
Comparative Efficacy of 14-Day Tegoprazan-Based Triple vs. 10-Day Tegoprazan-Based Concomitant Therapy for Helicobacter pylori Eradication


Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. H. pylori Eradication Regimen
2.3. Study Endpoint and Measurements
2.4. Statistical Analysis
3. Results
3.1. Study Population and Baseline Patient Characteristics
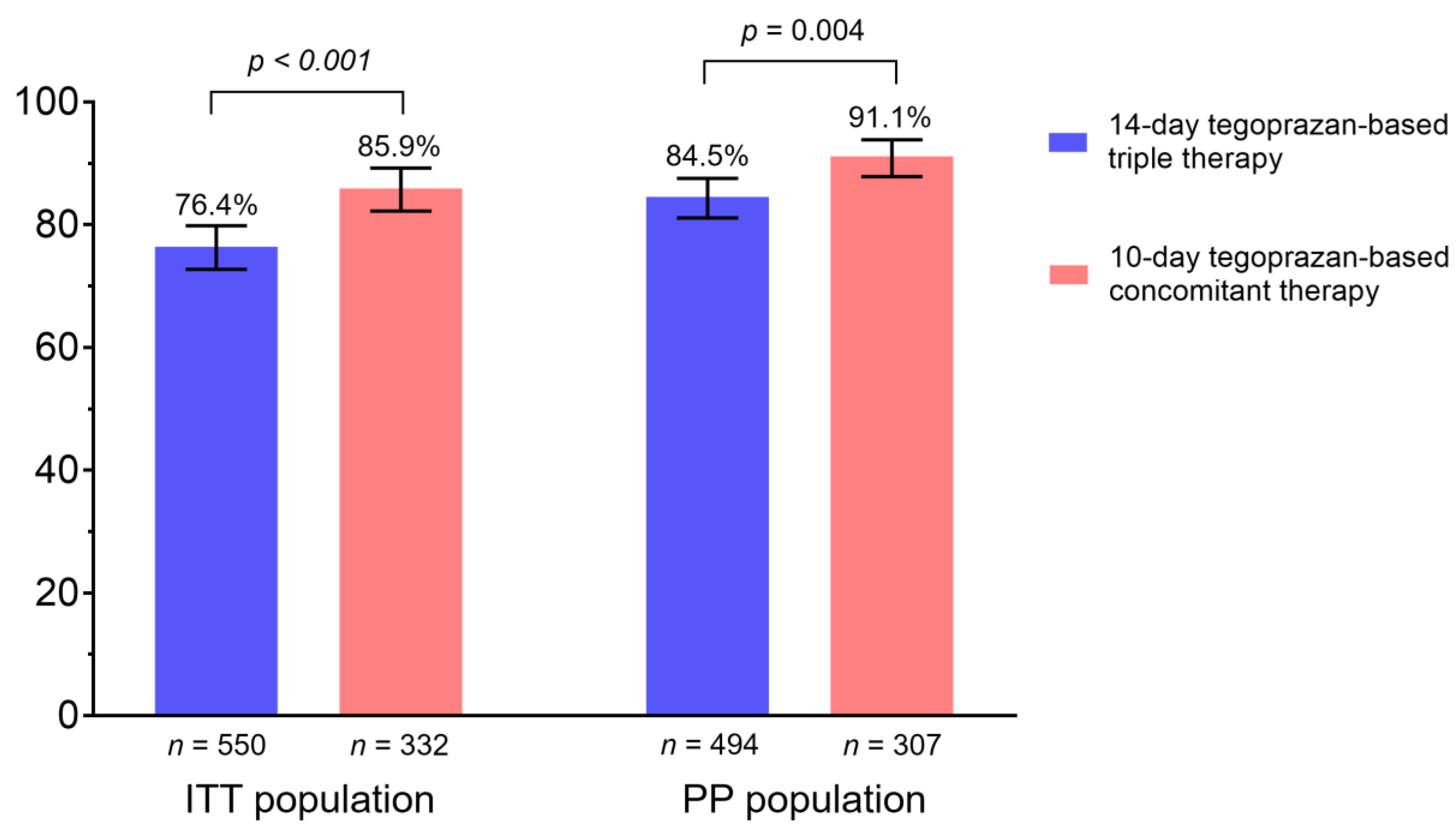
3.2. Efficacy of the First-Line Eradication Therapy
3.3. Adherence and Adverse Events
3.4. Factors Associated with H. pylori Eradication Failure
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gisbert, J.P.; Pajares, R.; Pajares, J.M. Evolution of Helicobacter pylori therapy from a meta-analytical perspective. Helicobacter 2007, 12 (Suppl. 2), 50–58. [Google Scholar] [CrossRef] [PubMed]
- Lamouliatte, H.; Cayla, R.; Megraud, F.; Zerbib, F.; Stablo, M.; Bouchard, S.; Quinton, A. Amoxicillin-clarithromycin-omeprazole: The best therapy for Helicobacter pylori infection. Acta Gastroenterol. Belg. 1993, 56, A140. [Google Scholar]
- Shin, W.G.; Lee, S.W.; Baik, G.H.; Huh, K.C.; Lee, S.I.; Chung, J.W.; Jung, W.T.; Park, M.I.; Jung, H.K.; Kim, H.U.; et al. Eradication rates of Helicobacter pylori in korea over the past 10 years and correlation of the amount of antibiotics use: Nationwide survey. Helicobacter 2016, 21, 266–278. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Kim, N.; Kim, J.M.; Nam, R.H.; Chang, H.; Kim, J.Y.; Shin, C.M.; Park, Y.S.; Lee, D.H.; Jung, H.C. Prevalence of primary and secondary antimicrobial resistance of Helicobacter pylori in Korea from 2003 through 2012. Helicobacter 2013, 18, 206–214. [Google Scholar] [CrossRef]
- De Francesco, V.; Giorgio, F.; Hassan, C.; Manes, G.; Vannella, L.; Panella, C.; Ierardi, E.; Zullo, A. Worldwide H. pylori antibiotic resistance: A systematic review. J. Gastrointestin. Liver Dis. 2010, 19, 409–414. [Google Scholar]
- Sasaki, H.; Nagahara, A.; Hojo, M.; Asaoka, D.; Matsumoto, K.; Osada, T.; Watanabe, S. Ten-year trend of the cumulative Helicobacter pylori eradication rate for the ‘japanese eradication strategy’. Digestion 2013, 88, 272–278. [Google Scholar] [CrossRef]
- Malfertheiner, P.; Megraud, F.; Rokkas, T.; Gisbert, J.P.; Liou, J.M.; Schulz, C.; Gasbarrini, A.; Hunt, R.H.; Leja, M.; O’Morain, C.; et al. Management of Helicobacter pylori infection: The maastricht vi/florence consensus report. Gut 2022, 71, 1724–1762. [Google Scholar] [CrossRef]
- Jung, H.K.; Kang, S.J.; Lee, Y.C.; Yang, H.J.; Park, S.Y.; Shin, C.M.; Kim, S.E.; Lim, H.C.; Kim, J.H.; Nam, S.Y.; et al. Evidence-based guidelines for the treatment of Helicobacter pylori infection in korea 2020. Gut Liver 2021, 15, 168–195. [Google Scholar] [CrossRef]
- Murakami, K.; Sakurai, Y.; Shiino, M.; Funao, N.; Nishimura, A.; Asaka, M. Vonoprazan, a novel potassium-competitive acid blocker, as a component of first-line and second-line triple therapy for Helicobacter pylori eradication: A phase iii, randomised, double-blind study. Gut 2016, 65, 1439–1446. [Google Scholar] [CrossRef] [Green Version]
- Jung, Y.S.; Kim, E.H.; Park, C.H. Systematic review with meta-analysis: The efficacy of vonoprazan-based triple therapy on Helicobacter pylori eradication. Aliment. Pharmacol. Ther. 2017, 46, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Chey, W.D.; Megraud, F.; Laine, L.; Lopez, L.J.; Hunt, B.J.; Howden, C.W. Vonoprazan triple and dual therapy for Helicobacter pylori infection in the United States and Europe: Randomized clinical trial. Gastroenterology 2022, 163, 608–619. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, Y.; Wang, M.; Xu, Y.L.; Zhu, Y.; Lu, N.H.; Hu, Y. Amoxicillin-vonoprazan dual therapy for Helicobacter pylori eradication: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2022, 37, 1666–1672. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Lee, Y.C.; Kim, J.M.; Kim, J.I.; Moon, J.S.; Lim, Y.J.; Baik, G.H.; Son, B.K.; Lee, H.L.; Kim, K.O.; et al. Triple therapy-based on tegoprazan, a new potassium-competitive acid blocker, for first-line treatment of Helicobacter pylori infection: A randomized, double-blind, phase iii, clinical trial. Gut Liver 2022, 16, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.S.; Kim, S.; Kim, H.Y.; Noh, S.J.; Park, J.H.; Park, C.H. 7-day versus 14-day tegoprazan-based triple therapy to treat Helicobacter pylori infection: Real-world evidence. J. Gastroenterol. Hepatol. 2022, 37, 1911–1918. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Takemoto, T. An endoscopic recognition of the atrophic border and its significance in chronic gastritis. Endoscopy 1969, 1, 87–97. [Google Scholar] [CrossRef]
- Jung, Y.S.; Park, C.H.; Park, J.H.; Nam, E.; Lee, H.L. Efficacy of Helicobacter pylori eradication therapies in korea: A systematic review and network meta-analysis. Helicobacter 2017, 22, e12389. [Google Scholar] [CrossRef]
- Rokkas, T.; Gisbert, J.P.; Malfertheiner, P.; Niv, Y.; Gasbarrini, A.; Leja, M.; Megraud, F.; O’Morain, C.; Graham, D.Y. Comparative effectiveness of multiple different first-line treatment regimens for Helicobacter pylori infection: A network meta-analysis. Gastroenterology 2021, 161, 495–507.e494. [Google Scholar] [CrossRef]
- Graham, D.Y.; Lu, H.; Yamaoka, Y. A report card to grade Helicobacter pylori therapy. Helicobacter 2007, 12, 275–278. [Google Scholar] [CrossRef]
- Jung, Y.S.; Kim, S.; Kim, H.Y.; Noh, S.J.; Park, J.H.; Sohn, C.I.; Park, C.H. Efficacy and tolerability of 14-day tegoprazan- versus rabeprazole-based triple therapy for eradication of Helicobacter pylori: A real-world evidence study. Gut Liver 2022, in press. [Google Scholar]
- Lee, J.H.; Ahn, J.Y.; Choi, K.D.; Jung, H.Y.; Kim, J.M.; Baik, G.H.; Kim, B.W.; Park, J.C.; Jung, H.K.; Cho, S.J.; et al. Nationwide antibiotic resistance mapping of Helicobacter pylori in korea: A prospective multicenter study. Helicobacter 2019, 24, e12592. [Google Scholar] [CrossRef]
- Chang, Y.W.; Ko, W.J.; Oh, C.H.; Park, Y.M.; Oh, S.J.; Moon, J.R.; Cho, J.H.; Kim, J.W.; Jang, J.Y. Clarithromycin resistance and female gender affect Helicobacter pylori eradication failure in chronic gastritis. Korean J. Intern. Med. 2019, 34, 1022–1029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cai, W.; Zhou, L.; Ren, W.; Deng, L.; Yu, M. Variables influencing outcome of Helicobacter pylori eradication therapy in south china. Helicobacter 2009, 14, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Osato, M.S.; Reddy, R.; Reddy, S.G.; Penland, R.L.; Malaty, H.M.; Graham, D.Y. Pattern of primary resistance of Helicobacter pylori to metronidazole or clarithromycin in the United States. Arch. Intern. Med. 2001, 161, 1217–1220. [Google Scholar] [CrossRef] [PubMed]
- Kim, T.; Song, H.J.; Shin, S.Y.; Kim, J.H.; Na, S.Y.; Boo, S.J.; Choi, E.K.; Cho, Y.K.; Kim, H.U.; Song, B.C. Clarithromycin-resistant Helicobacter pylori associated with 23s rrna point mutations in jeju island. Korean J. Gastroenterol. 2013, 61, 252–258. [Google Scholar] [CrossRef] [Green Version]
- Gwilt, P.R.; Nahhas, R.R.; Tracewell, W.G. The effects of diabetes mellitus on pharmacokinetics and pharmacodynamics in humans. Clin. Pharmacokinet. 1991, 20, 477–490. [Google Scholar] [CrossRef]
- Nam, S.J.; Park, S.C.; Lee, S.H.; Choi, D.W.; Lee, S.J.; Bang, C.S.; Baik, G.H.; Park, J.K. Helicobacter pylori eradication in patients with type 2 diabetes mellitus: Multicenter prospective observational study. SAGE Open Med. 2019, 7, 2050312119832093. [Google Scholar] [CrossRef] [Green Version]
- Groop, L.C.; Luzi, L.; DeFronzo, R.A.; Melander, A. Hyperglycaemia and absorption of sulphonylurea drugs. Lancet 1989, 2, 129–130. [Google Scholar] [CrossRef]
- Kong, M.F.; Macdonald, I.A.; Tattersall, R.B. Gastric emptying in diabetes. Diabet Med. 1996, 13, 112–119. [Google Scholar] [CrossRef]
- Marhoffer, W.; Stein, M.; Maeser, E.; Federlin, K. Impairment of polymorphonuclear leukocyte function and metabolic control of diabetes. Diabetes Care 1992, 15, 256–260. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| 14-Day Tegoprazan-Based Triple Therapy (n = 551) | 10-Day Tegoprazan-Based Concomitant Therapy (n = 377) | p-Value | |
|---|---|---|---|
| Age, year, mean ± SD | 55.7 ± 11.1 | 55.3 ± 11.1 | 0.539 |
| Male, n (%) | 303 (55.0) | 171 (45.4) | 0.004 |
| BMI, a kg/m, mean ± SD | 24.3 ± 3.3 | 24.0 ± 3.2 | 0.163 |
| Smoking habit | 0.712 | ||
| Never smoker | 306 (55.5) | 216 (57.3) | |
| Former smoker | 146 (26.5) | 101 (26.8) | |
| Current smoker | 99 (18.0) | 60 (15.9) | |
| Alcohol use | 0.419 b | ||
| Absent | 289 (52.5) | 184 (48.8) | |
| Present | 262 (47.5) | 193 (51.2) | |
| <2/week | 157 (28.5) | 109 (28.9) | |
| ≥2/week | 105 (19.1) | 84 (22.3) | |
| Comorbidity | |||
| Hypertension | 120 (21.8) | 94 (24.9) | 0.262 |
| Cardiovascular disease | 24 (4.4) | 14 (3.7) | 0.628 |
| Diabetes | 60 (10.9) | 39 (10.3) | 0.792 |
| Cerebrovascular accident | 14 (2.5) | 10 (2.7) | 0.916 |
| 14-Day Tegoprazan-Based Triple Therapy (n = 551) | 10-Day Tegoprazan-Based Concomitant Therapy (n = 377) | p-Value | |
|---|---|---|---|
| Symptom | |||
| Reflux symptom a | 12 (2.2) | 10 (2.7) | 0.641 |
| Nausea or vomiting | 7 (1.3) | 5 (1.3) | >0.999 |
| Gastric soreness | 44 (8.0) | 48 (12.7) | 0.017 |
| Abdominal discomfort | 79 (14.3) | 61 (16.2) | 0.441 |
| Abdominal pain | 16 (2.9) | 13 (3.4) | 0.640 |
| Others b | 15 (2.7) | 23 (6.1) | 0.011 |
| Indication for H. pylori eradication | 0.010 | ||
| Gastric and duodenal ulcers | 2 (0.4) | 4 (1.1) | |
| Gastric ulcer | 37 (6.7) | 11 (2.9) | |
| Duodenal ulcer | 43 (7.8) | 34 (9.0) | |
| MALT lymphoma | 1 (0.2) | 0 (0.0) | |
| EGC treated with ESD | 10 (1.8) | 1 (0.3) | |
| Gastric adenoma treated with ESD | 7 (1.3) | 2 (0.5) | |
| H. pylori-associated gastritis | 451 (81.9) | 325 (86.2) | |
| Nodular gastritis c | 46 (8.3) | 33 (8.8) | 0.828 |
| Atrophic gastritis c,d | 0.002 | ||
| Absent (C-0) | 115 (20.9) | 53 (14.1) | |
| Present | |||
| C-1 | 127 (23.1) | 80 (21.2) | |
| C-2 | 74 (13.5) | 48 (12.7) | |
| C-3 | 93 (16.9) | 75 (19.9) | |
| O-1 | 62 (11.3) | 71 (18.8) | |
| O-2 | 48 (8.7) | 40 (10.6) | |
| O-3 | 30 (5.5) | 10 (2.7) |
| 14-Day Tegoprazan-Based Triple Therapy (n = 551) | 10-Day Tegoprazan-Based Concomitant Therapy (n = 377) | p-Value | |
|---|---|---|---|
| Adherence, a n (%) | 496 (90.0) | 349 (92.6) | 0.180 |
| Loss of follow-up | 47 (8.5) | 18 (4.8) | 0.028 |
| Insufficient medication | 8 (1.5) | 10 (2.7) | 0.193 |
| Adverse event, b n (%) | |||
| Any adverse event | 160 (29.0) | 173 (45.9) | <0.001 |
| Mild | 153 (27.8) | 164 (43.5) | |
| Moderate | 7 (1.3) | 8 (2.1) | |
| Severe | 0 (0.0) | 1 (0.3) | |
| General weakness | 1 (0.2) | 7 (1.9) | 0.009 |
| Dizziness | 1 (0.2) | 7 (1.9) | 0.009 |
| Hedache | 2 (0.4) | 4 (1.1) | 0.231 |
| Myalgia | 0 (0.0) | 0 (0.0) | N/A d |
| Acid regurgitation | 1 (0.2) | 3 (0.8) | 0.310 |
| Nausea or vomiting | 26 (4.7) | 34 (9.0) | 0.009 |
| Dysgeusia | 62 (11.3) | 42 (11.1) | 0.958 |
| Abdominal discomfort | 6 (1.1) | 6 (1.6) | 0.561 |
| Abdominal pain | 3 (0.5) | 4 (1.1) | 0.451 |
| Diarrhea | 51 (9.3) | 86 (22.8) | <0.001 |
| Constipation | 3 (0.5) | 1 (0.3) | 0.650 |
| Skin rash | 9 (1.6) | 3 (0.8) | 0.379 |
| Others c | 5 (0.9) | 14 (3.7) | 0.003 |
| n | Failure n (%) | Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |||
| Treatment duration | ||||||
| 14-day tegoprazan-based triple | 501 | 81 (16.2) | 1.5 (1.27–3.01) | 0.003 | 2.08 (1.34–3.24) | 0.001 |
| 10-day tegoprazan-based concomitant | 356 | 32 (9.0) | 1 | 1 | ||
| Adherence | ||||||
| Adherent | 844 | 108 (12.8) | 1 | 1 | ||
| Non-adherent | 13 | 5 (38.5) | 4.26 (1.67–13.26) | 0.012 | 4.35 (1.31–14.4) | 0.016 |
| Age | ||||||
| <60 years | 519 | 65 (12.5) | 1 | |||
| ≥60 years | 338 | 48 (14.2) | 1.16 (0.77–1.73) | 0.478 | ||
| Sex | ||||||
| Male | 433 | 48 (11.1) | 1 | 1 | ||
| Female | 424 | 65 (15.3) | 1.45 (0.97–2.17) | 0.067 | 1.59 (1.06–2.39) | 0.026 |
| BMI | ||||||
| <25 kg/m2 | 537 | 68 (12.7) | 1 | |||
| ≥25 kg/m2 | 320 | 45 (14.1) | 1.13 (0.75–1.69) | 0.558 | ||
| Smoking habit | ||||||
| Never smoker | 481 | 70 (14.6) | 1 | |||
| Former smoker | 233 | 29 (12.4) | 0.84 (0.53–1.33) | 0.445 | ||
| Current smoker | 143 | 14 (9.8) | 0.64 (0.35–1.17) | 0.146 | ||
| Alcohol use | ||||||
| Absent | 437 | 62 (14.2) | 1 | |||
| <2/week | 246 | 33 (13.4) | 0.94 (0.60–1.48) | 0.779 | ||
| ≥2/week | 174 | 18 (10.3) | 0.70 (0.40–1.22) | 0.206 | ||
| Comorbidity | ||||||
| Hypertension | 194 | 30 (15.5) | 1.28 (0.81–2.01) | 0.287 | ||
| Cardiovascular disease | 34 | 7 (20.6) | 1.75 (0.75–4.13) | 0.198 | ||
| Diabetes | 91 | 19 (20.9) | 1.89 (1.09–3.27) | 0.024 | 1.90 (1.08–3.34) | 0.027 |
| Cerebrovascular accident | 24 | 1 (4.2) | 0.28 (0.04–2.09) | 0.215 | ||
| Symptom | ||||||
| Reflux symptom b | 19 | 1 (5.3) | 0.36 (0.05–2.72) | 0.323 | ||
| Nausea or vomiting | 12 | 0 (0.0) | N/A | 0.999 | ||
| Gastric soreness | 87 | 14 (16.1) | 1.30 (0.71–2.39) | 0.399 | ||
| Abdominal discomfort | 128 | 18 (14.1) | 1.09 (0.63–1.88) | 0.751 | ||
| Abdominal pain | 28 | 6 (21.4) | 1.84 (0.73–4.64) | 0.196 | ||
| Others c | 36 | 6 (16.7) | 1.34 (0.54–3.28) | 0.530 | ||
| Indication for H. pylori eradication | ||||||
| Peptic ulcer | 118 | 14 (11.9) | 0.89 (0.49–1.63) | 0.713 | ||
| MALT lymphoma | 1 | 1 (100.0) | N/A | >0.999 | ||
| EGC treated with ESD | 11 | 3 (27.3) | 2.49 (0.65–9.55) | 0.184 | ||
| Gastric adenoma treated with ESD | 9 | 1 (11.1) | 0.83 (0.10–6.71) | 0.861 | ||
| H. pylori-associated gastritis | 718 | 94 (13.1) | 1 | |||
| Nodular gastritis | 72 | 8 (11.1) | 0.81 (0.38–1.74) | 0.587 | ||
| Atrophic gastritis d | ||||||
| Normal (C-0) | 148 | 19 (12.8) | 1 | |||
| Mild (C-1, C-2) | 302 | 34 (11.3) | 0.86 (0.74–1.57) | 0.626 | ||
| Moderate (C-3, O-1) | 284 | 42 (14.8) | 1.18 (0.66–2.11) | 0.581 | ||
| Severe (O-2, O-3) | 122 | 18 (14.8) | 1.18 (0.59–2.35) | 0.649 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, C.H.; Song, M.J.; Jung, B.W.; Park, J.H.; Jung, Y.S. Comparative Efficacy of 14-Day Tegoprazan-Based Triple vs. 10-Day Tegoprazan-Based Concomitant Therapy for Helicobacter pylori Eradication. J. Pers. Med. 2022, 12, 1918. https://doi.org/10.3390/jpm12111918
Park CH, Song MJ, Jung BW, Park JH, Jung YS. Comparative Efficacy of 14-Day Tegoprazan-Based Triple vs. 10-Day Tegoprazan-Based Concomitant Therapy for Helicobacter pylori Eradication. Journal of Personalized Medicine. 2022; 12(11):1918. https://doi.org/10.3390/jpm12111918
Chicago/Turabian StylePark, Chan Hyuk, Myung Jin Song, Byung Wook Jung, Jung Ho Park, and Yoon Suk Jung. 2022. "Comparative Efficacy of 14-Day Tegoprazan-Based Triple vs. 10-Day Tegoprazan-Based Concomitant Therapy for Helicobacter pylori Eradication" Journal of Personalized Medicine 12, no. 11: 1918. https://doi.org/10.3390/jpm12111918
APA StylePark, C. H., Song, M. J., Jung, B. W., Park, J. H., & Jung, Y. S. (2022). Comparative Efficacy of 14-Day Tegoprazan-Based Triple vs. 10-Day Tegoprazan-Based Concomitant Therapy for Helicobacter pylori Eradication. Journal of Personalized Medicine, 12(11), 1918. https://doi.org/10.3390/jpm12111918