
Simple and Efficient Pressure Ulcer Reconstruction via Primary Closure Combined with Closed-Incision Negative Pressure Wound Therapy (CiNPWT)—Experience of a Single Surgeon

 , , , , , , ,
, , , , , , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Device Application
2.2. Statistical Analysis
2.3. Clinical Outcomes
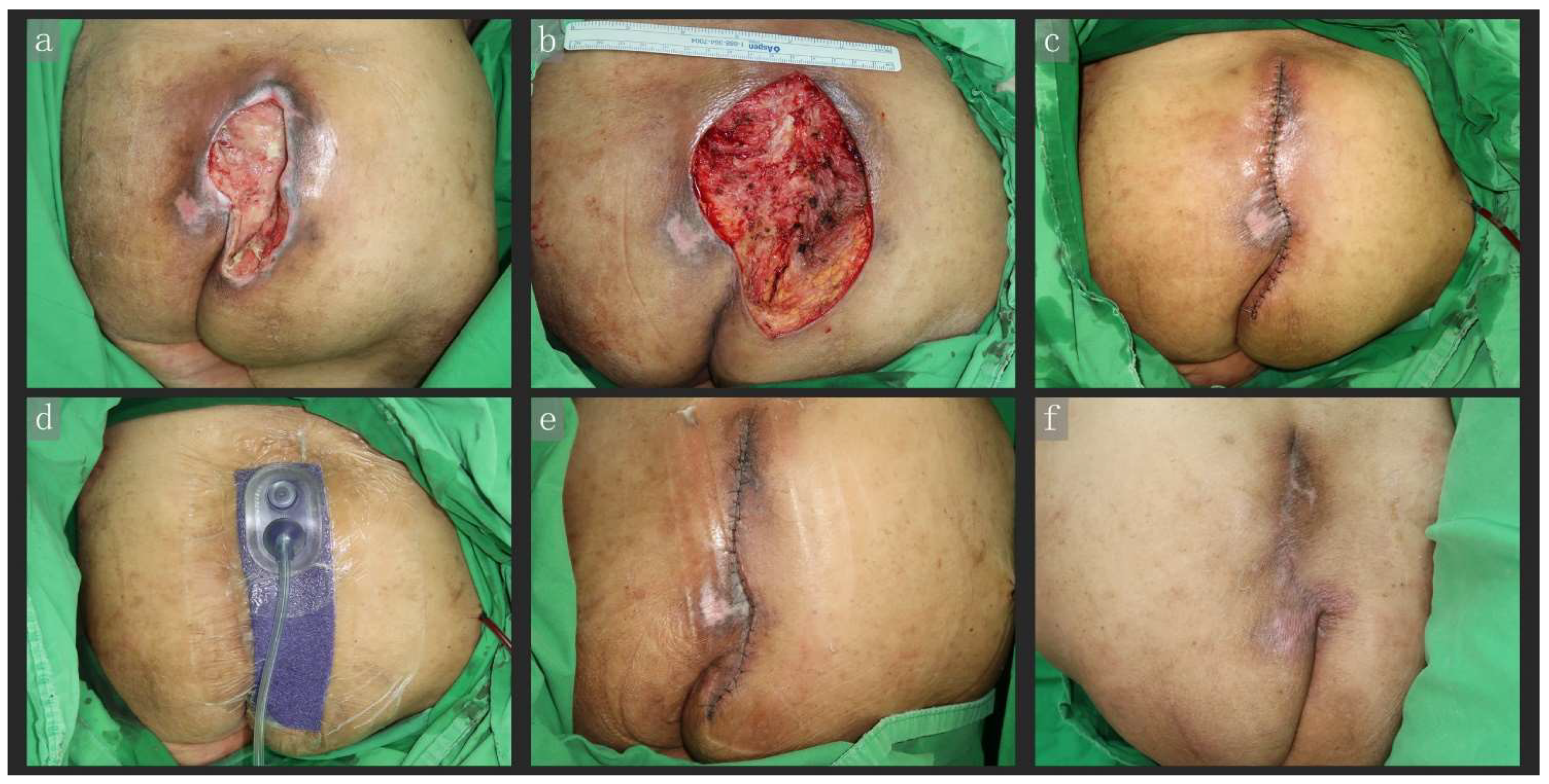
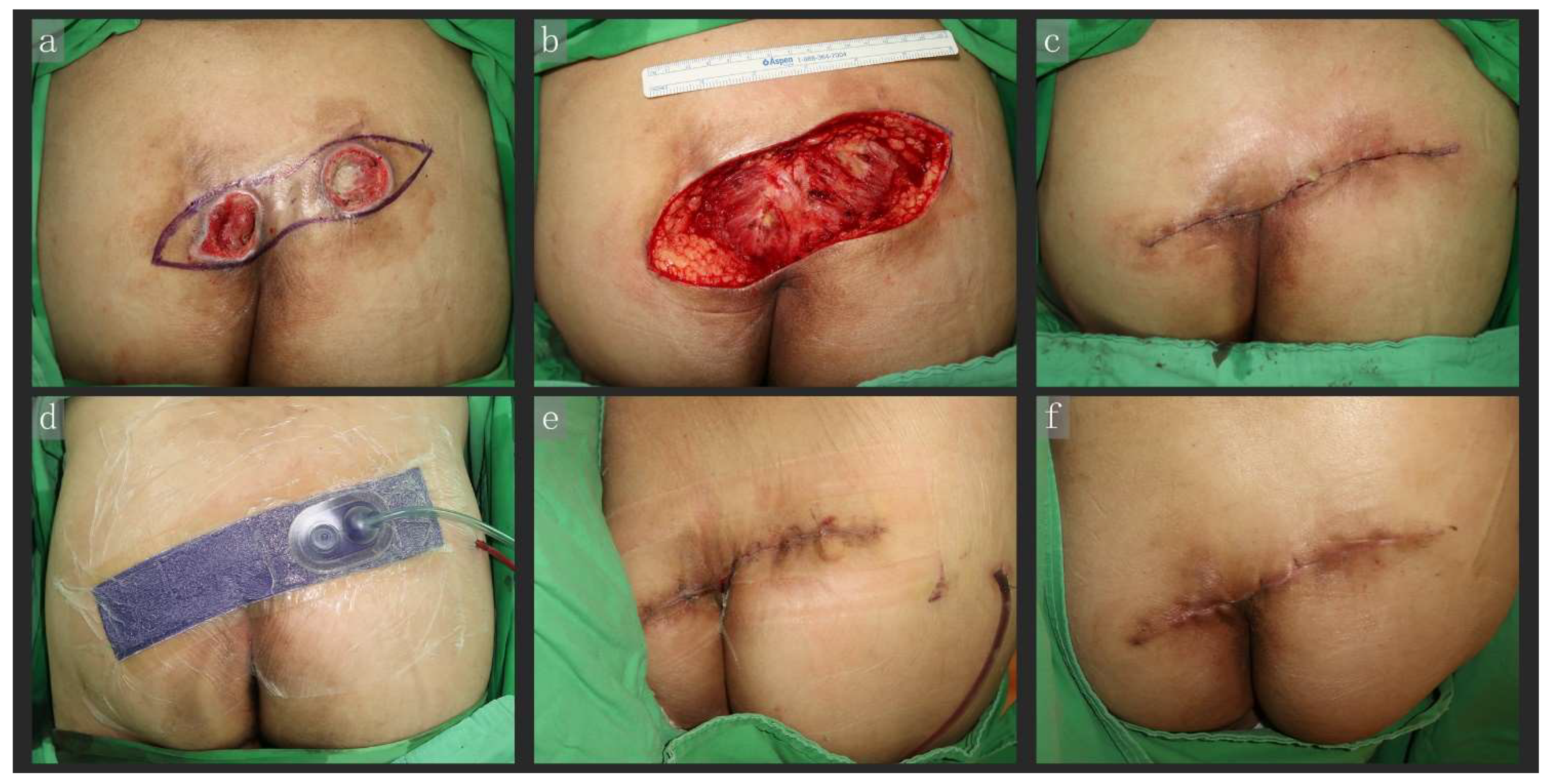
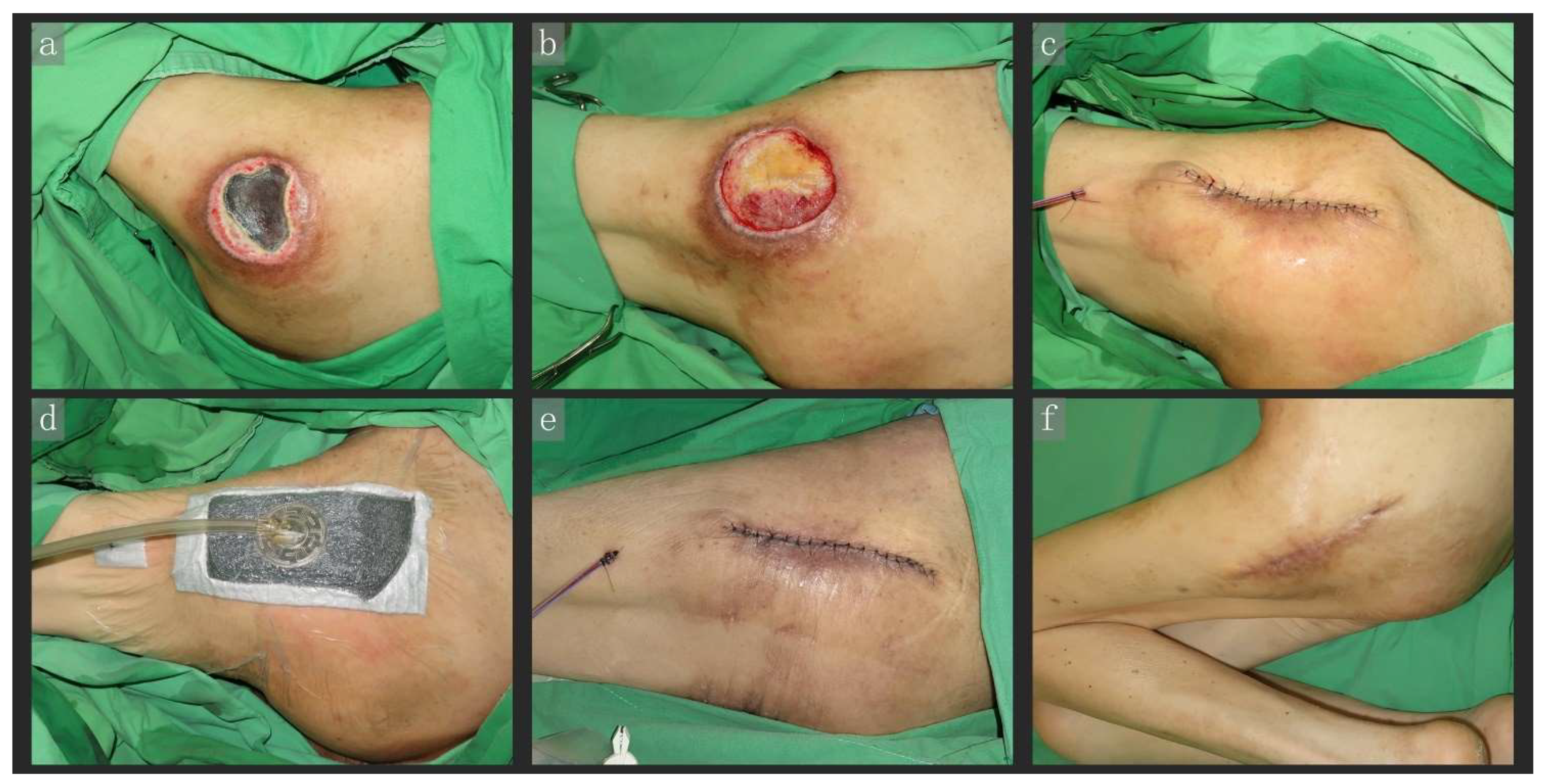
2.4. Representative Cases
2.4.1. Case 1
2.4.2. Case 2
2.4.3. Case 3
2.4.4. Case 4
3. Results
3.1. Patient Characteristics
3.2. Comparison of Overall Outcomes
3.3. Comparison of Outcomes between the Traditional and PC + CiNPWT Groups
3.4. Comparison of Outcomes between the PC and PC + CiNPWT Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, T.H. Bilateral gluteus maximus V-Y advancement musculocutaneous flaps for the coverage of large sacral pressure sores: Revisit and refinement. Ann. Plast. Surg. 1995, 35, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.T.; Chang, S.C.; Chen, S.G.; Tzeng, Y.S. Modification of the superior gluteal artery perforator flap for reconstruction of sacral sores. J. Plast. Reconstr. Aesthet. Surg. JPRAS 2014, 67, 526–532. [Google Scholar] [CrossRef]
- Marchi, M.; Battaglia, S.; Marchese, S.; Intagliata, E.; Spataro, C.; Vecchio, R. Surgical reconstructive procedures for treatment of ischial, sacral and trochanteric pressure ulcers. Il G. Di Chir. 2015, 36, 112–116. [Google Scholar] [CrossRef]
- Mervis, J.S.; Phillips, T.J. Pressure ulcers: Prevention and management. J. Am. Acad. Dermatol. 2019, 81, 893–902. [Google Scholar] [CrossRef]
- Argenta, L.C.; Morykwas, M.J. Vacuum-assisted closure: A new method for wound control and treatment: Clinical experience. Ann. Plast. Surg. 1997, 38, 563–576; discussion 577. [Google Scholar] [CrossRef] [PubMed]
- Dumville, J.C.; Webster, J.; Evans, D.; Land, L. Negative pressure wound therapy for treating pressure ulcers. Cochrane Database Syst. Rev. 2015, 5, Cd011334. [Google Scholar] [CrossRef]
- Dwivedi, M.K.; Srivastava, R.N.; Bhagat, A.K.; Agarwal, R.; Baghel, K.; Jain, A.; Raj, S. Pressure ulcer management in paraplegic patients with a novel negative pressure device: A randomised controlled trial. J. Wound Care 2016, 25, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Atkins, B.Z.; Tetterton, J.K.; Petersen, R.P.; Hurley, K.; Wolfe, W.G. Laser Doppler flowmetry assessment of peristernal perfusion after cardiac surgery: Beneficial effect of negative pressure therapy. Int. Wound J. 2011, 8, 56–62. [Google Scholar] [CrossRef] [PubMed]
- DeFazio, M.V.; Economides, J.M.; Anghel, E.L.; Mathis, R.K.; Barbour, J.R.; Attinger, C.E. Traction-assisted Internal Negative Pressure Wound Therapy With Bridging Retention Sutures to Facilitate Staged Closure of High-risk Wounds Under Tension. Wounds Compend. Clin. Res. Pract. 2017, 29, 289–296. [Google Scholar] [CrossRef]
- Googe, B.; Davidson, J.C.; Arnold, P.B.; Medina, A. Closed Incisional Negative Pressure Wound Therapy Sponge Width and Tension Off-Loading: A Laboratory Model. Ann. Plast. Surg. 2020, 85, 295–298. [Google Scholar] [CrossRef]
- Kafka-Ritsch, R.; Zitt, M.; Schorn, N.; Stroemmer, S.; Schneeberger, S.; Pratschke, J.; Perathoner, A. Open abdomen treatment with dynamic sutures and topical negative pressure resulting in a high primary fascia closure rate. World J. Surg. 2012, 36, 1765–1771. [Google Scholar] [CrossRef] [PubMed]
- Kilpadi, D.V.; Lessing, C.; Derrick, K. Healed porcine incisions previously treated with a surgical incision management system: Mechanical, histomorphometric, and gene expression properties. Aesthet. Plast. Surg. 2014, 38, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Jung, H.; Kwon, H.; Jung, S.N. Extended negative pressure wound therapy-assisted dermatotraction for the closure of large open fasciotomy wounds in necrotizing fasciitis patients. World J. Emerg. Surg. WJES 2014, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pliakos, I.; Papavramidis, T.S.; Mihalopoulos, N.; Koulouris, H.; Kesisoglou, I.; Sapalidis, K.; Deligiannidis, N.; Papavramidis, S. Vacuum-assisted closure in severe abdominal sepsis with or without retention sutured sequential fascial closure: A clinical trial. Surgery 2010, 148, 947–953. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.; Sumpio, B.J.; Tsay, C.; Swallow, M.; Dash, B.; Thorn, S.L.; Sinusas, A.J.; Koo, A.; Hsia, H.C.; Au, A. Incisional Negative Pressure Wound Therapy Augments Perfusion and Improves Wound Healing in a Swine Model Pilot Study. Ann. Plast. Surg. 2019, 82, S222–S227. [Google Scholar] [CrossRef]
- Timmers, M.S.; Le Cessie, S.; Banwell, P.; Jukema, G.N. The effects of varying degrees of pressure delivered by negative-pressure wound therapy on skin perfusion. Ann. Plast. Surg. 2005, 55, 665–671. [Google Scholar] [CrossRef]
- Wilkes, R.P.; Kilpad, D.V.; Zhao, Y.; Kazala, R.; McNulty, A. Closed incision management with negative pressure wound therapy (CIM): Biomechanics. Surg. Innov. 2012, 19, 67–75. [Google Scholar] [CrossRef]
- Agarwal, A. Management of Closed Incisions Using Negative-Pressure Wound Therapy in Orthopedic Surgery. Plast. Reconstr. Surg. 2019, 143, 21s–26s. [Google Scholar] [CrossRef]
- Atema, J.J.; Gans, S.L.; Boermeester, M.A. Systematic review and meta-analysis of the open abdomen and temporary abdominal closure techniques in non-trauma patients. World J. Surg. 2015, 39, 912–925. [Google Scholar] [CrossRef]
- Ferrando, P.M.; Ala, A.; Bussone, R.; Bergamasco, L.; Actis Perinetti, F.; Malan, F. Closed Incision Negative Pressure Therapy in Oncological Breast Surgery: Comparison with Standard Care Dressings. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1732. [Google Scholar] [CrossRef]
- Gabriel, A.; Maxwell, G.P. Economic Analysis Based on the Use of Closed-Incision Negative-Pressure Therapy after Postoperative Breast Reconstruction. Plast. Reconstr. Surg. 2019, 143, 36s–40s. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, A.; Sigalove, S.; Sigalove, N.; Storm-Dickerson, T.; Rice, J.; Maxwell, P.; Griffin, L. The Impact of Closed Incision Negative Pressure Therapy on Postoperative Breast Reconstruction Outcomes. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1880. [Google Scholar] [CrossRef] [PubMed]
- Galiano, R.D.; Hudson, D.; Shin, J.; van der Hulst, R.; Tanaydin, V.; Djohan, R.; Duteille, F.; Cockwill, J.; Megginson, S.; Huddleston, E. Incisional Negative Pressure Wound Therapy for Prevention of Wound Healing Complications Following Reduction Mammaplasty. Plast. Reconstr. Surg. Glob. Open 2018, 6, e1560. [Google Scholar] [CrossRef] [PubMed]
- Norman, G.; Goh, E.L.; Dumville, J.C.; Shi, C.; Liu, Z.; Chiverton, L.; Stankiewicz, M.; Reid, A. Negative pressure wound therapy for surgical wounds healing by primary closure. Cochrane Database Syst. Rev. 2020, 5, Cd009261. [Google Scholar] [CrossRef] [PubMed]
- Peter Suh, H.S.; Hong, J.P. Effects of Incisional Negative-Pressure Wound Therapy on Primary Closed Defects after Superficial Circumflex Iliac Artery Perforator Flap Harvest: Randomized Controlled Study. Plast. Reconstr. Surg. 2016, 138, 1333–1340. [Google Scholar] [CrossRef]
- Suissa, D.; Danino, A.; Nikolis, A. Negative-pressure therapy versus standard wound care: A meta-analysis of randomized trials. Plast. Reconstr. Surg. 2011, 128, 498e–503e. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.T.; Sumpio, B.J.; Miller, S.; Sumpio, B.E. Use of Closed-Incision Negative-Pressure Therapy: Cardiothoracic and Vascular Surgery. Plast. Reconstr. Surg. 2019, 143, 31s–35s. [Google Scholar] [CrossRef]
- LaVela, S.L.; Heinemann, A.W.; Etingen, B.; Miskovic, A.; Locatelli, S.M.; Chen, D. Relational empathy and holistic care in persons with spinal cord injuries. J. Spinal Cord Med. 2017, 40, 30–42. [Google Scholar] [CrossRef]
- Zhou, Q.; Yu, T.; Liu, Y.; Shi, R.; Tian, S.; Yang, C.; Gan, H.; Zhu, Y.; Liang, X.; Wang, L.; et al. The prevalence and specific characteristics of hospitalised pressure ulcer patients: A multicentre cross-sectional study. J. Clin. Nurs. 2018, 27, 694–704. [Google Scholar] [CrossRef]
- Lefèvre, C.; Bellier-Waast, F.; Lejeune, F.; Duteille, F.; Kieny, P.; Le Fort, M.; Perrouin-Verbe, B. Ten years of myocutaneous flaps for pressure ulcers in patients with spinal lesions: Analysis of complications in the framework of a specialised medical-surgical pathway. J. Plast. Reconstr. Aesthet. Surg. JPRAS 2018, 71, 1652–1663. [Google Scholar] [CrossRef]
- Yildirim, S.; Taylan, G.; Aköz, T. Freestyle perforator-based V-Y advancement flap for reconstruction of soft tissue defects at various anatomic regions. Ann. Plast. Surg. 2007, 58, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.K.; Wu, C.J.; Chen, C.Y.; Wang, C.Y.; Chu, T.S.; Hsu, K.F.; Chiu, H.T.; Liu, H.H.; Chou, C.Y.; Wang, C.H.; et al. Intraoperative indocyanine green fluorescent angiography-assisted modified superior gluteal artery perforator flap for reconstruction of sacral pressure sores. Int. Wound J. 2017, 14, 1170–1174. [Google Scholar] [CrossRef] [PubMed]
- Li, C.C.; Chang, S.C.; Fu, J.P.; Tzeng, Y.S.; Wang, C.H.; Chen, T.M.; Chen, S.G. Comparison of hatchet-shaped tensor fascia lata flap and pedicle anterior lateral thigh flap for treatment of trochanteric sores: A retrospective analysis of 48 patients. Ann. Plast. Surg. 2013, 71, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.T.; Chen, S.Y.; Chen, S.G.; Tzeng, Y.S.; Chang, S.C. Parasacral Perforator Flaps for Reconstruction of Sacral Pressure Sores. Ann. Plast. Surg. 2015, 75, 62–65. [Google Scholar] [CrossRef]
- Oksman, D.; de Almeida, O.M.; de Arruda, R.G.; de Almeida, M.L.M.; do Carmo, F.S. Comparative study between fasciocutaneous and myocutaneous flaps in the surgical treatment of pressure ulcers of the sacral region. JPRAS Open 2018, 16, 50–60. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Lu, W.; Zhang, Y.; Liu, Y.; Yang, X.; Liao, S.; Zhang, Z. Application of gluteus maximus fasciocutaneous V-Y advancement flap combined with resection in sacrococcygeal pressure ulcers: A CONSORT-compliant article. Medicine 2017, 96, e8829. [Google Scholar] [CrossRef]
- Chen, C.Y.; Chiang, I.H.; Ou, K.L.; Chiu, Y.L.; Liu, H.H.; Chang, C.K.; Wu, C.J.; Chu, T.S.; Hsu, K.F.; Huang, D.W.; et al. Surgical treatment and strategy in patients with pressure sores: A single-surgeon experience. Medicine 2020, 99, e23022. [Google Scholar] [CrossRef]
- Scalise, A.; Calamita, R.; Tartaglione, C.; Pierangeli, M.; Bolletta, E.; Gioacchini, M.; Gesuita, R.; Di Benedetto, G. Improving wound healing and preventing surgical site complications of closed surgical incisions: A possible role of Incisional Negative Pressure Wound Therapy. A systematic review of the literature. Int. Wound J. 2016, 13, 1260–1281. [Google Scholar] [CrossRef]
- Willy, C.; Agarwal, A.; Andersen, C.A.; Santis, G.; Gabriel, A.; Grauhan, O.; Guerra, O.M.; Lipsky, B.A.; Malas, M.B.; Mathiesen, L.L.; et al. Closed incision negative pressure therapy: International multidisciplinary consensus recommendations. Int. Wound J. 2017, 14, 385–398. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.; Ver Halen, J.P. Closed Incision Negative-Pressure Therapy Is Associated with Decreased Surgical-Site Infections: A Meta-Analysis. Plast. Reconstr. Surg. 2016, 138, 156e–157e. [Google Scholar] [CrossRef]
- Zaidi, A.; El-Masry, S. Closed-incision negative-pressure therapy in high-risk general surgery patients following laparotomy: A retrospective study. Colorectal Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2017, 19, 283–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehsani, R.; Djalali Motlagh, S.; Zaman, B.; Sehat Kashani, S.; Ghodraty, M.R. Effect of General Versus Spinal Anesthesia on Postoperative Delirium and Early Cognitive Dysfunction in Elderly Patients. Anesthesiol. Pain Med. 2020, 10, e101815. [Google Scholar] [CrossRef] [PubMed]
- Evered, L.A.; Silbert, B.S. Postoperative Cognitive Dysfunction and Noncardiac Surgery. Anesth. Analg. 2018, 127, 496–505. [Google Scholar] [CrossRef] [PubMed]
- Harris, M.; Chung, F. Complications of general anesthesia. Clin. Plast. Surg. 2013, 40, 503–513. [Google Scholar] [CrossRef]
- Jenkins, K.; Baker, A.B. Consent and anaesthetic risk. Anaesthesia 2003, 58, 962–984. [Google Scholar] [CrossRef]
- Papaioannou, A.; Fraidakis, O.; Michaloudis, D.; Balalis, C.; Askitopoulou, H. The impact of the type of anaesthesia on cognitive status and delirium during the first postoperative days in elderly patients. Eur. J. Anaesthesiol. 2005, 22, 492–499. [Google Scholar] [CrossRef]
- Strøm, C.; Rasmussen, L.S.; Sieber, F.E. Should general anaesthesia be avoided in the elderly? Anaesthesia 2014, 69 (Suppl. S1), 35–44. [Google Scholar] [CrossRef]
- Niskakangas, M.; Dahlbacka, S.; Liisanantti, J.; Vakkala, M.; Kaakinen, T. Spinal or general anaesthesia for lower-limb amputation in peripheral artery disease—A retrospective cohort study. Acta Anaesthesiol. Scand. 2018, 62, 226–233. [Google Scholar] [CrossRef]
- Pu, X.; Sun, J.M. General anesthesia vs spinal anesthesia for patients undergoing total-hip arthroplasty: A meta-analysis. Medicine 2019, 98, e14925. [Google Scholar] [CrossRef]
- Roberts, D.J.; Nagpal, S.K.; Kubelik, D.; Brandys, T.; Stelfox, H.T.; Lalu, M.M.; Forster, A.J.; McCartney, C.J.; McIsaac, D.I. Association between neuraxial anaesthesia or general anaesthesia for lower limb revascularisation surgery in adults and clinical outcomes: Population based comparative effectiveness study. BMJ 2020, 371, m4104. [Google Scholar] [CrossRef]
- Van Waesberghe, J.; Stevanovic, A.; Rossaint, R.; Coburn, M. General vs. neuraxial anaesthesia in hip fracture patients: A systematic review and meta-analysis. BMC Anesthesiol. 2017, 17, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinstein, S.M.; Poultsides, L.; Baaklini, L.R.; Mörwald, E.E.; Cozowicz, C.; Saleh, J.N.; Arrington, M.B.; Poeran, J.; Zubizarreta, N.; Memtsoudis, S.G. Postoperative delirium in total knee and hip arthroplasty patients: A study of perioperative modifiable risk factors. Br. J. Anaesth. 2018, 120, 999–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrianasolo, J.; Ferry, T.; Boucher, F.; Chateau, J.; Shipkov, H.; Daoud, F.; Braun, E.; Triffault-Fillit, C.; Perpoint, T.; Laurent, F.; et al. Pressure ulcer-related pelvic osteomyelitis: Evaluation of a two-stage surgical strategy (debridement, negative pressure therapy and flap coverage) with prolonged antimicrobial therapy. BMC Infect. Dis. 2018, 18, 166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, D.; Holtom, P.; Spellberg, B. Osteomyelitis Complicating Sacral Pressure Ulcers: Whether or Not to Treat With Antibiotic Therapy. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 68, 338–342. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Total Patients (n = 128) | |
|---|---|---|
| n | % | |
| Age (Mean ± SD) | 75.80 ± 14.71 | |
| Sex | ||
| Male | 60 | 46.88 |
| Female | 68 | 53.13 |
| Etiology of bedridden state | ||
| Dementia | 36 | 28.13 |
| Cerebrovascular accident | 30 | 23.44 |
| Parkinson’s disease | 14 | 10.94 |
| Spinal cord injury | 24 | 18.75 |
| Fracture of femur | 13 | 10.16 |
| Other | 11 | 8.59 |
| Variable | Total Wounds (nT = 162) | |
| nT | % | |
| Location of defect | ||
| Sacral | 114 | 70.37 |
| Trochanter | 31 | 19.14 |
| Ischial | 7 | 4.32 |
| Back | 5 | 3.09 |
| Other | 5 | 3.09 |
| Variable | Total Patients (n = 128) | |||||||
|---|---|---|---|---|---|---|---|---|
| VY (n = 56) | SGAP (n = 13) | pALT (n = 6) | TFL (n = 4) | PC (n = 17) | Other (n = 2) | PC + CiNPWT (n = 30) | p Value | |
| Sex a | 0.7220 | |||||||
| Male | 27 | 7 | 3 | 1 | 5 | 1 | 16 | |
| Female | 29 | 6 | 3 | 3 | 12 | 1 | 14 | |
| Age (Mean ± SD) b | 76.93 ± 12.35 | 74.15 ± 17.86 | 61.17 ± 20.19 | 75.75 ± 14.41 | 78.29 ± 12.37 | 54.50 ± 33.23 | 77.33 ± 15.08 | 0.0715 |
| Case follow-up time (month, Mean ± SD) | 20.40 ± 19.24 | 12.96 ± 14.03 | 13.38 ± 14.81 | 33.88 ± 24.98 | 22.32 ± 17.64 | 24.00 ± 2.83 | 11.4 3± 8.74 | 0.0546 |
| Comorbidity a | ||||||||
| HTN | 33 | 7 | 2 | 3 | 10 | 1 | 17 | 0.9218 |
| CHF | 5 | 0 | 0 | 0 | 3 | 0 | 1 | 0.5594 |
| VHD | 3 | 0 | 0 | 1 | 0 | 0 | 2 | 0.4590 |
| CAD | 9 | 0 | 0 | 0 | 2 | 0 | 3 | 0.7590 |
| Arrhythmia | 5 | 1 | 1 | 0 | 1 | 0 | 3 | 0.9478 |
| Dyslipidemia | 3 | 0 | 1 | 0 | 1 | 0 | 4 | 0.5472 |
| PAOD | 2 | 0 | 0 | 0 | 1 | 0 | 1 | 0.9220 |
| DM | 22 | 4 | 2 | 3 | 7 | 1 | 13 | 0.8478 |
| CKD | 9 | 1 | 0 | 0 | 1 | 0 | 3 | >0.999 |
| ESRD HD | 3 | 0 | 0 | 0 | 0 | 0 | 1 | >0.999 |
| Other | 8 | 1 | 1 | 0 | 2 | 0 | 4 | >0.999 |
| Nil | 10 | 6 | 3 | 1 | 4 | 1 | 8 | 0.2137 |
| Variable | Total Wounds (nT = 162) | |||||||
| VY (nT = 66) | SGAP (nT = 14) | pALT (nT = 8) | TFL (nT = 10) | PC (nT = 30) | Other (nT = 2) | PC + CiNPWT (nT = 32) | pValue | |
| Wound size (cm2, Mean ± SD) b | 64.24 ± 56.88 | 103.29 ± 36.31 | 92.38 ± 31.01 | 56.00 ± 40.52 | 35.03 ± 23.13 | 67.50 ± 60.10 | 63.47 ± 42.70 | <0.001 |
| Operation time (min, Mean ± SD) b | 78.85 ± 26.82 | 126.00 ± 32.26 | 174.88 ± 45.16 | 121.60 ± 61.13 | 38.33 ± 12.70 | 141.00 ± 124.45 | 38.16 ± 14.02 | <0.001 |
| Debridement time (Mean ± SD) b,c | 2.50 ± 1.83 | 3.79 ± 4.35 | 4.50 ± 2.39 | 2.60 ± 1.51 | 2.40 ± 1.25 | 3.50 ± 2.12 | 2.13 ± 0.98 | 0.0229 |
| Hospital days (Mean ± SD) b | 60.92 ± 73.39 | 63.15 ± 61.55 | 61.00 ± 25.60 | 45.80 ± 27.84 | 47.00 ± 26.10 | 58.00 ± 65.05 | 36.78 ± 26.92 | 0.4906 |
| Location of defect | ||||||||
| Sacral | 65 | 14 | 0 | 0 | 11 | 0 | 24 | |
| Trochanter | 1 | 0 | 6 | 10 | 8 | 0 | 6 | |
| Ischial | 0 | 0 | 2 | 0 | 4 | 0 | 1 | |
| Back | 0 | 0 | 0 | 0 | 3 | 1 | 1 | |
| Other | 0 | 0 | 0 | 0 | 4 | 1 | 0 | |
| Variable | Total Patients (n = 128) | ||||
|---|---|---|---|---|---|
| Traditional Reconstruction (n = 98) | PC + CiNPWT (n = 30) | p Value | |||
| n | % | n | % | ||
| Sex a | 0.4179 | ||||
| Male | 44 | 44.9 | 16 | 53.33 | |
| Female | 54 | 55.1 | 14 | 46.67 | |
| Age (Mean ± SD) b | 75.33 ± 14.65 | 77.33 ± 15.08 | 0.5155 | ||
| Variable | Total Wounds (nT = 162) | ||||
| Traditional Reconstruction (nT = 130) | PC + CiNPWT (nT = 32) | p Value | |||
| nT | % | nT | % | ||
| Wound size (cm2, Mean ± SD) b | 62.85 ± 49.94 | 63.47 ± 42.70 | 0.9490 | ||
| Operation time (min, Mean ± SD) b | 84.73 ± 48.55 | 38.16 ± 14.02 | <0.001 | ||
| Debridement time (Mean ± SD) b | 2.76 ± 2.20 | 2.13 ± 0.98 | 0.0153 | ||
| Hospital days (Mean ± SD) b | 56.70 ± 58.43 | 36.78 ± 26.92 | 0.0054 | ||
| Outcome a | |||||
| Healed | 98 | 75.38 | 26 | 81.25 | 0.4830 |
| Minor | 28 | 21.54 | 6 | 18.75 | 0.7286 |
| Major | 5 | 3.85 | 0 | 0 | 0.2598 |
| Mortality | 13 | 10.00 | 2 | 6.25 | 0.7374 |
| Location of defect a | 0.9641 | ||||
| Sacral | 90 | 69.23 | 24 | 75 | |
| Trochanter | 25 | 19.23 | 6 | 18.75 | |
| Ischial | 6 | 4.62 | 1 | 3.13 | |
| Back | 4 | 3.08 | 1 | 3.13 | |
| Other | 5 | 3.85 | 0 | 0 | |
| Variable | Total Wounds (nT = 62) | ||||
|---|---|---|---|---|---|
| PC (nT = 30) | PC + CiNPWT (nT = 32) | p Value | |||
| nT | % | nT | % | ||
| Wound size (cm2, Mean ± SD) a | 35.03 ± 23.13 | 63.47 ± 42.70 | 0.0019 | ||
| Operation time (min, Mean ± SD) a | 38.33 ± 12.70 | 38.16 ± 14.02 | 0.9587 | ||
| Debridement time (Mean ± SD) a | 2.40 ± 1.25 | 2.13 ± 0.98 | 0.3360 | ||
| Hospital days (Mean ± SD) a | 47.00 ± 26.10 | 36.78 ± 26.92 | 0.1349 | ||
| Outcome b | |||||
| Healed | 28 | 93.33 | 26 | 81.25 | 0.2577 |
| Minor | 4 | 13.33 | 6 | 18.75 | 0.7331 |
| Major | 1 | 3.33 | 0 | 0 | 0.4839 |
| Mortality | 1 | 3.33 | 2 | 6.25 | 0.5928 |
| Location of defect b | 0.0109 | ||||
| Sacral | 11 | 36.67 | 24 | 75 | |
| Trochanter | 8 | 26.67 | 6 | 18.75 | |
| Ischial | 4 | 13.33 | 1 | 3.13 | |
| Back | 3 | 10 | 1 | 3.13 | |
| Other | 4 | 13.33 | 0 | 0 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, K.-F.; Kao, L.-T.; Chu, P.-Y.; Chen, C.-Y.; Chou, Y.-Y.; Huang, D.-W.; Liu, T.-H.; Tsai, S.-L.; Wu, C.-W.; Hou, C.-C.; et al. Simple and Efficient Pressure Ulcer Reconstruction via Primary Closure Combined with Closed-Incision Negative Pressure Wound Therapy (CiNPWT)—Experience of a Single Surgeon. J. Pers. Med. 2022, 12, 182. https://doi.org/10.3390/jpm12020182
Hsu K-F, Kao L-T, Chu P-Y, Chen C-Y, Chou Y-Y, Huang D-W, Liu T-H, Tsai S-L, Wu C-W, Hou C-C, et al. Simple and Efficient Pressure Ulcer Reconstruction via Primary Closure Combined with Closed-Incision Negative Pressure Wound Therapy (CiNPWT)—Experience of a Single Surgeon. Journal of Personalized Medicine. 2022; 12(2):182. https://doi.org/10.3390/jpm12020182
Chicago/Turabian StyleHsu, Kuo-Feng, Li-Ting Kao, Pei-Yi Chu, Chun-Yu Chen, Yu-Yu Chou, Dun-Wei Huang, Ting-Hsuan Liu, Sheng-Lin Tsai, Chien-Wei Wu, Chih-Chun Hou, and et al. 2022. "Simple and Efficient Pressure Ulcer Reconstruction via Primary Closure Combined with Closed-Incision Negative Pressure Wound Therapy (CiNPWT)—Experience of a Single Surgeon" Journal of Personalized Medicine 12, no. 2: 182. https://doi.org/10.3390/jpm12020182