
Efficacy of Myopia Control and Distribution of Corneal Epithelial Thickness in Children Treated with Orthokeratology Assessed Using Optical Coherence Tomography

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
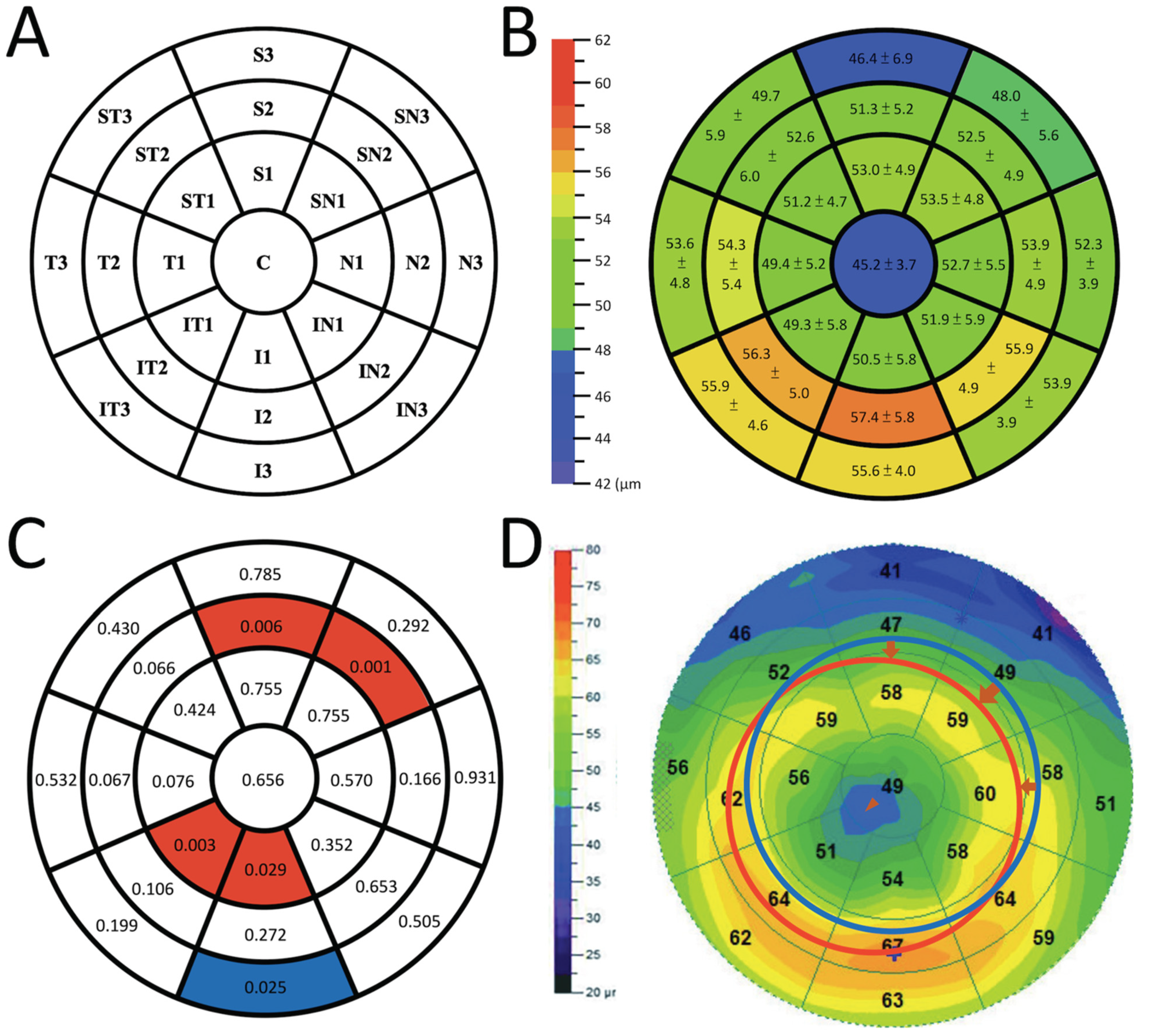
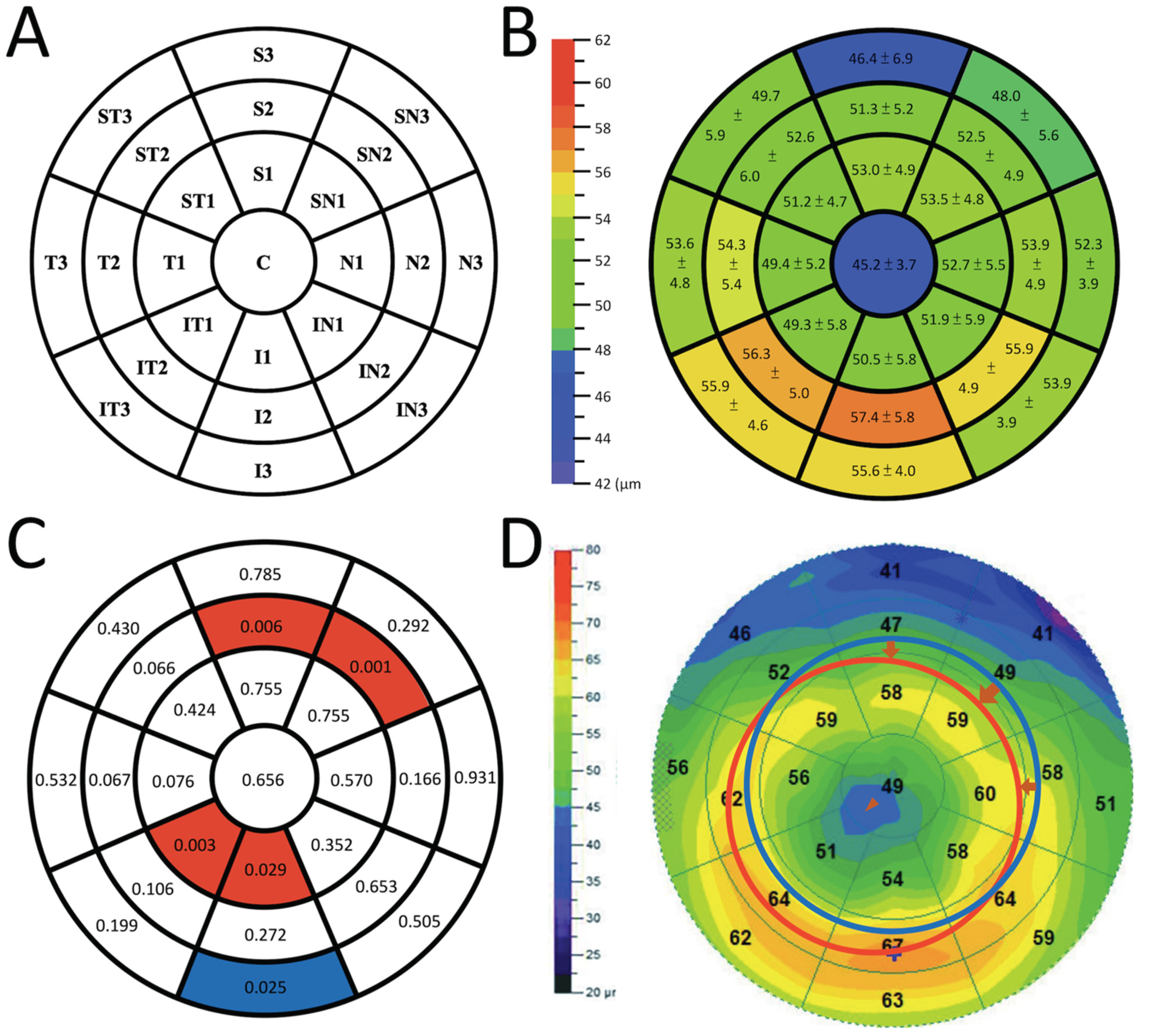
2.1. Corneal Epithelial Thickness Map
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vincent, S.J.; Cho, P.; Chan, K.Y.; Fadel, D.; Ghorbani-Mojarrad, N.; Gonzalez-Meijome, J.M.; Johnson, L.; Kang, P.; Michaud, L.; Simard, P.; et al. CLEAR-Orthokeratology. Contact Lens Anterior Eye 2021, 44, 240–269. [Google Scholar] [CrossRef] [PubMed]
- Gifford, K.L.; Richdale, K.; Kang, P.; Aller, T.A.; Lam, C.S.; Liu, Y.M.; Michaud, L.; Mulder, J.; Orr, J.B.; Rose, K.A.; et al. IMI—Clinical Management Guidelines Report. Investig. Ophthalmol. Vis. Sci. 2019, 60, M184–M203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, Y.M.; Xie, P. The Safety of Orthokeratology—A Systematic Review. Eye Contact Lens 2016, 42, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Friedman, I.B.; Medow, N.B.; Zhang, C. Update on Orthokeratology in Managing Progressive Myopia in Children: Efficacy, Mechanisms, and Concerns. J. Pediatr. Ophthalmol. Strabismus 2017, 54, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Kim, W.K.; Kim, B.J.; Ryu, I.H.; Kim, J.K.; Kim, S.W. Corneal epithelial and stromal thickness changes in myopic orthokeratology and their relationship with refractive change. PLoS ONE 2018, 13, e0203652. [Google Scholar] [CrossRef]
- Tsukiyama, J.; Miyamoto, Y.; Higaki, S.; Fukuda, M.; Shimomura, Y. Changes in the anterior and posterior radii of the corneal curvature and anterior chamber depth by orthokeratology. Eye Contact Lens 2008, 34, 17–20. [Google Scholar] [CrossRef]
- Chen, D.; Lam, A.K.; Cho, P. Posterior corneal curvature change and recovery after 6 months of overnight orthokeratology treatment. Ophthalmic Physiol. Opt. 2010, 30, 274–280. [Google Scholar] [CrossRef]
- Li, F.; Jiang, Z.X.; Hao, P.; Li, X. A Meta-Analysis of Central Corneal Thickness Changes With Overnight Orthokeratology. Eye Contact Lens 2016, 42, 141–146. [Google Scholar] [CrossRef]
- Smith, E.L., 3rd; Kee, C.S.; Ramamirtham, R.; Qiao-Grider, Y.; Hung, L.F. Peripheral vision can influence eye growth and refractive development in infant monkeys. Investig. Ophthalmol. Vis. Sci. 2005, 46, 3965–3972. [Google Scholar] [CrossRef]
- Smith, E.L., 3rd; Ramamirtham, R.; Qiao-Grider, Y.; Hung, L.F.; Huang, J.; Kee, C.S.; Coats, D.; Paysse, E. Effects of foveal ablation on emmetropization and form-deprivation myopia. Investig. Ophthalmol. Vis. Sci. 2007, 48, 3914–3922. [Google Scholar] [CrossRef]
- Liu, Y.; Wildsoet, C. The effect of two-zone concentric bifocal spectacle lenses on refractive error development and eye growth in young chicks. Investig. Ophthalmol. Vis. Sci. 2011, 52, 1078–1086. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Si, J.K.; Tang, K.; Bi, H.S.; Guo, D.D.; Guo, J.G.; Wang, X.R. Orthokeratology for myopia control: A meta-analysis. Optom. Vis. Sci. 2015, 92, 252–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, P.W.; Yeung, L.; Sun, C.C.; Chen, H.M.; Peng, S.Y.; Chen, Y.T.; Liu, C.F. Correlation of corneal pigmented arc with wide epithelial thickness map in orthokeratology-treated children using optical coherence tomography measurements. Contact Lens Anterior Eye 2020, 43, 238–243. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.F.; Lee, J.S.; Sun, C.C.; Lin, K.K.; Hou, C.H.; Yeung, L.; Peng, S.Y. Correlation between pigmented arc and epithelial thickness (COPE) study in orthokeratology-treated patients using OCT measurements. Eye 2020, 34, 352–359. [Google Scholar] [CrossRef]
- Charman, W.N.; Mountford, J.; Atchison, D.A.; Markwell, E.L. Peripheral refraction in orthokeratology patients. Optom. Vis. Sci. 2006, 83, 641–648. [Google Scholar] [CrossRef]
- Cheung, S.W.; Boost, M.V.; Cho, P. Pre-treatment observation of axial elongation for evidence-based selection of children in Hong Kong for myopia control. Contact Lens Anterior Eye 2019, 42, 392–398. [Google Scholar] [CrossRef]
- Chen, Z.; Xue, F.; Zhou, J.; Qu, X.; Zhou, X.; Shanghai, O.; Study, G. Prediction of Orthokeratology Lens Decentration with Corneal Elevation. Optom. Vis. Sci. Off. Publ. Am. Acad. Optom. 2017, 94, 903–907. [Google Scholar] [CrossRef]
- Wang, A.; Yang, C. Influence of Overnight Orthokeratology Lens Treatment Zone Decentration on Myopia Progression. J. Ophthalmol. 2019, 2019, 2596953. [Google Scholar] [CrossRef]
- Wu, G.Y.; Lai, X.Q.; Dai, X.D. Effect of decentration in controlling the development of myopia after orthokeratology. Int. Eye Sci. 2018, 18, 188–191. [Google Scholar] [CrossRef]
- Liu, C.F.; Tseng, C.H.; Huang, C.Y.; Sun, C.C.; Yang, M.L.; Chen, W.Y.; Yeung, L. Correlation between higher-order aberrations and visual acuity recovery (CoHORT) after spectacles treatment for pediatric refractive amblyopia: A pilot study using iDesign measurement. PLoS ONE 2020, 15, e0228922. [Google Scholar] [CrossRef]
- Hiraoka, T.; Mihashi, T.; Okamoto, C.; Okamoto, F.; Hirohara, Y.; Oshika, T. Influence of induced decentered orthokeratology lens on ocular higher-order wavefront aberrations and contrast sensitivity function. J. Cataract. Refract. Surg. 2009, 35, 1918–1926. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.; Wang, L.; Gao, J.; Yang, M.; Zhao, Q. Influence of Overnight Orthokeratology on Corneal Surface Shape and Optical Quality. J. Ophthalmol. 2017, 2017, 3279821. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, T.; Kakita, T.; Okamoto, F.; Oshika, T. Influence of ocular wavefront aberrations on axial length elongation in myopic children treated with overnight orthokeratology. Ophthalmology 2015, 122, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Lau, J.K.; Vincent, S.J.; Collins, M.J.; Cheung, S.W.; Cho, P. Ocular higher-order aberrations and axial eye growth in young Hong Kong children. Sci. Rep. 2018, 8, 6726. [Google Scholar] [CrossRef] [PubMed]
- Charm, J.; Cho, P. High myopia-partial reduction ortho-k: A 2-year randomized study. Optom. Vis. Sci. 2013, 90, 530–539. [Google Scholar] [CrossRef] [Green Version]
- VanderVeen, D.K.; Kraker, R.T.; Pineles, S.L.; Hutchinson, A.K.; Wilson, L.B.; Galvin, J.A.; Lambert, S.R. Use of Orthokeratology for the Prevention of Myopic Progression in Children: A Report by the American Academy of Ophthalmology. Ophthalmology 2019, 126, 623–636. [Google Scholar] [CrossRef] [Green Version]
- Qian, Y.; Xue, F.; Huang, J.; Qu, X.; Zhou, X.; Lanen-Wanek, D.V. Pachymetry map of corneal epithelium in children wearing orthokeratology contact lenses. Curr. Eye Res. 2014, 39, 263–270. [Google Scholar] [CrossRef]
- Chen, R.; Chen, Y.; Lipson, M.; Kang, P.; Lian, H.; Zhao, Y.; McAlinden, C.; Huang, J. The Effect of Treatment Zone Decentration on Myopic Progression during Or-thokeratology. Curr. Eye Res. 2020, 45, 645–651. [Google Scholar] [CrossRef]
- Kao, P.-H.; Chuang, L.-H.; Lai, C.-C.; Chen, S.-Y.; Lin, K.-K.; Lee, J.-S.; Hou, C.-H.; Chen, C.-T.; Kuo, Y.-K.; Sun, C.-C.; et al. Evaluation of axial length to identify the effects of monocular 0.125% atropine treatment for pediatric anisometropia. Sci. Rep. 2021, 11, 21511. [Google Scholar] [CrossRef]
- Lu, W.; Jin, W. Clinical observations of the effect of orthokeratology in children with myopic anisometropia. Contact Lens Anterior Eye 2020, 43, 222–225. [Google Scholar] [CrossRef]
- Liu, C.F.; Chen, S.C.; Chen, K.J.; Liu, L.; Chen, Y.P.; Kang, E.Y.; Liu, P.K.; Yeung, L.; Wu, W.C.; Lai, C.C.; et al. Higher HbA1c may reduce axial length elongation in myopic children: A comparison cohort study. Acta Diabetol. 2021, 58, 779–786. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| N = 83 | β | p-Value a | |
|---|---|---|---|
| Age (years) | 11.2 ± 1.9 | −14.43 | 0.008 * |
| Gender (male:female) | 22:21 | −13.87 | 0.623 |
| Target power (diopter) | 3.28 ± 1.29 | −0.26 | 0.008 * |
| Diameter (mm) | 10.56 ± 0.13 | <0.001 | 0.777 |
| Alignment-curve power (diopter) b | 42.59 ± 1.21 | 0.04 | 0.691 |
| Prescription astigmatism (eye) | Yes 27; No 56 | −8.36 | 0.686 |
| Mean AS-OCT exam time point (months) c | 21.20 ± 11.80 | −1.36 | 0.186 |
| Follow-up duration (months) | 28.27 ± 12.09 | −1.30 | 0.215 |
| Axial length at baseline (mm) | 25.08 ± 0.93 | −23.81 | 0.137 |
| Axial length at 6 months after lens wear (mm) | 25.20 ± 0.91 | −19.98 | 0.219 |
| Axial length at final visit (mm) | 25.46 ± 0.92 | 3.64 | 0.809 |
| Annual axial length changes (μm/year) | 168.86 ± 157.54 | ||
| Variable | Mean Thickness (μm) | β | 95% CI for β | p-Value | |
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Central Zone (2 mm) | 45.2 ± 3.7 | −1.162 | −6.274 | 3.949 | 0.656 |
| Ring 1 (2–5 mm) | |||||
| N1 | 52.7 ± 5.5 | 1.349 | −3.302 | 6.000 | 0.570 |
| SN1 | 53.5 ± 4.8 | 0.815 | −4.311 | 5.941 | 0.755 |
| S1 | 53.0 ± 4.9 | 0.751 | −3.973 | 5.475 | 0.755 |
| ST1 | 51.2 ± 4.7 | 1.616 | −2.350 | 5.582 | 0.424 |
| T1 | 49.4 ± 5.2 | 3.387 | −0.355 | 7.128 | 0.076 |
| IT1 | 49.3 ± 5.8 | 4.638 | 1.583 | 7.693 | 0.003 * |
| I1 | 50.5 ± 5.8 | 4.445 | 0.459 | 8.432 | 0.029 * |
| IN1 | 51.9 ± 5.9 | 2.234 | −2.473 | 6.941 | 0.352 |
| Ring 2 (5–7 mm) | |||||
| N2 | 53.9 ± 4.9 | 3.438 | −1.426 | 8.301 | 0.166 |
| SN2 | 52.5 ± 4.9 | 5.723 | 2.312 | 9.134 | 0.001 * |
| S2 | 51.3 ± 5.2 | 5.325 | 1.531 | 9.119 | 0.006 * |
| ST2 | 52.6 ± 6.0 | 3.774 | −0.252 | 7.799 | 0.066 |
| T2 | 54.3 ± 5.4 | 3.746 | −0.265 | 7.757 | 0.067 |
| IT2 | 56.3 ± 5.0 | 3.778 | −0.799 | 8.355 | 0.106 |
| I2 | 57.4 ± 5.8 | 2.092 | −1.639 | 5.822 | 0.272 |
| IN2 | 55.9 ± 4.9 | 0.981 | −3.294 | 5.257 | 0.653 |
| Ring 3 (7–9 mm) | |||||
| N3 | 52.3 ± 3.9 | −0.269 | −6.347 | 5.810 | 0.931 |
| SN3 | 48.0 ± 5.6 | 1.970 | −1.693 | 5.634 | 0.292 |
| S3 | 46.4 ± 6.9 | 0.537 | −3.317 | 4.391 | 0.785 |
| ST3 | 49.7 ± 5.9 | 1.768 | −2.625 | 6.161 | 0.430 |
| T3 | 53.6 ± 4.8 | 1.931 | −4.130 | 7.992 | 0.532 |
| IT3 | 55.9 ± 4.6 | −3.128 | −7.907 | 1.650 | 0.199 |
| I3 | 55.6 ± 4.0 | −5.372 | −10.069 | −0.674 | 0.025 * |
| IN3 | 53.9 ± 3.9 | −1.817 | −7.155 | 3.521 | 0.505 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuo, Y.-K.; Chen, Y.-T.; Chen, H.-M.; Wu, P.-C.; Sun, C.-C.; Yeung, L.; Lin, K.-K.; Chen, H.-C.; Chuang, L.-H.; Lai, C.-C.; et al. Efficacy of Myopia Control and Distribution of Corneal Epithelial Thickness in Children Treated with Orthokeratology Assessed Using Optical Coherence Tomography. J. Pers. Med. 2022, 12, 278. https://doi.org/10.3390/jpm12020278
Kuo Y-K, Chen Y-T, Chen H-M, Wu P-C, Sun C-C, Yeung L, Lin K-K, Chen H-C, Chuang L-H, Lai C-C, et al. Efficacy of Myopia Control and Distribution of Corneal Epithelial Thickness in Children Treated with Orthokeratology Assessed Using Optical Coherence Tomography. Journal of Personalized Medicine. 2022; 12(2):278. https://doi.org/10.3390/jpm12020278
Chicago/Turabian StyleKuo, Yu-Kai, Yen-Ting Chen, Ho-Min Chen, Pei-Chang Wu, Chi-Chin Sun, Ling Yeung, Ken-Kuo Lin, Hung-Chi Chen, Lan-Hsin Chuang, Chi-Chun Lai, and et al. 2022. "Efficacy of Myopia Control and Distribution of Corneal Epithelial Thickness in Children Treated with Orthokeratology Assessed Using Optical Coherence Tomography" Journal of Personalized Medicine 12, no. 2: 278. https://doi.org/10.3390/jpm12020278
APA StyleKuo, Y.-K., Chen, Y.-T., Chen, H.-M., Wu, P.-C., Sun, C.-C., Yeung, L., Lin, K.-K., Chen, H.-C., Chuang, L.-H., Lai, C.-C., Chen, Y.-H., & Liu, C.-F. (2022). Efficacy of Myopia Control and Distribution of Corneal Epithelial Thickness in Children Treated with Orthokeratology Assessed Using Optical Coherence Tomography. Journal of Personalized Medicine, 12(2), 278. https://doi.org/10.3390/jpm12020278