
The Effects of a Patient-Specific Integrated Education Program on Pain, Perioperative Anxiety, and Functional Recovery following Total Knee Replacement

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
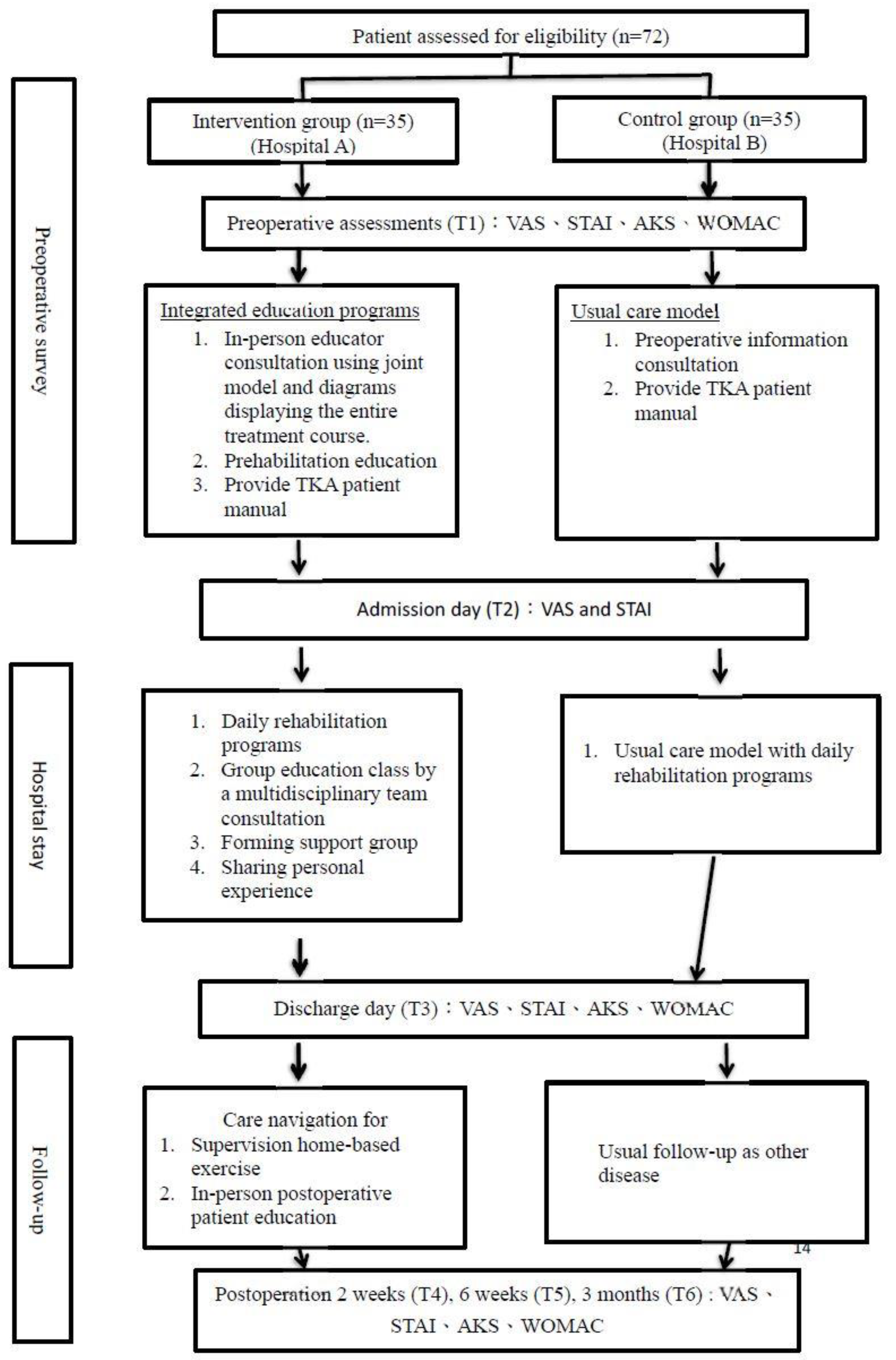
2.1. Study Design
2.2. Participants
2.3. Intervention Group (Hospital A)
2.4. Control Group (Hospital B)
2.5. Outcome Assessments
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics and Preoperative Assessment
3.2. IEP Reduced the Clinical Pain Intensity Pre-and Postoperatively
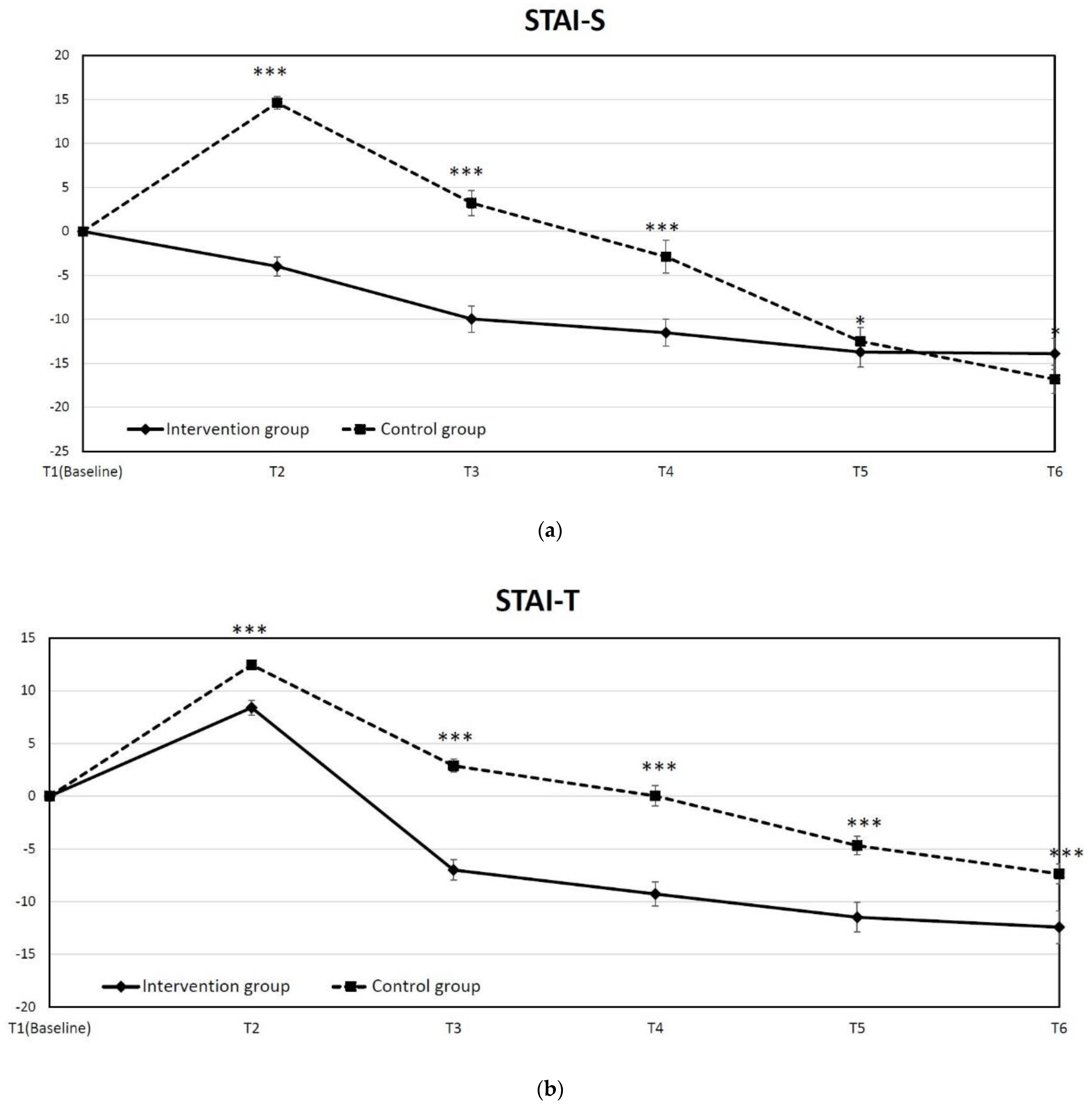
3.3. IEP Reduced Both State and Trait Anxiety in TKR
3.4. IEP Enhanced the Physical Function after TKR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Clinical Trial Registration System
References
- Rupp, M.; Lau, E.; Kurtz, S.M.; Alt, V. Projections of Primary TKA and THA in Germany from 2016 Through 2040. Clin. Orthop. Relat. Res. 2020, 478, 1622–1633. [Google Scholar] [CrossRef] [PubMed]
- Culliford, D.; Maskell, J.; Judge, A.; Cooper, C.; Prieto-Alhambra, D.; Arden, N.K.; COASt Study Group. Future projections of total hip and knee arthroplasty in the UK: Results from the UK Clinical Practice Research Datalink. Osteoarthr. Cartil. 2015, 23, 594–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inacio, M.; Paxton, E.; Graves, S.; Namba, R.; Nemes, S. Projected increase in total knee arthroplasty in the United States—An alternative projection model. Osteoarthr. Cartil. 2017, 25, 1797–1803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Argenson, J.-N.A.; Husted, H.; Lombardi, A.; Booth, R.E.; Thienpont, E. Global Forum: An International Perspective on Outpatient Surgical Procedures for Adult Hip and Knee Reconstruction. J. Bone Jt. Surg. 2016, 98, e55. [Google Scholar] [CrossRef] [PubMed]
- Berend, M.E.; Lackey, W.G.; Carter, J.L. Outpatient-Focused Joint Arthroplasty Is the Future: The Midwest Center for Joint Replacement Experience. J. Arthroplast. 2018, 33, 1647–1648. [Google Scholar] [CrossRef] [PubMed]
- Stark, J.; Ingadottir, B.; Salanterä, S.; Sigurdardottir, A.K.; Valkeapää, K.; Bachrach-Lindström, M.; Unosson, M. Fulfilment of knowledge expectations and emotional state among people undergoing hip replacement: A multi-national survey. Int. J. Nurs. Stud. 2014, 51, 1491–1499. [Google Scholar] [CrossRef] [Green Version]
- Solano, M.A.; Ramcharran, K.K.; Jones, L.C.; Sterling, R.S.; Samaroo, D.R.; Khanuja, H.S. Preoperative Patient Education Class During an Orthopedic Mission Trip: Effects on Knowledge, Anxiety, and Informed Consent. J. Arthroplast. 2020, 35, 2410–2417. [Google Scholar] [CrossRef]
- Madan, A.K.; Tichansky, D.S. Patients Postoperatively Forget Aspects of Preoperative Patient Education. Obes. Surg. 2005, 15, 1066–1069. [Google Scholar] [CrossRef]
- Gandhi, R.; Mahomed, N.N.; Cram, P.; Perruccio, A.V. Understanding the Relationship Between 3-Month and 2-Year Pain and Function Scores after Total Knee Arthroplasty for Osteoarthritis. J. Arthroplast. 2018, 33, 1368–1372. [Google Scholar] [CrossRef]
- Williams, D.; O’Brien, S.; Doran, E.; Price, A.; Beard, D.; Murray, D.; Beverland, D. Early postoperative predictors of satisfaction following total knee arthroplasty. Knee 2013, 20, 442–446. [Google Scholar] [CrossRef]
- McDonald, D.D.; Freeland, M.; Thomas, G.; Moore, J. Testing a preoperative pain management intervention for elders. Res. Nurs. Health 2001, 24, 402–409. [Google Scholar] [CrossRef] [PubMed]
- Louw, A.; Zimney, K.; Reed, J.; Landers, M.; Puentedura, E.J. Immediate Preoperative Outcomes of Pain Neuroscience Education for Patients Undergoing Total Knee Arthroplasty: A Case Series. Physiother. Theory Pract. 2019, 35, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Tilbury, C.; Haanstra, T.M.; Leichtenberg, C.S.; Verdegaal, S.H.; Ostelo, R.W.; de Vet, H.C.; Nelissen, R.G.; Vlieland, T.V. Unfulfilled Expectations after Total Hip and Knee Arthroplasty Surgery: There Is a Need for Better Preoperative Patient Information and Education. J. Arthroplast. 2016, 31, 2139–2145. [Google Scholar] [CrossRef]
- Lingard, E.A.; Riddle, D.L. Impact of Psychological Distress on Pain and Function Following Knee Arthroplasty. J. Bone Jt. Surg. Am. 2007, 89, 1161–1169. [Google Scholar] [CrossRef]
- Ginsel, B.L.; Heesterbeek, P.J.C. Pain and Depression Influence Outcome 5 Years after Knee Replacement Surgery. Clin. Orthop. Relat. Res. 2007, 464, 21–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paulsen, M.G.; Dowsey, M.M.; Castle, D.; Choong, P.F.M. Preoperative psychological distress and functional outcome after knee replacement. ANZ J. Surg. 2011, 81, 681–687. [Google Scholar] [CrossRef]
- Pan, X.; Wang, J.; Lin, Z.; Dai, W.; Shi, Z. Depression and Anxiety Are Risk Factors for Postoperative Pain-Related Symptoms and Complications in Patients Undergoing Primary Total Knee Arthroplasty in the United States. J. Arthroplast. 2019, 34, 2337–2346. [Google Scholar] [CrossRef]
- Hiyama, Y.; Kamitani, T.; Wada, O. Association between disease-specific anxiety at discharge and functional outcome in patients after total knee arthroplasty. Knee 2019, 26, 477–483. [Google Scholar] [CrossRef]
- Alattas, S.A.; Smith, T.; Bhatti, M.; Wilson-Nunn, D.; Donell, S. Greater pre-operative anxiety, pain and poorer function predict a worse outcome of a total knee arthroplasty. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 3403–3410. [Google Scholar] [CrossRef] [Green Version]
- McDonald, S.; Page, M.J.; Beringer, K.; Wasiak, J.; Sprowson, A. Pre-Operative Education for Hip or Knee Replacement. Cochrane Database Syst. Rev. 2004, Cd003526. [Google Scholar] [CrossRef]
- Moyer, R.; Ikert, K.; Long, K.; Marsh, J. The Value of Preoperative Exercise and Education for Patients Undergoing Total Hip and Knee Arthroplasty: A Systematic Review and Meta-Analysis. JBJS Rev. 2017, 5, e2. [Google Scholar] [CrossRef] [PubMed]
- Calatayud, J.; Casaña, J.; Ezzatvar, Y.; Jakobsen, M.D.; Sundstrup, E.; Andersen, L.L. High-Intensity Preoperative Training Improves Physical and Functional Recovery in the Early Post-Operative Periods after Total Knee Arthroplasty: A Randomized Controlled Trial. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 2864–2872. [Google Scholar] [CrossRef]
- Hoogeboom, T.J.; Oosting, E.; Vriezekolk, J.E.; Veenhof, C.; Siemonsma, P.C.; de Bie, R.A.; Ende, C.H.M.V.D.; van Meeteren, N.L.U. Therapeutic Validity and Effectiveness of Preoperative Exercise on Functional Recovery after Joint Replacement: A Systematic Review and Meta-Analysis. PLoS ONE 2012, 7, e38031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabilan, C.; Hines, S.; Munday, J. The effectiveness of prehabilitation or preoperative exercise for surgical patients: A systematic review. JBI Evid. Synth. 2015, 13, 146–187. [Google Scholar] [CrossRef] [PubMed]
- Kahn, T.L.; Soheili, A.; Schwarzkopf, R. Outcomes of Total Knee Arthroplasty in Relation to Preoperative Patient-Reported and Radiographic Measures: Data from the Osteoarthritis Initiative. Geriatr. Orthop. Surg. Rehabil. 2013, 4, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Fortin, P.R.; Clarke, A.E.; Joseph, L.; Liang, M.H.; Tanzer, M.; Ferland, D.; Phillips, C.; Partridge, A.J.; Fossel, A.H.; Mahomed, N.; et al. Outcomes of total hip and knee replacement: Preoperative functional status predicts outcomes at six months after surgery. Arthritis Rheum. 1999, 42, 1722–1728. [Google Scholar] [CrossRef]
- Jones, C.A.; Voaklander, D.C.; Suarez-Almazor, M.E. Determinants of Function After Total Knee Arthroplasty. Phys. Ther. 2003, 83, 696–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kennedy, D.M.; Hanna, S.E.; Stratford, P.; Wessel, J.; Gollish, J.D. Preoperative Function and Gender Predict Pattern of Functional Recovery After Hip and Knee Arthroplasty. J. Arthroplast. 2006, 21, 559–566. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Intervention Group (n = 35) | Control Group (n = 35) | ||||||
|---|---|---|---|---|---|---|---|
| Variables | Mean | SD | Rang | Mean | SD | Rang | p |
| Age | 73.5 | 5.3 | 68–85 | 74.4 | 5.4 | 65–86 | 0.521 |
| Gender | 0.073 | ||||||
| Male | 10 | 28.6% | 4 | 11.4% | |||
| Female | 25 | 71.4% | 31 | 88.6% | |||
| BMI | 28.0 | 3.2 | 23.2–38.1 | 26.6 | 4.0 | 17.8–40.1 | 0.058 |
| Education level | 0.068 | ||||||
| Illiterate | 7 | 20.0% | 11 | 31.4% | |||
| Elementary school | 13 | 37.1% | 17 | 48.6% | |||
| Junior high school | 5 | 14.3% | 2 | 5.7% | |||
| Senior high school | 9 | 25.7% | 4 | 11.4% | |||
| College or above | 1 | 2.9% | 1 | 2.8% | |||
| Pain (VAS) | 7.1 | 1.8 | 4–10 | 7.3 | 1.4 | 5–10 | 0.585 |
| State anxiety | 33.9 | 10.6 | 20–54 | 29.6 | 5.5 | 20.40 | 0.178 |
| Trait anxiety | 33.9 | 10.5 | 20.57 | 30.0 | 6.8 | 21–50 | 0.208 |
| AKS | 56.6 | 9.5 | 28–73 | 59.2 | 7.3 | 38–70 | 0.202 |
| WOMAC | 51.1 | 13.5 | 24–88 | 44.5 | 11.1 | 23–88 | 0.009 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, C.-J.; Chen, Y.-T.; Wu, H.-L.; Huang, H.-T.; Lin, S.-Y. The Effects of a Patient-Specific Integrated Education Program on Pain, Perioperative Anxiety, and Functional Recovery following Total Knee Replacement. J. Pers. Med. 2022, 12, 719. https://doi.org/10.3390/jpm12050719
Ho C-J, Chen Y-T, Wu H-L, Huang H-T, Lin S-Y. The Effects of a Patient-Specific Integrated Education Program on Pain, Perioperative Anxiety, and Functional Recovery following Total Knee Replacement. Journal of Personalized Medicine. 2022; 12(5):719. https://doi.org/10.3390/jpm12050719
Chicago/Turabian StyleHo, Cheng-Jung, Yen-Ti Chen, Hung-Lan Wu, Hsuan-Ti Huang, and Sung-Yen Lin. 2022. "The Effects of a Patient-Specific Integrated Education Program on Pain, Perioperative Anxiety, and Functional Recovery following Total Knee Replacement" Journal of Personalized Medicine 12, no. 5: 719. https://doi.org/10.3390/jpm12050719