
Validity and Reliability of the Dental Neglect Scale among Romanian Adults

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Dental Neglect Scale
3. Materials and Methods
3.1. Translating and Adapting the Scale
3.2. Ethical Consideration
3.3. Design and Data Collection
3.4. Measures
3.5. Sociodemographic Variables
3.6. The Hypotheses
3.7. Data Analysis
4. Results
4.1. Socio-Demographic Characteristics
4.2. The Descriptive Analysis
4.3. The Convergent Validity
4.4. Gender Differences
4.5. DNS and Other Socio-Demographic Characteristics
4.6. The Exploratory Factor Analysis
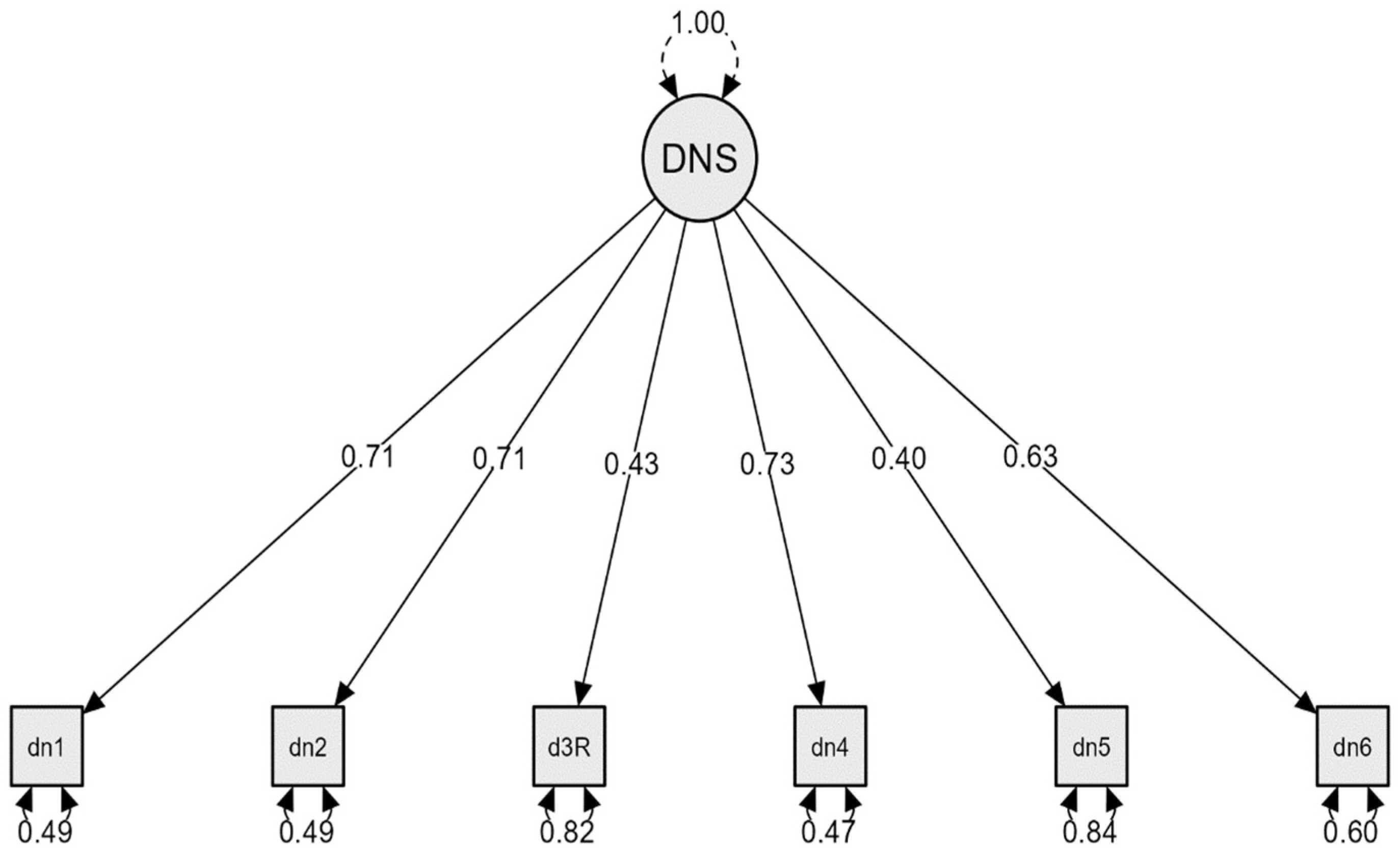
4.7. The Confirmatory Factor Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Thomson, W.M.; Spencer, A.J.; Gaughwin, A. Testing a child dental neglect scale in South Australia. Community Dent. Oral Epidemiol. 1996, 24, 351–356. [Google Scholar] [CrossRef]
- Spiller, L.; Lukefahr, J.; Kellogg, N. Dental Neglect. J. Child Adolesc. Trauma 2019, 13, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Lourenço, C.B.; Saintrain, M.V.; Vieira, A.P. Child, neglect and oral health. BMC Pediatr. 2013, 13, 188. [Google Scholar] [CrossRef] [Green Version]
- Thomson, W.M.; Locker, D. Dental neglect and dental health among 26-year-olds in the Dunedin Multidisciplinary Health and Development Study. Community Dent Oral Epidemiol. 2000, 28, 414–418. [Google Scholar] [CrossRef] [PubMed]
- Jamieson, L.M.; Thomson, W.M. The Dental Neglect and Dental Indifference scales compared. Community Dent. Oral Epidemiol. 2002, 30, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Skaret, E.; Astrøm, A.N.; Haugejorden, O.; Klock, K.S.; Trovik, T.A. Assessment of the reliability and validity of the Dental Neglect Scale in Norwegian adults. Community Dent. Health 2007, 24, 247–252. [Google Scholar]
- Ortega, C.E.T.; Caparó, E.V.; Barahona, C.P.A.; Chávez, J.K.H.; Chauca, B.N.C. Neglect of dental care in young adults of the Parish Baños Cuenca-Ecuador, 2017. Científica Espec. Odontológicas UG. 2021, 4, 29–36. [Google Scholar]
- Coolidge, T.; Heima, M.; Johnson, E.K.; Weinstein, P. The Dental Neglect Scale in adolescents. BMC Oral Health 2009, 9, 2. [Google Scholar] [CrossRef] [Green Version]
- Ajagannanavar, S.L.; Sequeira, P.S.; Jain, J.; Battur, H. Dental neglect among college going adolescents in Virajpet, India. J. Indian Assoc. Public Health Dent. 2014, 12, 215–218. [Google Scholar] [CrossRef]
- Gurunathan, D.; Shanmugaavel, A.K. Dental neglect among children in Chennai. J. Indian Soc. Pedod. Prev. Dent. 2016, 34, 364–369. [Google Scholar] [CrossRef]
- Sharma, I.; Chauhan, P.; Galhotra, V.; Duhan, H.; Kaur, M. Dental Neglect among children and their parents in District Panchkula. Int. Healthc. Res. J. 2019, 2, 265–269. [Google Scholar] [CrossRef]
- Soares, R.C.; Moysés, S.T.; Rocha, J.S.; Baldani, M.H.; Werneck, R.I.; Moysés, S.J. Cross-cultural adaptation of the Dental Neglect Scale for five-year-old children in Brazil. Braz. Oral Res. 2021, 35, e115. [Google Scholar] [CrossRef]
- Sarkar, P.; Dasar, P.; Nagarajappa, S.; Mishra, P.; Kumar, S.; Balsaraf, S.; Lalani, A.; Chauhan, A. Impact of Dental Neglect Scale on Oral Health Status Among Different Professionals in Indore City-A Cross- Sectional Study. J. Clin. Diagn. Res. 2015, 9, ZC67–ZC70. [Google Scholar] [CrossRef]
- Athira, S.; Vallabhan, C.G.; Sivarajan, S.; Dithi, C.; Swathy Anand, P.J.; Chandran, T. Association of Dental Neglect Scale and severity of dental caries among Nursing Students: A cross-sectional Study. J. Pharm. Bioallied Sci. 2021, 13, S812–S816. [Google Scholar] [CrossRef]
- McGrath, C.; Sham, A.S.; Ho, D.K.; Wong, J.H. The impact of dental neglect on oral health: A population based study in Hong Kong. Int. Dent. J. 2007, 57, 3–8. [Google Scholar] [CrossRef]
- Bhattarai, R.; Khanal, S.; Shrestha, S.; Rao, G.N. Dental Neglect score and its association with oral hygiene and dental caries among adults visiting a tertiary Hospital in Kathmandu. J. Nepal. Soc. Periodontol. Oral Implantol. 2020, 4, 14–17. [Google Scholar] [CrossRef]
- Nuttall, N.M. Initial development of a scale to measure dental indifference. Community Dent. Oral Epidemiol. 1996, 24, 112–116. [Google Scholar] [CrossRef]
- Mahanta, S.K.; Humagain, M.; Upadhyaya, C.; Prajapati, D.; Srii, R. The impact of Dental Neglect on oral health among 16-30-year-olds in Dhulikhel, Kavrepalanchok, Nepal. J. Nepal. Soc. Periodontol. Oral Implantol. 2021, 5, 45–48. [Google Scholar] [CrossRef]
- Sanders, A.E.; Spencer, A.J.; Slade, G.D. Evaluating the role of dental behaviour in oral health inequalities. Community Dent. Oral Epidemiol. 2006, 34, 71–79. [Google Scholar] [CrossRef]
- Edwards, C.B.; Randall, C.L.; McNeil, D.W. Development and validation of the Oral Health Values Scale. Community Dent. Oral Epidemiol. 2021, 49, 454–463. [Google Scholar] [CrossRef]
- Edwards, C.B. Development and Validation of an Oral Health Values Scale. Ph.D. Theses, Eberly College of Arts and Sciences, Morgantown, WV, USA, 2017. Available online: https://researchrepository.wvu.edu/etd/5529 (accessed on 1 June 2022).
- Balgiu, B.A.; Sfeatcu, R.; Sluşanschi, O.; Dumitrache, M.A. Linguistic and cultural validation of the Romanian version of the Revised Dental Beliefs survey. Int. J. Med. Dent. 2020, 24, 381–389. [Google Scholar]
- Acharya, S.; Pentapati, K.; Bhat, P. Dental neglect and adverse birth outcomes: A validation and observational study. Int. J. Dent. Hyg. 2013, 11, 91–98. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Process of Translation and Adaptation of Instruments. 2020. Available online: http://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 1 June 2022).
- Milgrom, P.; Weinstein, P.; Getz, T. Treating Fearful Dental Patients: A Patient Management Handbook, 2nd ed.; University of Washington Continuing Dental Education: Seattle, WA, USA, 1995. [Google Scholar]
- Slade, G.D.; Spencer, A.J. Development and evaluation of the Oral Health Impact Profile. Community Dent. Health 1994, 11, 3–11. [Google Scholar] [PubMed]
- Slade, G.D. Derivation and validation of a short-form oral health impact profile. Community Dent. Oral Epidemiol. 1997, 25, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Slușanschi, O.; Moraru, R.; Garneata, L.; Mircescu, G.; Cuculescu, M.; Preoteasa, E. Validation of a Romanian version of the short form of the oral health impact profile (OHIP-14) for use in an urban adult population. Oral Health Prev. Dent. 2013, 11, 235–242. [Google Scholar] [CrossRef]
- Balgiu, B.A.; Sfeatcu, R.; Mihai, C.; Lupușoru, M.; Bucur, V.M.; Tribus, L. Romanian version of the Oral Health Values Scale: Adaptation and validation. Medicina 2022, 58, 544. [Google Scholar] [CrossRef]
- Kiyak, H.A. Measuring psychosocial variables that predict older persons’ oral health behaviour. Gerodontology. 1996, 13, 69–75. [Google Scholar] [CrossRef]
- Peterson, R.A.; Kim, Y. On the relationship between coefficient alpha and composite reliability. J. Appl. Psychol. 2013, 98, 194–198. [Google Scholar] [CrossRef]
- Hayes, A.F.; Coutts, J.J. Use omega rather than Cronbach’s alpha for estimating reliability. Commun. Methods Meas. 2020, 14, 1–24. [Google Scholar] [CrossRef]
- Field, A. Discovering Statistics Using SPSS, 3rd ed.; Sage: Beverly Hills, CA, USA, 2009. [Google Scholar]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 6th ed.; Allyn & Bacon/Pearson Education: Boston, MA, USA, 2013. [Google Scholar]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the fit of structural equation models: Tests of significance and descriptive goodness-of-fit measures. Methods Psychol. Res. 2003, 8, 23–74. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Modeling A Multidiscip. J. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Kim, H.Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar] [CrossRef] [PubMed]
- De Vaus, D.A. Analyzing Social Science Data: 50 Key Problems in Data Analysis, 1st ed.; Sage Publications Ltd.: Beverly Hills, CA, USA, 2002. [Google Scholar]
- Chechile, R.A. A Bayesian analysis for the Mann-Whitney statistic. Commun. Stat. Theory Methods 2019, 49, 670–696. [Google Scholar] [CrossRef]
- Van Doorn, J.; van den Bergh, D.; Böhm, U.; Dablander, F.; Derks, K.; Draws, T.; Etz, A.; Evans, N.J.; Gronau, Q.F.; Haaf, J.M.; et al. The JASP guidelines for conducting and reporting a Bayesian analysis. Psychon. Bull. Rev. 2021, 28, 813–826. [Google Scholar] [CrossRef]
- Labăr, A.V. SPSS Pentru Științele Educației [SPSS for Educational Sciences]; Polirom Publishing: Iaşi, Romania, 2008. [Google Scholar]
- Hancock, G.R.; Mueller, R.O. Structural Equation Modeling: A Second Course, 2nd ed.; Information Age Publishing: Charlotte, NC, USA, 2013. [Google Scholar]
- Nevitt, J.; Hancock, G.R. Performance of bootstrapping approaches to model test statistics and parameter standard error estimation in structural equation modelling. Struct. Equ. Modeling 2001, 8, 353–377. [Google Scholar] [CrossRef]
- Varian, H. Bootstrap tutorial. Math. J. 2005, 9, 768–775. Available online: http://www.mathematica-journal.com/issue/v9i4/BootstrapTutorial.html (accessed on 1 June 2022).
- Lee, J.Y.; Divaris, K.; Baker, A.D.; Rozier, R.G.; Vann, W.F., Jr. The relationship of oral health literacy and self-efficacy with oral health status and dental neglect. Am. J. Public Health 2012, 102, 923–929. [Google Scholar] [CrossRef]
- Janto, M.; Iurcov, R.; Daina, C.M.; Neculoiu, D.C.; Venter, A.C.; Badau, D.; Cotovanu, A.; Negrau, M.; Suteu, C.L.; Sabau, M.; et al. Oral health among elderly, impact on life quality, access of elderly patients to oral health services and methods to improve oral health: A narrative review. J. Pers. Med. 2022, 12, 372. [Google Scholar] [CrossRef]
- Machado, V.; Mendonça, A.; Proença, L.; Mendes, J.J.; Botelho, J.; McNeill, D.W.; Delgado, A.S. Cross-cultural adaptation and validation of the Oral Health Values Scale for the Portuguese Population. J. Pers. Med. 2022, 12, 672. [Google Scholar] [CrossRef]
- Henson, R.K.; Roberts, J.K. Use of exploratory factor analysis in published research: Common errors and some comment on improved practice. Educ. Psihol. Meas. 2006, 66, 393–416. [Google Scholar] [CrossRef] [Green Version]
- Thompson, A.E.; Anisimowicz, Y.; Miedema, B.; Hogg, W.; Wodchis, W.P.; Aubrey-Bassler, K. The influence of gender and other patient characteristics on health care-seeking behaviour: A QUALICOPC study. BMC Fam. Pract. 2016, 17, 38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aranza, D.; Nota, A.; Galić, T.; Kozina, S.; Tecco, S.; Poklepović Peričić, T.; Milavić, B. Development and initial validation of the Oral Health Activities Questionnaire. Int. J. Environ. Res. Public Health 2022, 19, 5556. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Items | M | S.D. | Skew. | Kurt. | α If Item Deleted | Corrected Item-Total Correlation |
|---|---|---|---|---|---|---|
| 1. I keep up my home dental care | 4.72 | 0.56 | −2.48 | 8.07 | 0.64 | 0.59 |
| 2. I receive the dental care I should | 4.33 | 0.95 | −1.34 | 1.07 | 0.61 | 0.57 |
| 3. I need dental care, but I put it off (reversed) | 3,71 | 1.31 | −0.68 | −0.77 | 0.69 | 0.38 |
| 4. I brush as well as I should | 4.56 | 0.69 | −1.79 | 3.83 | 0.64 | 0.54 |
| 5. I control snacking between meals as well as I should | 3.16 | 1.28 | −0.09 | −0.95 | 0.70 | 0.35 |
| 6. I consider my dental health to be important | 4.78 | 0.54 | −2.92 | 9.79 | 0.66 | 0.50 |
| ω = 0.70 (0.67–0.73) | ||||||
| α = 0.70 (0.66–0.72) |
| Percentiles | Scores | Qualitative Interpretation (Attitudes towards Oral Health Care) |
|---|---|---|
| 10th | 20.00 | Highly unfavorable |
| 25th | 23.00 | Favorable |
| 50th | 26.00 | Neutral |
| 75th | 28.00 | Unfavorable |
| 90th | 30.00 | Highly favorable |
| Measures | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. DNS | - | |||
| 2. OHIP-14 | –0.11 *** | - | ||
| 3. R-DBS | –0.13 *** | −0.20 *** | - | |
| 4. OHVS | 0.37 *** | –0.16 *** | –0.33 *** | - |
| 5. DIS | –0.42 *** | 0.12 *** | 0.25 *** | –0.49 *** |
| Groups | Mean Rank | Chi-Square (H) |
|---|---|---|
| Age group | ||
| 18–29 years | 379.27 | 88,743 df = 2; p < 0.001 |
| 30–49 years | 508.92 | |
| 50+ years | 595.36 | |
| Education * | ||
| High school | 389.03 | 16,433 df = 2; p < 0.001 |
| Universitary | 431.71 | |
| Post-universitary | 490.44 | |
| Work sector | ||
| Public | 213.76 | 4.73 df = 1; p = 0.030 |
| Private | 188.61 |
| Items | Component 1 |
|---|---|
| Item 1 | 0.80 |
| Item 2 | 0.72 |
| Item 3 | 0.60 |
| Item 4 | 0.70 |
| Item 5 | 0.54 |
| Item 6 | 0.68 |
| Variance % | 46.32% |
| Cronbach’s α | 0.70 (0.65–0.74) |
| McDonald’s ω | 0.70 (0.65–0.74) |
| Models | χ2 | df | χ2/df | CFI | NFI | TLI | RMSEA (90%CI) | SRMR | p |
|---|---|---|---|---|---|---|---|---|---|
| Default model | 10.199 | 9 | 1.13 | 0.99 | 0.97 | 0.99 | 0.017 (0.000–0.056) | 0.059 | 0.335 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balgiu, B.A.; Sfeatcu, R.; Mihai, C.; Ilici, R.R.; Parlatescu, I.; Tribus, L. Validity and Reliability of the Dental Neglect Scale among Romanian Adults. J. Pers. Med. 2022, 12, 1035. https://doi.org/10.3390/jpm12071035
Balgiu BA, Sfeatcu R, Mihai C, Ilici RR, Parlatescu I, Tribus L. Validity and Reliability of the Dental Neglect Scale among Romanian Adults. Journal of Personalized Medicine. 2022; 12(7):1035. https://doi.org/10.3390/jpm12071035
Chicago/Turabian StyleBalgiu, Beatrice Adriana, Ruxandra Sfeatcu, Christina Mihai, Roxana Romanița Ilici, Ioanina Parlatescu, and Laura Tribus. 2022. "Validity and Reliability of the Dental Neglect Scale among Romanian Adults" Journal of Personalized Medicine 12, no. 7: 1035. https://doi.org/10.3390/jpm12071035
APA StyleBalgiu, B. A., Sfeatcu, R., Mihai, C., Ilici, R. R., Parlatescu, I., & Tribus, L. (2022). Validity and Reliability of the Dental Neglect Scale among Romanian Adults. Journal of Personalized Medicine, 12(7), 1035. https://doi.org/10.3390/jpm12071035