
Impact of Increased End-Tidal Carbon Dioxide on Continuous Noninvasive Hemoglobin Monitoring during Laparoscopic Gastrectomy: A Randomized Controlled Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Interventions
2.3. Data Collection
2.4. Statistical Analysis
3. Results
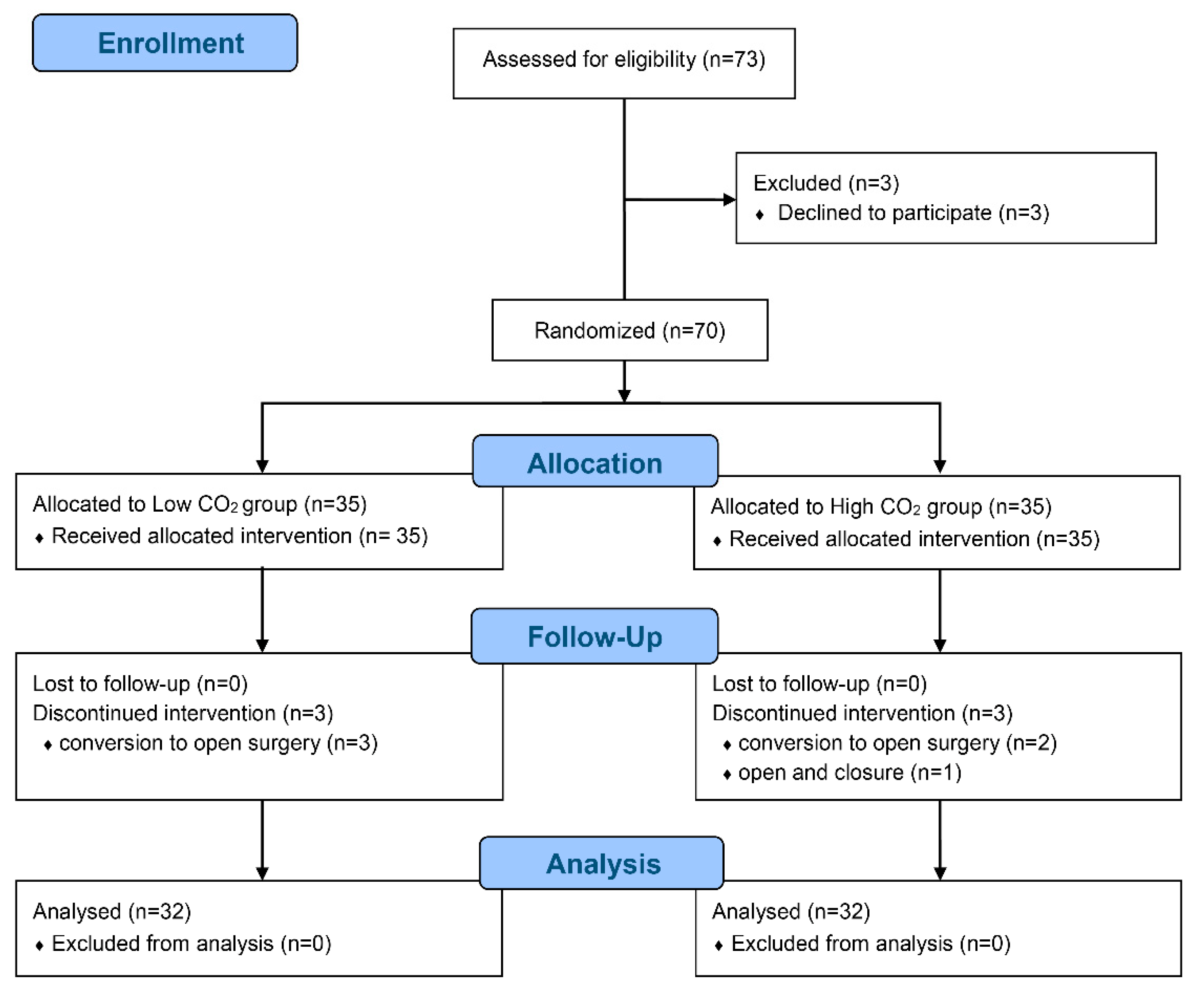
3.1. Study Population and Intraoperative Characteristics
3.2. Collection of SpHb and tHb Values
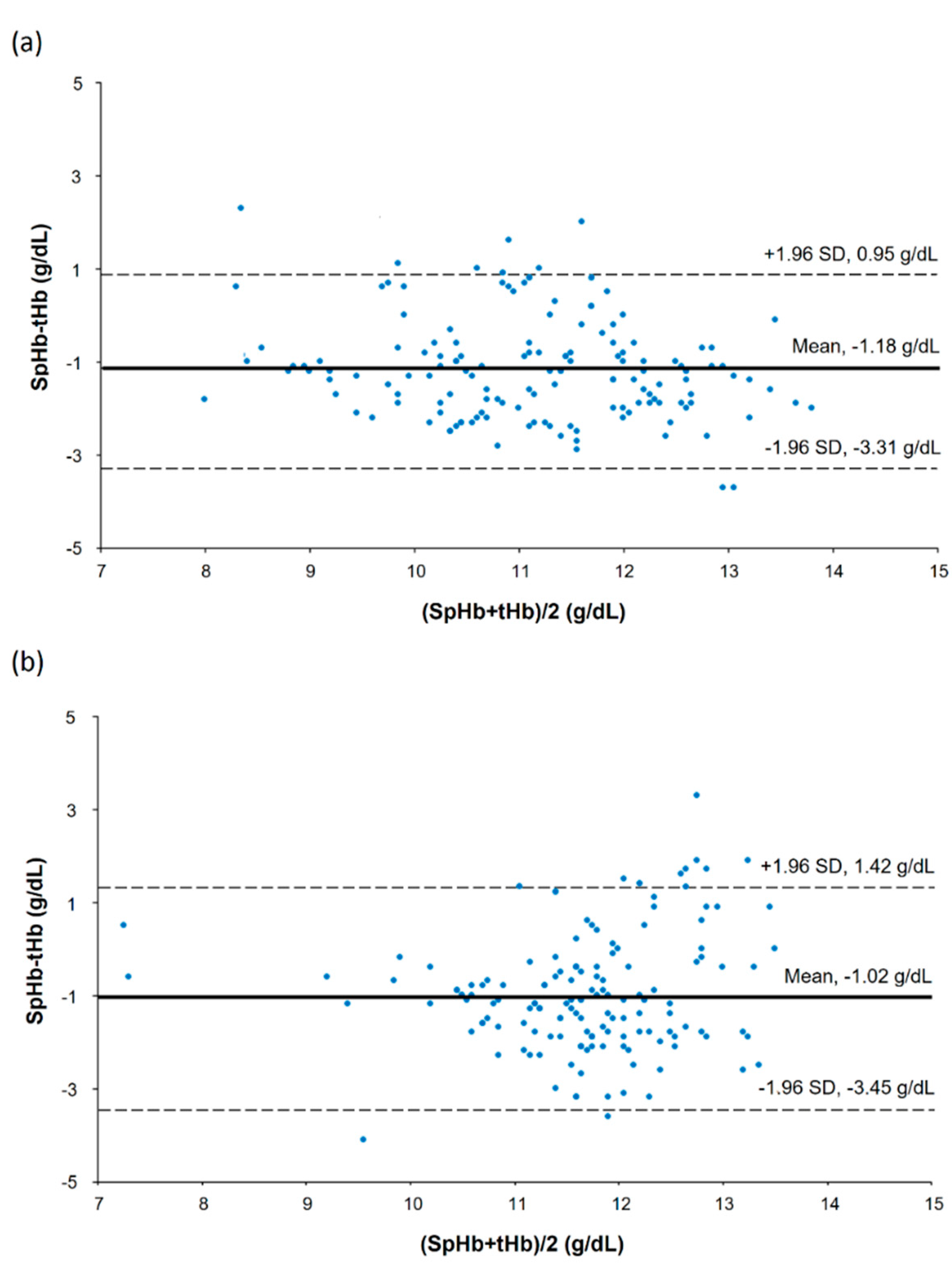
3.3. Accuracy and Trending Ability of SpHb
3.4. Comparisons According to the PaCO2 Ranges
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tomimaru, Y.; Noguchi, K.; Morita, S.; Imamura, H.; Iwazawa, T.; Dono, K. Is intraoperative blood loss underestimated in patients undergoing laparoscopic hepatectomy? World J. Surg. 2018, 42, 3685–3691. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, T.M.; Giraud, G.D.; Togioka, B.M.; Jones, D.B.; Cigarroa, J.E. Cardiovascular and ventilatory consequences of laparoscopic surgery. Circulation 2017, 135, 700–710. [Google Scholar] [CrossRef] [PubMed]
- Shamir, M.Y.; Avramovich, A.; Smaka, T. The current status of continuous noninvasive measurement of total, carboxy, and methemoglobin concentration. Anesth. Analg. 2012, 114, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Frank, S.M.; Savage, W.J.; Rothschild, J.A.; Rivers, R.J.; Ness, P.M.; Paul, S.L.; Ulatowski, J.A. Variability in blood and blood component utilization as assessed by an anesthesia information management system. Anesthesiology 2012, 117, 99–106. [Google Scholar] [CrossRef] [Green Version]
- Ribed-Sanchez, B.; Gonzalez-Gaya, C.; Varea-Diaz, S.; Corbacho-Fabregat, C.; Perez-Oteyza, J.; Belda-Iniesta, C. Economic analysis of the reduction of blood transfusions during surgical procedures while continuous hemoglobin monitoring is used. Sensors 2018, 18, 1367. [Google Scholar] [CrossRef] [Green Version]
- Goodnough, L.T.; Shander, A. Patient blood management. Anesthesiology 2012, 116, 1367–1376. [Google Scholar] [CrossRef] [Green Version]
- Isosu, T.; Satoh, T.; Oishi, R.; Imaizumi, T.; Hakozaki, T.; Obara, S.; Ikegami, Y.; Kurosawa, S.; Murakawa, M. Effects of indigo carmine intravenous injection on noninvasive and continuous total hemoglobin measurement. J. Clin. Monit. Comput. 2016, 30, 313–316. [Google Scholar] [CrossRef]
- Riess, M.L.; Pagel, P.S. Noninvasively measured hemoglobin concentration reflects arterial hemoglobin concentration before but not after cardiopulmonary bypass in patients undergoing coronary artery or valve surgery. J. Cardiothorac. Vasc. Anesth. 2016, 30, 1167–1171. [Google Scholar] [CrossRef] [Green Version]
- Erdogan Kayhan, G.; Colak, Y.Z.; Sanli, M.; Ucar, M.; Toprak, H.I. Accuracy of non-invasive hemoglobin monitoring by pulse CO-oximeter during liver transplantation. Minerva Anestesiol. 2017, 83, 485–492. [Google Scholar] [CrossRef]
- Yang, S.; Hu, P.F.; Anazodo, A.; Gao, C.; Chen, H.; Wade, C.; Hartsky, L.; Miller, C.; Imle, C.; Fang, R.; et al. Trends of hemoglobin oximetry: Do they help predict blood transfusion during trauma patient resuscitation? Anesth. Analg. 2016, 122, 115–125. [Google Scholar] [CrossRef]
- Murphy, S.M.; Omar, S. The clinical utility of noninvasive pulse co-oximetry hemoglobin measurements in dark-skinned critically ill patients. Anesth. Analg. 2018, 126, 1519–1526. [Google Scholar] [CrossRef] [PubMed]
- Bubenek-Turconi, Ş.I.; Văleanu, L.; Popescu, M.; Panaitescu, E.; Tomescu, D.; Cacoveanu, M.C.; Perel, A. Continuous noninvasive hemoglobin monitoring reflects the development of acute hemodilution after consecutive fluid challenges. Anesth. Analg. 2020, 130, 696–703. [Google Scholar] [CrossRef] [PubMed]
- Munoz, X.; Torres, F.; Sampol, G.; Rios, J.; Marti, S.; Escrich, E. Accuracy and reliability of pulse oximetry at different arterial carbon dioxide pressure levels. Eur. Respir. J. 2008, 32, 1053–1059. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.S.; Yoo, J.W.; Kim, H.Y.; Kim, N.Y.; Kim, J.E. Accuracy of continuous and noninvasive hemoglobin monitoring in the presence of CO2 insufflation: An observational pilot study. Med. Sci. Monit. 2021, 27, e933027. [Google Scholar] [CrossRef] [PubMed]
- Macknet, M.R.; Allard, M.; Applegate, R.L., 2nd; Rook, J. The accuracy of noninvasive and continuous total hemoglobin measurement by pulse CO-Oximetry in human subjects undergoing hemodilution. Anesth. Analg. 2010, 111, 1424–1426. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.D.; Chan, M.M.; Chan, M.M. Pulse oximetry: Understanding its basic principles facilitates appreciation of its limitations. Respir. Med. 2013, 107, 789–799. [Google Scholar] [CrossRef] [Green Version]
- Nitzan, M.; Romem, A.; Koppel, R. Pulse oximetry: Fundamentals and technology update. Med. Devices 2014, 7, 231–239. [Google Scholar] [CrossRef]
- Miller, R.D.; Ward, T.A.; Shiboski, S.C.; Cohen, N.H. A Comparison of three methods of hemoglobin monitoring in patients undergoing spine surgery. Anesth. Analg. 2011, 112, 858–863. [Google Scholar] [CrossRef]
- Shabaninejad, H.; Ghadimi, N.; Sayehmiri, K.; Hosseinifard, H.; Azarfarin, R.; Gorji, H.A. Comparison of invasive and noninvasive blood hemoglobin measurement in the operating room: A systematic review and meta-analysis. J. Anesth. 2019, 33, 441–453. [Google Scholar] [CrossRef]
- Isosu, T.; Obara, S.; Hosono, A.; Ohashi, S.; Nakano, Y.; Imaizumi, T.; Mogami, M.; Murakawa, M. Validation of continuous and noninvasive hemoglobin monitoring by pulse CO-oximetry in Japanese surgical patients. J. Clin. Monit. Comput. 2013, 27, 55–60. [Google Scholar] [CrossRef]
- Kim, S.H.; Lilot, M.; Murphy, L.S.; Sidhu, K.S.; Yu, Z.; Rinehart, J.; Cannesson, M. Accuracy of continuous noninvasive hemoglobin monitoring: A systematic review and meta-analysis. Anesth. Analg. 2014, 119, 332–346. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, B.V.; Vincent, J.L.; Nowak, E.; Coat, M.; Paleiron, N.; Gouny, P.; Ould-Ahmed, M.; Guillouet, M.; Arvieux, C.C.; Gueret, G. The accuracy of noninvasive hemoglobin measurement by multiwavelength pulse oximetry after cardiac surgery. Anesth. Analg. 2011, 113, 1052–1057. [Google Scholar] [CrossRef] [PubMed]
- Barker, S.J.; Shander, A.; Ramsay, M.A. Continuous noninvasive hemoglobin monitoring: A measured response to a critical review. Anesth. Analg. 2016, 122, 565–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, W.; Iain, C. Respiration: Gas transfer. Anaesth. Intensive Care Med. 2005, 6, 363–366. [Google Scholar]
- Kuznetsova, D.V.; Kulikov, V.P. Cerebrovascular and systemic hemodynamic response to carbon dioxide in humans. Blood Press. Monit. 2014, 19, 81–89. [Google Scholar] [CrossRef]
- Walløe, L. Arterio-venous anastomoses in the human skin and their role in temperature control. Temperature 2016, 3, 92–103. [Google Scholar] [CrossRef] [Green Version]
- Cicha, I.; Suzuki, Y.; Tateishi, N.; Maeda, N. Changes of RBC aggregation in oxygenation-deoxygenation: pH dependency and cell morphology. Am. J. Physiol. Heart Circ. Physiol. 2003, 284, H2335–H2342. [Google Scholar] [CrossRef]
- Berkow, L. Factors affecting hemoglobin measurement. J. Clin. Monit. Comput. 2013, 27, 499–508. [Google Scholar] [CrossRef]
- Basaranoglu, G.; Bakan, M.; Umutoglu, T.; Zengin, S.U.; Idin, K.; Salihoglu, Z. Comparison of SpO2 values from different fingers of the hands. Springerplus 2015, 4, 561. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low CO2 Group (n = 32) | High CO2 Group (n = 32) | p-Value | |
|---|---|---|---|
| Age (yr) | 62 ± 14 | 61 ± 12 | 0.871 |
| Height (cm) | 165.6 ± 8.8 | 166.1 ± 7.4 | 0.808 |
| Weight (kg) | 67.6 ± 12.3 | 66.8 ± 10.6 | 0.800 |
| Sex (male/female) | 27/5 | 27/5 | >0.999 |
| ASA physical status (1/2/3) | 15/14/3 | 15/14/3 | >0.999 |
| Diabetes | 4 (13%) | 8 (25%) | 0.200 |
| COPD | 0 | 2 (6%) | 0.492 |
| Crystalloid + colloid (mL) | 1575 (1453−1775) | 1600 (1200−2075) | 0.962 |
| Urine (mL) | 165 (110−308) | 138 (95−290) | 0.629 |
| Bleeding (mL) | 100 (100−150) | 100 (100−150) | 0.482 |
| Infusion of norepinephrine | 4 (13%) | 6 (19%) | 0.491 |
| Infusion of isosorbide dinitrate | 2 (6%) | 2 (6%) | >0.999 |
| Perfusion index (%) | 3.9 ± 2.0 | 4.2 ± 2.5 | 0.145 |
| SpHb (g/dL) | 10.6 ± 1.2 | 11.2 ± 1.2 | <0.001 |
| tHb (g/dL) | 11.7 ± 1.4 | 12.2 ± 1.1 | 0.003 |
| EtCO2 (mmHg) | 31.8 ± 2.3 | 42.0 ± 2.9 | <0.001 |
| PaCO2 (mmHg) | 32.0 ± 3.2 | 42.3 ± 4.6 | <0.001 |
| Pneumoperitoneum time (min) | 131 (116−145) | 119 (98−156) | 0.383 |
| Anesthesia time (min) | 198 ± 37 | 188 ± 46 | 0.351 |
| PACU profiles | |||
| Pain score | 7 (6−8) | 7 (6.5−9) | |
| Nausea (1/2/3/4) | 2/26/3/0 | 1/30/1/0 | |
| Vomiting | 0 | 1 (3%) | |
| Antiemetics | 3 (10%) | 1 (3%) | |
| Analgesics | 29 (94%) | 30 (94%) | |
| Duration of PACU stay (min) | 50 (40−60) | 50 (40−55) |
| Bias (95% CI) (g/dL) | SD (g/dL) | |
|---|---|---|
| PaCO2 < 35 mmHg | −1.09 (−1.28 to −0.90) | 1.06 |
| 35 ≤ PaCO2 < 45 mmHg | −0.97 (−1.17 to −0.76) | 1.22 |
| 45 mmHg ≤ PaCO2 * | −1.59 (−1.99 to −1.19) | 1.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, H.-Y.; Choi, J.-B.; Han, S.-U.; Lee, H.-S.; Lee, K.; Kim, J.-E. Impact of Increased End-Tidal Carbon Dioxide on Continuous Noninvasive Hemoglobin Monitoring during Laparoscopic Gastrectomy: A Randomized Controlled Study. J. Pers. Med. 2022, 12, 160. https://doi.org/10.3390/jpm12020160
Kim H-Y, Choi J-B, Han S-U, Lee H-S, Lee K, Kim J-E. Impact of Increased End-Tidal Carbon Dioxide on Continuous Noninvasive Hemoglobin Monitoring during Laparoscopic Gastrectomy: A Randomized Controlled Study. Journal of Personalized Medicine. 2022; 12(2):160. https://doi.org/10.3390/jpm12020160
Chicago/Turabian StyleKim, Ha-Yeon, Jong-Bum Choi, Sang-Uk Han, Hye-Sun Lee, Kyuhyeok Lee, and Ji-Eun Kim. 2022. "Impact of Increased End-Tidal Carbon Dioxide on Continuous Noninvasive Hemoglobin Monitoring during Laparoscopic Gastrectomy: A Randomized Controlled Study" Journal of Personalized Medicine 12, no. 2: 160. https://doi.org/10.3390/jpm12020160
APA StyleKim, H.-Y., Choi, J.-B., Han, S.-U., Lee, H.-S., Lee, K., & Kim, J.-E. (2022). Impact of Increased End-Tidal Carbon Dioxide on Continuous Noninvasive Hemoglobin Monitoring during Laparoscopic Gastrectomy: A Randomized Controlled Study. Journal of Personalized Medicine, 12(2), 160. https://doi.org/10.3390/jpm12020160