
Association between Thyroid Cancer and Breast Cancer: Two Longitudinal Follow-Up Studies Using a National Health Screening Cohort


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definition of Thyroid Cancer
2.3. Definition of Breast Cancer
2.4. Participant Selection
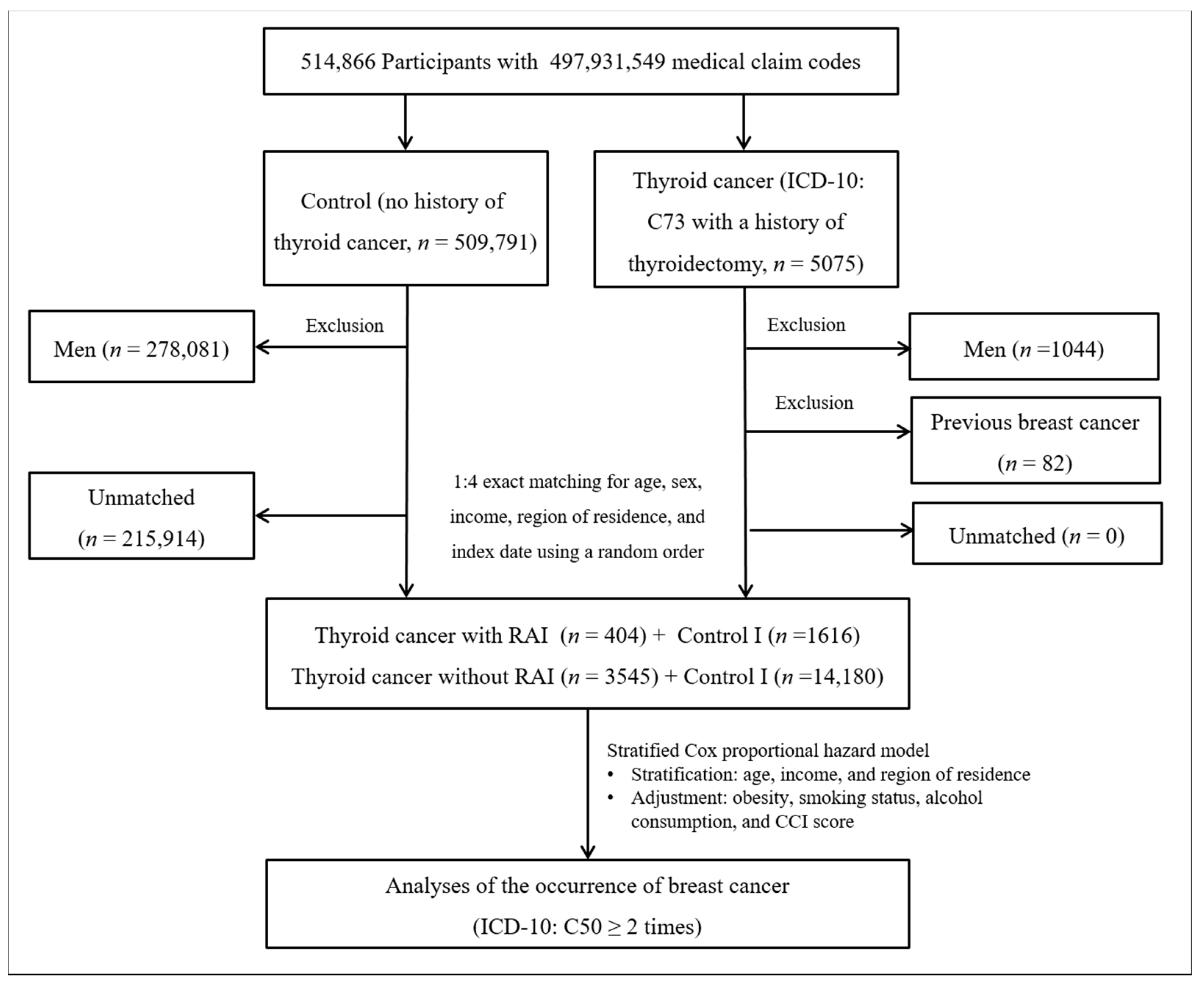
2.4.1. Study I
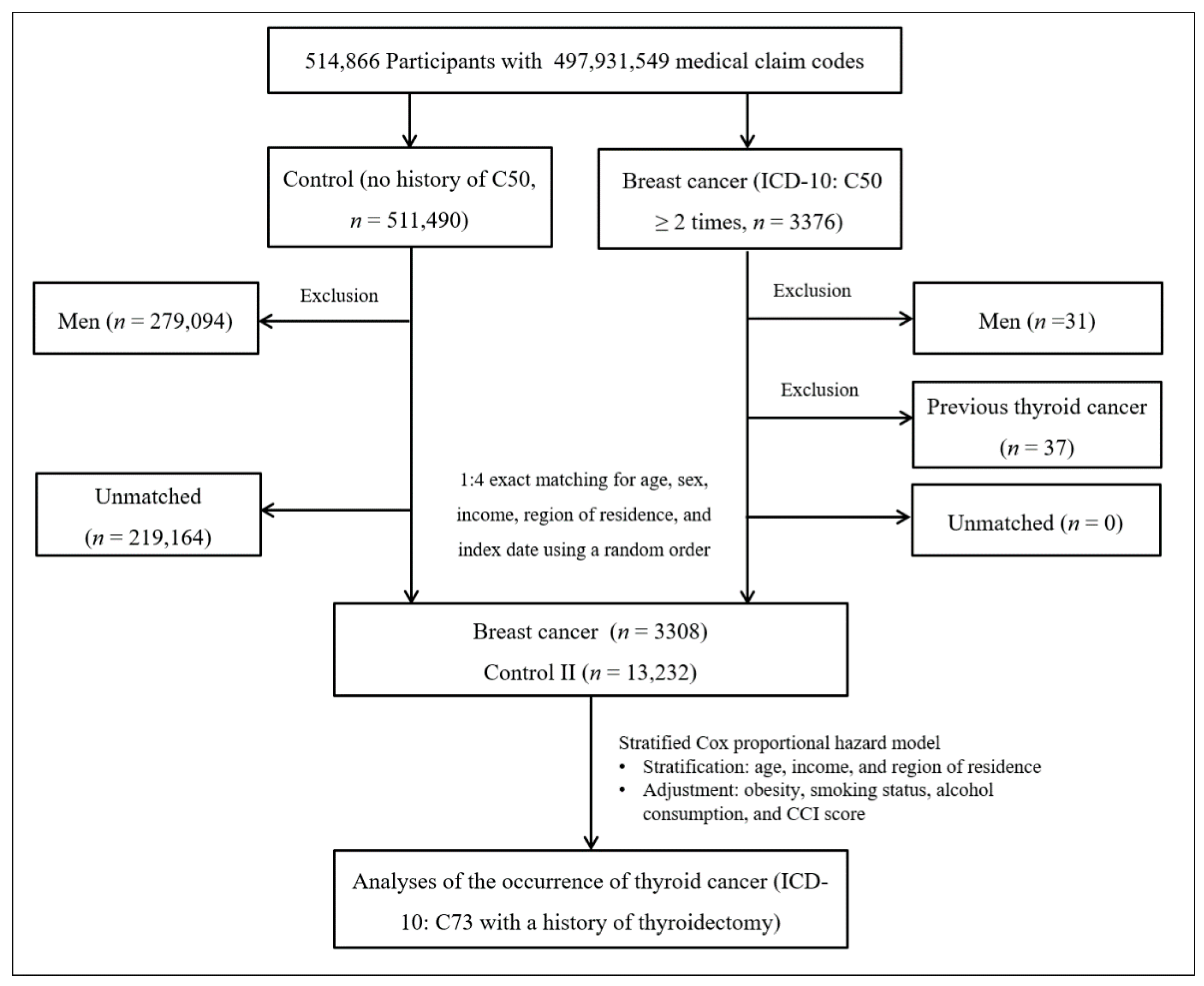
2.4.2. Study II
2.5. Covariates
2.6. Statistical Analyses
3. Results
3.1. Detailed Descriptions
3.1.1. Study I. Risk of Breast Cancer in the Thyroid Cancer Group
3.1.2. Study II. Risk of Thyroid Cancer in the Breast Cancer Group
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA A Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Cancer Statistics. Available online: https://ncc.re.kr/main.ncc?uri=english/sub04_Statistics (accessed on 21 January 2020).
- DeSantis, C.; Ma, J.; Bryan, L.; Jemal, A. Breast cancer statistics, 2013. CA A Cancer J. Clin. 2014, 64, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.; Krapcho, M.; Miller, D.; Bishop, K.; Altekruse, S.; Kosary, C.; Yu, M.; Ruhl, J.; Tatalovich, Z. SEER Cancer Statistics Review, 1975–2013; National Cancer Institute: Bethesda, MD, USA, 2016; Volume 19.
- Ahn, H.S.; Kim, H.J.; Welch, H.G. Korea’s thyroid-cancer “epidemic”—Screening and overdiagnosis. N. Engl. J. Med. 2014, 371, 1765–1767. [Google Scholar] [CrossRef] [PubMed]
- Joseph, K.R.; Edirimanne, S.; Eslick, G.D. The association between breast cancer and thyroid cancer: A meta-analysis. Breast Cancer Res. Treat. 2015, 152, 173–181. [Google Scholar] [CrossRef] [PubMed]
- An, J.H.; Hwangbo, Y.; Ahn, H.Y.; Keam, B.; Lee, K.E.; Han, W.; Park, D.J.; Park, I.A.; Noh, D.-Y.; Youn, Y.-K. A possible association between thyroid cancer and breast cancer. Thyroid 2015, 25, 1330–1338. [Google Scholar] [CrossRef]
- Evans, H.; Lewis, C.; Robinson, D.; Bell, C.; Møller, H.; Hodgson, S. Incidence of multiple primary cancers in a cohort of women diagnosed with breast cancer in southeast England. Br. J. Cancer 2001, 84, 435–440. [Google Scholar] [CrossRef]
- Jung, H.K.; Park, S.; Kim, N.W.; Lee, J.E.; Kim, Z.; Han, S.W.; Hur, S.M.; Kim, S.Y.; Lim, C.W.; Lee, M.H. Development of second primary cancer in Korean breast cancer survivors. Ann. Surg. Treat. Res. 2017, 93, 287–292. [Google Scholar] [CrossRef]
- Consorti, F.; Di Tanna, G.; Milazzo, F.; Antonaci, A. Nulliparity enhances the risk of second primary malignancy of the breast in a cohort of women treated for thyroid cancer. World J. Surg. Oncol. 2011, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Subramanian, S.; Goldstein, D.P.; Parlea, L.; Thabane, L.; Ezzat, S.; Ibrahim-Zada, I.; Straus, S.; Brierley, J.D.; Tsang, R.W.; Gafni, A.; et al. Second primary malignancy risk in thyroid cancer survivors: A systematic review and meta-analysis. Thyroid 2007, 17, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Dong, L.; Lu, J.; Zhao, B.; Wang, W.; Zhao, Y. Review of the possible association between thyroid and breast carcinoma. World J. Surg. Oncol. 2018, 16, 130. [Google Scholar] [CrossRef]
- Catsburg, C.; Miller, A.B.; Rohan, T.E. Active cigarette smoking and risk of breast cancer. Int. J. Cancer 2015, 136, 2204–2209. [Google Scholar] [CrossRef]
- Chan, D.; Vieira, A.; Aune, D.; Bandera, E.; Greenwood, D.; McTiernan, A.; Navarro Rosenblatt, D.; Thune, I.; Vieira, R.; Norat, T. Body mass index and survival in women with breast cancer—systematic literature review and meta-analysis of 82 follow-up studies. Ann. Oncol. 2014, 25, 1901–1914. [Google Scholar] [CrossRef] [PubMed]
- Kitahara, C.M.; Pfeiffer, R.M.; Sosa, J.A.; Shiels, M.S. Impact of overweight and obesity on US papillary thyroid cancer incidence trends (1995–2015). J. Natl. Cancer Inst. 2020, 112, 810–817. [Google Scholar] [CrossRef]
- Kim, S.Y.; Min, C.Y.; Oh, D.J.; Choi, H.G. Tobacco Smoking and Alcohol Consumption Are Related to Benign Parotid Tumor: A Nested Case-Control Study Using a National Health Screening Cohort. Clin. Exp. Otorhinolaryngol. 2019, 12, 412–419. [Google Scholar] [CrossRef] [PubMed]
- Sung, M.-W.; Park, B.; An, S.-Y.; Hah, J.H.; Jung, Y.H.; Choi, H.G. Increasing thyroid cancer rate and the extent of thyroid surgery in Korea. PLoS ONE 2014, 9, e113464. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.-S.; Kim, S.Y.; Kim, J.-H.; Park, B.; Choi, H.G. Depression in breast cancer patients who have undergone mastectomy: A national cohort study. PLoS ONE 2017, 12, e0175395. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Oh, D.J.; Park, B.; Choi, H.G. Bell’s palsy and obesity, alcohol consumption and smoking: A nested case-control study using a national health screening cohort. Sci. Rep. 2020, 10, 4248. [Google Scholar] [CrossRef] [PubMed]
- Quan, H.; Li, B.; Couris, C.M.; Fushimi, K.; Graham, P.; Hider, P.; Januel, J.-M.; Sundararajan, V. Updating and validating the Charlson comorbidity index and score for risk adjustment in hospital discharge abstracts using data from 6 countries. Am. J. Epidemiol. 2011, 173, 676–682. [Google Scholar] [CrossRef] [PubMed]
- Liaw, D.; Marsh, D.J.; Li, J.; Dahia, P.L.; Wang, S.I.; Zheng, Z.; Bose, S.; Call, K.M.; Tsou, H.C.; Peacoke, M. Germline mutations of the PTEN gene in Cowden disease, an inherited breast and thyroid cancer syndrome. Nat. Genet. 1997, 16, 64–67. [Google Scholar] [CrossRef] [PubMed]
- Colditz, G.A.; Peterson, L.L. Obesity and cancer: Evidence, impact, and future directions. Clin. Chem. 2018, 64, 154–162. [Google Scholar] [CrossRef]
- Winsløw, U.C.; Rode, L.; Nordestgaard, B.G. High tobacco consumption lowers body weight: A Mendelian randomization study of the Copenhagen General Population Study. Int. J. Epidemiol. 2015, 44, 540–550. [Google Scholar] [CrossRef] [PubMed]
- Soldin, O.P.; Goughenour, B.E.; Gilbert, S.Z.; Landy, H.J.; Soldin, S.J. Thyroid hormone levels associated with active and passive cigarette smoking. Thyroid 2009, 19, 817–823. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.-H.; Myung, S.-K.; Kim, H.S.; Group, K.M.-A.S. Alcohol intake and risk of thyroid cancer: A meta-analysis of observational studies. Cancer Res. Treat. Off. J. Korean Cancer Assoc. 2017, 49, 534. [Google Scholar] [CrossRef] [PubMed]
- Brand, J.S.; Chan, M.-F.; Dowsett, M.; Folkerd, E.; Wareham, N.J.; Luben, R.N.; van der Schouw, Y.T.; Khaw, K.-T. Cigarette smoking and endogenous sex hormones in postmenopausal women. J. Clin. Endocrinol. Metab. 2011, 96, 3184–3192. [Google Scholar] [CrossRef] [PubMed]
- Gaudet, M.M.; Gapstur, S.M.; Sun, J.; Diver, W.R.; Hannan, L.M.; Thun, M.J. Active smoking and breast cancer risk: Original cohort data and meta-analysis. J. Natl. Cancer Inst. 2013, 105, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Scoccianti, C.; Lauby-Secretan, B.; Bello, P.-Y.; Chajes, V.; Romieu, I. Female breast cancer and alcohol consumption: A review of the literature. Am. J. Prev. Med. 2014, 46, S16–S25. [Google Scholar] [CrossRef] [PubMed]
- Fallahi, B.; Adabi, K.; Majidi, M.; Fard-Esfahani, A.; Heshmat, R.; Larijani, B.; Haghpanah, V. Incidence of second primary malignancies during a long-term surveillance of patients with differentiated thyroid carcinoma in relation to radioiodine treatment. Clin. Nucl. Med. 2011, 36, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Rubino, C.; De Vathaire, F.; Dottorini, M.; Hall, P.; Schvartz, C.; Couette, J.; Dondon, M.-G.; Abbas, M.; Langlois, C.; Schlumberger, M. Second primary malignancies in thyroid cancer patients. Br. J. Cancer 2003, 89, 1638–1644. [Google Scholar] [CrossRef]
- Lang, B.H.-H.; Wong, I.O.L.; Wong, K.P.; Cowling, B.J.; Wan, K.-Y. Risk of second primary malignancy in differentiated thyroid carcinoma treated with radioactive iodine therapy. Surgery 2012, 151, 844–850. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.Y.; Saeed, O.; Goldberg, A.S.; Farooq, S.; Fazelzad, R.; Goldstein, D.P.; Tsang, R.W.; Brierley, J.D.; Ezzat, S.; Thabane, L. A systematic review and meta-analysis of subsequent malignant neoplasm risk after radioactive iodine treatment of thyroid cancer. Thyroid 2018, 28, 1662–1673. [Google Scholar] [CrossRef]
- Lin, C.Y.; Lin, C.L.; Huang, W.S.; Kao, C.H. Risk of Breast Cancer in Patients with Thyroid Cancer Receiving or Not Receiving I-131 Treatment: A Nationwide Population-Based Cohort Study. J. Nucl. Med. 2016, 57, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Curtis, R.E. New Malignancies among Cancer Survivors: SEER Cancer Registries, 1973–2000; US Department of Health and Human Services, National Institutes of Health, National Cancer Institute: Washington, DC, USA, 2006.
- Dinda, S.; Sanchez, A.; Moudgil, V. Estrogen-like effects of thyroid hormone on the regulation of tumor suppressor proteins, p53 and retinoblastoma, in breast cancer cells. Oncogene 2002, 21, 761–768. [Google Scholar] [CrossRef]
- Tanaka, H.; Tsukuma, H.; Koyama, H.; Kinoshita, Y.; Kinoshita, N.; Oshima, A. Second primary cancers following breast cancer in the Japanese female population. Jpn. J. Cancer Res. 2001, 92, 1–8. [Google Scholar] [CrossRef]
- Kim, J.Y.; Song, H.S. Metachronous Double Primary Cancer after Treatment of Breast Cancer. Cancer Res. Treat. 2015, 47, 64–71. [Google Scholar] [CrossRef]
- Grantzau, T.; Overgaard, J. Risk of second non-breast cancer after radiotherapy for breast cancer: A systematic review and meta-analysis of 762,468 patients. Radiother. Oncol. 2015, 114, 56–65. [Google Scholar] [CrossRef]
- Dalwadi, S.M.; Dorman, C.; Fisher, S.B.; Bonnen, M.; Grubbs, E.; Ludwig, M.S. Risk of thyroid cancer after therapeutic irradiation in adult patients: An Age-Based surveillance, epidemiology, and end results analysis. Laryngoscope 2020, 130, 2081–2086. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Study I | Study II | |||||
|---|---|---|---|---|---|---|---|
| Thyroid Cancer (n, %) | Control I (n, %) | p-Value | Breast Cancer (n, %) | Control II (n, %) | p-Value | ||
| Age (years old) | 1.000 | 1.000 | |||||
| 40–59 | 2714 (68.7) | 10,856 (68.7) | 2307 (69.7) | 9228 (69.7) | |||
| ≥60 | 1235 (31.3) | 4940 (31.3) | 1001 (30.3) | 4004 (30.3) | |||
| Income | 1.000 | 1.000 | |||||
| Low (1–3) | 1666 (42.2) | 6664 (42.2) | 1482 (44.8) | 5928 (44.8) | |||
| High (4–5) | 2283 (57.8) | 9132 (57.8) | 1826 (55.2) | 7304 (55.2) | |||
| Region of residence | 1.000 | 1.000 | |||||
| Urban | 1919 (48.6) | 7676 (48.6) | 1651 (49.9) | 6604 (49.9) | |||
| Rural | 2030 (51.4) | 8120 (51.4) | 1657 (50.1) | 6628 (50.1) | |||
| CCI score | <0.001 * | <0.001 * | |||||
| 0 | 3861 (97.8) | 15,588 (98.7) | 3165 (95.7) | 13,034 (98.5) | |||
| 1 | 9 (0.2) | 37 (0.2) | 17 (0.5) | 47 (0.4) | |||
| ≥ 2 | 79 (2.0) | 171 (1.1) | 126 (3.8) | 151 (1.1) | |||
| Obesity † | <0.001 * | 0.018 * | |||||
| Underweight | 53 (1.3) | 333 (2.1) | 275 (1.6) | 54 (2.1) | |||
| Normal | 1425 (36.1) | 6236 (39.5) | 5122 (36.5) | 1208 (38.7) | |||
| Overweight | 1100 (27.9) | 4090 (25.9) | 3475 (26.7) | 882 (26.3) | |||
| Obese | 1371 (34.7) | 5137 (32.5) | 1164 (35.2) | 4360 (33.0) | |||
| Current smoker | 40 (1.0) | 299 (1.9) | <0.001 * | 55 (1.7) | 297 (2.2) | 0.015 * | |
| Alcohol ≥ 1 time a week | 204 (5.2) | 1022 (6.5) | 0.002 * | 189 (5.7) | 906 (6.9) | 0.019 * | |
| Breast cancer | 39 (1.0) | 94 (0.6) | 0.007 * | 3308 (100.0) | 0 (0.0) | <0.001 * | |
| Thyroid cancer | 3949 (100.0) | 0 (0.0) | <0.001 * | 84 (2.5) | 181 (1.4) | <0.001 * | |
| Characteristics | Breast Cancer | Hazard Ratios for Breast Cancer | ||||
|---|---|---|---|---|---|---|
| (Exposure/Total, %) | Crude † | p-Value | Adjusted †‡ | p-Value | ||
| Total participants (n = 19,745) | ||||||
| Thyroid cancer | 39/3949 (1.0) | 1.67 (1.15–2.43) | 0.007 * | 1.64 (1.13–2.39) | 0.010 * | |
| Control I | 94/15,796 (0.6) | 1.00 | 1.00 | |||
| Age < 60 years old (n = 13,570) | ||||||
| Thyroid cancer | 27/2714 (1.0) | 1.45 (0.93–2.25) | 0.097 | 1.41 (0.91–2.20) | 0.127 | |
| Control I | 75/10,856 (0.7) | 1.00 | 1.00 | |||
| Age ≥ 60 years old (n = 6175) | ||||||
| Thyroid cancer | 12/1235 (1.0) | 2.55 (1.24–5.26) | 0.011 * | 2.56 (1.24–5.29) | 0.011 * | |
| Control I | 19/4940 (0.4) | 1.00 | 1.00 | |||
| Thyroid cancer with RAI and controls (n = 2020) | ||||||
| Thyroid cancer | 8/404 (2.0) | 1.90 (0.82–4.41) | 0.134 | 1.84 (0.78–4.30) | 0.162 | |
| Control I | 17/1616 (1.1) | 1.00 | 1.00 | |||
| Thyroid cancer without RAI and controls (n = 17,725) | ||||||
| Thyroid cancer | 31/3545 (0.9) | 1.62 (1.06–2.45) | 0.024 * | 1.59 (1.04–2.42) | 0.031 * | |
| Control I | 77/14,180 (0.5) | 1.00 | 1.00 | |||
| Characteristics | Thyroid Cancer | Hazard Ratios for Thyroid Cancer | ||||
|---|---|---|---|---|---|---|
| (Exposure/Total, %) | Crude † | p-Value | Adjusted †‡ | p-Value | ||
| Total participants (n = 16,540) | ||||||
| Breast cancer | 84/3308 (2.5) | 1.96 (1.51–2.54) | <0.001 * | 1.91 (1.47–2.49) | <0.001 * | |
| Control II | 181/13,232 (1.4) | 1.00 | 1.00 | |||
| Age < 60 years old (n = 11,535) | ||||||
| Breast cancer | 63/2307 (2.7) | 1.78 (1.32–2.38) | <0.001 * | 1.72 (1.27–2.31) | <0.001 * | |
| Control II | 150/9228 (1.6) | 1.00 | 1.00 | |||
| Age ≥ 60 years old (n = 5005) | ||||||
| Breast cancer | 21/1001 (2.1) | 2.82 (1.62–4.92) | <0.001 * | 2.91 (1.67–5.09) | <0.001 * | |
| Control II | 31/4004 (0.8) | 1.00 | 1.00 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jin, Y.J.; Kwon, M.J.; Kim, J.H.; Kim, J.-H.; Choi, H.G. Association between Thyroid Cancer and Breast Cancer: Two Longitudinal Follow-Up Studies Using a National Health Screening Cohort. J. Pers. Med. 2022, 12, 133. https://doi.org/10.3390/jpm12020133
Jin YJ, Kwon MJ, Kim JH, Kim J-H, Choi HG. Association between Thyroid Cancer and Breast Cancer: Two Longitudinal Follow-Up Studies Using a National Health Screening Cohort. Journal of Personalized Medicine. 2022; 12(2):133. https://doi.org/10.3390/jpm12020133
Chicago/Turabian StyleJin, Young Ju, Mi Jung Kwon, Ji Hee Kim, Joo-Hee Kim, and Hyo Geun Choi. 2022. "Association between Thyroid Cancer and Breast Cancer: Two Longitudinal Follow-Up Studies Using a National Health Screening Cohort" Journal of Personalized Medicine 12, no. 2: 133. https://doi.org/10.3390/jpm12020133
APA StyleJin, Y. J., Kwon, M. J., Kim, J. H., Kim, J.-H., & Choi, H. G. (2022). Association between Thyroid Cancer and Breast Cancer: Two Longitudinal Follow-Up Studies Using a National Health Screening Cohort. Journal of Personalized Medicine, 12(2), 133. https://doi.org/10.3390/jpm12020133