
Evaluation of Pharmacogenetics of Drug-Metabolizing Enzymes and Drug Efflux Transporter in Renal Transplants Receiving Immunosuppressants

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Ethics
2.2. Study Procedure
2.3. Estimation of Genetic Polymorphisms
2.4. Estimation of Blood Tacrolimus, Sirolimus, and Cyclosporine Concentrations
2.5. Laboratory Reference Ranges
2.6. Statistical Analysis
3. Results
3.1. Demographics
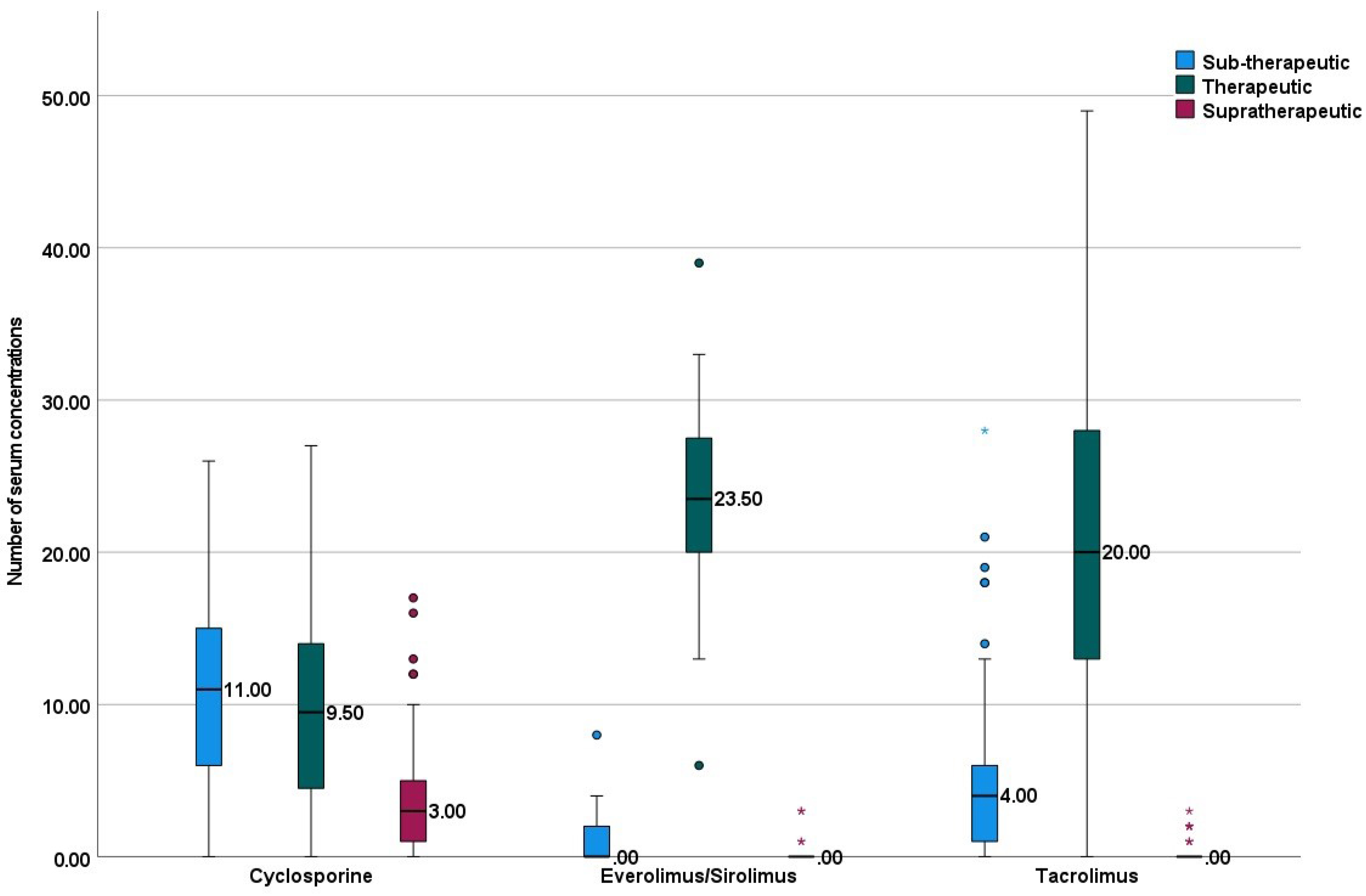
3.2. Immunosuppressive Drugs and Serum Levels
3.3. Prevalence of SNPs
3.4. Association between Drug Concentrations and SNPs
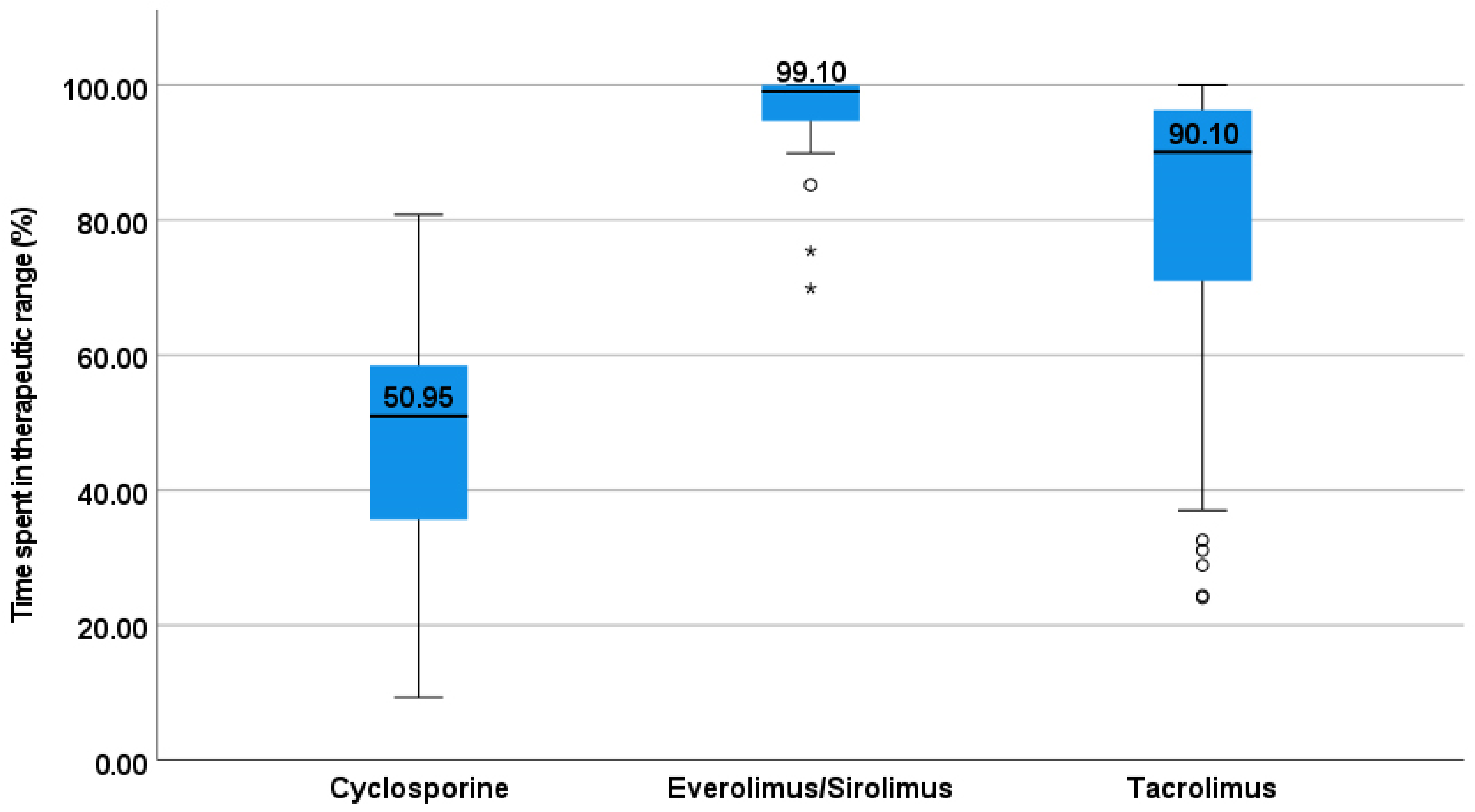
3.5. Association of SNPs with the Time Spent in the Therapeutic Range
3.6. Association of SNPs with the Laboratory Adverse Events
4. Discussion
4.1. Key Findings from the Present Study
4.2. Comparison with the Existing Literature
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gomes, R.M.; Barbosa, W.B.; Godman, B.; Costa, J.D.O.; Junior, N.G.R.; Filho, C.S.; Cherchiglia, M.L.; Acurcio, F.D.A.; Júnior, A.A.G. Effectiveness of Maintenance Immunosuppression Therapies in a Matched-Pair Analysis Cohort of 16 Years of Renal Transplant in the Brazilian National Health System. Int. J. Environ. Res. Public Health 2020, 17, 1974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ekberg, H.; Tedesco-Silva, H.; Demirbas, A.; Vítko, Š.; Nashan, B.; Guerkan, A.; Margreiter, R.; Hugo, C.; Grinyó, J.M.; Frei, U.; et al. Reduced Exposure to Calcineurin Inhibitors in Renal Transplantation. N. Engl. J. Med. 2007, 357, 2562–2575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seyfinejad, B.; Jouyban, A. Overview of therapeutic drug monitoring of immunosuppressive drugs: Analytical and clinical practices. J. Pharm. Biomed. Anal. 2021, 205, 114315. [Google Scholar] [CrossRef] [PubMed]
- Staatz, C.E.; Isbel, N.M.; Bergmann, T.K.; Jespersen, B.; Buus, N.H. Editorial: Therapeutic Drug Monitoring in Solid Organ Transplantation. Front. Pharmacol. 2021, 12, 815117. [Google Scholar] [CrossRef] [PubMed]
- Coto, E.; Tavira, B.; Suárez-Álvarez, B.; López-Larrea, C.; Díaz-Corte, C.; Ortega, F.; Alvarez, V. Pharmacogenetics of tacrolimus: Ready for clinical translation? Kidney Int. Suppl. 2011, 1, 58–62. [Google Scholar] [CrossRef] [Green Version]
- Sata, F.; Sapone, A.; Elizondo, G.; Stocker, P.; Miller, V.P.; Zheng, W.; Raunio, H.; Crespi, C.L.; Gonzalez, F.J. CYP3A4 allelic variants with amino acid substitutions in exons 7 and 12: Evidence for an allelic variant with altered catalytic activity. Clin. Pharmacol. Ther. 2000, 67, 48–56. [Google Scholar] [CrossRef]
- Mulder, T.A.M.; van Eerden, R.A.G.; de With, M.; Elens, L.; Hesselink, D.A.; Matic, M.; Bins, S.; Mathijssen, R.H.J.; van Schaik, R.H.N. CYP3A4*22 Genotyping in Clinical Practice: Ready for Implementation? Front. Genet. 2021, 12, 711943. [Google Scholar] [CrossRef]
- Wang, D.; Guo, Y.; Wrighton, S.A.; Cooke, G.E.; Sadee, W. Intronic polymorphism in CYP3A4 affects hepatic expression and response to statin drugs. Pharm. J. 2011, 11, 274–286. [Google Scholar] [CrossRef] [Green Version]
- Provenzani, A.; Santeusanio, A.; Mathis, E.; Notarbartolo, M.; Labbozzetta, M.; Poma, P.; Provenzani, A.; Polidori, C.; Vizzini, G.; Polidori, P.; et al. Pharmacogenetic considerations for optimizing tacrolimus dosing in liver and kidney transplant patients. World J. Gastroenterol. 2013, 19, 9156–9173. [Google Scholar] [CrossRef]
- Hustert, E.; Haberl, M.; Burk, O.; Wolbold, R.; He, Y.-Q.; Klein, K.; Nuessler, A.C.; Neuhaus, P.; Klattig, J.; Eiselt, R.; et al. The genetic determinants of the CYP3A5 polymorphism. Pharmacogenetics 2001, 11, 773–779. [Google Scholar] [CrossRef]
- Choudhuri, S.; Klaassen, C.D. Structure, Function, Expression, Genomic Organization, and Single Nucleotide Polymorphisms of Human ABCB1 (MDR1), ABCC (MRP), and ABCG2 (BCRP) Efflux Transporters. Int. J. Toxicol. 2006, 25, 231–259. [Google Scholar] [CrossRef] [PubMed]
- Brambila-Tapia, A.J.L. MDR1 (ABCB1) polymorphisms: Functional effects and clinical implications. Rev. Investig. Clin. 2013, 65, 445–454. [Google Scholar]
- Wang, R.; Sun, X.; Deng, Y.S.; Qiu, X.W. Effects of MDR1 1236C > T-2677G > T-3435C > T polymorphisms on the intracellular accumulation of tacrolimus, cyclosporine A, sirolimus and everolimus. Xenobiotica 2019, 49, 1373–1378. [Google Scholar] [PubMed]
- Klein, K.; Thomas, M.; Winter, S.; Nussler, A.K.; Niemi, M.; Schwab, M.; Zanger, U.M. PPARA: A Novel Genetic Determinant of CYP3A4 In Vitro and In Vivo. Clin. Pharmacol. Ther. 2012, 91, 1044–1052. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.V.; Sproll, P. Pharmacogenomics of human P450 oxidoreductase. Front. Pharmacol. 2014, 5, 103. [Google Scholar] [CrossRef] [Green Version]
- Zanger, U.M.; Schwab, M. Cytochrome P450 enzymes in drug metabolism: Regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol. Ther. 2013, 138, 103–141. [Google Scholar] [CrossRef]
- Sridharan, K.; Al Banna, R.; Malalla, Z.; Husain, A.; Sater, M.; Jassim, G.; Otoom, S. Influence of CYP2C9, VKORC1, and CYP4F2 polymorphisms on the pharmacodynamic parameters of warfarin: A cross-sectional study. Pharmacol. Rep. 2021, 73, 1405–1417. [Google Scholar] [CrossRef]
- Yang, G.; Fu, Z.; Chen, X.; Yuan, H.; Yang, H.; Huang, Y.; Ouyang, D.; Tan, Z.; Tan, H.; Huang, Z.; et al. Effects of the CYP Oxidoreductase Ala503Val Polymorphism on CYP3A Activity In Vivo: A Randomized, Open-Label, Crossover Study in Healthy Chinese Men. Clin. Ther. 2011, 33, 2060–2070. [Google Scholar] [CrossRef]
- Zhou, Y.; Ingelman-Sundberg, M.; Lauschke, V.M. Worldwide Distribution of Cytochrome P450 Alleles: A Meta-analysis of Population-scale Sequencing Projects. Clin. Pharmacol. Ther. 2017, 102, 688–700. [Google Scholar] [CrossRef] [Green Version]
- Jithesh, P.V.; Abuhaliqa, M.; Syed, N.; Ahmed, I.; El Anbari, M.; Bastaki, K.; Sherif, S.; Umlai, U.-K.; Jan, Z.; Gandhi, G.; et al. A population study of clinically actionable genetic variation affecting drug response from the Middle East. NPJ Genom. Med. 2022, 7, 10. [Google Scholar] [CrossRef]
- Tang, J.; Andrews, L.; Van Gelder, T.; Shi, Y.; Van Schaik, R.; Wang, L.; Hesselink, D. Pharmacogenetic aspects of the use of tacrolimus in renal transplantation: Recent developments and ethnic considerations. Expert Opin. Drug Metab. Toxicol. 2016, 12, 555–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jonge, H.; de Loor, H.; Verbeke, K.; Vanrenterghem, Y.; Kuypers, D.R. Impact of CYP3A5 genotype on tacrolimus versus midazolam clearance in renal transplant recipients: New insights in CYP3A5-mediated drug metabolism. Pharmacogenomics 2013, 14, 1467–1480. [Google Scholar] [CrossRef] [PubMed]
- Vannaprasaht, S.; Reungjui, S.; Supanya, D.; Sirivongs, D.; Pongskul, C.; Avihingsanon, Y.; Tassaneeyakul, W. Personalized Tacrolimus Doses Determined by CYP3A5 Genotype for Induction and Maintenance Phases of Kidney Transplantation. Clin. Ther. 2013, 35, 1762–1769. [Google Scholar] [CrossRef] [PubMed]
- Elens, L.; Bouamar, R.; Hesselink, D.A.; Haufroid, V.; van der Heiden, I.P.; van Gelder, T.; van Schaik, R.H. A new functional CYP3A4 intron 6 polymorphism significantly affects tacrolimus pharmacokinetics in kidney transplant recipients. Clin. Chem. 2011, 57, 1574–1583. [Google Scholar] [CrossRef] [Green Version]
- Moes, D.; Swen, J.; Hartigh, J.D.; van der Straaten, T.; van der Heide, J.H.; Sanders, J.; Bemelman, F.; de Fijter, J.; Guchelaar, H. Effect of CYP3A4*22, CYP3A5*3, and CYP3A Combined Genotypes on Cyclosporine, Everolimus, and Tacrolimus Pharmacokinetics in Renal Transplantation. CPT Pharmacometr. Syst. Pharmacol. 2014, 3, 100–112. [Google Scholar] [CrossRef]
- Abdel-Kahaar, E.; Winter, S.; Tremmel, R.; Schaeffeler, E.; Olbricht, C.J.; Wieland, E.; Schwab, M.; Shipkova, M.; Jaeger, S.U. The Impact of CYP3A4*22 on Tacrolimus Pharmacokinetics and Outcome in Clinical Practice at a Single Kidney Transplant Center. Front. Genet. 2019, 10, 871. [Google Scholar] [CrossRef] [Green Version]
- Thervet, E.; Loriot, M.-A.; Barbier, S.; Buchler, M.; Ficheux, M.; Choukroun, G.; Toupance, O.; Touchard, G.; Alberti, C.; Le Pogamp, P.; et al. Optimization of Initial Tacrolimus Dose Using Pharmacogenetic Testing. Clin. Pharmacol. Ther. 2010, 87, 721–726. [Google Scholar] [CrossRef]
- Shuker, N.; Bouamar, R.; van Schaik, R.H.N.; Groningen, M.C.C.-V.; Damman, J.; Baan, C.C.; van de Wetering, J.; Rowshani, A.T.; Weimar, W.; van Gelder, T.; et al. A Randomized Controlled Trial Comparing the Efficacy of Cyp3a5 Genotype-Based with Body-Weight-Based Tacrolimus Dosing After Living Donor Kidney Transplantation. Am. J. Transplant. 2015, 16, 2085–2096. [Google Scholar] [CrossRef] [Green Version]
- Sherry, S.T.; Ward, M.-H.; Kholodov, M.; Baker, J.; Phan, L.; Smigielski, E.M.; Sirotkin, K. dbSNP: The NCBI database of genetic variation. Nucleic Acids Res. 2001, 29, 308–311. [Google Scholar] [CrossRef] [Green Version]
- Elens, L.; Hesselink, D.A.; Bouamar, R.; Budde, K.; de Fijter, J.W.; De Meyer, M.; Mourad, M.; Kuypers, D.R.J.; Haufroid, V.; van Gelder, T.; et al. Impact of POR*28 on the Pharmacokinetics of Tacrolimus and Cyclosporine A in Renal Transplant Patients. Ther. Drug Monit. 2014, 36, 71–79. [Google Scholar] [CrossRef]
- Lee, D.-H.; Lee, H.; Yoon, H.-Y.; Yee, J.; Gwak, H.-S. Association of P450 Oxidoreductase Gene Polymorphism with Tacrolimus Pharmacokinetics in Renal Transplant Recipients: A Systematic Review and Meta-Analysis. Pharmaceutics 2022, 14, 261. [Google Scholar] [CrossRef] [PubMed]
- Woillard, J.-B.; Kamar, N.; Coste, S.; Rostaing, L.; Marquet, P.; Picard, N. Effect of CYP3A4*22, POR*28, and PPARA rs4253728 on Sirolimus In Vitro Metabolism and Trough Concentrations in Kidney Transplant Recipients. Clin. Chem. 2013, 59, 1761–1769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, R.B.; Leake, B.F.; Choo, E.F.; Dresser, G.K.; Kubba, S.V.; Schwarz, U.I.; Taylor, A.; Xie, H.G.; McKinsey, J.; Zhou, S.; et al. Identification of functionally variant MDR1 alleles among European Americans and African Americans. Clin. Pharmacol. Ther. 2001, 70, 189–199. [Google Scholar] [CrossRef] [PubMed]
- Abanda, N.N.; Riches, Z.; Collier, A.C. Lobular Distribution and Variability in Hepatic ATP Binding Cassette Protein B1 (ABCB1, P-gp): Ontogenetic Differences and Potential for Toxicity. Pharmaceutics 2017, 9, 8. [Google Scholar] [CrossRef]
- Shao, S.; Hu, L.; Han, Z.; Hou, K.; Fang, H.; Zhang, G.; Feng, Y.; Huang, L. The effect of ABCB1 polymorphism on sirolimus in renal transplant recipients: A meta-analysis. Transl. Androl. Urol. 2020, 9, 673–683. [Google Scholar] [CrossRef]
- Llaudó, I.; Colom, H.; Giménez-Bonafé, P.; Torras, J.; Caldés, A.; Sarrias, M.; Cruzado, J.M.; Oppenheimer, F.; Sánchez-Plumed, J.; Gentil, M.; et al. Do drug transporter (ABCB1) SNPs and P-glycoprotein function influence cyclosporine and macrolides exposure in renal transplant patients? Results of the pharmacogenomic substudy within the symphony study. Transpl. Int. 2012, 26, 177–186. [Google Scholar] [CrossRef]
- He, Y.; Ma, Y.; Fu, Q.; Liang, J.; Yu, X.; Huang, H.; Zhong, L.; Huang, B. The CYP3A5 and ABCB1 Gene Polymorphisms in Kidney Transplant Patients and Establishment of Initial Daily Tacrolimus Dosing Formula. Ann. Pharmacother. 2021, 56, 393–400. [Google Scholar] [CrossRef]
- Azam, F.; Khan, M.; Khaliq, T.; Bhatti, A.H. Influence of ABCB1 gene polymorphism on concentration to dose ratio and adverse effects of tacrolimus in Pakistani liver transplant recipients. Pak. J. Med Sci. 2021, 37, 689–694. [Google Scholar] [CrossRef]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases; 2012. Cyclosporine. [Updated 17 February 2020]. Available online: https://www.ncbi.nlm.nih.gov/books/NBK548753/ (accessed on 31 March 2022).
- Gulbis, B.; Adler, M.; Ooms, H.A.; Desmet, J.M.; Leclerc, J.L.; Primo, G. Liver-function studies in heart-transplant recipients treated with cyclosporin A. Clin. Chem. 1988, 34, 1772–1774. [Google Scholar] [CrossRef]
- Lo, P.; Kearney, K.; Muir, C.A.; Song, N.; Eisman, J.A.; Macdonald, P.S. Severe Hypertriglyceridemia Associated with Everolimus Treatment After Heart Transplantation. AACE Clin. Case Rep. 2020, 6, e269–e272. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | Values | |
|---|---|---|
| Age (years) $ | 50.5 (21–74) | |
| Males: Females (n) | 90: 56 | |
| Duration of renal transplantation (years) | 7 (1–34) | |
| Immunosuppressive drugs (n) # | Tacrolimus | 77 |
| Cyclosporine | 44 | |
| Everolimus | 23 | |
| Sirolimus | 4 | |
| Concomitant disorders (n) | Systemic hypertension | 118 |
| Diabetes mellitus | 60 | |
| Dyslipidemia | 65 | |
| Hyperuricemia | 15 | |
| Immunosuppressant Drugs | Dosing Regimen Per Day (n) | Median (Range) Dose/Day (mg) |
|---|---|---|
| Cyclosporine (n = 44) | 25 mg OD (4) | 100 (25–450) |
| 25 mg BD (2) | ||
| 50 mg BD (16) | ||
| 75 mg OD (1) | ||
| 75 mg BD (2) | ||
| 100 mg BD (5) | ||
| 200 mg BD (3) | ||
| 225 mg BD (1) | ||
| 25-0-50 mg (1) | ||
| 25-0-75 mg (1) | ||
| 50-0-100 mg (1) | ||
| 50-0-25 mg (3) | ||
| 50-0-75 mg (1) | ||
| 75-0-50 mg (1) | ||
| 100-0-50 mg (1) | ||
| 100-0-175 mg (1) | ||
| Everolimus (n = 24) | 0.25 mg OD (1) | 1 (0.25–2) |
| 0.25 mg BD (1) | ||
| 0.5 mg BD (9) | ||
| 0.75 mg OD (1) | ||
| 1 mg OD (2) | ||
| 1 mg BD (5) | ||
| 1.5 mg OD (1) | ||
| 0.25-0-0.5 mg (1) | ||
| 0.5-0-0.25 mg (1) | ||
| 1-0-0.75 mg (1) | ||
| 1-0-1 mg (1) | ||
| Sirolimus (n = 3) | 1 mg OD (3) | 1 |
| Tacrolimus (n = 77) | 0.5 mg OD (1) | 2 (0.5–9.5) |
| 0.5 mg BD (5) | ||
| 1 mg OD (1) | ||
| 1 mg BD (24) | ||
| 1.5 mg BD (3) | ||
| 2 mg OD (1) | ||
| 2 mg BD (7) | ||
| 3 mg BD (4) | ||
| 3.5 mg BD (1) | ||
| 1.5-0-1 mg (1) | ||
| 1-0-0.5 mg (17) | ||
| 1-0-1.5 mg (2) | ||
| 2.5-0-2.5 mg (1) | ||
| 2-0-1 mg (1) | ||
| 2-0-1.5 mg (1) | ||
| 2-0-2 mg (1) | ||
| 2-0-2.5 mg (1) | ||
| 3-0-2 mg (2) | ||
| 3-0-2.5 mg (1) | ||
| 4-0-3 mg (1) | ||
| 5-0-4.5 mg (1) |
| SNPs | Numbers (%) | |
|---|---|---|
| ABCB1 | AA | 26 (17.8) |
| AG | 80 (54.8) | |
| GG | 40 (27.4) | |
| POR*28 | CC | 66 (45.2) |
| CT | 62 (42.5) | |
| TT | 18 (12.3) | |
| PPAR-alpha | AA | 7 (4.8) |
| AG | 45 (30.8) | |
| GG | 94 (64.4) | |
| CYP3A4*22 | GG | 120 (82.2) |
| GA | 20 (13.7) | |
| AA | 6 (4.3) | |
| CYP3A5*3 | TT | 8 (5.5) |
| CT | 46 (31.5) | |
| CC | 92 (63) | |
| SNPs | Median (Range) Dose-Adjusted Concentrations | p-Values | |
|---|---|---|---|
| CYP3A4*22 | GG | 2.8 (0.3–19.7) | 0.8 |
| GA | 2.9 (0.5–23.8) | ||
| AA | 2.7 (0.9–5.2) | ||
| CYP3A5*3 | TT | 2.5 (1.5–7.3) | 0.4 |
| CT | 2.2 (0.6–23.8) | ||
| CC | 3.2 (0.3–19.7) | ||
| ABCB1 | AA | 3.3 (0.7–7) | 0.6 |
| AG | 3.1 (0.3–23.8) | ||
| GG | 2.3 (0.4–9.4) | ||
| PPAR-alpha | AA | 2.6 (1–5.8) | 0.2 |
| AG | 2.6 (0.3–7.3) | ||
| GG | 3.1 (0.4–23.8) | ||
| POR*28 | CC | 4 (0.6–12.5) | 0.003 * |
| CT | 1.8 (0.3–19.7) | ||
| TT | 3.9 (0.5–23.8) | ||
| POR*28 activity | Normal | 2.6 (0.3–19.8) | 0.09 |
| Higher | 3.9 (0.5–23.8) | ||
| SNPs | Cyclosporine | Everolimus/Sirolimus | Tacrolimus | ||||
|---|---|---|---|---|---|---|---|
| Median (Range) Concentrations | p-Values a,b | Median (Range) Concentrations | p-Values a,b | Median (Range) Concentrations | p-Values a,b | ||
| CYP3A4*22 | GG | 103 | 0.2; 0.4 | 5.5 (3.6–12.1) | 0.4; 0.4 | 7.6 (4.2–16.5) | 0.2; 0.09 |
| (69.9–333.5) | |||||||
| GA | 120.6 | 5.6 (5.2–10.1) | 6.8 (4.8–8.5) | ||||
| (102.1–162.1) | |||||||
| AA | 90.5 | Nil | 7.7 (3.8–8.2) | ||||
| CYP3A5*3 | TT | 114.1 | 0.7; 0.6 | 5.9 (5.5–6.4) | 0.8; 0.8 | 1.8 (1.5–5.3) | 0.3; 0.3 |
| CT | 116 | 5.5 (4.9–6.4) | 2.7 (0.8–7) | ||||
| (69.9–247.7) | |||||||
| CC | 99.2 | 5.4 (3.6–12.1) | 4.3 (1–19.7) | ||||
| (83.3–333.5) | |||||||
| ABCB1 | AA | 98.8 | 0.1; 0.7 | 5.3 (5–5.6) | 0.2; 0.6 | 7.7 (5.3–10.7) | 0.01*; 0.02 * |
| (85.4–107.1) | |||||||
| AG | 113.1 | 5.7 (3.9–12.1) | 7.8 (4.8–16.5) | ||||
| (84.3–247.7) | |||||||
| GG | 97.2 | 4.7 (3.6–7.9) | 6.7 (3.8–9.9) | ||||
| (69.9–333.5) | |||||||
| PPAR-alpha | AA | 101.4 | 0.3; 0.2 | 5.5 | 0.5; 0.4 | 7.8 (4.8–8.7) | 0.6; 0.4 |
| (98.4–104.4) | |||||||
| AG | 115.6 | 5.3 (4.6–12.1) | 7 (3.8–11) | ||||
| (69.9–333.5) | |||||||
| GG | 99 (83.3–247.7) | 5.6 (3.6–10.1) | 7.7 (4.2–16.5) | ||||
| POR*28 | CC | 98.8 | 0.4; 0.9 | 5.6 (3.9–12.1) | 0.5; 0.3 | 7.8 (4.2–13.5) | 0.8; 0.9 |
| (83.3–333.5) | |||||||
| CT | 105.6 | 5.3 (4.9–10) | 7.1 (3.8–16.5) | ||||
| (69.9–204.3) | |||||||
| TT | 96.7 | 5.1 (3.6–6) | 7.7 (4.7–10.7) | ||||
| (85.4–114.1) | |||||||
| POR*28 activity | Normal | 103 (41–69.8) | NA | 5.5 (3.9–12.1) | NA | 7.5 (3.8–16.5) | NA |
| Higher | 96.7 (85.4–114) | 5.1 (3.6–6) | 7.7 (4.7–10.7) | ||||
| SNPs | Cyclosporine | Everolimus/Sirolimus | Tacrolimus | ||||
|---|---|---|---|---|---|---|---|
| Median (range) Dose-Adjusted Concentrations | p-Values a,b | Median (range) Dose-Adjusted Concentrations | p-Values a,b | Median (Range) Dose-Adjusted Concentrations | p-Values a,b | ||
| CYP3A4*22 | GG | 1.1 (0.3–4.6) | 0.6; 0.3 | 5.1 (2.7–7.9) | 0.7; 0.7 | 3.6 (0.8–19.7) | 0.2; 0.08 |
| GA | 0.7 (0.5–1.6) | 5.2 (2.6–23.8) | 2.9 (1–4.3) | ||||
| AA | 0.9 | Nil | 3.4 (1.3–5.2) | ||||
| CYP3A5*3 | TT | 1.5 | 0.2; 0.2 | 6.8 (6.4–7.3) | 0.2; 0.9 | 1.8 (1.5–5.3) | 0.05 *; 0.2 |
| CT | 1.2 (0.6–4.6) | 5.7 (4.9–23.8) | 2.7 (0.8–7) | ||||
| CC | 1 (0.3–4.1) | 4.9 (2.6–7.9) | 4.3 (1–19.7) | ||||
| ABCB1 | AA | 1.1 (0.7–4) | 0.5; 0.9 | 5.1 (2.8–5.3) | 0.3; 0.8 | 3.5 (1.3–7) | 0.7; 0.5 |
| AG | 1 (0.3–4.6) | 6.1 (2.7–23.8) | 3.7 (0.8–19.7) | ||||
| GG | 1.2 (0.4–4.1) | 4.7 (2.6–7.9) | 2.7 (0.8–9.4) | ||||
| PPAR-alpha | AA | 1.2 (1–1.4) | 0.09; 0.08 | 3.7 | 0.6; 0.7 | 2.9 (1–5.8) | 0.3; 0.09 |
| AG | 0.8 (0.3–2.2) | 5.3 (4.6–7.3) | 3.4 (1–5.3) | ||||
| GG | 1.2 (0.4–4.6) | 5 (2.6–23.8) | 3.6 (0.8–19.7) | ||||
| POR*28 | CC | 1.1 (0.6–4.6) | 0.05 *; 0.02 * | 5.5 (2.8–7.9) | 0.8; 0.5 | 4.6 (1–12.5) | 0.007 *; 0.5 |
| CT | 0.9 (0.3–4.1) | 5.3 (2.6–7.3) | 2.6 (0.8–19.7) | ||||
| TT | 0.7 (0.5–1.5) | 4.2 (2.7–23.8) | 4.9 (2.4–7) | ||||
| POR*28 activity | Normal | 1 (0.3–4.6) | NA | 5.3 (2.6–7.9) | NA | 3.2 (0.8–19.7) | NA |
| Higher | 0.7 (0.5–1.5) | 4.2 (2.7–23.8) | 4.9 (2.4–7) | ||||
| SNPs | Cyclosporine | Everolimus/Sirolimus | Tacrolimus | ||||
|---|---|---|---|---|---|---|---|
| Median (Range) Time Spent in Therapeutic Range (%) | p-Values a | Median (Range) Time Spent in Therapeutic Range (%) | p-Values a | Median (Range) Time Spent in Therapeutic Range (%) | p-Values a | ||
| CYP3A4*22 | GG | 50.2 (9–81) | 0.2 | 97 (52–100) | 0.3 | 90.5 (24.4–100) | 0.8 |
| GA | 63.8 (55–70) | 99 (44–100) | 75.8 (32.6–100) | ||||
| AA | 49.4 | NA | 87.1 (24.1–100) | ||||
| CYP3A5*3 | TT | 49.5 | 0.8 | 92.6 (85.2–100) | 0.7 | 91.8 (37.6–96.6) | 0.7 |
| CT | 54.7 (17–85) | 99.6 (96.1–100) | 90.1 (37.6–100) | ||||
| CC | 51 (9–81) | 96.3 (44–100) | 85.8 (24.1–100) | ||||
| ABCB1 | AA | 46.4 (35–52) | 0.04 * | 100 (99.2–100) | 0.05 * | 87.3 (38.7–99.1) | 0.2 |
| AG | 56.5 (17–81) | 96.6 (44–100) | 93.6 (31.1–100) | ||||
| GG | 40.5 (9–66) | 75.4 (60–100) | 85.6 (24.1–100) | ||||
| PPAR-alpha | AA | 55 (51–59) | 0.3 | 97 | 0.4 | 91.7 (89.6–96.5) | 0.8 |
| AG | 55.3 (35–70) | 100 (60–100) | 91.3 (24.1–100) | ||||
| GG | 49.2 (9–81) | 95.8 (44–100) | 87 (24.4–100) | ||||
| POR*28 | CC | 50.2 (9–81) | 0.6 | 93.9 (44–100) | 0.08 | 91.7 (24.4–100) | 0.4 |
| CT | 56.5 (17–70) | 100 (93–100) | 85.8 (24.1–100) | ||||
| TT | 47.6 (46–50) | 95.8 (69.9–97) | 87.6 (28.9–99.1) | ||||
| POR*28 activity | Normal | 51.4 (9–81) | 0.5 | 99.6 (44–100) | 0.07 | 90.5 (24.1–100) | 0.6 |
| Higher | 47.6 (46–50) | 95.8 (69.9–97) | 87.6 (28.9–99.1) | ||||
| Adverse Events | Number of Patients | Cyclosporine | Everolimus/ Sirolimus | Tacrolimus | p-Values |
|---|---|---|---|---|---|
| Elevated serum creatinine (number of events = 49) | Number of patients | 15 (37.5%) | 6 (24%) | 28 (37.3%) | 0.4 |
| Total number of patients evaluated | 40 | 25 | 75 | ||
| Hyperbilirubinemia (number of events = 20) | Number of patients | 9 (45%) | 1 (7.7%) | 10 (25%) | 0.06 |
| Total number of patients evaluated | 20 | 13 | 40 | ||
| Elevated GGT (number of events = 34) | Number of patients | 15 (35.7%) | 7 (28%) | 12 (16.2%) | 0.05 * |
| Total number of patients evaluated | 42 | 25 | 74 | ||
| Hypercholesterolemia (number of events = 92) | Number of patients | 28 (65.1%) | 20 (80%) | 44 (60.3%) | 0.2 |
| Total number of patients evaluated | 43 | 25 | 73 | ||
| Hypertriglyceridemia (number of events = 116) | Number of patients | 36 (83.7%) | 20 (80%) | 60 (62.5%) | 0.8 |
| Total number of patients evaluated | 4 | 25 | 96 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sridharan, K.; Shah, S.; Jassim, A.; Hammad, M.; Ebrahim Al Gadhban, J.; Al Segai, O. Evaluation of Pharmacogenetics of Drug-Metabolizing Enzymes and Drug Efflux Transporter in Renal Transplants Receiving Immunosuppressants. J. Pers. Med. 2022, 12, 823. https://doi.org/10.3390/jpm12050823
Sridharan K, Shah S, Jassim A, Hammad M, Ebrahim Al Gadhban J, Al Segai O. Evaluation of Pharmacogenetics of Drug-Metabolizing Enzymes and Drug Efflux Transporter in Renal Transplants Receiving Immunosuppressants. Journal of Personalized Medicine. 2022; 12(5):823. https://doi.org/10.3390/jpm12050823
Chicago/Turabian StyleSridharan, Kannan, Shamik Shah, Anfal Jassim, Mona Hammad, Johaina Ebrahim Al Gadhban, and Ola Al Segai. 2022. "Evaluation of Pharmacogenetics of Drug-Metabolizing Enzymes and Drug Efflux Transporter in Renal Transplants Receiving Immunosuppressants" Journal of Personalized Medicine 12, no. 5: 823. https://doi.org/10.3390/jpm12050823
APA StyleSridharan, K., Shah, S., Jassim, A., Hammad, M., Ebrahim Al Gadhban, J., & Al Segai, O. (2022). Evaluation of Pharmacogenetics of Drug-Metabolizing Enzymes and Drug Efflux Transporter in Renal Transplants Receiving Immunosuppressants. Journal of Personalized Medicine, 12(5), 823. https://doi.org/10.3390/jpm12050823