
Biological Predictors of Treatment Response in Adult Attention Deficit Hyperactivity Disorder (ADHD): A Systematic Review

 ,
,  , ,
, , 

Abstract
:1. Introduction
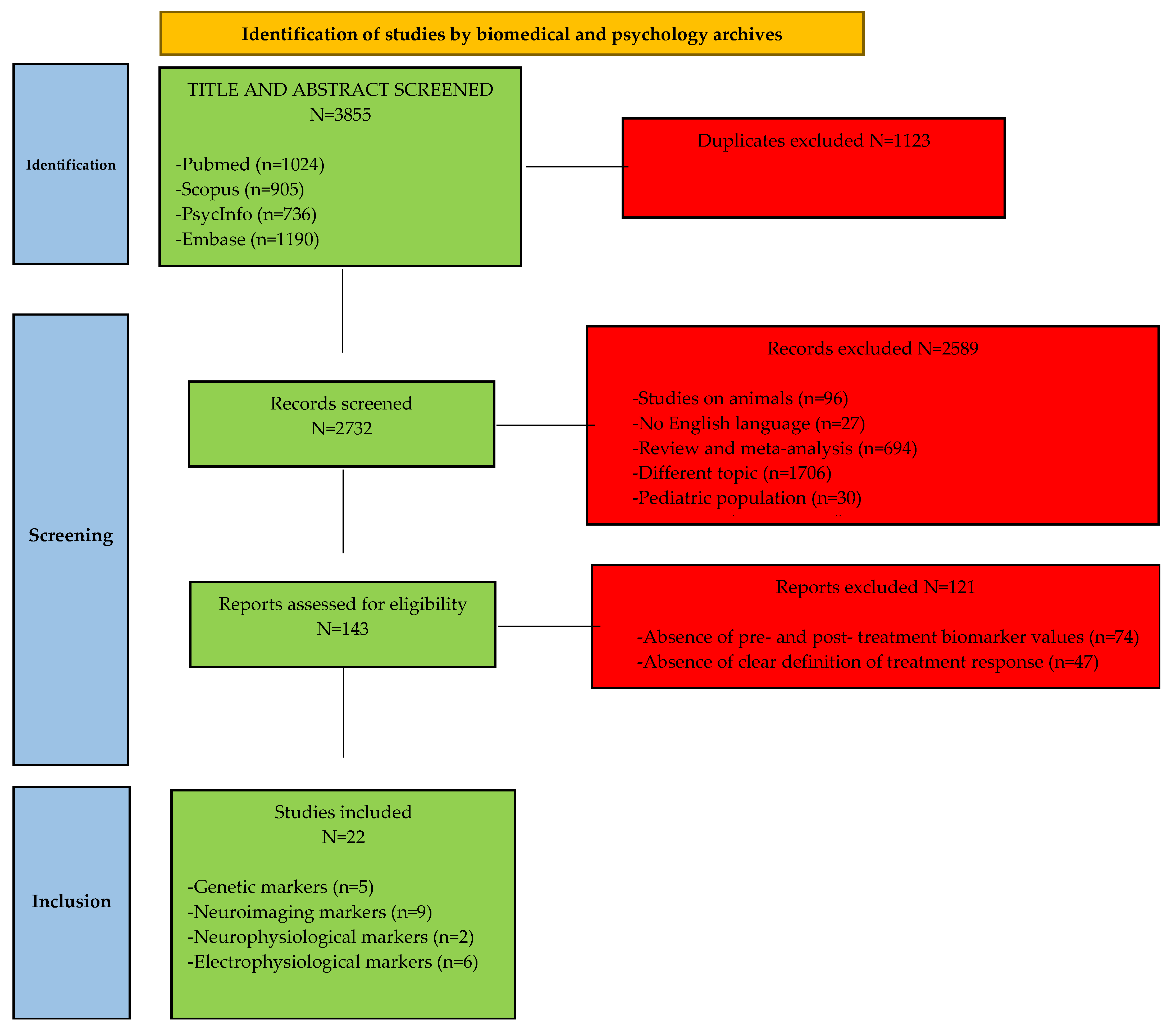
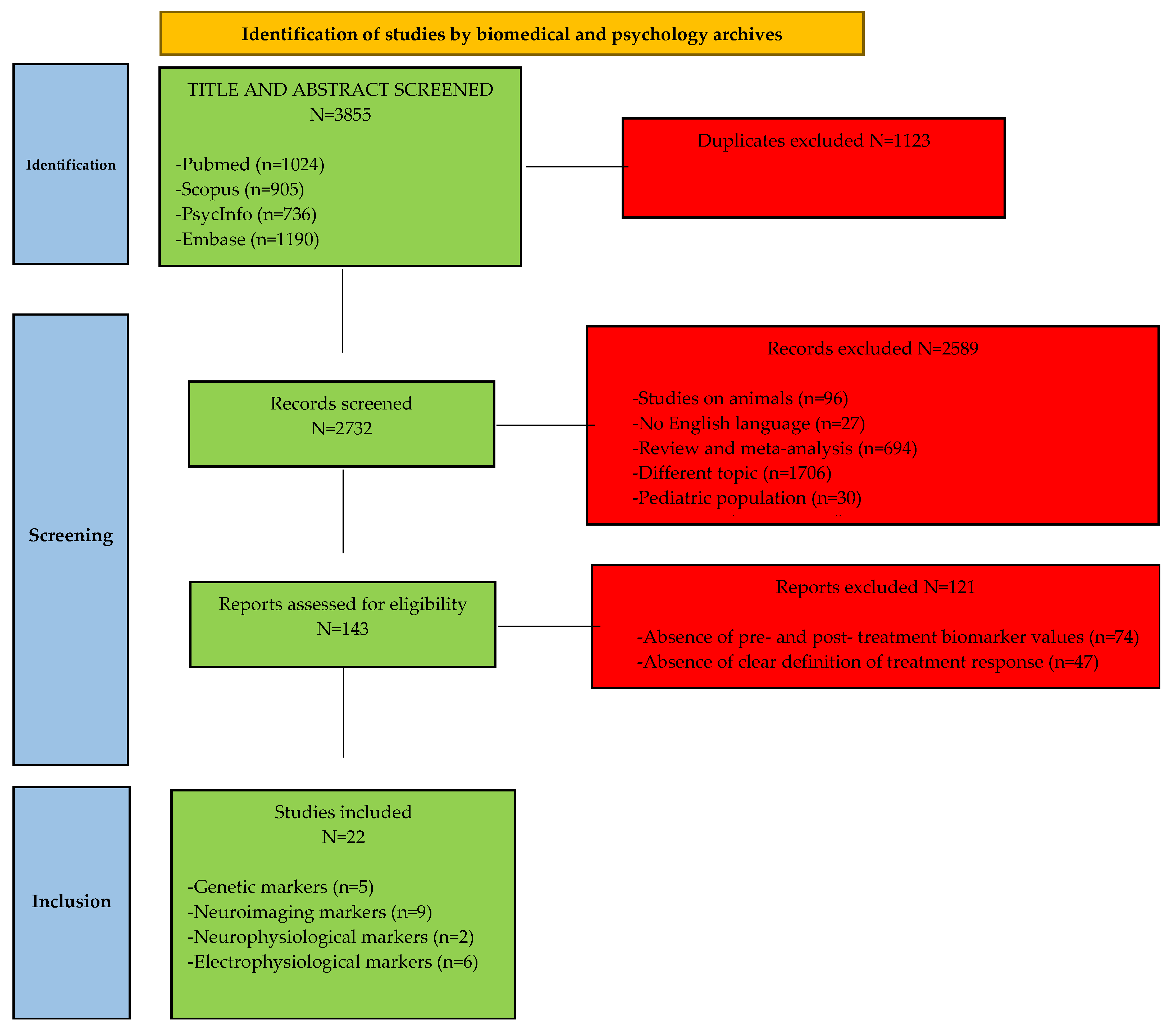
2. Methods
3. Results
3.1. Genetic Markers

{kind=link}
| Reference | Markers | Design | N | HC | Sex (% Male) | Mean Age ± SD | Drug-Free/Naive | Treatment | Treatment Duration | Treatment Response | Results | ES (d) | Quality of the Study * |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Da Silva et al., 2018 [31] | SNARE complex-related genes | Prospective | 272 | / | 55.9% | 33.95 ± 10.56 | Free | MPH | ≥30 days | ↓ ≥30% SNAP-IV ↓ CGI ≤ 2 points | SYT1-rs2251214 associated with: (1) short-term response (p = 0.006); (2) treatment persistence (p = 0.002) | (1) 0.478 (2) 0.291 | 1 |
| Hegvik et al., 2016 [32] | ADRA2A | Observational | 564 | / | 48.0% | 34.11 ± 10.0 | / | MPH | variable | Options: - Very good - Good - Has had effect, but discontinued due to side effects in 2 questionnaires ** | rs1800544 in ADRA2A (p = 0.033) associated with treatment response | 0.320 | 2 |
| Contini et al., 2012 [33] | SLC6A4 HTR1B TPH2 DBH DRD4 COMT SNAP25 | Observational | 136 | 7 | 70.0% | 35.0 ± 11.0 | Free | MPH | 30 days | ↓ SNAP-IV | NS | N/A | 1 |
| Contini et al., 2011 [34] | ADRA2A | Observational | 165 | / | 54.5% | 35.0 ± 11.0 | / | MPH | 30 days | ↓ ≥30% SNAP-IV ↓ CGI ≤ 2 points | Three ADRA2A polymorphisms not associated with treatment response (p = 0.55, p = 0.34, p = 0.73 respectively) | 0.159, 0.237, and 0.083, respectively | 1 |
| Mick et al., 2006 [35] | DAT1 | RCT | 66 | 40 | 58.0% | 36.9 ± 9.1 35.1 ± 6.9 33.3 ± 6.7 | / | MPH | 6 weeks | CGI: much/very much improved + ↓ ≥30% AISRS | DAT1 VNTR not associated with treatment response (p = 0.90) | 0.041 | 1 |
Conclusions
3.2. Neuroimaging Markers
| Reference | Markers | Brain Imaging Technique | Design | N | HC | Sex (% Male) | Mean Age ± SD | Drug-Free/Naive | Treatment | Treatment Duration | Treatment Response | Results | ES (d) | Quality of the Study * |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Chang et al., 2021 [38] | Volume of left putamen and precuneus | fMRI (T1-weighted images) | Machine learning comparison: good responders (n = 63) versus poor responders (n = 16) | 79 | / | 54.0% | 18.0 ± 10.0 | Naive | MPH | 1 month | CGI: much/very much improved | Poor responders: (1) smaller regional GM volumes in the left putamen (p = 0.010); (2) higher volumes in the right (p = 0.025); (3) left (p = 0.031) precuneus | (1) 0.651 (2) 0.655 (3) 0.548 | 2 |
| Sugimoto et al., 2021 [39] | Regional brain activity | NIRS | Prospective interventional: near-infrared spectroscopy examinations during a go/no-go task pre- and post-treatment | 31 | / | 61.3% | 31.2 ± 8.6 | Free | ATX | 8 weeks | ↓ CAARS; ADHD test program | ↑ PFC activity associated with severity of clinical symptoms before treatment in the group of non-responders | N/A | 2 |
| Sethi et al., 2018 [40] | Substantia nigra/ventral tegmental area, ventral striatum | fMRI (T2-weighted images) | RCT | 30 | 30 | 63.3% | 33.7 ± 9.5 | / | D-AMP/MPH | ≥2 months (suspended 2 days before the test) | N/A | ADHD patients in treatment showed a change in signalling of left ventral striatum (p = 0.042) | 1.67 | 1 |
| Fan et al., 2017 [41] | Inhibitory control visual processing (Stroop fMRI and CANTAB) | fMRI | RCT | 24 | 12 | 71.4% | 28.9 ± 7.8 | Naive | ATX | 8 weeks | ↓ CGI ↓ ASRS | Pre-treatment anterior cingulate activation improvement of clinical symptoms (p < 0.05) | N/A | 2 |
| Volkow et al., 2012 [42] | Dopamine release changes (PET) | PET scans | Prospective, single-blind | 20 | / | 40.0% | 32.0 ± 6.0 | Naive | MPH | 12 months | ↓ CAARS | Responders: ↑ DA in ventral striatum | N/A | 2 |
| Bush et al., 2008 [43] | Increased fMRI activation in the daMCC and other frontoparietal regions involved in attention (MSIT) | fMRI | RCT | 11 | 10 | 63.6% | 29.5 ± 5.9 | Free | MPH | 6 weeks | ↓ ADHD ISRS ↓ CGI 1 or 2 points | Degree of daMCC activation was related to treatment response | 1.084 | 2 |
| La Fougère et al., 2006 [44] | Striatal DAT captation | SPECT | CT | 22 | 14 | 50.0% | 37.8 ± 11.0 | Free | MPH | 10 weeks | ↓ CGI | Poor response: pre-treatment ↓ striatal DAT binding (p = 0.04) | 2.334 | 2 |
| Krause et al., 2005 [45] | DAT availability | SPECT | CT, single-blind | 18 | 14 | 55.6% | 39.5 ± 11.1 | Naive | MPH | 10 weeks | ↓ CGI | Among the group of responders, all patients had high DAT availability prior to therapy; all except one of non-responders presented a low DAT availability before treatment | 2.491 | 2 |
| Schweitzer et al., 2003 [46] | - Posterior cerebellum - Precentral gyri - Left caudate nucleus - Right claustrum | PET | Prospective, open-label | 10 | / | 100.0% | 31.5 ± 8.2 | / | MPH | 3 weeks | ↓ CGI ↓ ADHD-RS | Change in clinical symptoms after the treatment was negatively correlated with rCBF increases in the midbrain, cerebellar vermis, and the precentral and middle frontal gyri in the off-MPH condition | N/A | 1 |
3.2.1. Structural Neuroimaging Studies
3.2.2. Dopamine Levels and Regional Cerebral Blood Flow
3.2.3. Dopamine Transporters
3.2.4. Task-Based Functional Neuroimaging
3.2.5. Conclusions
3.3. Neurophysiological Markers
| Reference | Markers | Design | N | HC | Sex (% Male) | Mean Age ± SD | Drug-Free/Naive | Treatment | Treatment Duration | Treatment Response | Results | ES (d) | Quality of the Study * |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Duval et al., 2021 [47] | Antisaccade task performance | Prospective | 97 | 50 | 49.5% | 35.1 ± 9.5 | Naive | MPH | 6 months | ↓ ASRS ↓ CGI | Low percentage of direction errors after the first MPH dose predicted remission after 6 months of pharmacotherapy (p = 0.001) | 0.973 | 2 |
| Biederman et al., 2011 [48] | Attentional networks (Attention Network Test); Inhibitory control (Stop Signal Test) | Cross-sectional RCT | 87 | 146 | 40.0% | 34.7 ± 9.2 | / | MPH | 6 weeks | CGI: much/very much improved (≤2) + ↓ ≥30% AISRS | EFDs: (1) do not moderate the response to MPH (p = 0.35); (2) are not associated with response to MPH (0.794) | (1) N/A (2) 0.255 | 1 |
Conclusions
3.4. Electrophysiological Markers
| Reference | Markers | Design | N | HC | Sex (% Male) | Mean Age ± SD | Drug-Free/Naive | Treatment | Treatment Duration | Treatment Response | Results | ES (d) | Quality of the Study * |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alyagon et al., 2020 [49] | Alpha and low-gamma power | Semi-blinded RCT | 15 | AC: 14 Sham treatment: 14 | 13.3% | 26.6 ± 0.7 | Naive | rTMS | 3 weeks | ↓ ≥25% CAARS (total and subscales); ↓ BAARS-IV; ↓ BRIEF-A; ↓ BDI | Treatment response associated with: (1)↓ α activity (p = 0.035) (2) ↑ low-γ (p = 0.012) (3) ↓ α + ↑ low-γ (p = 0.0001) | (1) 1.352 (2) 2.200 (3) 3.695 | 1 |
| Werner et al., 2020 [50] | Retinal background noise | Longitudinal | 20 | 21 | 55.0% | 30.5 ± 10.0 | Naive | MPH | 7 weeks | ↓ CAARS | ↓ retinal background noise at follow-up after treatment in ADHD patients (p = 0.035); no changes in HC | 0.847 | 2 |
| Strauss et al., 2020 [51] | Brain arousal instability during resting-state EEG (Vigilance Algorithm Leipzig (VIGALL 2.1)) | Open-label | 28 | / | 28.6% | 36.6 ± 11.6 | Free | MPH | 4 weeks | ↓ CAARS | Arousal stability at baseline predicted MPH response (p = 0.027) | N/A | 2 |
| Cooper et al., 2014 [52] | VLF-EEG oscillation | Longitudinal case-control | 17 | 34 | 100.0% | 28.7 ± 7.7 | Free | MPH | Mean: 9.4 months | ↑ CPT OX | VLF-EEG activity and omission errors reduced in cases after treatment to the same level as healthy controls | N/A | 2 |
| Leuchter et al., 2014 [53] | qEEG absolute and relative power, cordance | RCT | 14 | 15 | N/A | 18–30 | Free | ATX | 12 weeks | ↓ CAARS; ↑ AAQOL-29 | Responders and non-responders to ATX differed significantly in week 1 theta band left tempoparietal cordance, with atomoxetine responders showing the lowest and non-responders the highest values (p = 0.015) | 1.503 | 2 |
| Skirrow et al., 2015 [54] | Frontal theta activity | Open-label | 21 | 36 | 100.0% | 30.0 ± 10.4 | Free | MPH | Mean: 3.5 months | ↑ CPT OX/SART | Normalisation of frontal theta activity pattern after treatment (p = 0.02) | N/A | 2 |
Conclusions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fayyad, J.; Sampson, N.A.; Hwang, I.; Adamowski, T.; Aguilar-Gaxiola, S.; Al-Hamzawi, A.; Andrade, L.H.; Borges, G.; de Girolamo, G.; Florescu, S.; et al. The descriptive epidemiology of DSM-IV Adult ADHD in the World Health Organization World Mental Health Surveys. Atten. Defic. Hyperact. Disord. 2017, 9, 47–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sibley, M.H.; Arnold, L.E.; Swanson, J.M.; Hechtman, L.T.; Kennedy, T.M.; Owens, E.; Molina, B.S.G.; Jensen, P.S.; Hinshaw, S.P.; Royet, A.; et al. Variable Patterns of Remission From ADHD in the Multimodal Treatment Study of ADHD. Am. J. Psychiatry 2022, 179, 142–151. [Google Scholar] [CrossRef]
- Ginsberg, Y.; Quintero, J.; Anand, E.; Casillas, M.; Upadhyaya, H.P. Underdiagnosis of attention-deficit/hyperactivity disorder in adult patients: A review of the literature. Prim. Care Companion CNS Disord. 2014, 16, 23591. [Google Scholar] [CrossRef] [PubMed]
- Almeida Montes, L.G.; Hernández García, A.O.; Ricardo-Garcell, J. ADHD prevalence in adult outpatients with nonpsychotic psychiatric illnesses. J. Atten. Disord. 2007, 11, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Capuzzi, E.; Capellazzi, M.; Caldiroli, A.; Cova, F.; Auxilia, A.M.; Rubelli, P.; Tagliabue, I.; Zanvit, F.G.; Peschi, G.; Buoli, M.; et al. Screening for ADHD Symptoms among Criminal Offenders: Exploring the Association with Clinical Features. Healthcare 2022, 10, 180. [Google Scholar] [CrossRef]
- Skokauskas, N.; Hitoshi, K.; Shuji, H.; Frodl, T. Neuroimaging markers for the prediction of treatment response to Methylphenidate in ADHD. Eur. J. Paediatr. Neurol. 2013, 17, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Serati, M.; Barkin, J.L.; Orsenigo, G.; Altamura, A.C.; Buoli, M. Research Review: The role of obstetric and neonatal complications in childhood attention deficit and hyperactivity disorder-a systematic review. J. Child Psychol. Psychiatry 2017, 58, 1290–1300. [Google Scholar] [CrossRef]
- Arnsten, A.F. Fundamentals of attention-deficit/hyperactivity disorder: Circuits and pathways. J. Clin. Psychiatry 2006, 67 (Suppl. 8), 7–12. [Google Scholar]
- Hodgkins, P.; Shaw, M.; Coghill, D.; Hechtman, L. Amfetamine and methylphenidate medications for attention-deficit/hyperactivity disorder: Complementary treatment options. Eur. Child. Adolesc. Psychiatry 2012, 21, 477–492. [Google Scholar] [CrossRef] [Green Version]
- Buoli, M.; Serati, M.; Cahn, W. Alternative pharmacological strategies for adult ADHD treatment: A systematic review. Expert Rev. Neurother. 2016, 16, 131–144. [Google Scholar] [CrossRef]
- Faltinsen, E.; Zwi, M.; Castells, X.; Gluud, C.; Simonsen, E.; Storebø, O.J. Updated 2018 NICE guideline on pharmacological treatments for people with ADHD: A critical look. BMJ Evid. Based Med. 2019, 24, 99–102. [Google Scholar] [CrossRef] [PubMed]
- McGough, J.J. Treatment Controversies in Adult ADHD. Am. J. Psychiatry 2016, 173, 960–966. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cortese, S.; Adamo, N.; Del Giovane, C.; Mohr-Jensen, C.; Hayes, A.J.; Carucci, S.; Atkinson, L.Z.; Tessari, L.; Banaschewski, T.; Coghill, D.; et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: A systematic review and network meta-analysis. Lancet Psychiatry 2018, 5, 727–738. [Google Scholar] [CrossRef] [Green Version]
- Mészáros, A.; Czobor, P.; Bálint, S.; Komlósi, S.; Simon, V.; Bitter, I. Pharmacotherapy of adult attention deficit hyperactivity disorder (ADHD): A meta-analysis. Int. J. Neuropsychopharmacol. 2009, 12, 1137–1147. [Google Scholar] [CrossRef] [Green Version]
- Faraone, S.V.; Glatt, S.J. A comparison of the efficacy of medications for adult attention-deficit/hyperactivity disorder using meta-analysis of effect sizes. J. Clin. Psychiatry 2010, 71, 754–763. [Google Scholar] [CrossRef] [Green Version]
- Kooij, J.J.S.; Bijlenga, D.; Salerno, L.; Jaeschke, R.; Bitter, I.; Balázs, J.; Thome, J.; Dom, G.; Kasper, S.; Nunes Filipe, C.; et al. Updated European Consensus Statement on diagnosis and treatment of adult ADHD. Eur. Psychiatry 2019, 56, 14–34. [Google Scholar] [CrossRef] [PubMed]
- Greenhill, L.L.; Pliszka, S.; Dulcan, M.K.; Bernet, W.; Arnold, V.; Beitchman, J.; Benson, R.S.; Bukstein, O.; Kinlan, J.; McClellan, J.; et al. American Academy of Child and Adolescent Psychiatry. Practice parameter for the use of stimulant medications in the treatment of children, adolescents, and adults. J. Am. Acad. Child Adolesc. Psychiatry 2022, 41 (Suppl. 2), 26S–49S. [Google Scholar] [CrossRef]
- Retz, W.; Retz-Junginger, P. Prediction of methylphenidate treatment outcome in adults with attention-deficit/hyperactivity disorder (ADHD). Eur. Arch. Psychiatry Clin. Neurosci. 2014, 264 (Suppl. 1), S35–S43. [Google Scholar] [CrossRef]
- Pan, P.Y.; Bölte, S. The association between ADHD and physical health: A co-twin control study. Sci. Rep. 2020, 10, 22388. [Google Scholar] [CrossRef]
- Bonvicini, C.; Faraone, S.V.; Scassellati, C. Attention-deficit hyperactivity disorder in adults: A systematic review and meta-analysis of genetic, pharmacogenetic and biochemical studies. Mol. Psychiatry 2016, 21, 1643. [Google Scholar] [CrossRef] [Green Version]
- Rucklidge, J.J.; Johnstone, J.; Gorman, B.; Boggis, A.; Frampton, C.M. Moderators of treatment response in adults with ADHD treated with a vitamin-mineral supplement. Prog. Neuropsychopharmacol. Biol. Psychiatry 2014, 50, 163–171. [Google Scholar] [CrossRef] [PubMed]
- Scassellati, C.; Bonvicini, C.; Faraone, S.V.; Gennarelli, M. Biomarkers and attention-deficit/hyperactivity disorder: A systematic review and meta-analyses. J. Am. Acad. Child Adolesc. Psychiatry 2012, 51, 1003–1019.e20. [Google Scholar] [CrossRef] [PubMed]
- Clemow, D.B.; Walker, D.J. The potential for misuse and abuse of medications in ADHD: A review. Postgrad. Med. 2014, 126, 64–81. [Google Scholar] [CrossRef]
- Furczyk, K.; Thome, J. Adult ADHD and suicide. Atten. Defic. Hyperact. Disord. 2014, 6, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Habel, L.A.; Cooper, W.O.; Sox, C.M.; Chan, K.A.; Fireman, B.H.; Arbogast, P.G.; Cheetham, T.C.; Quinn, V.P.; Dublin, S.; Boudreau, D.M.; et al. ADHD medications and risk of serious cardiovascular events in young and middle-aged adults. JAMA 2011, 306, 2673–2683. [Google Scholar] [CrossRef] [PubMed]
- Bushe, C.; Sobanski, E.; Coghill, D.; Berggren, L.; De Bruyckere, K.; Leppämäki, S. Post Hoc Analysis of Potential Predictors of Response to Atomoxetine for the Treatment of Adults with Attention-Deficit/Hyperactivity Disorder using an Integrated Database. CNS Drugs 2016, 30, 317–334. [Google Scholar] [CrossRef]
- Christiansen, H.; Chavanon, M.L.; Hirsch, O.; Schmidt, M.H.; Meyer, C.; Müller, A.; Rumpf, H.J.; Grigorev, I.; Hoffmann, A. Use of machine learning to classify adult ADHD and other conditions based on the Conners’ Adult ADHD Rating Scales. Sci. Rep. 2020, 10, 18871. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Armijo-Olivo, S.; Stiles, C.R.; Hagen, N.A.; Biondo, P.D.; Cummings, G.G. Assessment of study quality for systematic reviews: A comparison of the Cochrane Collaboration Risk of Bias Tool and the Effective Public Health Practice Project Quality Assessment Tool: Methodological research. J. Eval. Clin. Pract. 2012, 18, 12–18. [Google Scholar] [CrossRef] [PubMed]
- da Silva, B.S.; Cupertino, R.B.; Rovaris, D.L.; Schuch, J.B.; Kappel, D.B.; Müller, D.; Bandeira, C.E.; Victor, M.M.; Karam, R.G.; Mota, N.R.; et al. Exocytosis-related genes and response to methylphenidate treatment in adults with ADHD. Mol. Psychiatry 2018, 23, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Hegvik, T.A.; Jacobsen, K.K.; Fredriksen, M.; Zayats, T.; Haavik, J. A candidate gene investigation of methylphenidate response in adult attention-deficit/hyperactivity disorder patients: Results from a naturalistic study. J. Neural Transm. 2016, 123, 859–865. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Contini, V.; Victor, M.M.; Bertuzzi, G.P.; Salgado, C.A.; Picon, F.A.; Grevet, E.H.; Rohde, L.A.; Belmonte-de-Abreu, P.; Bau, C.H. No significant association between genetic variants in 7 candidate genes and response to methylphenidate treatment in adult patients with ADHD. J. Clin. Psychopharmacol. 2012, 32, 820–823. [Google Scholar] [CrossRef] [PubMed]
- Contini, V.; Victor, M.M.; Cerqueira, C.C.; Polina, E.R.; Grevet, E.H.; Salgado, C.A.; Karam, R.G.; Vitola, E.S.; Belmonte-de-Abreu, P.; Bau, C.H. Adrenergic á2A receptor gene is not associated with methylphenidate response in adults with ADHD. Eur. Arch. Psychiatry Clin. Neurosci. 2011, 261, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Mick, E.; Biederman, J.; Spencer, T.; Faraone, S.V.; Sklar, P. Absence of association with DAT1 polymorphism and response to methylphenidate in a sample of adults with ADHD. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2006, 141B, 890–894. [Google Scholar] [CrossRef] [Green Version]
- Johansson, S.; Halleland, H.; Halmøy, A.; Jacobsen, K.K.; Landaas, E.T.; Dramsdahl, M.; Fasmer, O.B.; Bergsholm, P.; Lundervold, A.J.; Gillberg, C.; et al. Genetic analyses of dopamine related genes in adult ADHD patients suggest an association with the DRD5-microsatellite repeat, but not with DRD4 or SLC6A3 VNTRs. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2008, 147B, 1470–1475. [Google Scholar] [CrossRef]
- Halmøy, A.; Fasmer, O.B.; Gillberg, C.; Haavik, J. Occupational outcome in adult ADHD: Impact of symptom profile, comorbid psychiatric problems, and treatment: A cross-sectional study of 414 clinically diagnosed adult ADHD patients. J. Atten. Disord. 2009, 13, 175–187. [Google Scholar] [CrossRef] [Green Version]
- Chang, J.C.; Lin, H.Y.; Lv, J.; Tseng, W.I.; Gau, S.S. Regional brain volume predicts response to methylphenidate treatment in individuals with ADHD. BMC Psychiatry 2021, 21, 26. [Google Scholar] [CrossRef]
- Sugimoto, A.; Suzuki, Y.; Yoshinaga, K.; Orime, N.; Hayashi, T.; Egawa, J.; Ono, S.; Sugai, T.; Someya, T. Influence of Atomoxetine on Relationship Between ADHD Symptoms and Prefrontal Cortex Activity During Task Execution in Adult Patients. Front. Hum. Neurosci. 2021, 15, 755025. [Google Scholar] [CrossRef]
- Sethi, A.; Voon, V.; Critchley, H.D.; Cercignani, M.; Harrison, N.A. A neurocomputational account of reward and novelty processing and effects of psychostimulants in attention deficit hyperactivity disorder. Brain 2018, 141, 1545–1557. [Google Scholar] [CrossRef] [Green Version]
- Fan, L.Y.; Chou, T.L.; Gau, S.S. Neural correlates of atomoxetine improving inhibitory control and visual processing in Drug-naïve adults with attention-deficit/hyperactivity disorder. Hum. Brain Mapp. 2017, 38, 4850–4864. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Wang, G.J.; Tomasi, D.; Kollins, S.H.; Wigal, T.L.; Newcorn, J.H.; Telang, F.W.; Fowler, J.S.; Logan, J.; Wong, C.T.; et al. Methylphenidate-elicited dopamine increases in ventral striatum are associated with long-term symptom improvement in adults with attention deficit hyperactivity disorder. J. Neurosci. 2012, 32, 841–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bush, G.; Spencer, T.J.; Holmes, J.; Shin, L.M.; Valera, E.M.; Seidman, L.J.; Makris, N.; Surman, C.; Aleardi, M.; Mick, E.; et al. Functional magnetic resonance imaging of methylphenidate and placebo in attention-deficit/hyperactivity disorder during the multi-source interference task. Arch. Gen. Psychiatry 2008, 65, 102–114. [Google Scholar] [CrossRef] [Green Version]
- la Fougère, C.; Krause, J.; Krause, K.H.; Josef Gildehaus, F.; Hacker, M.; Koch, W.; Hahn, K.; Tatsch, K.; Dresel, S. Value of 99mTc-TRODAT-1 SPECT to predict clinical response to methylphenidate treatment in adults with attention deficit hyperactivity disorder. Nucl. Med. Commun. 2006, 27, 733–737. [Google Scholar] [CrossRef]
- Krause, J.; la Fougère, C.; Krause, K.H.; Ackenheil, M.; Dresel, S.H. Influence of striatal dopamine transporter availability on the response to methylphenidate in adult patients with ADHD. Eur. Arch. Psychiatry Clin. Neurosci. 2005, 255, 428–431. [Google Scholar] [CrossRef]
- Schweitzer, J.B.; Lee, D.O.; Hanford, R.B.; Tagamets, M.A.; Hoffman, J.M.; Grafton, S.T.; Kilts, C.D. A positron emission tomography study of methylphenidate in adults with ADHD: Alterations in resting blood flow and predicting treatment response. Neuropsychopharmacology 2003, 28, 967–973. [Google Scholar] [CrossRef]
- Duval, F.; Erb, A.; Mokrani, M.C.; Weiss, T.; Carcangiu, R. First-Dose Methylphenidate-Induced Changes in the Anti-Saccade Task Performance and Outcome in Adults with Attention-Deficit/Hyperactivity Disorder. Psychiatr. Res. Clin. Pract. 2021, 3, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Biederman, J.; Mick, E.; Fried, R.; Wilner, N.; Spencer, T.J.; Faraone, S.V. Are stimulants effective in the treatment of executive function deficits? Results from a randomized double blind study of OROS-methylphenidate in adults with ADHD. Eur. Neuropsychopharmacol. 2011, 21, 508–515. [Google Scholar] [CrossRef]
- Alyagon, U.; Shahar, H.; Hadar, A.; Barnea-Ygael, N.; Lazarovits, A.; Shalev, H.; Zangen, A. Alleviation of ADHD symptoms by non-invasive right prefrontal stimulation is correlated with EEG activity. Neuroimage Clin. 2020, 26, 102206. [Google Scholar] [CrossRef]
- Werner, A.L.; Tebartz van Elst, L.; Ebert, D.; Friedel, E.; Bubl, A.; Clement, H.W.; Lukaèin, R.; Bach, M.; Bubl, E. Normalization of increased retinal background noise after ADHD treatment: A neuronal correlate. Schizophr. Res. 2020, 219, 77–83. [Google Scholar] [CrossRef]
- Strauß, M.; Reif, A.; Ulke, C.; Paucke, M.; Sander, C.; Hegerl, U.; Weber, H.; Heupel, J.; Kopf, J.; Kittel-Schneider, S. Is brain arousal regulation a predictor of response to psychostimulant therapy in adult ADHD patients? Eur. Arch. Psychiatry Clin. Neurosci. 2020, 270, 1073–1076. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.E.; Skirrow, C.; Tye, C.; McLoughlin, G.; Rijsdijk, F.; Banaschweski, T.; Brandeis, D.; Kuntsi, J.; Asherson, P. The effect of methylphenidate on very low frequency electroencephalography oscillations in adult ADHD. Brain Cogn. 2014, 86, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Leuchter, A.F.; McGough, J.J.; Korb, A.S.; Hunter, A.M.; Glaser, P.E.; Deldar, A.; Durell, T.M.; Cook, I.A. Neurophysiologic predictors of response to atomoxetine in young adults with attention deficit hyperactivity disorder: A pilot project. J. Psychiatr. Res. 2014, 54, 11–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skirrow, C.; McLoughlin, G.; Banaschewski, T.; Brandeis, D.; Kuntsi, J.; Asherson, P. Normalisation of frontal theta activity following methylphenidate treatment in adult attention-deficit/hyperactivity disorder. Eur. Neuropsychopharmacol. 2015, 25, 85–94. [Google Scholar] [CrossRef] [PubMed]
- Edvinsson, D.; Ekselius, L. Six-year outcome in subjects diagnosed with attention-deficit/hyperactivity disorder as adults. Eur. Arch. Psychiatry Clin. Neurosci. 2018, 268, 337–347. [Google Scholar] [CrossRef] [Green Version]
- Luciano, M.; Hagenaars, S.P.; Davies, G.; Hill, W.D.; Clarke, T.K.; Shirali, M.; Harris, S.E.; Marioni, R.E.; Liewald, D.C.; Fawns-Ritchie, C.; et al. Association analysis in over 329,000 individuals identifies 116 independent variants influencing neuroticism. Nat. Genet. 2019, 51, 577. [Google Scholar] [CrossRef]
- Liu, Y.S.; Dai, X.; Wu, W.; Yuan, F.F.; Gu, X.; Chen, J.G.; Zhu, L.Q.; Wu, J. The Association of SNAP25 Gene Polymorphisms in Attention Deficit/Hyperactivity Disorder: A Systematic Review and Meta-Analysis. Mol. Neurobiol. 2017, 54, 2189–2200. [Google Scholar] [CrossRef]
- Cupertino, R.B.; Schuch, J.B.; Bandeira, C.E.; da Silva, B.S.; Rovaris, D.L.; Kappel, D.B.; Contini, V.; Salatino-Oliveira, A.; Vitola, E.S.; Karam, R.G.; et al. Replicated association of Synaptotagmin (SYT1) with ADHD and its broader influence in externalizing behaviors. Eur. Neuropsychopharmacol. 2017, 27, 239–247. [Google Scholar] [CrossRef]
- Robison, R.J.; Reimherr, F.W.; Gale, P.D.; Marchant, B.K.; Williams, E.D.; Soni, P.; Halls, C.; Strong, R.E. Personality disorders in ADHD Part 2: The effect of symptoms of personality disorder on response to treatment with OROS methylphenidate in adults with ADHD. Ann. Clin. Psychiatry 2010, 22, 94–102. [Google Scholar]
- Andrews, G.D.; Lavin, A. Methylphenidate increases cortical excitability via activation of alpha-2 noradrenergic receptors. Neuropsychopharmacology 2006, 31, 594–601. [Google Scholar] [CrossRef] [Green Version]
- Holland, J.; Sayal, K. Relative age and ADHD symptoms, diagnosis and medication: A systematic review. Eur. Child Adolesc. Psychiatry 2019, 28, 1417–1429. [Google Scholar] [CrossRef] [Green Version]
- Shingai, Y.; Tateno, A.; Arakawa, R.; Sakayori, T.; Kim, W.; Suzuki, H.; Okubo, Y. Age-related decline in dopamine transporter in human brain using PET with a new radioligand [18F]FE-PE2I. Ann. Nucl. Med. 2014, 28, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Alonso-Gonzalez, A.; Calaza, M.; Rodriguez-Fontenla, C.; Carracedo, A. Gene-based analysis of ADHD using PASCAL: A biological insight into the novel associated genes. BMC Med. Genom. 2019, 12, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Gong, Q.; Sweeney, J.A.; Biswal, B.B. Progress in psychoradiology, the clinical application of psychiatric neuroimaging. Br. J. Radiol. 2019, 92, 20181000. [Google Scholar] [CrossRef] [PubMed]
- Takamatsu, Y.; Hagino, Y.; Sato, A.; Takahashi, T.; Nagasawa, S.Y.; Kubo, Y.; Mizuguchi, M.; Uhl, G.R.; Sora, I.; Ikeda, K. Improvement of learning and increase in dopamine level in the frontal cortex by methylphenidate in mice lacking dopamine transporter. Curr. Mol. Med. 2015, 15, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Morón, J.A.; Brockington, A.; Wise, R.A.; Rocha, B.A.; Hope, B.T. Dopamine uptake through the norepinephrine transporter in brain regions with low levels of the dopamine transporter: Evidence from knock-out mouse lines. J. Neurosci. 2002, 22, 389–395. [Google Scholar] [CrossRef] [Green Version]
- Williams, J.; Dayan, P. Dopamine, learning, and impulsivity: A biological account of attention-deficit/hyperactivity disorder. J. Child Adolesc. Psychopharmacol. 2005, 15, 160–179. [Google Scholar] [CrossRef]
- Dreyer, J.K.; Herrik, K.F.; Berg, R.W.; Hounsgaard, J.D. Influence of phasic and tonic dopamine release on receptor activation. J. Neurosci. 2010, 30, 14273–14283. [Google Scholar] [CrossRef] [Green Version]
- Czerniak, S.M.; Sikoglu, E.M.; King, J.A.; Kennedy, D.N.; Mick, E.; Frazier, J.; Moore, C.M. Areas of the brain modulated by single-dose methylphenidate treatment in youth with ADHD during task-based fMRI: A systematic review. Harv. Rev. Psychiatry 2013, 21, 151–162. [Google Scholar] [CrossRef]
- Schulz, K.P.; Fan, J.; Bédard, A.C.; Clerkin, S.M.; Ivanov, I.; Tang, C.Y.; Halperin, J.M.; Newcorn, J.H. Common and unique therapeutic mechanisms of stimulant and nonstimulant treatments for attention-deficit/hyperactivity disorder. Arch. Gen. Psychiatry 2012, 69, 952–961. [Google Scholar] [CrossRef] [Green Version]
- Martella, D.; Aldunate, N.; Fuentes, L.J.; Sánchez-Pérez, N. Arousal and Executive Alterations in Attention Deficit Hyperactivity Disorder (ADHD). Front. Psychol. 2020, 11, 1991. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, R.B.; Pipingas, A.; Farrow, M.; Levy, F.; Stough, C.K. Dopaminergic modulation of default mode network brain functional connectivity in attention deficit hyperactivity disorder. Brain Behav. 2016, 6, e00582. [Google Scholar] [CrossRef] [PubMed]
- Michels, L.; Lüchinger, R.; Koenig, T.; Martin, E.; Brandeis, D. Developmental changes of BOLD signal correlations with global human EEG power and synchronization during working memory. PLoS ONE 2012, 7, e39447. [Google Scholar] [CrossRef] [Green Version]
- Ivanov, I.; Bansal, R.; Hao, X.; Zhu, H.; Kellendonk, C.; Miller, L.; Sanchez-Pena, J.; Miller, A.M.; Chakravarty, M.M.; Klahr, K.; et al. Morphological abnormalities of the thalamus in youths with attention deficit hyperactivity disorder. Am. J. Psychiatry 2010, 167, 397–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sonuga-Barke, E.J.; Castellanos, F.X. Spontaneous attentional fluctuations in impaired states and pathological conditions: A neurobiological hypothesis. Neurosci. Biobehav. Rev. 2007, 31, 977–986. [Google Scholar] [CrossRef] [PubMed]
- Baþar, E.; Baþar-Eroðlu, C.; Güntekin, B.; Yener, G.G. Brain’s alpha, beta, gamma, delta, and theta oscillations in neuropsychiatric diseases: Proposal for biomarker strategies. Suppl. Clin. Neurophysiol. 2013, 62, 19–54. [Google Scholar] [CrossRef]
- Keune, P.M.; Wiedemann, E.; Schneidt, A.; Schönenberg, M. Frontal brain asymmetry in adult attention-deficit/hyperactivity disorder (ADHD): Extending the motivational dysfunction hypothesis. Clin. Neurophysiol. 2015, 126, 711–720. [Google Scholar] [CrossRef]
- Rosenau, P.T.; Openneer, T.; Matthijssen, A.M.; van de Loo-Neus, G.; Buitelaar, J.K.; van den Hoofdakker, B.J.; Hoekstra, P.J.; Dietrich, A. Effects of methylphenidate on executive functioning in children and adolescents with ADHD after long-term use: A randomized, placebo-controlled discontinuation study. J. Child. Psychol. Psychiatry 2021, 62, 1444–1452. [Google Scholar] [CrossRef]
- McGough, J.J.; Faraone, S.V. Estimating the size of treatment effects: Moving beyond p values. Psychiatry 2009, 6, 21–29. [Google Scholar] [PubMed]
- Johnston, B.A.; Coghill, D.; Matthews, K.; Steele, J.D. Predicting methylphenidate response in attention deficit hyperactivity disorder: A preliminary study. J. Psychopharmacol. 2015, 29, 24–30. [Google Scholar] [CrossRef]
- Kim, J.W.; Sharma, V.; Ryan, N.D. Predicting Methylphenidate Response in ADHD Using Machine Learning Approaches. Int. J. Neuropsychopharmacol. 2015, 18, pyv052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fraticelli, S.; Caratelli, G.; De Berardis, D.; Ducci, G.; Pettorruso, M.; Martinotti, G.; Di Cesare, G.; di Giannantonio, M. Gender differences in attention deficit hyperactivity disorder: An update of the current evidence. Riv. Psichiatr. 2022, 57, 159–164. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capuzzi, E.; Caldiroli, A.; Auxilia, A.M.; Borgonovo, R.; Capellazzi, M.; Clerici, M.; Buoli, M. Biological Predictors of Treatment Response in Adult Attention Deficit Hyperactivity Disorder (ADHD): A Systematic Review. J. Pers. Med. 2022, 12, 1742. https://doi.org/10.3390/jpm12101742
Capuzzi E, Caldiroli A, Auxilia AM, Borgonovo R, Capellazzi M, Clerici M, Buoli M. Biological Predictors of Treatment Response in Adult Attention Deficit Hyperactivity Disorder (ADHD): A Systematic Review. Journal of Personalized Medicine. 2022; 12(10):1742. https://doi.org/10.3390/jpm12101742
Chicago/Turabian StyleCapuzzi, Enrico, Alice Caldiroli, Anna Maria Auxilia, Riccardo Borgonovo, Martina Capellazzi, Massimo Clerici, and Massimiliano Buoli. 2022. "Biological Predictors of Treatment Response in Adult Attention Deficit Hyperactivity Disorder (ADHD): A Systematic Review" Journal of Personalized Medicine 12, no. 10: 1742. https://doi.org/10.3390/jpm12101742
APA StyleCapuzzi, E., Caldiroli, A., Auxilia, A. M., Borgonovo, R., Capellazzi, M., Clerici, M., & Buoli, M. (2022). Biological Predictors of Treatment Response in Adult Attention Deficit Hyperactivity Disorder (ADHD): A Systematic Review. Journal of Personalized Medicine, 12(10), 1742. https://doi.org/10.3390/jpm12101742