
The Paris System for Reporting Urinary Cytology: A Meta-Analysis

 , , ,
, , ,
Abstract
:1. Introduction
- Calculate the pooled risk of high-grade malignancy (ROHM) of each of the categories of TPS.
- Display the diagnostic accuracy of urine cytology reported with TPS, by:
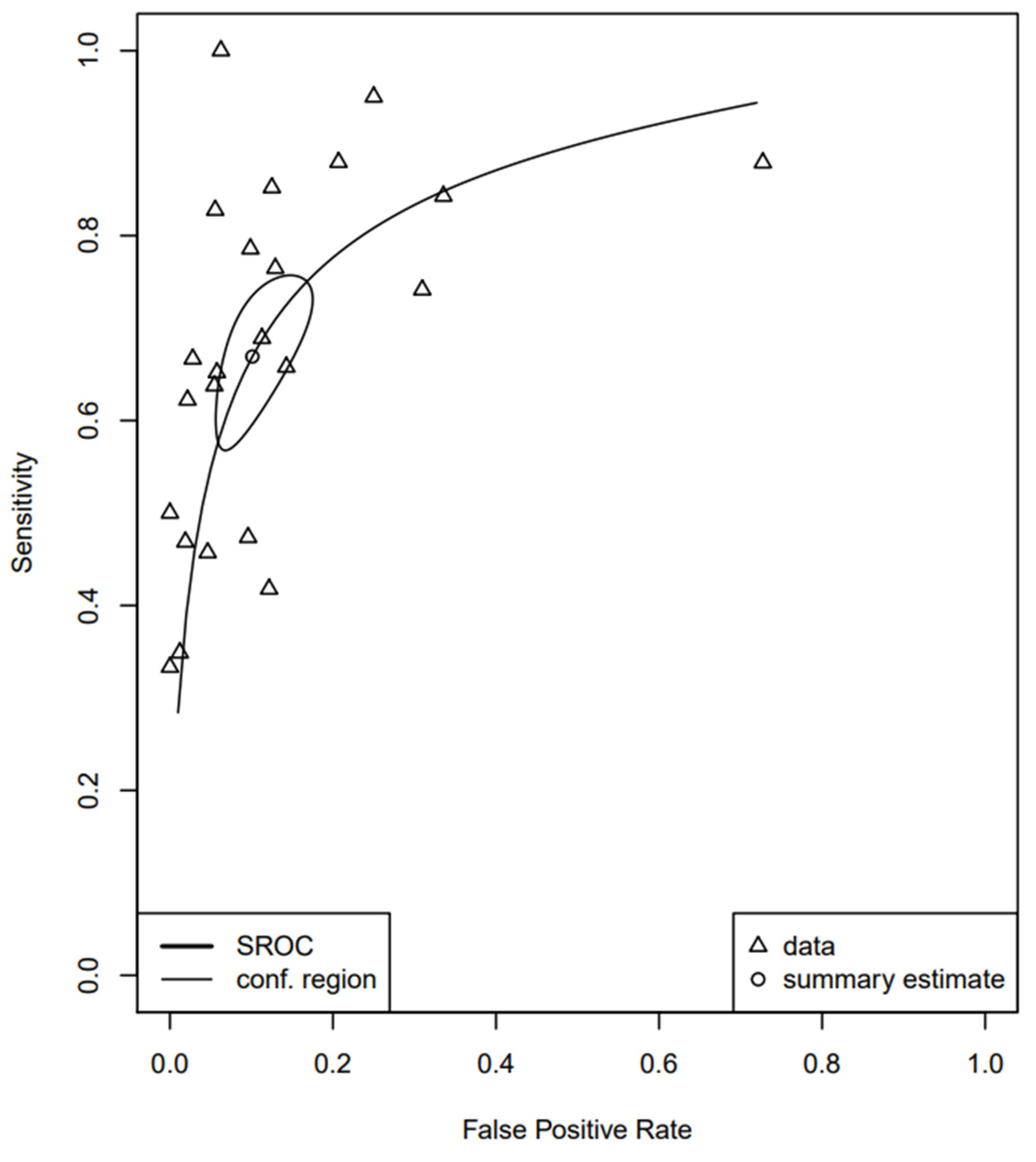
- Creating a pooled summary ROC (sROC) curve and subsequently estimating the pooled sensitivity and false-positive rate.
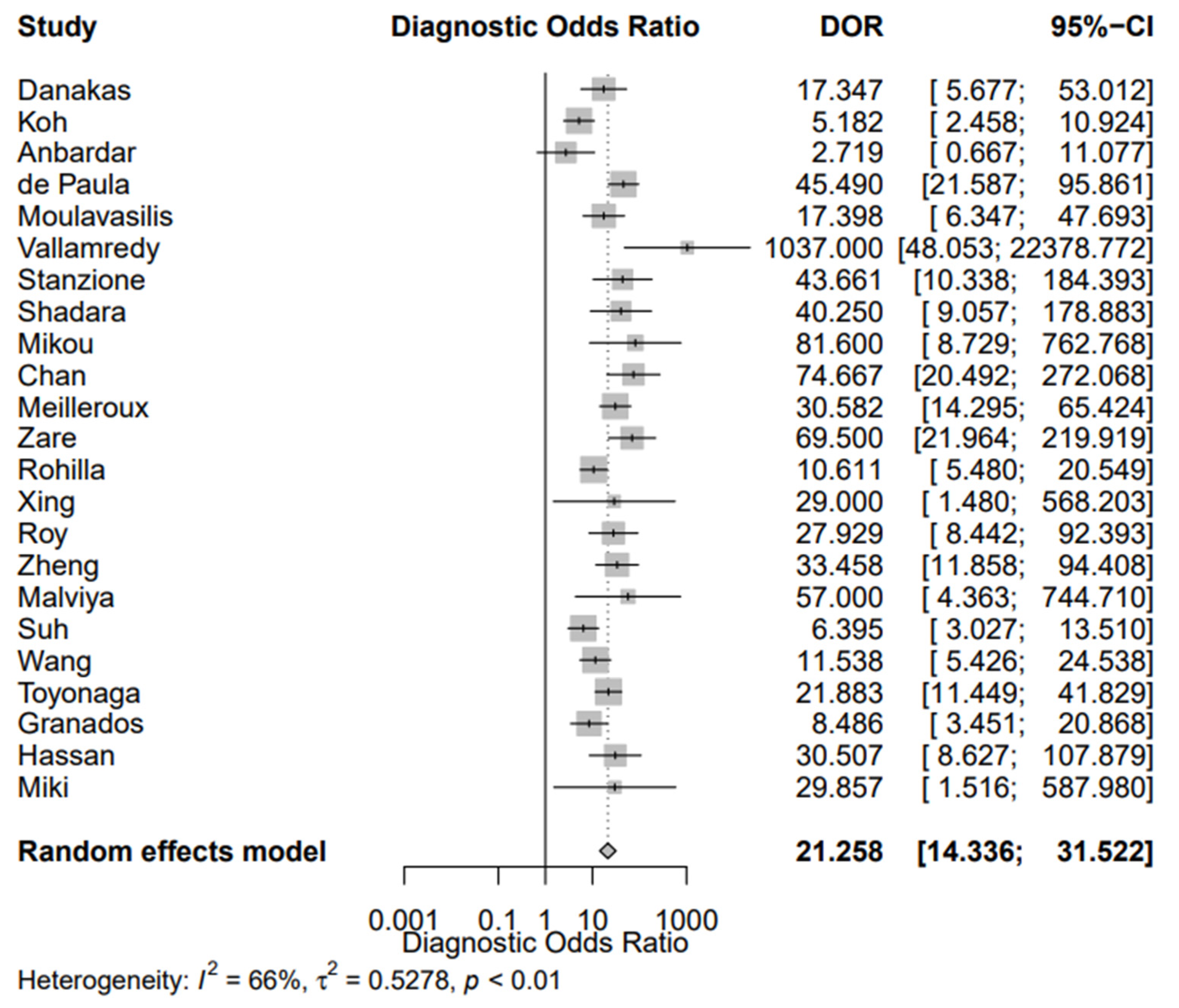
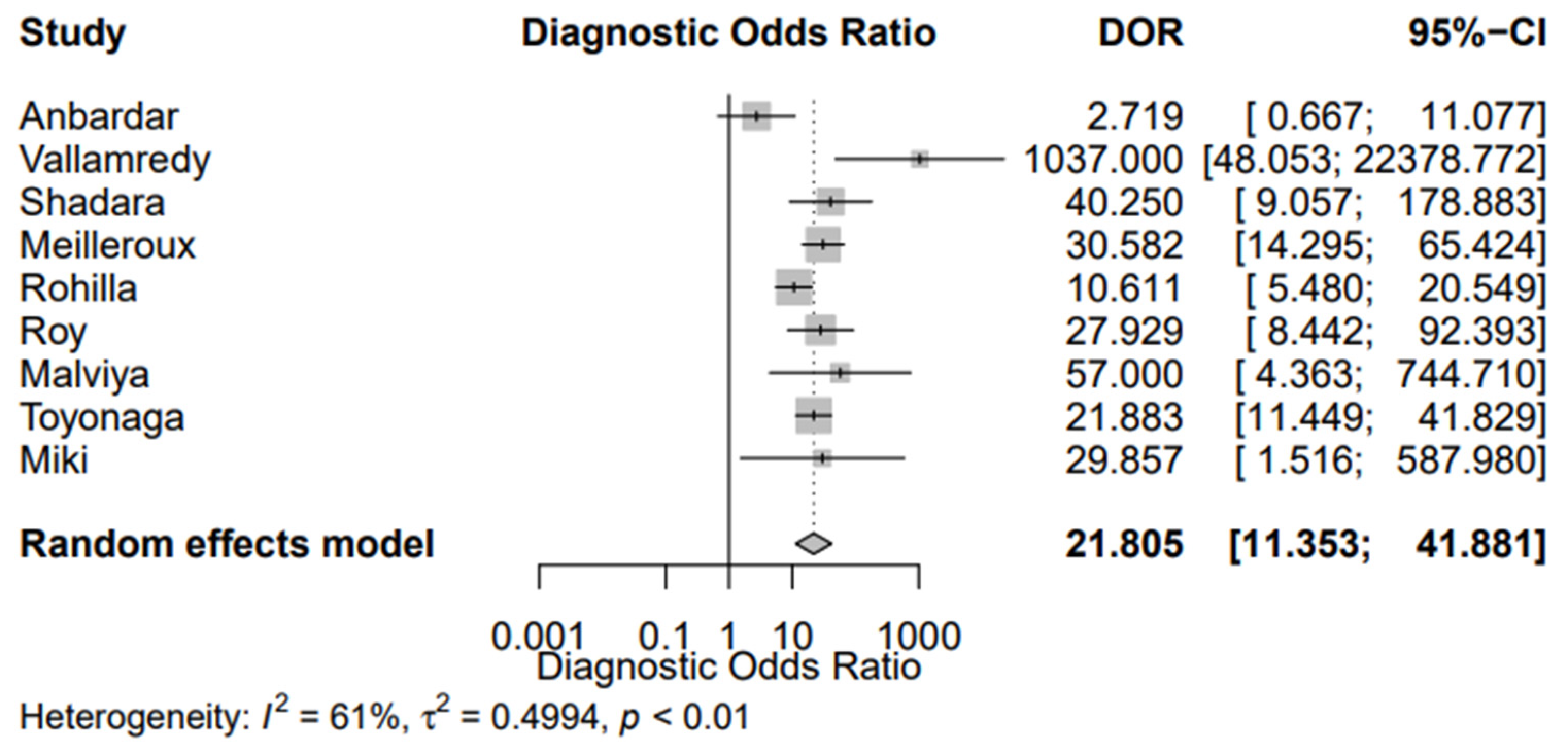
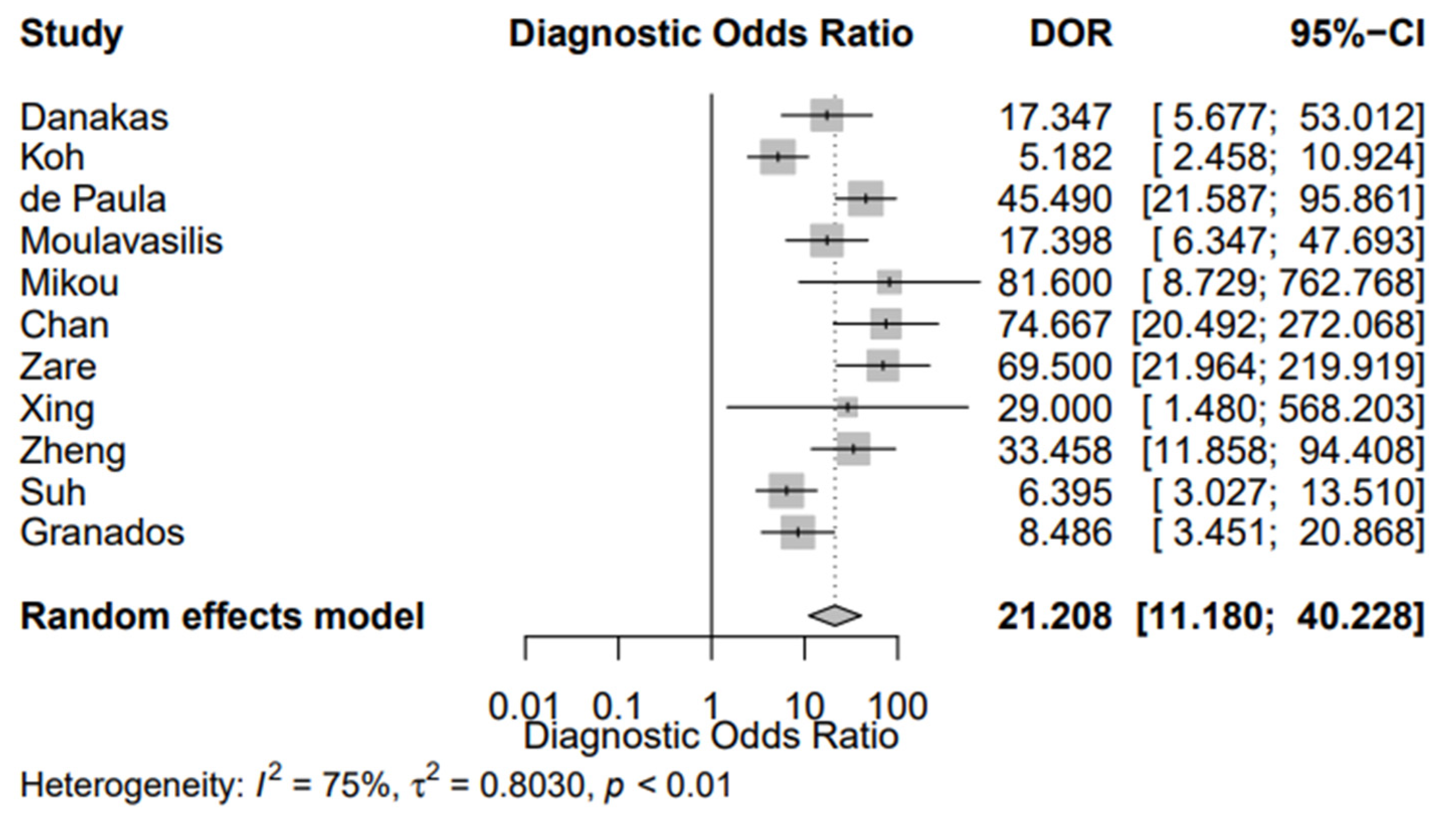
- Calculating the pooled Diagnostic Odds Ratio (DOR).
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
- Studies on humans;
- Original studies;
- Follow-up present;
- Results reported with TPS.
- Review articles, conference abstracts, editorials, and case reports;
- Articles written in a language other than English;
- In vitro or animal studies;
- Inability to extract data;
- Potential data overlap with already included studies;
- All enrolled patients had cancer and/or all follow-up cases showed cancer (high selection bias).
2.3. Data Extraction
2.4. Study Quality Assessment
2.5. Statistical Analysis
3. Results
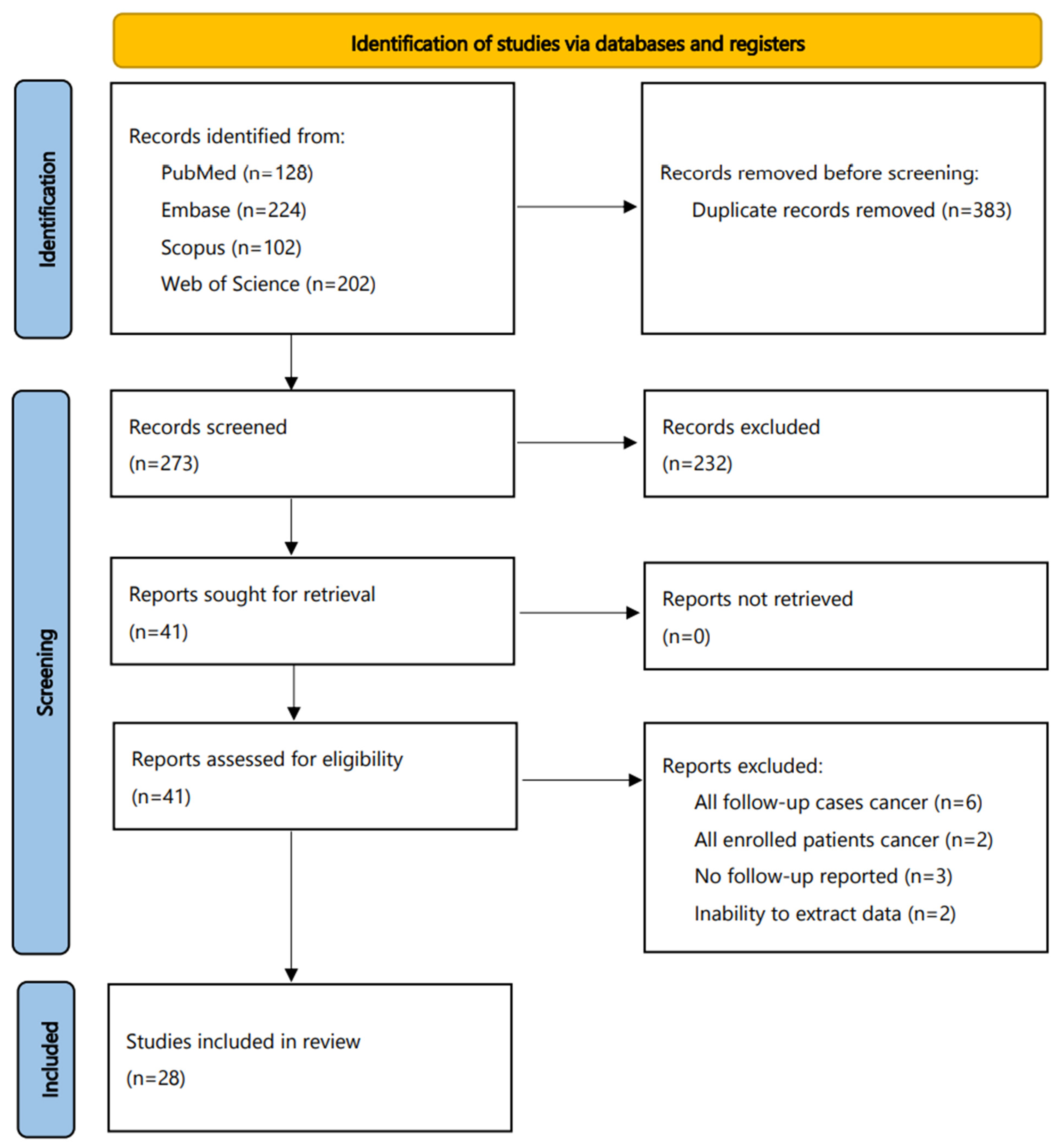
3.1. Literature Search
3.2. Characteristics of the Included Studies
3.3. ROHM of the Categories of TPS
3.4. Diagnostic Accuracy of Urine Cytology, Using TPS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Xing, J.; Reynolds, J.P. Diagnostic Advances in Urine Cytology. Surg. Pathol. Clin. 2018, 11, 601–610. [Google Scholar] [CrossRef] [PubMed]
- Van den Bussche, C.J. A Review of the Paris System for Reporting Urinary Cytology. Cytopathology 2016, 27, 153–156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Soualhi, A.; Rammant, E.; George, G.; Russell, B.; Enting, D.; Nair, R.; Van Hemelrijck, M.; Bosco, C. The Incidence and Prevalence of Upper Tract Urothelial Carcinoma: A Systematic Review. BMC Urol. 2021, 21, 110. [Google Scholar] [CrossRef]
- Chamie, K.; Litwin, M.S.; Bassett, J.C.; Daskivich, T.J.; Lai, J.; Hanley, J.M.; Konety, B.R.; Saigal, C.S. Urologic Diseases in America Project Recurrence of High-Risk Bladder Cancer: A Population-Based Analysis. Cancer 2013, 119, 3219–3227. [Google Scholar] [CrossRef] [Green Version]
- Gupta, M.; VandenBussche, C.J.; Bivalacqua, T.J. Urinary Cytology and the Paris System for Reporting Urinary Cytology: Implications for Urological Management. Cytopathology 2018, 29, 368–370. [Google Scholar] [CrossRef]
- Barkan, G.A.; Wojcik, E.M.; Nayar, R.; Savic-Prince, S.; Quek, M.L.; Kurtycz, D.F.I.; Rosenthal, D.L. The Paris System for Reporting Urinary Cytology: The Quest to Develop a Standardized Terminology. J. Am. Soc. Cytopathol. 2016, 23, 193–201. [Google Scholar]
- Cowan, M.L.; VandenBussche, C.J. The Paris System for Reporting Urinary Cytology: Early Review of the Literature Reveals Successes and Rare Shortcomings. J. Am. Soc. Cytopathol. 2018, 7, 185–194. [Google Scholar] [CrossRef]
- Vlajnic, T.; Gut, A.; Savic, S.; Bubendorf, L. The Paris System for Reporting Urinary Cytology in Daily Practice with Emphasis on Ancillary Testing by Multiprobe FISH. J. Clin. Pathol. 2019, 73, 90–95. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Campbell, J.M.; Klugar, M.; Ding, S.; Carmody, D.P.; Hakonsen, S.J.; Jadotte, Y.T.; White, S.; Munn, Z. Diagnostic Test Accuracy: Methods for Systematic Review and Meta-Analysis. Int. J. Evid. Based Healthc. 2015, 13, 154–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abro, S.; Nomani, L.; Wojcik, E.M.; Pambuccian, S.E.; Chatt, G.; Barkan, G.A. Outcome Analysis and Negative Predictive Value of the “Unsatisfactory/nondiagnostic” Category of The Paris System for Reporting Urinary Cytology. J. Am. Soc. Cytopathol. 2021, 10, 64–70. [Google Scholar] [CrossRef]
- McIntire, P.J.; Kilic, I.; Pambuccian, S.E.; Wojcik, E.M.; Barkan, G.A. The Paris System for Reporting Urinary Cytology Reduces Atypia Rates and Does Not Alter the Negative Predictive Value of Urine Cytology. J. Am. Soc. Cytopathol. 2021, 10, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Danakas, A.; Sweeney, M.; Cheris, S.; Agrawal, T. Urinary Tract Cytology: A Cytologic-Histopathologic Correlation with the Paris System, an Institutional Study. J. Am. Soc. Cytopathol. 2021, 10, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.; Nilforoushan, N.; Krane, J.F.; Bose, S.; Bakkar, R. Should “Suspicious for High-Grade Urothelial Carcinoma” and “Positive for High-Grade Urothelial Carcinoma” Remain Separate Categories? Cancer Cytopathol. 2020, 129, 156–163. [Google Scholar] [CrossRef]
- Koh, H.H.; Lee, M.J.; Park, N.J.; Kim, H.-S.; Oh, Y.L. Impact of Implementing the Paris System for Reporting Urinary Cytology: A Single-Institutional Experience with Emphasis on Diagnostic Yield of High-Grade Urothelial Carcinoma and Low-Grade Urothelial Neoplasm. Anticancer Res. 2020, 40, 3477–3484. [Google Scholar] [CrossRef]
- Anbardar, M.H.; Monjazeb, R. Reclassification of Urinary Cytology Regarding the Paris System for Reporting Urinary Cytology with Cytohistological Correlation Demonstrates High Sensitivity for High-Grade Urothelial Carcinoma. Diagn. Cytopathol. 2020, 48, 446–452. [Google Scholar] [CrossRef]
- Kuan, K.C.; Segura, S.E.; Ahlstedt, J.; Khader, S.N.; Hakima, L. The Predictive Value of Positive and Suspicious Urine Cytology: Are They Different? Diagn. Cytopathol. 2020, 48, 998–1002. [Google Scholar] [CrossRef]
- de Paula, R.; Oliveira, A.; Nunes, W.; Bovolim, G.; Domingos, T.; De Brot, L.; Bezerra, S.; Cunha, I.; Morini, M.; Saieg, M. Two-Year Study on the Application of the Paris System for Urinary Cytology in a Cancer Centre. Cytopathology 2020, 31, 41–46. [Google Scholar] [CrossRef]
- Moulavasilis, N.; Lazaris, A.; Katafigiotis, I.; Stravodimos, K.; Constantinides, C.; Mikou, P. Risk of Malignancy Assessment for the Paris System for Reporting Urinary Cytology. Diagn. Cytopathol. 2020, 48, 1194–1198. [Google Scholar] [CrossRef] [PubMed]
- Begam, K.V.; Vallamreddy, S.K.R.; Pratima, J. Implementation of the Paris System versus Institutional Diagnosis in the Performance of Urinary Cytology: A 5 Years Correlative Study of 74 Cases. IP Arch. Cytol. Histopathol. Res. 2019, 4, 193–198. [Google Scholar] [CrossRef]
- Stanzione, N.; Ahmed, T.; Fung, P.C.; Cai, D.; Lu, D.Y.; Sumida, L.C.; Moatamed, N.A. The Continual Impact of the Paris System on Urine Cytology, a 3-Year Experience. Cytopathology 2019, 31, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.; Lali, B.S.; Venkataramana, C.G.; Philipose, C.S.; Rao, R.; Prabhu, G.L. A Quest for Accuracy: Evaluation of The Paris System in Diagnosis of Urothelial Carcinomas. J. Cytol. 2019, 36, 169–173. [Google Scholar] [PubMed]
- Mikou, P.; Lenos, M.; Papaioannou, D.; Vrettou, K.; Trigka, E.-A.; Sousouris, S.; Constantinides, C. Evaluation of the Paris System in Atypical Urinary Cytology. Cytopathology 2018, 29, 545–549. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.; Balassanian, R.; Tabatabai, Z.L.; Lou, H.; Vohra, P. Improved Diagnostic Precision of Urine Cytology by Implementation of The Paris System and the Use of Cell Blocks. Cancer Cytopathol. 2018, 126, 809–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meilleroux, J.; Daniel, G.; Aziza, J.; d’Aure, D.M.; Quintyn-Ranty, M.-L.; Basset, C.M.L.; Evrard, S.M.; Courtade-Saidi, M.M. One Year of Experience Using the Paris System for Reporting Urinary Cytology. Cancer Cytopathol. 2018, 126, 430–436. [Google Scholar] [CrossRef] [Green Version]
- Zare, S.; Mirsadraei, L.; Reisian, N.; Liao, X.; Roma, A.; Shabaik, A.; Hasteh, F. A Single Institutional Experience with the Paris System for Reporting Urinary Cytology: Correlation of Cytology and Histology in 194 Cases. Am. J. Clin. Pathol. 2018, 150, 162–167. [Google Scholar] [CrossRef]
- Rohilla, M.; Singh, P.; Rajwanshi, A.; Gupta, N.; Srinivasan, R.; Dey, P.; Kakkar, N. Cytohistological Correlation of Urine Cytology in a Tertiary Centre with Application of the Paris System. Cytopathology 2018, 29, 436–443. [Google Scholar] [CrossRef]
- Xing, J.; Monaco, S.E.; Pantanowitz, L. Utility of the Paris System for Reporting Urinary Cytology in Upper Urinary Tract Specimens. J. Am. Soc. Cytopathol. 2018, 7, 311–317. [Google Scholar] [CrossRef]
- Roy, M.; Kaushal, S.; Jain, D.; Seth, A.; Iyer, V.K.; Mathur, S.R. An Institutional Experience with The Paris System: A Paradigm Shift from Ambiguous Terminology to More Objective Criteria for Reporting Urine Cytology. Cytopathology 2017, 28, 509–515. [Google Scholar] [CrossRef] [PubMed]
- Zheng, X.; Si, Q.; Du, D.; Harshan, M.; Zhang, Z.; Haines, K., 3rd; Shi, W.; Chhieng, D.C. The Paris System for Urine Cytology in Upper Tract Urothelial Specimens: A Comparative Analysis with Biopsy and Surgical Resection. Cytopathology 2018, 29, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Malviya, K.; Fernandes, G.; Naik, L.; Kothari, K.; Agnihotri, M. Utility of the Paris System in Reporting Urine Cytology. Acta Cytol. 2017, 61, 145–152. [Google Scholar] [CrossRef]
- Suh, J.; Go, H.; Sung, C.; Baek, S.; Hwang, H.; Jeong, S.; Cho, Y. Modification of The Paris System for Urinary Tract Washing Specimens Using Diagnostic Cytological Features. Cytopathology 2017, 28, 516–523. [Google Scholar] [CrossRef]
- Wang, Y.; Auger, M.; Kanber, Y.; Caglar, D.; Brimo, F. Implementing the Paris System for Reporting Urinary Cytology Results in a Decrease in the Rate of the “atypical” Category and an Increase in Its Prediction of Subsequent High-Grade Urothelial Carcinoma. Cancer Cytopathol. 2017, 126, 207–214. [Google Scholar] [CrossRef]
- Toyonaga, Y.; Yamazaki, K.; Koyama, Y.; Yamada, M.; Ishida, Y. A Modified Direct-Smear Processing Technique Employing Two-Step Centrifugation/Fixation Is Useful for Detecting High-Grade Urothelial Carcinoma. Acta Cytol. 2017, 61, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Granados, R.; Duarte, J.A.; Corrales, T.; Camarmo, E.; Bajo, P. Applying the Paris System for Reporting Urine Cytology Increases the Rate of Atypical Urothelial Cells in Benign Cases: A Need for Patient Management Recommendations. Acta Cytol. 2016, 61, 71–76. [Google Scholar] [CrossRef]
- Hassan, M.; Solanki, S.; Kassouf, W.; Kanber, Y.; Caglar, D.; Auger, M.; Brimo, F. Impact of Implementing the Paris System for Reporting Urine Cytology in the Performance of Urine Cytology: A Correlative Study of 124 Cases. Am. J. Clin. Pathol. 2016, 146, 384–390. [Google Scholar] [CrossRef]
- Miki, Y.; Neat, M.; Chandra, A. Application of The Paris System to Atypical Urine Cytology Samples: Correlation with Histology and UroVysion (R) FISH. Cytopathology 2016, 28, 88–95. [Google Scholar] [CrossRef]
- Joudi, A.M.; Pambuccian, S.E.; Wojcik, E.M.; Barkan, G.A. The Positive Predictive Value of “Suspicious for High-Grade Urothelial Carcinoma” in Urinary Tract Cytology Specimens: A Single-Institution Study of 665 Cases. Cancer Cytopathol. 2016, 124, 811–819. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2 Group QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring Inconsistency in Meta-Analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holling, H.; Böhning, W.; Böhning, D. Meta-Analysis of Diagnostic Studies Based upon SROC-Curves: A Mixed Model Approach Using the Lehmann Family. Stat. Model. 2012, 12, 347–375. [Google Scholar] [CrossRef]
- Reitsma, J.B.; Glas, A.S.; Rutjes, A.W.S.; Scholten, R.J.P.M.; Bossuyt, P.M.; Zwinderman, A.H. Bivariate Analysis of Sensitivity and Specificity Produces Informative Summary Measures in Diagnostic Reviews. J. Clin. Epidemiol. 2005, 58, 982–990. [Google Scholar] [CrossRef]
- Jones, C.M.; Athanasiou, T. Summary Receiver Operating Characteristic Curve Analysis Techniques in the Evaluation of Diagnostic Tests. Ann. Thorac. Surg. 2005, 79, 16–20. [Google Scholar] [CrossRef]
- McIntire, P.J.; Snow, J.T.; Robinson, B.D.; Rao, R.A.; Goyal, A.; Heymann, J.J.; Siddiqui, M.T. Improved Correlation of Urinary Cytology Specimens Using the Paris System in Biopsy-Proven Upper Tract Urothelial Carcinomas. Cancer Cytopathol. 2018, 126, 498–504. [Google Scholar] [CrossRef] [Green Version]
- Bertsch, E.C.; Siddiqui, M.T.; Ellis, C.L. The Paris System for Reporting Urinary Cytology Improves Correlation with Surgical Pathology Biopsy Diagnoses of the Lower Urinary Tract. Diagn. Cytopathol. 2018, 46, 221–227. [Google Scholar] [CrossRef]
- Torous, V.F.; Brancely, D.; VanderLaan, P.A. Implementation of the Paris System for Reporting Urinary Cytology Results in Lower Atypical Diagnostic Rates. J. Am. Soc. Cytopathol. 2017, 6, 205–210. [Google Scholar] [CrossRef]
- Hang, J.-F.; Charu, V.; Zhang, M.L.; VandenBussche, C.J. Digital Image Analysis Supports a Nuclear-to-Cytoplasmic Ratio Cutoff Value of 0.5 for Atypical Urothelial Cells. Cancer Cytopathol. 2017, 125, 710–716. [Google Scholar] [CrossRef] [Green Version]
- Rohra, P.; Ocampo Gonzalez, F.A.; Yan, L.; Mir, F.; Furlan, K.; Basu, S.; Barua, A.; Cheng, L.; Park, J.-W. Effect of the Paris System for Reporting Urinary Cytology with Histologic Follow-Up. Diagn. Cytopathol. 2021, 49, 691–699. [Google Scholar] [CrossRef]
- Tian, W.; Shore, K.T.; Shah, R.B. Significant Reduction of Indeterminate (atypical) Diagnosis after Implementation of The Paris System for Reporting Urinary Cytology: A Single-Institution Study of More than 27,000 Cases. Cancer Cytopathol. 2021, 129, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Pierconti, F.; Martini, M.; Straccia, P.; Fiorentino, V.; Musarra, T.; Larocca, L.M.; Lopez-Beltran, A. Hypochromatic Large Urothelial Cells in Urine Cytology Are Indicative of High Grade Urothelial Carcinoma. APMIS 2018, 126, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Kurtycz, D.F.I.; Sundling, K.E.; Barkan, G.A. The Paris System of Reporting Urinary Cytology: Strengths and Opportunities. Diagn. Cytopathol. 2020, 48, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Suo, L.; Vega, I.; Thrall, M. Cyto-Histo Correlations of Plasmacytoid and Micropapillary Variants of High-Grade Urothelial Carcinoma: Do They Fit Well in The Paris System for Reporting Urinary Cytology? J. Am. Soc. Cytopathol. 2021, 10, 20–24. [Google Scholar] [CrossRef] [PubMed]
- Simon, C.T.; Skala, S.L.; Magers, M.J.; Weizer, A.; Kaffenberger, S.D.; Chinnaiyan, A.M.; Spratt, D.E.; Montgomery, J.; Mehra, R.; Lew, M. The Utility of Upper Urinary Tract Urine Cytology before and after Application of the Paris System. Diagn. Cytopathol. 2018, 47, 421–427. [Google Scholar] [CrossRef] [PubMed]
- Virk, R.K.; Abro, S.; de Ubago, J.M.M.; Pambuccian, S.E.; Quek, M.L.; Wojcik, E.M.; Mehrotra, S.; Chatt, G.U.; Barkan, G.A. The Value of the UroVysion® FISH Assay in the Risk-Stratification of Patients with “atypical Urothelial Cells” in Urinary Cytology Specimens. Diagn. Cytopathol. 2017, 45, 481–500. [Google Scholar] [CrossRef]
- Rodriguez Pena, M.D.C.; Springer, S.U.; Taheri, D.; Li, L.; Tregnago, A.C.; Eich, M.-L.; Eltoum, I.-E.A.; VandenBussche, C.J.; Papadopoulos, N.; Kinzler, K.W.; et al. Performance of Novel Non-Invasive Urine Assay UroSEEK in Cohorts of Equivocal Urine Cytology. Virchows Arch. 2019, 476, 423–429. [Google Scholar] [CrossRef]
- Zhang, M.L.; Guo, A.X.; VandenBussche, C.J. Morphologists Overestimate the Nuclear-to-Cytoplasmic Ratio. Cancer Cytopathol. 2016, 124, 669–677. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.-H.; Hang, J.-F.; Wen, C.-H.; Liao, K.-C.; Lee, W.-Y.; Lai, C.-R. Diagnostic Agreement for High-Grade Urothelial Cell Carcinoma in Atypical Urine Cytology: A Nationwide Survey Reveals a Tendency for Overestimation in Specimens with an N/C Ratio Approaching 0.5. Cancers 2020, 12, 272. [Google Scholar] [CrossRef] [Green Version]
- Xie, Q.; Huang, Z.; Zhu, Z.; Zheng, X.; Liu, J.; Zhang, M.; Zhang, Y. Diagnostic Value of Urine Cytology in Bladder Cancer. A Meta-Analysis. Anal. Quant. Cytopathol. Histpathol. 2016, 38, 38–44. [Google Scholar]
- Luo, Y.; She, D.-L.; Xiong, H.; Yang, L.; Fu, S.-J. Diagnostic Value of Liquid-Based Cytology in Urothelial Carcinoma Diagnosis: A Systematic Review and Meta-Analysis. PLoS ONE 2015, 10, e0134940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, C.J.; Pambuccian, S.E.; Barkan, G.A. Split-Sample Comparison of Urothelial Cells in ThinPrep and Cytospin Preparations in Urinary Cytology: Do We Need to Adjust the Paris System for Reporting Urinary Cytology Criteria? Cancer Cytopathol. 2020, 128, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Straccia, P.; Bizzarro, T.; Fadda, G.; Pierconti, F. Comparison between Cytospin and Liquid-Based Cytology in Urine Specimens Classified according to the Paris System for Reporting Urinary Cytology. Cancer Cytopathol. 2016, 124, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Farahani, S.J.; Baloch, Z. Retrospective Assessment of the Effectiveness of the Milan System for Reporting Salivary Gland Cytology: A Systematic Review and Meta-Analysis of Published Literature. Diagn. Cytopathol. 2019, 47, 67–87. [Google Scholar] [CrossRef]
- Hoda, R.S.; Finer, E.B.; Arpin, R.N., 3rd; Rosenbaum, M.; Pitman, M.B. Risk of Malignancy in the Categories of the Papanicolaou Society of Cytopathology System for Reporting Pancreaticobiliary Cytology. J. Am. Soc. Cytopathol. 2019, 8, 120–127. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author/Year/Reference | Study Period | Country | Specimen Type | Lower vs. Upper Tract | Cytopreparation Type | Initial Dx or Reclassification | Reference Standard | Total Cases | Cases with Follow-Up |
|---|---|---|---|---|---|---|---|---|---|
| Abro, 2021 [13] | 3 years | USA | Voided and Instrumented | Lower and Upper | LBC | Initial | Histology and follow-up cytology | 230 | 116 |
| McIntire, 2021 [14] | 2 years | USA | Voided and Instrumented | Lower and Upper | LBC | Initial | Histology and follow-up cytology | 2960 | 2960 |
| Danakas, 2021 [15] | 2 years | USA | Voided and Instrumented | NR | LBC | Initial | Histology | 170 | 170 |
| Nguyen, 2020 [16] | 3 years, 7 months | USA | Voided and Instrumented | Lower and Upper | LBC | Initial | Histology | 189 | 189 |
| Koh, 2020 [17] | 2 years | Korea | Voided | Lower | LBC | Reclassification | Histology | 299 | 299 |
| Anbardar, 2020 [18] | 2 years, 6 months | Iran | Voided | Lower | Conventional | Reclassification | Histology | 1842 | 55 |
| Kuan, 2020 [19] | 10 years, 5 months | USA | Voided and Instrumented | NR | Conventional | Initial | Histology | 378 | 378 |
| de Paula, 2020 [20] | 2 years | Brazil | Voided and Instrumented | NR | LBC | Initial | Histology | 1660 | 611 |
| Moulavasilis, 2020 [21] | 1 year | Greece | Voided and Instrumented | Lower | LBC | Initial | Histology | 110 | 110 |
| Vallamredy, 2019 [22] | 5 years | India | NR | NR | Conventional | Reclassification | Histology | 74 | 74 |
| Stanzione, 2019 [23] | 2 years, 7 months | USA | Voided and Instrumented | NR | NR | Initial | Histology | 3202 | 294 |
| Rai, 2019 [24] | 1 year | India | NR | NR | Conventional | Initial | Histology | 90 | 60 |
| Mikou, 2018 [25] | 1 year | Greece | Voided | Lower | LBC | Reclassification | Histology | 720 | 47 |
| Chan, 2018 [26] | 6 years | USA | Voided and Instrumented | Lower and Upper | LBC | Reclassification | Histology | 188 | 188 |
| Meilleroux, 2018 [27] | 2 years | France | Voided | Lower and Upper | Conventional | Initial | Histology | 1814 | 299 |
| Zare, 2018 [28] | 2 years | USA | Voided and Instrumented | Lower | LBC | Reclassification | Histology | 194 | 194 |
| Rohilla, 2018 [29] | 2 years | India | Voided | Lower and Upper | Conventional | Reclassification | Histology | 4188 | 244 |
| Xing, 2018 [30] | NR | USA | Instrumented | Upper | LBC | Reclassification | Histology | 30 | 30 |
| Roy, 2017 [31] | 10 months | India | Voided | Lower and Upper | Conventional | Reclassification | Histology | 255 | 97 |
| Zheng, 2017 [32] | 3 years, 4 months | USA | Instrumented | Upper | LBC | Reclassification | Histology | 324 | 125 |
| Malviya, 2017 [33] | 1 year | India | Voided and Instrumented | Lower and Upper | Conventional | Reclassification | Histology | 176 | 34 |
| Suh, 2017 [34] | 3 years | Korea | Instrumented | Lower and Upper | LBC | Reclassification | Histology | 142 | 142 |
| Wang, 2017 [35] | 1 year | Canada | Voided and Instrumented | NR | LBC and Conventional | Initial | Histology | 2392 | 167 |
| Toyonaga, 2017 [36] | 5 years, 8 months | Japan | Voided | Lower | Conventional | Reclassification | Histology | 287 | 287 |
| Granados, 2016 [37] | 3 years | Spain | Voided | NR | LBC | Reclassification | Histology | 149 | 149 |
| Hassan, 2016 [38] | 3 years | Canada | Voided and Instrumented | Lower | LBC and Conventional | Reclassification | Histology | 124 | 124 |
| Miki, 2016 [39] | 6 years | UK | Voided and Instrumented | Lower and Upper | Conventional | Reclassification | Histology | 91 | 45 |
| Joudi, 2016 [40] | 11 years | USA | Voided and Instrumented | Lower and Upper | LBC | Initial | Histology and follow-up cytology | 662 | 662 |
| Paris System Categories | No of Studies Pooled | ROHM (%) | 95% CI | Tau2 | Q | I2 (%) |
|---|---|---|---|---|---|---|
| Nondiagnostic | 11 | 17.70 | (0.0650; 0.3997) | 1.8070 | 29.22 | 72.6 |
| NHGUC | 24 | 13.04 | (0.0932; 0.1796) | 0.6056 | 355.67 | 87.3 |
| AUC | 23 | 38.65 | (0.3042; 0.4759) | 0.5272 | 84.57 | 76.4 |
| LGUN | 10 | 12.45 | (0.0431; 0.3101) | 1.1790 | 4.89 | 55.4 |
| SHGUC | 26 | 76.89 | (0.7063; 0.8216) | 0.3291 | 53.12 | 66.1% |
| HGUC and other malignancies | 25 | 91.79 | (0.8722; 0.9482) | 0.8732 | 92.36 | 82.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nikas, I.P.; Seide, S.; Proctor, T.; Kleinaki, Z.; Kleinaki, M.; Reynolds, J.P. The Paris System for Reporting Urinary Cytology: A Meta-Analysis. J. Pers. Med. 2022, 12, 170. https://doi.org/10.3390/jpm12020170
Nikas IP, Seide S, Proctor T, Kleinaki Z, Kleinaki M, Reynolds JP. The Paris System for Reporting Urinary Cytology: A Meta-Analysis. Journal of Personalized Medicine. 2022; 12(2):170. https://doi.org/10.3390/jpm12020170
Chicago/Turabian StyleNikas, Ilias P., Svenja Seide, Tanja Proctor, Zoi Kleinaki, Maria Kleinaki, and Jordan P. Reynolds. 2022. "The Paris System for Reporting Urinary Cytology: A Meta-Analysis" Journal of Personalized Medicine 12, no. 2: 170. https://doi.org/10.3390/jpm12020170
APA StyleNikas, I. P., Seide, S., Proctor, T., Kleinaki, Z., Kleinaki, M., & Reynolds, J. P. (2022). The Paris System for Reporting Urinary Cytology: A Meta-Analysis. Journal of Personalized Medicine, 12(2), 170. https://doi.org/10.3390/jpm12020170