

Five-Year Cardiovascular Outcomes after Infective Endocarditis in Patients with versus without Drug Use History

 , , ,
, , , 

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Source
2.2. Cohorts and Sample Selection
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
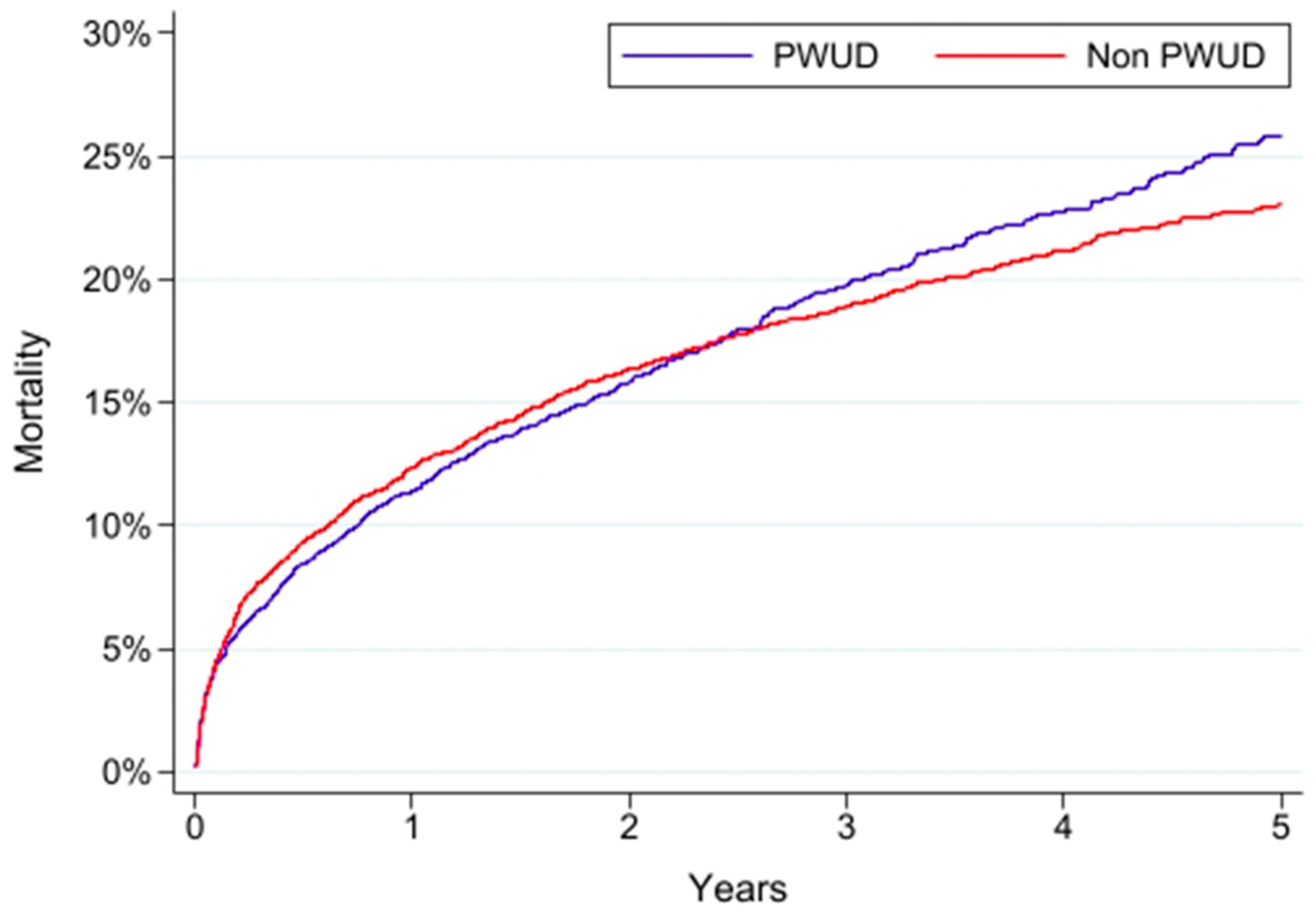
3.2. Five-Year Mortality
3.3. Five-Year Cardiovascular Events
3.4. Secondary Analyses
3.4.1. Surgical and Medical Treatment
3.4.2. Sex
3.4.3. Race
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taquet, M.; Geddes, J.R.; Husain, M.; Luciano, S.; Harrison, P.J. 6-month neurological and psychiatric outcomes in 236 379 survivors of COVID-19: A retrospective cohort study using electronic health records. Lancet Psychiatry 2021, 8, 416–427. [Google Scholar] [CrossRef]
- Topaloglu, U.; Palchuk, M.B. Using a Federated Network of Real-World Data to Optimize Clinical Trials Operations. JCO Clin. Cancer Inform. 2018, 2, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Parcha, V.; Booker, K.S.; Kalra, R.; Kuranz, S.; Berra, L.; Arora, G.; Arora, P. A retrospective cohort study of 12,306 pediatric COVID-19 patients in the United States. Sci. Rep. 2021, 11, 10231. [Google Scholar] [CrossRef] [PubMed]
- Evans, L.; London, J.W.; Palchuk, M.B. Assessing real-world medication data completeness. J. Biomed Inform. 2021, 119, 103847. [Google Scholar] [CrossRef] [PubMed]
- Stapff, M.P. Using real world data to assess cardiovascular outcomes of two antidiabetic treatment classes. World J. Diabetes 2018, 9, 252–257. [Google Scholar] [CrossRef]
- Benchimol, E.I.; Smeeth, L.; Guttmann, A.; Harron, K.; Moher, D.; Petersen, I.; Sørensen, H.T.; von Elm, E.; Langan, S.M. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015, 12, e1001885. [Google Scholar] [CrossRef]
- Kadri, A.N.; Wilner, B.; Hernandez, A.V.; Nakhoul, G.; Chahine, J.; Griffin, B.; Pettersson, G.; Grimm, R.; Navia, J.; Gordon, S.; et al. Geographic Trends, Patient Characteristics, and Outcomes of Infective Endocarditis Associated With Drug Abuse in the United States From 2002 to 2016. J. Am. Heart Assoc. 2019, 8, e012969. [Google Scholar] [CrossRef]
- Cooper, H.L.; Brady, J.E.; Ciccarone, D.; Tempalski, B.; Gostnell, K.; Friedman, S.R. Nationwide increase in the number of hospitalizations for illicit injection drug use-related infective endocarditis. Clin. Infect. Dis. 2007, 45, 1200–1203. [Google Scholar] [CrossRef]
- Marks, L.R.; Nolan, N.S.; Jiang, L.; Muthulingam, D.; Liang, S.Y.; Durkin, M.J. Use of ICD-10 Codes for Identification of Injection Drug Use–Associated Infective Endocarditis Is Nonspecific and Obscures Critical Findings on Impact of Medications for Opioid Use Disorder. Open Forum Infect. Dis. 2020, 7, ofaa414. [Google Scholar] [CrossRef]
- McGrew, K.M.; Garwe, T.; Jafarzadeh, S.R.; Drevets, D.A.; Zhao, Y.D.; Williams, M.B.; Carabin, H. Misclassification Error-Adjusted Prevalence of Injection Drug Use Among Infective Endocarditis Hospitalizations in the United States: A Serial Cross-Sectional Analysis of the 2007-2016 National Inpatient Sample. Am. J. Epidemiol. 2021, 190, 588–599. [Google Scholar] [CrossRef]
- McGrew, K.M.; Carabin, H.; Garwe, T.; Jafarzadeh, S.R.; Williams, M.B.; Zhao, Y.D.; Drevets, D.A. Validity of ICD-based algorithms to estimate the prevalence of injection drug use among infective endocarditis hospitalizations in the absence of a reference standard. Drug Alcohol Depend. 2020, 209, 107906. [Google Scholar] [CrossRef] [PubMed]
- Tan, C.; Hansen, M.; Cohen, G.; Boyle, K.; Daneman, N.; Adhikari, N.K. Accuracy of administrative data for identification of patients with infective endocarditis. Int. J. Cardiol. 2016, 224, 162–164. [Google Scholar] [CrossRef]
- Austin, P.C. Primer on statistical interpretation or methods report card on propensity-score matching in the cardiology literature from 2004 to 2006: A systematic review. Circ. Cardiovasc. Qual. Outcomes 2008, 1, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Kim, H.J.; Lonjon, G.; Zhu, Y.; written on behalf of AME Big-Data Clinical Trial Collaborative Group. Balance diagnostics after propensity score matching. Ann. Transl. Med. 2019, 7, 16. [Google Scholar] [CrossRef]
- Harris, C.M.; Khaliq, W.; Albaeni, A.; Norris, K.C. The influence of race in older adults with infective endocarditis. BMC Infect. Dis. 2020, 20, 146. [Google Scholar] [CrossRef]
- Khan, M.Z. Racial and Gender Trends in Infective Endocarditis Related Deaths in United States (2004–2017). Am. J. Cardiol. 2020, 129, 125–126. [Google Scholar] [CrossRef]
- Sambola, A.; Fernández-Hidalgo, N.; Almirante, B.; Roca, I.; González-Alujas, T.; Serra, B.; Pahissa, A.; García-Dorado, D.; Tornos, P. Sex differences in native-valve infective endocarditis in a single tertiary-care hospital. Am. J. Cardiol. 2010, 106, 92–98. [Google Scholar] [CrossRef]
- Pettersson, G.B.; Coselli, J.S.; Pettersson, G.B.; Coselli, J.S.; Hussain, S.T.; Griffin, B.; Blackstone, E.H.; Gordon, S.M.; LeMaire, S.A.; Woc-Colburn, L.E. 2016 The American Association for Thoracic Surgery (AATS) consensus guidelines: Surgical treatment of infective endocarditis: Executive summary. J. Thorac. Cardiovasc. Surg. 2017, 153, 1241–1258.e1229. [Google Scholar] [CrossRef]
- Prendergast, B.D.; Tornos, P. Surgery for infective endocarditis: Who and when? Circulation 2010, 121, 1141–1152. [Google Scholar] [CrossRef]
- Haibe-Kains, B.; Desmedt, C.; Sotiriou, C.; Bontempi, G. A comparative study of survival models for breast cancer prognostication based on microarray data: Does a single gene beat them all? Bioinformatics 2008, 24, 2200–2208. [Google Scholar] [CrossRef]
- Hall, R.; Shaughnessy, M.; Boll, G.; Warner, K.; Boucher, H.W.; Bannuru, R.R.; Wurcel, A.G. Drug Use and Postoperative Mortality Following Valve Surgery for Infective Endocarditis: A Systematic Review and Meta-analysis. Clin. Infect. Dis. 2019, 69, 1120–1129. [Google Scholar] [CrossRef] [PubMed]
- Straw, S.; Baig, M.W.; Gillott, R.; Wu, J.; Witte, K.K.; O’Regan D, J.; Sandoe, J.A.T. Long-term Outcomes Are Poor in Intravenous Drug Users Following Infective Endocarditis, Even After Surgery. Clin. Infect. Dis. 2020, 71, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Rodger, L.; Shah, M.; Shojaei, E.; Hosseini, S.; Koivu, S.; Silverman, M. Recurrent Endocarditis in Persons Who Inject Drugs. Open Forum Infect. Dis. 2019, 6, ofz396. [Google Scholar] [CrossRef] [PubMed]
- Mocchegiani, R.; Nataloni, M. Complications of infective endocarditis. Cardiovasc. Hematol. Disord. Drug Targets 2009, 9, 240–248. [Google Scholar] [CrossRef]
- Pericàs, J.M.; Hernández-Meneses, M.; Muñoz, P.; Martínez-Sellés, M.; Álvarez-Uria, A.; de Alarcón, A.; Gutiérrez-Carretero, E.; Goenaga, M.A.; Zarauza, M.J.; Falces, C.; et al. Characteristics and Outcome of Acute Heart Failure in Infective Endocarditis: Focus on Cardiogenic Shock. Clin. Infect. Dis. 2021, 73, 765–774. [Google Scholar] [CrossRef]
- Shih, C.J.; Chu, H.; Chao, P.W.; Lee, Y.J.; Kuo, S.C.; Li, S.Y.; Tarng, D.C.; Yang, C.Y.; Yang, W.C.; Ou, S.M.; et al. Long-term clinical outcome of major adverse cardiac events in survivors of infective endocarditis: A nationwide population-based study. Circulation 2014, 130, 1684–1691. [Google Scholar] [CrossRef]
- Clarelin, A.; Rasmussen, M.; Olaison, L.; Ragnarsson, S. Comparing right- and left sided injection-drug related infective endocarditis. Sci. Rep. 2021, 11, 1177. [Google Scholar] [CrossRef]
- Miró, J.M.; Moreno, A.; Mestres, C.A. Infective Endocarditis in Intravenous Drug Abusers. Curr. Infect. Dis. Rep. 2003, 5, 307–316. [Google Scholar] [CrossRef]
- Esse, K.; Fossati-Bellani, M.; Traylor, A.; Martin-Schild, S. Epidemic of illicit drug use, mechanisms of action/addiction and stroke as a health hazard. Brain Behav. 2011, 1, 44–54. [Google Scholar] [CrossRef]
- Nakhaee, S.; Ghasemi, S.; Karimzadeh, K.; Zamani, N.; Alinejad-Mofrad, S.; Mehrpour, O. The effects of opium on the cardiovascular system: A review of side effects, uses, and potential mechanisms. Subst. Abus. Treat. Prev. Policy 2020, 15, 30. [Google Scholar] [CrossRef] [Green Version]
- Krishnamoorthy, S.; Lip, G.Y.; Lane, D.A. Alcohol and illicit drug use as precipitants of atrial fibrillation in young adults: A case series and literature review. Am. J. Med. 2009, 122, 851–856.e853. [Google Scholar] [CrossRef]
- Fonseca, A.C.; Ferro, J.M. Drug Abuse and Stroke. Curr. Neurol. Neurosci. Rep. 2013, 13, 325. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Ejiofor, J.I.; Yammine, M.; Ando, M.; Camuso, J.M.; Youngster, I.; Nelson, S.B.; Kim, A.Y.; Melnitchouk, S.I.; Rawn, J.D.; et al. Surgical outcomes of infective endocarditis among intravenous drug users. J. Thorac. Cardiovasc. Surg. 2016, 152, 832–841.e831. [Google Scholar] [CrossRef] [PubMed]
- Goodman-Meza, D.; Weiss, R.E.; Gamboa, S.; Gallegos, A.; Bui, A.A.T.; Goetz, M.B.; Shoptaw, S.; Landovitz, R.J. Long term surgical outcomes for infective endocarditis in people who inject drugs: A systematic review and meta-analysis. BMC Infect. Dis. 2019, 19, 918. [Google Scholar] [CrossRef] [PubMed]
- Nguemeni Tiako, M.J.; Mszar, R.; Brooks, C., 2nd; Mahmood, S.U.B.; Mori, M.; Geirsson, A.; Weimer, M.B. Cardiac Surgeons’ Treatment Approaches for Infective Endocarditis Based on Patients’ Substance Use History. Semin. Thorac. Cardiovasc. Surg. 2020, 33, 703–709. [Google Scholar] [CrossRef]
- Dohmen, P.M.; Binner, C.; Mende, M.; Daviewala, P.; Etz, C.D.; Borger, M.A.; Misfeld, M.; Eifert, S.; Mohr, F.W. Gender-Based Long-Term Surgical Outcome in Patients with Active Infective Aortic Valve Endocarditis. Med. Sci. Monit. 2016, 22, 2520–2527. [Google Scholar] [CrossRef]
- Moss, R.; Munt, B. Injection drug use and right sided endocarditis. Heart 2003, 89, 577–581. [Google Scholar] [CrossRef]
- Suntai, Z.D.; Lee, L.H.; Leeper, J.D. Racial Disparities in Substance Use Treatment Completion Among Older Adults. Innov. Aging 2020, 4, igaa051. [Google Scholar] [CrossRef]
- Nguemeni Tiako, M.J.; Hong, S.; Bin Mahmood, S.U.; Mori, M.; Mangi, A.; Yun, J.; Juthani-Mehta, M.; Geirsson, A. Inconsistent Addiction Treatment for Patients Undergoing Cardiac Surgery for Injection Drug Use-associated Infective Endocarditis. J. Addict. Med. 2020, 14, e350–e354. [Google Scholar] [CrossRef]
- Thakarar, K.; Rokas, K.E.; Lucas, F.L.; Powers, S.; Andrews, E.; DeMatteo, C.; Mooney, D.; Sorg, M.H.; Valenti, A.; Cohen, M. Mortality, morbidity, and cardiac surgery in Injection Drug Use (IDU)-associated versus non-IDU infective endocarditis: The need to expand substance use disorder treatment and harm reduction services. PLoS ONE 2019, 14, e0225460. [Google Scholar] [CrossRef] [Green Version]
- Shah, M.; Wong, R.; Ball, L.; Puka, K.; Tan, C.; Shojaei, E.; Koivu, S.; Silverman, M. Risk factors of infective endocarditis in persons who inject drugs. Harm. Reduct. J. 2020, 17, 35. [Google Scholar] [CrossRef] [PubMed]
- Barocas, J.A.; Eftekhari Yazdi, G.; Savinkina, A.; Nolen, S.; Savitzky, C.; Samet, J.H.; Englander, H.; Linas, B.P. Long-term infective endocarditis mortality associated with injection opioid use in the United States: A modeling study. Clin. Infect. Dis. 2020, 73, e3661–e3669. [Google Scholar] [CrossRef] [PubMed]
- Rosenthal, E.S.; Karchmer, A.W.; Theisen-Toupal, J.; Castillo, R.A.; Rowley, C.F. Suboptimal Addiction Interventions for Patients Hospitalized with Injection Drug Use-Associated Infective Endocarditis. Am. J. Med. 2016, 129, 481–485. [Google Scholar] [CrossRef] [PubMed]
- Yucel, E.; Bearnot, B.; Paras, M.L.; Zern, E.K.; Dudzinski, D.M.; Soong, C.P.; Jassar, A.S.; Rosenfield, K.; Lira, J.; Lambert, E.; et al. Diagnosis and Management of Infective Endocarditis in People Who Inject Drugs: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2022, 79, 2037–2057. [Google Scholar] [CrossRef]
- Hawk, M.; Coulter, R.W.S.; Egan, J.E.; Fisk, S.; Reuel Friedman, M.; Tula, M.; Kinsky, S. Harm reduction principles for healthcare settings. Harm. Reduct. J. 2017, 14, 70. [Google Scholar] [CrossRef]
- Eckhardt, B.; Aponte-Meledez, Y.; Fung, C.; Kapadia, S.; Davis, L.; Smith, M.; Mateu-Gelabert, P.; Marks, K. Accessible Care Intervention for Engaging People Who Inject Illicit Drugs in Hepatitis C Virus Care: Preliminary Results from a Randomized Clinical Trial. Open Forum Infect. Dis. 2019, 6, S161. [Google Scholar] [CrossRef]
- Muncan, B.; Jordan, A.E.; Perlman, D.C.; Frank, D.; Ompad, D.C.; Walters, S.M. Acceptability and Effectiveness of Hepatitis C Care at Syringe Service Programs for People Who Inject Drugs in New York City. Subst. Use Misuse 2021, 56, 728–737. [Google Scholar] [CrossRef]
- Brothers, T.D.; Fraser, J.; MacAdam, E.; Morgan, B.; Francheville, J.; Nidumolu, A.; Cheung, C.; Hickcox, S.; Saunders, D.; O’Donnell, T.; et al. Implementation and evaluation of a novel, unofficial, trainee-organized hospital addiction medicine consultation service. Subst. Abus. 2020, 42, 433–437. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Before Matching | After Matching | |||||
|---|---|---|---|---|---|---|
| Characteristic (ICD-10/CPT Code) | PWUD (N = 15,573) | Non-PWUD (N = 49,521) | SMD | PWUD (N = 7132) | Non-PWUD (N = 7132) | SMD |
| Demographics | ||||||
| Age, years | 39.2 ± 11.2 | 44.9 ± 12.8 | 0.476 | 41.3 ± 11.5 | 42.0 ± 13.2 | 0.055 |
| Male, % | 51.4 | 52.6 | 0.024 | 52.2 | 52.2 | 0.001 |
| Race, % | ||||||
| White | 75.3 | 67.1 | 0.183 | 70.4 | 70.4 | 0.001 |
| Black or African American | 15.6 | 19.1 | 0.094 | 19.8 | 21.0 | 0.030 |
| Hispanic or Latino, % | 6.2 | 8.9 | 0.104 | 8.0 | 8.3 | 0.008 |
| Body mass index, kg/m2 | 26.7 ± 7.1 | 29.5 ± 7.9 | 0.378 | 27.8 ± 7.6 | 28.0 ± 7.8 | 0.022 |
| Comorbidities, % | ||||||
| Cardiovascular and Related | ||||||
| Essential hypertension (I10) | 35.1 | 35.6 | 0.011 | 39.6 | 44.4 | 0.097 |
| Diabetes mellitus (E08–E13) | 17.6 | 18.4 | 0.020 | 21.3 | 24.2 | 0.069 |
| Overweight, obesity (E65–E68) | 15.5 | 17.7 | 0.059 | 19.0 | 20.9 | 0.047 |
| Ischemic heart disease (I20–I25) | 21.2 | 16.4 | 0.125 | 21.8 | 24.3 | 0.058 |
| Previous cardiac surgery (02 procedure codes) | 23.1 | 12.4 | 0.284 | 19.2 | 21.1 | 0.048 |
| Prosthetic heart valve (Z95.2) * | 7.5 | 6.4 | 0.044 | 5.9 | 6.8 | 0.039 |
| Chronic rheumatic heart diseases (I05–I09) | 17.2 | 9.8 | 0.218 | 12.1 | 13.4 | 0.039 |
| Cerebrovascular disease (I60–I69) | 13.3 | 8.3 | 0.161 | 11.7 | 13.5 | 0.055 |
| Atrial fibrillation and flutter (I48) | 8.1 | 9.4 | 0.044 | 9.1 | 10.4 | 0.046 |
| Heart failure (I50) | 19.1 | 15.5 | 0.097 | 19.7 | 22.0 | 0.056 |
| Pulmonary heart disease (I26–I28) | 23.2 | 8.7 | 0.402 | 15.3 | 16.6 | 0.035 |
| Congenital cardiovascular malformations (Q20–Q28) | 6.0 | 8.9 | 0.109 | 5.9 | 6.2 | 0.012 |
| Respiratory | ||||||
| Chronic lower respiratory diseases (J40–J47) | 25.5 | 14.7 | 0.271 | 24.8 | 27.2 | 0.055 |
| Influenza and pneumonia (J09–J18) | 28.1 | 12.6 | 0.395 | 23.6 | 25.3 | 0.040 |
| Renal | ||||||
| Acute kidney failure and chronic kidney disease (N17-N19) | 32.1 | 19.3 | 0.296 | 29.0 | 32.0 | 0.065 |
| Other diseases of the urinary system (N30–N39) | 21.6 | 12.1 | 0.258 | 20.6 | 22.2 | 0.039 |
| Other disorders of kidney and ureter (N25–N29) | 13.2 | 9.5 | 0.117 | 14.0 | 15.6 | 0.044 |
| Infectious | ||||||
| Human immunodeficiency virus (B20) | 3.2 | 1.1 | 0.148 | 2.8 | 3.1 | 0.023 |
| Viral hepatitis (B15–B19) | 34.3 | 2.9 | 0.882 | 13.6 | 13.0 | 0.016 |
| Skin and soft tissue infections (L00–L08) | 37.3 | 11.9 | 0.617 | 30.1 | 32.4 | 0.049 |
| Bacterial and viral infectious agents (B95–B97) | 37.5 | 12.7 | 0.597 | 26.0 | 27.9 | 0.042 |
| Mycoses (B35–B49) | 15.8 | 8.1 | 0.237 | 14.3 | 16.0 | 0.048 |
| Hematologic and Oncologic | ||||||
| Aplastic anemia and bone marrow failure syndromes (D60–D64) | 38.9 | 22.0 | 0.373 | 33.7 | 37.5 | 0.079 |
| Coagulopathies (D65–D69) | 21.1 | 10.5 | 0.292 | 17.5 | 19.6 | 0.054 |
| Nutritional anemias (D50–D53) | 15.4 | 8.5 | 0.215 | 14.4 | 15.7 | 0.038 |
| Personal history of malignant neoplasm (Z85) | 4.8 | 4.4 | 0.017 | 5.9 | 6.7 | 0.034 |
| Mental Health | ||||||
| Mood disorders (F30–F39) | 41.6 | 13.6 | 0.661 | 32.7 | 35.5 | 0.058 |
| Anxiety disorders (F40–F48) | 41.1 | 14.2 | 0.631 | 31.9 | 33.6 | 0.037 |
| Schizophrenia and non-mood psychotic disorders (F20–F29) | 6.5 | 1.4 | 0.263 | 4.6 | 4.5 | 0.007 |
| Poisoning/overdose (T36–T50) | 28.4 | 7.0 | 0.584 | 21.3 | 22.6 | 0.030 |
| Long term opiate use (Z79.891) | 18.6 | 10.1 | 0.244 | 18.8 | 20.9 | 0.052 |
| Alcohol related disorders (F10) | 17.7 | 3.6 | 0.471 | 12.0 | 12.9 | 0.025 |
| Cannabis related disorders (F12) | 16.9 | 1.2 | 0.568 | 7.2 | 6.4 | 0.028 |
| Nicotine dependence (F17) | 57.6 | 11.8 | 1.096 | 39.1 | 41.0 | 0.039 |
| Other | ||||||
| Pregnancy, childbirth, and the puerperium (O00–O9A) | 8.8 | 2.7 | 0.263 | 6.3 | 6.6 | 0.011 |
| Health hazards due to socioeconomic circumstances (Z55–Z65) | 13.4 | 2.2 | 0.425 | 7.3 | 7.2 | 0.005 |
| PWUD (N = 7132) | Non-PWUD (N = 7132) | |||
|---|---|---|---|---|
| Outcome | Cumulative Incidence | Cumulative Incidence | HR (95% CI) | Log-Rank p |
| All-cause mortality | ||||
| Cumulative 5-year | 25.7% | 23.0% | 1.04 (0.96–1.13) | 0.363 |
| <1 Year | 11.6% | 12.2% | 0.95 (0.85–1.05) | 0.303 |
| 1–3 Years | 9.2% | 7.5% | 1.29 (1.02–1.42) | 0.032 |
| 3–5 Years | 7.3% | 5.1% | 1.39 (1.05–1.86) | 0.020 |
| VT/VF | 6.6% | 5.8% | 1.13 (0.94–1.36) | 0.211 |
| Myocardial infarction | 10.0% | 7.0% | 1.37 (1.16–1.62) | <0.001 |
| Heart failure | 19.3% | 15.2% | 1.22 (1.08–1.37) | 0.002 |
| Atrial fibrillation/flutter | 10.1% | 10.5% | 0.90 (0.77–1.04) | 0.154 |
| Ischemic stroke | 8.3% | 6.3% | 1.32 (1.12–1.57) | 0.001 |
| Intracranial hemorrhage | 4.1% | 2.8% | 1.38 (1.08–1.76) | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Muncan, B.; Abboud, A.; Papamanoli, A.; Jacobs, M.; McLarty, A.J.; Skopicki, H.A.; Kalogeropoulos, A.P. Five-Year Cardiovascular Outcomes after Infective Endocarditis in Patients with versus without Drug Use History. J. Pers. Med. 2022, 12, 1562. https://doi.org/10.3390/jpm12101562
Muncan B, Abboud A, Papamanoli A, Jacobs M, McLarty AJ, Skopicki HA, Kalogeropoulos AP. Five-Year Cardiovascular Outcomes after Infective Endocarditis in Patients with versus without Drug Use History. Journal of Personalized Medicine. 2022; 12(10):1562. https://doi.org/10.3390/jpm12101562
Chicago/Turabian StyleMuncan, Brandon, Alan Abboud, Aikaterini Papamanoli, Mark Jacobs, Allison J. McLarty, Hal A. Skopicki, and Andreas P. Kalogeropoulos. 2022. "Five-Year Cardiovascular Outcomes after Infective Endocarditis in Patients with versus without Drug Use History" Journal of Personalized Medicine 12, no. 10: 1562. https://doi.org/10.3390/jpm12101562
APA StyleMuncan, B., Abboud, A., Papamanoli, A., Jacobs, M., McLarty, A. J., Skopicki, H. A., & Kalogeropoulos, A. P. (2022). Five-Year Cardiovascular Outcomes after Infective Endocarditis in Patients with versus without Drug Use History. Journal of Personalized Medicine, 12(10), 1562. https://doi.org/10.3390/jpm12101562