
Comparison of the Results of Therapy for cT1 Renal Carcinoma with Nephron-Sparing Surgery (NSS) vs. Percutaneous Thermal Ablation (TA)

Abstract
:1. Objectives
2. Introduction
3. Material
4. Methods
5. Results Overview and Discussion
6. Conclusions
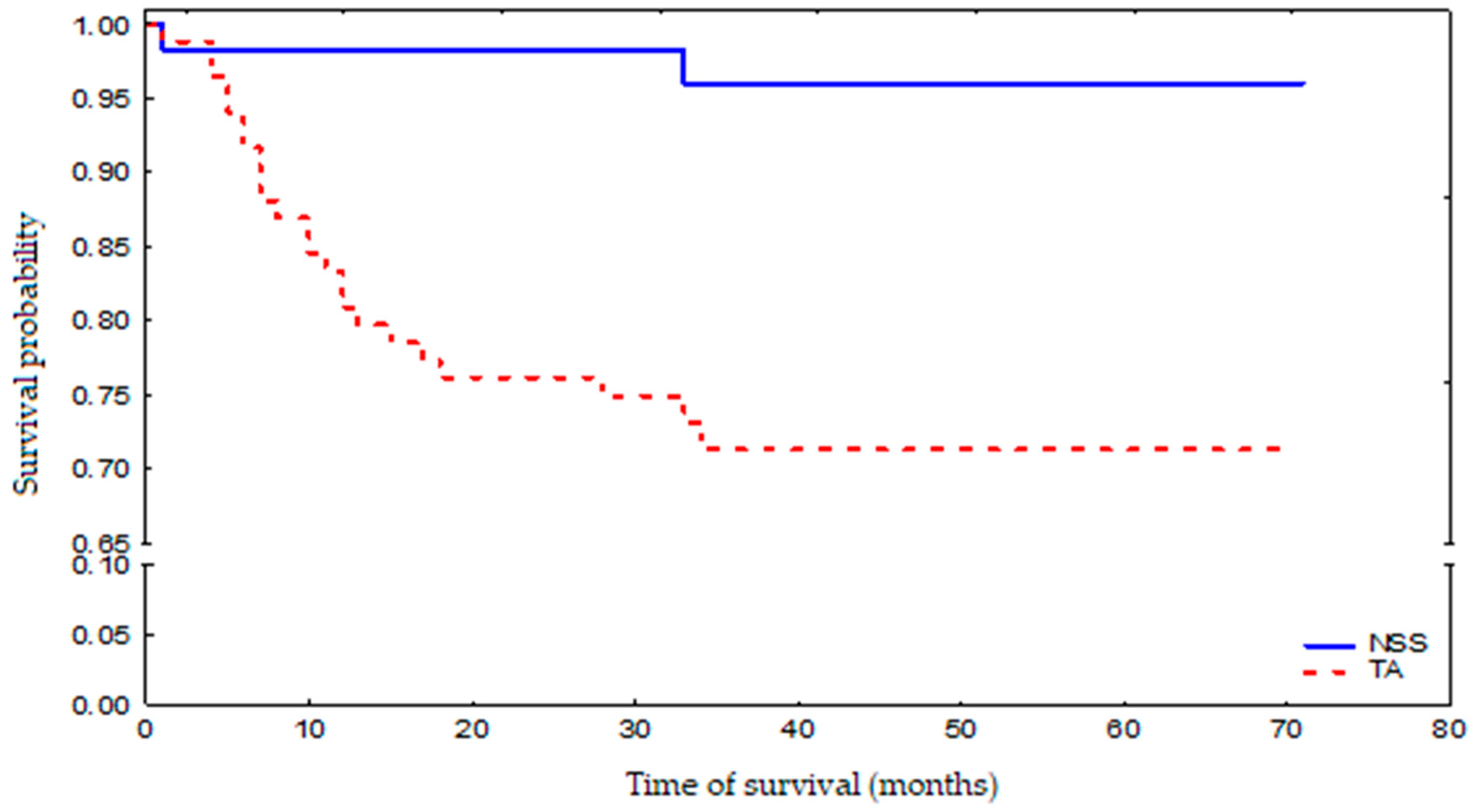
- NSS was associated with a slightly higher side effect rate but resulted in prolonged survival;
- TA was applied to elderly patients with comorbidities. Despite less invasive treatment, this group had poorer survival;
- The aim of presenting two widely different methods for small kidney tumour treatment was to demonstrate their application for various age groups and clinical conditions.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. J. Clin. 2018, 68, 394–4241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Znaor, A.; Lortet-Tieulent, J.; Laversanne, M.; Jemal, A.; Bray, F. International variations and trends in renal cell carcinoma incidence and mortality. Eur. Urol. 2015, 67, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Capitanio, U.; Bensalah, K.; Bex, A.; Boorjian, S.A.; Bray, F.; Coleman, J.; Russo, P. Epidemiology of Renal Cell Carcinoma. Eur. Urol. 2019, 75, 74–84. [Google Scholar] [CrossRef] [PubMed]
- Ziegelmüller, B.K.; Spek, A.; Szabados, B.; Casuscelli, J.; Clevert, D.A.; Staehler, M. Epidemiology and diagnostic assessment of small renal masses. Der. Urologe. Ausg. A 2018, 57, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Zequi, S.; da Costa, W.H.; Korkes, F.; Dos Reis, R.B.; Busato, W.F.S.; Matheus, W.E.; Soares, A. Renal cell cancer treatment: Anex pert panel recommendation from the Latin American cooperative group-genitourinary and the Latin American renal cancer group: Focus on burger. Ther. Adv. Urol. 2019, 11, 1756287219872324. [Google Scholar]
- Protzel, C.; Maruschke, M.; Hakenberg, O.W. Epidemiology, aetiology and pathogenesis of renal cell carcicoma. EAU-Eur. Urol. Suppl. 2012, 11, 52–59. [Google Scholar] [CrossRef]
- European Association of Urology Guidelines 2019 Edition. Renal Cell Carcinoma 7.1.4.3. Ablative Therapies. Available online: https://uroweb.org/guidelines/renal-cell-carcinoma (accessed on 6 December 2021).
- Yan, S.; Yang, W.; Zhu, C.-M.; Yan, P.-M.; Wang, Z.-C. Comparison among cryoablation, radiofrequency ablation, and partial nephrectomy for renal cell carcinomas sized smaller than 2 cm or sized 2–4 cm: A population-based study. Medicine 2019, 98, e15610. [Google Scholar] [CrossRef]
- Uhlig, J.; Kokabi, N.; Xing, M.; Kim, H.S. Ablation versus Resection for Stage 1A Renal Cell Carcinoma: National Variation in Clinical Management and Selected Outcomes. Radiology 2018, 288, 889–897. [Google Scholar] [CrossRef] [Green Version]
- Pantelidou, M.; Challacombe, B.; McGrath, A.; Brown, M.; Ilyas, S.; Katsanos, K.; Adam, A. Percutaneous Radiofrequency Ablation Versus Robotic-Assisted Partial Nephrectomy for the Treatment of Small Renal Cell Carcinoma. Cardiovasc. Interv. Radiol. 2016, 39, 1595–1603. [Google Scholar] [CrossRef] [Green Version]
- Van Poppel, H.; Da Pozzo, L.; Albrecht, W.; Matveev, V.; Bono, A.; Borkowski, A. Eastern Cooperative Oncology Group. A Prospective, randomized EORTC intergroup phase 3 study comparing the oncologic outcome of elective nephron-sparing surgery and radical nephrectomy for low-stage renal cell carcinoma. Eur. Urol. 2011, 59, 543. [Google Scholar] [CrossRef]
- Kates, M.; Badalato, G.M.; Pitman, M.; McKiernan, J.M. Increased risk of overall and cardiovascular mortality after radical nephrectomy for renal cell carcinoma 2 cm or less. J. Urol. 2011, 186, 1247. [Google Scholar] [CrossRef] [PubMed]
- Thompson, R.H.; Atwell, T.; Schmit, G.; Lohse, C.M.; Kurup, A.N.; Weisbrod, A.; Leibovich, B.C. Comparison of partial nephrectomy and percutaneous ablation for cT1 renal masses. Eur. Urol. 2015, 67, 252. [Google Scholar] [CrossRef]
- Gunn, A.J.; Gervais, D.A. Percutaneous Ablation of the Small Renal Mass—Techniques and Outcomes. Semin. Interv. Radiol. 2014, 31, 033–041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramanathan, R.; Leveillee, R.J. Ablative therapies for renal tumors. Ther. Adv. Urol. 2010, 2, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Wegner, R.E.; Abel, S.; Vemana, G.; Mao, S.; Fuhrer, R. Utilization of stereotactic ablative body radiation therapy for intact renal cell carcinoma: Trends in treatment and predictors of outcome. Adv. Radiat. Oncol. 2019, 5, 85–91. [Google Scholar] [CrossRef] [Green Version]
- Charlson, M.E. Charlson Comorbidity Index. Available online: https://www.mdcalc.com/charlson-comorbidity-index-cci (accessed on 6 December 2021).
- Garrido, D.; Dutra, S.; Amante, S.; Chaves, M.; Brum, M. The RENAL Nephrometry Score–What, Why and How. Eur. Congr. Radiol. 2018. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Salagierski, M.; Salagierski, M.; Różański, W. Termoablacja alternatywne rozwiązania i dylematy związane z postępowaniem w przypadkach nowotworów nerek. Urol. Pol. 2008, 61, 4. [Google Scholar]
- Salagierski, M.; Salagierski, M.; Różański, W. Ablacja termiczna guzów nerek monito. rowana w czasie trwania zabiegu. Przegląd Urol. 2010, 2, 60. [Google Scholar]
- Abu-Ghanem, Y.; Fernández-Pello, S.; Bex, A.; Ljungberg, B.; Albiges, L.; Dabestani, S.; Giles, R.H.; Hofmann, F.; Hora, M.; Kuczyk, M.A.; et al. Limitations of Available Studies Prevent Reliable Comparison Between Tumour Ablation and Partial Nephrectomy for Patients with Localised Renal Masses: A Systematic Review from the European Association of Urology Renal Cell Cancer Guideline Panel. Eur. Urol. Oncol. 2020, 3, 433–452. [Google Scholar] [CrossRef]
- Yin, X.; Cui, L.; Li, F.; Qi, S.; Yin, Z.; Gao, J. Radiofrequency Ablation Versus Partial Nephrectomy in Treating Small Renal Tumors: A systematic revive and meta-analysi. Medicine 2015, 94, e2255. [Google Scholar] [CrossRef]
- Stern, J.M.; Svatek, R.; Park, S.; Hermann, M.; Lotan, Y.; Sagalowsky, A.I.; Cadeddu, J.A. Intermediate comparison of partial nephrectomy and radiofrequency ablation for clinical T1a renal tumours. Br. J. Urol. 2007, 100, 287–290. [Google Scholar] [CrossRef] [PubMed]
- Banegas, M.; Harlan, L.; Mann, B.; Yabroff, K.R. Toward greater adoption of minimally-invasive and nephron-sparing surgical techniques for renal cell cancer in the U.S. Urol. Oncol. 2016, 34, 433.e9–433.e17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pan, X.-W.; Cui, X.-M.; Huang, H.; Huang, Y.; Li, L.; Wang, Z.-J.; Qu, F.-J.; Gao, Y.; Cui, X.-G.; Xu, D.-F. Radiofrequency ablation versus partial nephrectomy for treatment of renal masses: A systematic review and meta-analysis. Kaohsiung J. Med. Sci. 2015, 31, 649–658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Osawa, T.; Hafez, K.S.; Miller, D.C.; Montgomery, J.S.; Morgan, T.M.; Palapattu, G.S.; Weizer, A.Z.; Caoili, E.M.; Ellis, J.H.; Kunju, L.P.; et al. Age, Gender and R.E.N.A.L. Nephrometry Score do not Improve the Accuracy of a Risk Stratification Algorithm Based on Biopsy and Mass Size for Assigning Surveillance versus Treatment of Renal Tumors. J. Urol. 2015, 195, 574–580. [Google Scholar] [CrossRef] [PubMed]
- Kutikov, A.; Uzzo, R.G. The R.E.N.A.L. Nephrometry Score: A Comprehensive Standardized System for Quantitating Renal Tumor Size, Location and Depth. J. Urol. 2009, 182, 844–853. [Google Scholar] [CrossRef]
- Basu, S.; Khan, I.A.; Das, R.K.; Khan, D.; Agarwal, V. RENAL nephrometry score: Predicting perioperative outcomes following open partial nephrectomy. Urol. Ann. 2019, 11, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.K.; Huang, W.C.; Skolnik, E.Y.; Gervais, D.A.; Braithwaite, R.S.; Pandharipande, P.V. Tumor anatomy scoring and renal function for nephron-sparing treatment selection in patients with small renal masses: A micro simulation-based decision analysis. AJR Am. J. Roentgenol. 2016, 207, 344–353. [Google Scholar] [CrossRef]
- Konstantinidis, C.; Trilla, E.; Serres-Créixams, X.; Montealegre, C.; Lorente, D.; Castellón, R.; Morote, J. Association among the R.E.N.A.L. nephrometry score and clinical outcomes in patients with small renal masses treated with percutaneous contrast enhanced ultrasound radiofrequency ablation. Cent. Eur. J. Urol. 2019, 72, 92–99. [Google Scholar] [CrossRef]
- Veccia, A.; Antonelli, A.; Uzzo, R.G.; Novara, G.; Kutikov, A.; Ficarra, V.; Simeone, C.; Mirone, V.; Hampton, L.J.; Derweesh, I.; et al. Predictive Value of Nephrometry Scores in Nephron-sparing Surgery: A Systematic Review and Meta-analysis. Eur. Urol. Focus 2019, 6, 490–504. [Google Scholar] [CrossRef]
- Ficarra, V.; Crestani, A.; Inferrera, A.; Novara, G.; Rossanese, M.; Subba, E.; Giannarini, G. Positive Surgical Margins After Partial Nephrectomy: A Systematic Review and Meta-Analysis of Comparative Studies. Kidney Cancer 2018, 2, 133–145. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
{kind=link}
| Variable | Investigated Group (n = 140) | NSS (n = 56) | TA (n = 84) | p Value |
|---|---|---|---|---|
| sex | ||||
| Men | 86 (61.43%) | 37 (66.07%) | 49 (58.33%) | 0.3568 |
| Women | 54 (38.57%) | 19 (33.93%) | 35 (41.67%) | |
| Kidney | ||||
| Left | 76 (54.29%) | 28 (50%) | 48 (57.14%) | 0.4056 |
| Right | 64 (45.71%) | 28 (50%) | 36 (42.86%) | |
| R.E.N.A.L. | ||||
| 4 | 88 (62.86%) | 42 (75%) | 46 (54.76%) | 0.0387 |
| 5 | 28 (20%) | 6 (10.71%) | 22 (26.19%) | |
| 6 | 12 (8.57%) | 3 (5.36%) | 9 (10.71%) | |
| 7 | 6 (4.29%) | 2 (3.57%) | 4 (4.76%) | |
| 8 | 5 (3.57%) | 2 (3.57%) | 3 (3.57%) | |
| 9 | 1 (0.71%) | 1 (1.79%) | 0 (0%) | |
| CLAVIEN-DIDNO | ||||
| 1 | 133 (95%) | 51 (91.07%) | 82 (97.62%) | 0.0906 |
| 2 | 3 (2.14%) | 3 (5.36%) | 0 (0.00%) | |
| 3 | 2 (1.43%) | 1 (1.79%) | 1 (1.19%) | |
| 5 | 2 (1.43%) | 1 (1.79%) | 1 (1.19%) | |
| cT1 feature | ||||
| cT1a | 126 (90%) | 51 (91.07%) | 75 (89.29%) | 0.9541 |
| cT1b | 14 (10%) | 5 (8.93%) | 9 (10.71%) | |
| Type of cancer | ||||
| clear cell | 123 (87.86%) | 44 (78.57%) | 79 (94.05%) | |
| papillary type 1 | 6 (4.29%) | 4 (7.14%) | 2 (2.38%) | |
| papillary type 2 | 8 (5.71%) | 6 (10.71%) | 2 (2.38%) | 0.0534 |
| chromophobe | 3 (2.14%) | 2 (3.58%) | 1 (1.19%) | |
| Grading | ||||
| G1–G2 | 123 (87.86%) | 50 (89.28%) | 73 (86.90%) | 0.6726 |
| G3 | 17 (12.14%) | 6 (10.71%) | 11 (13.10%) | |
| Deaths | ||||
| All in follow-up period | 25 (17.8%) | 2 (3.5%) | 23 (27.3%) | 0.0005 |
| Perioperative | 2 (1.43%) | 1 (1.75%) | 1 (1.19%) | 1.0000 |
| Total (n = 140) | NSS (n = 56) | TA (n = 84) | p Value | |
|---|---|---|---|---|
| Variable | Mediana (25–75%) | Mediana (25–75%) | Mediana (25–75%) | p value |
| Age | 67.5 (59–74.5) | 68 (11.24–63.50) | 79 (10.95–72.00) | <0.0001 |
| CHARLSON [score] | 2 (0–4) | 3.00 (1.86–1.00) | 5 (2.28–3.00) | 0.0002 |
| Tumour diameter [mm] | 28 (23–34.5) | 30 (8.62–24.50) | 35.50 (7.48–31.00) | <0.0001 |
| Erytrocyt/RBC [mln/mL] | 4.58 (4.17–4.94) | 5 (0.68–4.80) | 4.92 (0.72–4.43) | 0.0032 |
| RDW-CV [%] | 13,6 (12.85–14.6) | 13,90 (1.20–13.10) | 14.75 (1.91–13.90) | <0.0001 |
| RDW-SD [%] | 44.5 (41.85–47.2) | 44.55 (3.60–42.55) | 48.3 (5.89–45.85) | <0.0001 |
| Haemoglobin [g/L] | 13.7 (12.5–14.85) | 15 (1.61–14.20) | 14.65 (2.00–13.20) | 0.0074 |
| Platelets [1000/uL] | 231 (197.5–281.5) | 291.50 (68.20–237.50) | 272.50 (61.83–224.50) | 0.0744 |
| Neutrophiles [1000/uL] | 4.7 (3.75–5.95) | 5.93 (2.08–4.76) | 6.02 (2.56–4.69) | 0.8951 |
| Lymphocytes [1000/uL] | 1.81 (1.53–2.16) | 2.21 (0.64–1.78) | 2.15 (0.78–1.84) | 0.6490 |
| Monocytes [1000/uL] | 0.64 (0.5–0.78) | 0.76 (0.27–0.62) | 0.81 (0.27–0.66) | 0.2605 |
| PLR | 130.44 (98.4–161.58) | 174.04 (63.94–147.25) | 159 (51.85–120.3) | 0.0959 |
| NLR | 2.59 (1.84–3.31) | 4.17 (1.88–2.47) | 3.2 (1.47–2.64) | 0.939 |
| LMR | 3.07 (2.16–3.85) | 4.18 (1.49–3.25) | 3.56 (1.17–3.02) | 0.3300 |
| Days in the hospital | 8 (3.07–11.0) | 8.1 (1.24–8.00) | 3.00 (2.30–3.00) | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rusinek, M.; Salagierski, M.; Różański, W.; Jakóbczyk, B.; Markowski, M.; Lipiński, M.; Wilkosz, J. Comparison of the Results of Therapy for cT1 Renal Carcinoma with Nephron-Sparing Surgery (NSS) vs. Percutaneous Thermal Ablation (TA). J. Pers. Med. 2022, 12, 495. https://doi.org/10.3390/jpm12030495
Rusinek M, Salagierski M, Różański W, Jakóbczyk B, Markowski M, Lipiński M, Wilkosz J. Comparison of the Results of Therapy for cT1 Renal Carcinoma with Nephron-Sparing Surgery (NSS) vs. Percutaneous Thermal Ablation (TA). Journal of Personalized Medicine. 2022; 12(3):495. https://doi.org/10.3390/jpm12030495
Chicago/Turabian StyleRusinek, Michał, Marek Salagierski, Waldemar Różański, Bartłomiej Jakóbczyk, Michał Markowski, Marek Lipiński, and Jacek Wilkosz. 2022. "Comparison of the Results of Therapy for cT1 Renal Carcinoma with Nephron-Sparing Surgery (NSS) vs. Percutaneous Thermal Ablation (TA)" Journal of Personalized Medicine 12, no. 3: 495. https://doi.org/10.3390/jpm12030495
APA StyleRusinek, M., Salagierski, M., Różański, W., Jakóbczyk, B., Markowski, M., Lipiński, M., & Wilkosz, J. (2022). Comparison of the Results of Therapy for cT1 Renal Carcinoma with Nephron-Sparing Surgery (NSS) vs. Percutaneous Thermal Ablation (TA). Journal of Personalized Medicine, 12(3), 495. https://doi.org/10.3390/jpm12030495