholar] [CrossRef]
- van den Eynden, G.G.; Neyret, A.; Fumey, G.; Rizk-Rabin, M.; Vermeulen, P.B.; Bouizar, Z.; Body, J.-J.; Dirix, L.Y. PTHrP, calcitonin and calcitriol in a case of severe, protracted and refractory hypercalcemia due to a pancreatic neuroendocrine tumor. Bone 2007, 40, 1166–1171. [Google Scholar] [CrossRef]
- Barakat, M.T.; Ashrafian, H.; Todd, J.F.; Meeran, K.; Williams, G.R. Severe hypercalcaemia from secretion of parathyroid hormone-related peptide. Lancet Oncol. 2004, 5, 633–635. [Google Scholar] [CrossRef]
- Mullerpatan, P.M.; Joshi, S.R.; Shah, R.C.; Tampi, C.S.; Doctor, V.M.; Jagannath, P.; Modlin, I. Calcitonin-secreting tumor of the pancreas. Dig. Surg. 2004, 21, 321–324. [Google Scholar] [CrossRef]
- Abraham, P.; Ralston, S.H.; Hewison, M.; Fraser, W.D.; Bevan, J.S. Presentation of a PTHrP-secreting pancreatic neuroendocrine tumour, with hypercalcaemic crisis, pre-eclampsia, and renal failure. Postgrad. Med. J. 2002, 78, 752–753. [Google Scholar] [CrossRef]
- Clemens, P.; Gregor, M.; Lamberts, R. Pancreatic neuroendocrine tumor with extensive vascularisation and parathyroid hormone-related protein (PTHrP)--associated hypercalcemia of malignancy. Exp. Clin. Endocrinol. Diabetes 2001, 109, 378–385. [Google Scholar] [CrossRef]
- Papazachariou, I.M.; Virlos, I.T.; Williamson, R.C. Parathyroid hormone-related peptide in pancreatic neuroendocrine tumours associated with hypercalcaemia. HPB 2001, 3, 221–225. [Google Scholar] [CrossRef]
- Loh, K.-C.; Matthay, K.K.; Hoover, M.; Bracho, F.A.; Cortez, A.B.; Conte, F.A.; Albanese, C.T.; Miller, T.R.; Price, D.C.; Flores, A.J.; et al. Hypercalcemia in malignant paraganglioma due to parathyroid hormone-related protein. Horm. Res. 1998, 50, 217–221. [Google Scholar] [CrossRef]
- van de Loosdrecht, A.A.; van Bodegraven, A.A.; Sepers, J.M.; Sindram, J.W. Long-term follow-up of two patients with metastatic neuroendocrine tumours treated with octreotide. Neth. J. Med. 1998, 53, 118–123. [Google Scholar] [CrossRef]
- Mantzoros, C.S.; Suva, L.J.; Moses, A.C.; Spark, R. Intractable hypercalcaemia due to parathyroid hormone-related peptide secretion by a carcinoid tumour. Clin. Endocrinol. 1997, 46, 373–375. [Google Scholar] [CrossRef]
- Wu, T.J.; Lin, C.L.; Taylor, R.L.; Kvols, L.K.; Kao, P.C. Increased parathyroid hormone-related peptide in patients with hypercalcemia associated with islet cell carcinoma. Mayo Clin. Proc. 1997, 72, 1111–1115. [Google Scholar] [CrossRef]
- Mao, C.; Carter, P.; Schaefer, P.; Zhu, L.; Dominguez, J.M.; Hanson, D.J.; Appert, H.E.; Kim, K.; Howard, J.M. Malignant islet cell tumor associated with hypercalcemia. Surgery 1995, 117, 37–40. [Google Scholar] [CrossRef]
- Anthony, L.B.; May, M.E.; Oates, J.A. Case report: Lanreotide in the management of hypercalcemia of malignancy. Am. J. Med. Sci. 1995, 309, 312–314. [Google Scholar] [CrossRef]
- Ratcliffe, W.A.; Bowden, S.J.; Dunnet, F.P.; Hughes, S.; Emly, J.F.; Baker, J.T.; Pye, J.K.; Williams, C.P. Expression and processing of parathyroid hormone-related protein in a pancreatic endocrine cell tumour associated with hypercalcaemia. Clin. Endocrinol. 1994, 40, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; Noguchi, Y.; Matsukawa, H.; Kondo, J.; Matsumoto, A.; Nakatani, Y.; Kitamura, H.; Ito, T. Thymus carcinoid producing parathyroid hormone (PTH)-related protein: Report of a case. Surg. Today 1994, 24, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Mune, T.; Katakami, H.; Kato, Y.; Yasuda, K.; Matsukura, S.; Miura, K. Production and secretion of parathyroid hormone-related protein in pheochromocytoma: Participation of an alpha-adrenergic mechanism. J. Clin. Endocrinol. Metab. 1993, 76, 757–762. [Google Scholar] [PubMed]
- Williams, E.J.; Ratcliffe, W.A.; Stavri, G.T.; Stamatakis, J.D. Hypercalcaemia secondary to secretion of parathyroid hormone related protein from a somatostatinoma of the pancreas. Ann. Clin. Biochem. 1992, 29, 354–357. [Google Scholar] [CrossRef]
- Bridgewater, J.A.; Ratcliffe, W.A.; Bundred, N.J.; Owens, C.W. Malignant phaeochromocytoma and hypercalcaemia. Postgrad. Med. J. 1993, 69, 77–79. [Google Scholar] [CrossRef]
- Miraliakbari, B.A.; Asa, S.L.; Boudreau, S.F. Parathyroid hormone-like peptide in pancreatic endocrine carcinoma and adenocarcinoma associated with hypercalcemia. Hum. Pathol. 1992, 23, 884–887. [Google Scholar] [CrossRef]
- Tarver, D.S.; Birch, S.J. Case report: Life-threatening hypercalcaemia secondary to pancreatic tumour secreting parathyroid hormone-related protein—Successful control by hepatic arterial embolization. Clin. Radiol. 1992, 46, 204–205. [Google Scholar] [CrossRef]
- Mitlak, B.H.; Hutchison, J.S.; Kaufman, S.D.; Nussbaum, S.R. Parathyroid hormone-related peptide mediates hypercalcemia in an islet cell tumor of the pancreas. Horm. Metab. Res. 1991, 23, 344–346. [Google Scholar] [CrossRef]
- Bresler, L.; Boissel, P.; Conroy, T.; Grosdidier, J. Pancreatic islet cell carcinoma with hypercalcemia: Complete remission 5 years after surgical excision and chemotherapy. Am. J. Gastroenterol. 1991, 86, 635–638. [Google Scholar]
- Harrison, M.; James, N.; Broadley, K.; Bloom, S.R.; Armour, R.; Wimalawansa, S.; Heath, D.; Waxman, J. Somatostatin analogue treatment for malignant hypercalcaemia. BMJ 1990, 300, 1313–1314. [Google Scholar] [CrossRef][Green Version]
- Kimura, S.; Nishimura, Y.; Yamaguchi, K.; Nagasaki, K.; Shimada, K.; Uchida, H. A case of pheochromocytoma producing parathyroid hormone-related protein and presenting with hypercalcemia. J. Clin. Endocrinol. Metab. 1990, 70, 1559–1563. [Google Scholar] [CrossRef]
- Rizzoli, R.; Sappino, A.P.; Bonjour, J.P. Parathyroid hormone-related protein and hypercalcemia in pancreatic neuro-endocrine tumors. Int. J. Cancer 1990, 46, 394–398. [Google Scholar] [CrossRef]
- Dodwell, D.; Gurney, H.; Scarffe, H.; Abbas, S. Treatment of a pancreatic tumour secreting parathyroid hormone related protein. BMJ 1990, 300, 1653. [Google Scholar] [CrossRef][Green Version]
- Wynick, D.; Ratcliffe, W.A.; Heath, D.A.; Ball, S.; Barnard, M.; Bloom, S.R. Treatment of a malignant pancreatic endocrine tumour secreting parathyroid hormone related protein. BMJ 1990, 300, 1314–1315. [Google Scholar] [CrossRef][Green Version]
- Heitz, P.U.; Harder, F.; Haas, H.G.; Kloeppel, G. Tumor of the pancreas inducing hypercalcemia. Ultrastruct. Pathol. 1989, 13, 585–588. [Google Scholar] [CrossRef]
- Venkatesh, S.; Vassilopoulou-Sellin, R.; Samaan, N.A. Somatostatin analogue: Use in the treatment of vipoma with hypercalcemia. Am. J. Med. 1989, 87, 356–357. [Google Scholar] [CrossRef]
- Friesen, S.R. Update on the diagnosis and treatment of rare neuroendocrine tumors. Surg. Clin. North Am. 1987, 67, 379–393. [Google Scholar] [CrossRef]
- Sarfati, E.; Lavergne, A.; Gossot, D.; Fischer, D.; Dubost, C. Bronchial carcinoid tumor and hypercalcemia. Ann. Intern. Med. 1987, 106, 476–477. [Google Scholar] [CrossRef]
- Shetty, M.R. Pancreatic islet cell tumors. Surgery 1987, 101, 380. [Google Scholar]
- Vair, D.B.; Boudreau, S.F.; Reid, E.L. Pancreatic islet-cell neoplasia, with secretion of a parathormone-like substance and hypercalcemia. Can. J. Surg. 1987, 30, 108–110. [Google Scholar]
- Arps, H.; Dietel, M.; Schulz, A.; Janzarik, H.; Kloppel, G. Pancreatic endocrine carcinoma with ectopic PTH-production and paraneoplastic hypercalcaemia. Virchows Arch. A Pathol. Anat. Histopathol. 1986, 408, 497–503. [Google Scholar] [CrossRef]
- Grossman, E.; Knecht, A.; Holtzman, E.; Nussinovich, N.; Rosenthal, T. Uncommon presentation of pheochromocytoma: Case studies. Angiology 1985, 36, 759–765. [Google Scholar] [CrossRef]
- Baba, S.; Machida, K.; Ozaki, I.; Okushima, T.; Murabayashi, S.; Kamata, Y.; Imamura, K.; Takebe, K. A malignant pheochromocytoma with ileus, polyuria and hypercalcemia: A case of recurrence 17 years after the initial operation. Endocrinol. JPN 1985, 32, 337–345. [Google Scholar] [CrossRef]
- Loveridge, N.; Kent, G.N.; Heath, D.A.; Jones, E.L. Parathyroid hormone-like bioactivity in a patient with severe osteitis fibrosa cystica due to malignancy: Renotropic actions of a tumour extract as assessed by cytochemical bioassay. Clin. Endocrinol. 1985, 22, 135–146. [Google Scholar] [CrossRef]
- Shanberg, A.M.; Baghdassarian, R.; Tansey, L.A.; Bacon, D.; Greenberg, P.; Perley, M. Pheochromocytoma with hypercalcemia: Case report and review of literature. J. Urol. 1985, 133, 258–259. [Google Scholar] [CrossRef]
- Stewart, A.F.; Hoecker, J.L.; Mallette, L.E.; Segre, G.V.; Amatruda, T.T., Jr.; Vignery, A. Hypercalcemia in pheochromocytoma. Evidence for a novel mechanism. Ann. Intern. Med. 1985, 102, 776–779. [Google Scholar] [CrossRef]
- Rasbach, D.A.; Hammond, J.M. Pancreatic islet cell carcinoma with hypercalcemia. Primary hyperparathyroidism or humoral hypercalcemia of malignancy. Am. J. Med. 1985, 78, 337–342. [Google Scholar] [CrossRef]
- Fairhurst, B.J.; Shettar, S.P. Hypercalcaemia and phaeochromocytoma. Postgrad. Med. J. 1981, 57, 459–460. [Google Scholar] [CrossRef]
- Oberg, K.; Loof, L.; Bostrom, H.; Grimelius, L.; Fahrenkrug, J.; Lundqvist, G. Hypersecretion of calcitonin in patients with the Verner-Morrison syndrome. Scand. J. Gastroenterol. 1981, 16, 135–144. [Google Scholar]
- De Plaen, J.F.; Boemer, F.; van Ypersele De Strihou, C. Hypercalcaemic phaeochromocytoma. Br. Med. J. 1976, 2, 734. [Google Scholar] [CrossRef][Green Version]
- Ghose, R.R.; Winsey, H.S.; Jemmett, J.; Woodhead, J.S. Phaeochromocytoma and hypercalcaemia. Postgrad. Med. J. 1976, 52, 593–595. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gray, R.S.; Gillon, J. Normotensive phaeochromocytoma with hypercalcaemia: Correction after adrenalectomy. Br. Med. J. 1976, 1, 378. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cryer, P.E.; Hill, G.J., II. Pancreatic islet cell carcinoma with hypercalcemia and hypergastrinemia: Response to streptozotocin. Cancer 1976, 38, 2217–2221. [Google Scholar] [CrossRef]
- Deftos, L.J.; McMillan, P.J.; Sartiano, G.P.; Abuid, J.; Robinson, A.G. Simultaneous ectopic production of parathyroid hormone and calcitonin. Metabolism 1976, 25, 543–550. [Google Scholar] [CrossRef]
- Hirose, S.; Kobayashi, K.; Kajikawa, K.; Sawabu, N. A case of watery diarrhea, hypokalemia and hypercalcemia associated with nonulcerogenic islet cell tumor of the pancreas. Am. J. Gastroenterol. 1975, 64, 382–391. [Google Scholar]
- Kukreja, S.C.; Hargis, G.K.; Rosenthal, I.M.; Williams, G.A. Pheochromocytoma causing excessive parathyroid hormone production and hypercalcemia. Ann. Intern. Med. 1973, 79, 838–840. [Google Scholar] [CrossRef]
- DeWys, W.D.; Stoll, R.; Au, W.Y.; Salisnjak, M.M. Effects of streptozotocin on an islet cell carcinoma with hypercalcemia. Am. J. Med. 1973, 55, 671–676. [Google Scholar] [CrossRef]
- Swinton, N.W.; Clerkin, E.P., Jr.; Flint, L.D. Hypercalcemia and familial pheochromocytoma. Correction after adrenalectomy. Ann. Intern. Med. 1972, 76, 455–457. [Google Scholar] [CrossRef]
- Lopes, V.M.; Reis, D.D.; Cunha, A.B. Islet-cell adenoma of the pancreas with reversible watery diarrhea and hypokalemia. WDHA syndrome. Am. J. Gastroenterol. 1970, 53, 17–35. [Google Scholar]
- Murray, J.S.; Paton, R.R.; Pope, C.E., 2nd. Pancreatic tumor associated with flushing and diarrhea. Report of a case. New Engl. J. Med. 1961, 26, 436–439. [Google Scholar] [CrossRef]
- Mozar, A.; Lin, H.; Williams, K.; Chin, C.; Li, R.; Kondegowda, N.G.; Stewart, A.F.; Garcia-Ocaña, A.; Vasavada, R.C. Parathyroid Hormone-Related Peptide (1–36) Enhances Beta Cell Regeneration and Increases Beta Cell Mass in a Mouse Model of Partial Pancreatectomy. PLoS ONE 2016, 11, e0158414. [Google Scholar] [CrossRef]
- Bhatia, V.; Cao, Y.; Ko, T.C.; Falzon, M. Parathyroid Hormone-Related Protein Interacts With the Transforming Growth Factor-beta/Bone Morphogenetic Protein-2/Gremlin Signaling Pathway to Regulate Proinflammatory and Profibrotic Mediators in Pancreatic Acinar and Stellate Cells. Pancreas 2016, 45, 659–670. [Google Scholar] [CrossRef]
- Wysolmerski, J.J. Parathyroid hormone-related protein: An update. J. Clin. Endocrinol. Metab. 2012, 97, 2947–2956. [Google Scholar] [CrossRef]
- McCauley, L.K.; Martin, T.J. Twenty-five years of PTHrP progress: From cancer hormone to multifunctional cytokine. J. Bone Miner. Res. 2012, 27, 1231–1239. [Google Scholar] [CrossRef]
- Mundy, G.R.; Edwards, J.R. PTH-related peptide (PTHrP) in hypercalcemia. J. Am. Soc. Nephrol. 2008, 19, 672–675. [Google Scholar] [CrossRef]
- Walker, R.E.; Lawson, M.A.; Buckle, C.H.; Snowden, J.A.; Chantry, A.D. Myeloma bone disease: Pathogenesis, current treatments and future targets. Br. Med. Bull. 2014, 111, 117–138. [Google Scholar] [CrossRef][Green Version]
- Uchimura, K.; Mokuno, T.; Nagasaka, A.; Hayakawa, N.; Kato, T.; Yamazaki, N.; Kobayashi, T.; Nagata, M.; Kotake, M.; Itoh, M.; et al. Lung cancer associated with hypercalcemia induced by concurrently elevated parathyroid hormone and parathyroid hormone-related protein levels. Metabolism 2002, 51, 871–875. [Google Scholar] [CrossRef]
- Weiss, E.S.; Doty, J.; Brock, M.V.; Halvorson, L.; Yang, S.C. A case of ectopic parathyroid hormone production by a pulmonary neoplasm. J. Thorac. Cardiovasc. Surg. 2006, 131, 923–924. [Google Scholar] [CrossRef][Green Version]
- Chen, L.; Dinh, T.A.; Haque, A. Small cell carcinoma of the ovary with hypercalcemia and ectopic parathyroid hormone production. Arch. Pathol. Lab. Med. 2005, 129, 531–533. [Google Scholar] [CrossRef]
- Donovan, P.J.; Sundac, L.; Pretorius, C.J.; d’Emden, M.C.; McLeod, D.S. Calcitriol-mediated hypercalcemia: Causes and course in 101 patients. J. Clin. Endocrinol. Metab. 2013, 98, 4023–4029. [Google Scholar] [CrossRef]
- Seymour, J.F.; Gagel, R.F. Calcitriol: The major humoral mediator of hypercalcemia in Hodgkin’s disease and non-Hodgkin’s lymphomas. Blood 1993, 82, 1383–1394. [Google Scholar] [CrossRef]
- Mudde, A.H.; Berg, H.V.D.; Boshuis, P.G.; Breedveld, F.C.; Markusse, H.M.; Kluin, P.M.; Bijvoet, O.L.M.; Papapoulos, S.E. Ectopic production of 1,25-dihydroxyvitamin D by B-cell lymphoma as a cause of hypercalcemia. Cancer 1987, 59, 1543–1546. [Google Scholar] [CrossRef]
- Hewison, M.; Kantorovich, V.; Liker, H.R.; Van Herle, A.J.; Cohan, P.; Zehnder, D.; Adams, J. Vitamin D-mediated hypercalcemia in lymphoma: Evidence for hormone production by tumor-adjacent macrophages. J. Bone Miner. Res. 2003, 18, 579–582. [Google Scholar] [CrossRef]
- Zandee, W.T.; Brabander, T.; Blažević, A.; Minczeles, N.S.; Feelders, R.A.; de Herder, W.W.; Hofland, J. Peptide Receptor Radionuclide Therapy With 177Lu-DOTATATE for Symptomatic Control of Refractory Carcinoid Syndrome. J. Clin. Endocrinol. Metab. 2021, 106, e3665–e3672. [Google Scholar] [CrossRef]
- Parghane, R.V.; Mitra, A.; Bannore, T.U.; Rakshit, S.; Banerjee, S.; Basu, S. Initial clinical evaluation of indigenous (90)Y-DOTATATE in sequential duo-PRRT approach ((177)Lu-DOTATATE and (90)Y-DOTATATE) in neuroendocrine tumors with large bulky disease: Observation on tolerability, (90)Y-DOTATATE post- PRRT imaging characteristics (bremsstrahlung and PETCT) and early adverse effects. World J. Nucl. Med. 2021, 20, 73–81. [Google Scholar]
- Raymond, L.M.; Korzun, T.; Kardosh, A.; Kolbeck, K.J.; Pommier, R.; Mittra, E.S. The State of Peptide Receptor Radionuclide Therapy and Its Sequencing among Current Therapeutic Options for Gastroenteropancreatic Neuroendocrine Tumors. Neuroendocrinology 2021, 111, 1086–1098. [Google Scholar] [CrossRef]
- Pusceddu, S.; Prinzi, N.; Tafuto, S.; Ibrahim, T.; Filice, A.; Brizzi, M.P.; Panzuto, F.; Baldari, S.; Grana, C.M.; Campana, D.; et al. Association of Upfront Peptide Receptor Radionuclide Therapy with Progression-Free Survival Among Patients With Enteropancreatic Neuroendocrine Tumors. JAMA Netw. Open. 2022, 5, e220290. [Google Scholar] [CrossRef]
- Thakker, R.V.; Newey, P.J.; Walls, G.V.; Bilezikian, J.; Dralle, H.; Ebeling, P.R.; Melmed, S.; Sakurai, A.; Tonelli, F.; Brandi, M.L. Clinical practice guidelines for multiple endocrine neoplasia type 1 (MEN1). J. Clin. Endocrinol. Metab. 2012, 97, 2990–3011. [Google Scholar] [CrossRef]
- Wells, S.A., Jr.; Asa, S.; Dralle, H.; Elisei, R.; Evans, D.B.; Gagel, R.F.; Lee, N.Y.; Machens, A.; Moley, J.F.; Pacini, F.; et al. Revised American Thyroid Association guidelines for the management of medullary thyroid carcinoma. Thyroid 2015, 25, 567–610. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).