
Head and Neck Cancer Types and Risks of Cervical–Cranial Vascular Complications within 5 Years after Radiation Therapy

 ,
,
Abstract
:1. Introduction
2. Methods
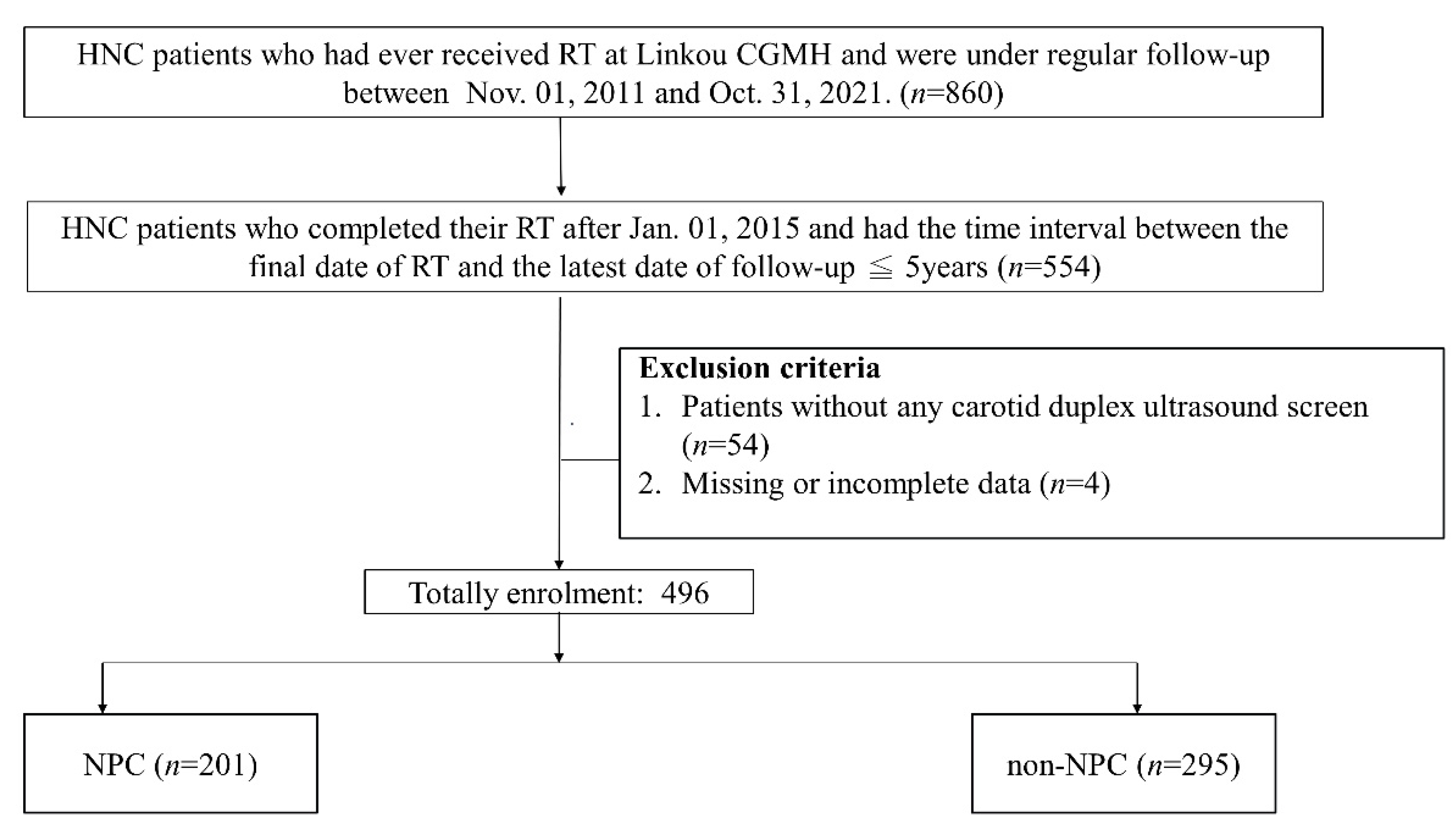
2.1. Patient Recruitment and Demographic Data
2.2. Cancer Treatment and RT Data
2.3. Grouping
2.4. Outcomes and Follow-Ups
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Abayomi, O.K. Neck irradiation, carotid injury and its consequences. Oral Oncol. 2004, 40, 872–878. [Google Scholar] [CrossRef] [PubMed]
- Carpenter, D.J.; Mowery, Y.M.; Broadwater, G.; Rodrigues, A.; Wisdom, A.J.; Dorth, J.A.; Patel, P.R.; Shortell, C.K.; Clough, R.; Brizel, D.M. The risk of carotid stenosis in head and neck cancer patients after radiation therapy. Oral Oncol. 2018, 80, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Gujral, D.M.; Chahal, N.; Senior, R.; Harrington, K.J.; Nutting, C.M. Radiation-induced carotid artery atherosclerosis. Radiother. Oncol. 2014, 110, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Arthurs, E.; Hanna, T.P.; Zaza, K.; Peng, Y.; Hall, S.F. Stroke After Radiation Therapy for Head and Neck Cancer: What Is the Risk? Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 589–596. [Google Scholar] [CrossRef]
- Plummer, C.; Henderson, R.D.; O’Sullivan, J.D.; Read, S.J. Ischemic stroke and transient ischemic attack after head and neck radiotherapy: A review. Stroke 2011, 42, 2410–2418. [Google Scholar] [CrossRef] [Green Version]
- Chang, Y.J.; Chang, T.C.; Lee, T.H.; Ryu, S.J. Predictors of carotid artery stenosis after radiotherapy for head and neck cancers. J. Vasc. Surg. 2009, 50, 280–285. [Google Scholar] [CrossRef] [Green Version]
- Wilbers, J.; Dorresteijn, L.D.; Haast, R.; Hoebers, F.J.; Kaanders, J.H.; Boogerd, W.; van Werkhoven, E.D.; Nowee, M.E.; Hansen, H.H.; de Korte, C.L.; et al. Progression of carotid intima media thickness after radiotherapy: A long-term prospective cohort study. Radiother. Oncol. 2014, 113, 359–363. [Google Scholar] [CrossRef]
- Zou, W.X.; Leung, T.W.; Yu, S.C.; Wong, E.H.; Leung, S.F.; Soo, Y.O.; Ip, V.H.; Chan, A.Y.; Lam, W.W.; Siu, D.Y.; et al. Angiographic features, collaterals, and infarct topography of symptomatic occlusive radiation vasculopathy: A case-referent study. Stroke 2013, 44, 401–406. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.W.; Wu, L.L.; Ting, A.C.; Lau, H.; Lam, L.K.; Wei, W.I. Irradiation-induced extracranial carotid stenosis in patients with head and neck malignancies. Am. J. Surg 1999, 178, 323–328. [Google Scholar] [CrossRef]
- Chou, Y.C.; Fan, K.H.; Lin, C.Y.; Hung, T.M.; Huang, B.S.; Chang, K.P.; Kang, C.J.; Huang, S.F.; Chang, P.H.; Hsu, C.L.; et al. Intensity Modulated Proton Beam Therapy versus Volumetric Modulated Arc Therapy for Patients with Nasopharyngeal Cancer: A Propensity Score-Matched Study. Cancers 2021, 13, 3555. [Google Scholar] [CrossRef]
- Mali, S.B. Proton therapy for head neck cancer. Oral Oncol. 2015, 51, e10–e12. [Google Scholar] [CrossRef] [PubMed]
- Leeman, J.E.; Romesser, P.B.; Zhou, Y.; McBride, S.; Riaz, N.; Sherman, E.; Cohen, M.A.; Cahlon, O.; Lee, N. Proton therapy for head and neck cancer: Expanding the therapeutic window. Lancet Oncol. 2017, 18, e254–e265. [Google Scholar] [CrossRef]
- Kim, J.K.; Leeman, J.E.; Riaz, N.; McBride, S.; Tsai, C.J.; Lee, N.Y. Proton Therapy for Head and Neck Cancer. Curr. Treat. Options Oncol. 2018, 19, 28. [Google Scholar] [CrossRef] [PubMed]
- Taheri-Kadkhoda, Z.; Bjork-Eriksson, T.; Nill, S.; Wilkens, J.J.; Oelfke, U.; Johansson, K.A.; Huber, P.E.; Munter, M.W. Intensity-modulated radiotherapy of nasopharyngeal carcinoma: A comparative treatment planning study of photons and protons. Radiat. Oncol. 2008, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Lewis, G.D.; Holliday, E.B.; Kocak-Uzel, E.; Hernandez, M.; Garden, A.S.; Rosenthal, D.I.; Frank, S.J. Intensity-modulated proton therapy for nasopharyngeal carcinoma: Decreased radiation dose to normal structures and encouraging clinical outcomes. Head Neck 2016, 38 (Suppl. 1), E1886–E1895. [Google Scholar] [CrossRef]
- Wang, H.M.; Lin, C.Y.; Hsieh, C.H.; Hsu, C.L.; Fan, K.H.; Chang, J.T.; Huang, S.F.; Kang, C.J.; Liao, C.T.; Ng, S.H.; et al. Induction chemotherapy with dose-modified docetaxel, cisplatin, and 5-fluorouracil in Asian patients with borderline resectable or unresectable head and neck cancer. J. Formos. Med. Assoc. 2017, 116, 185–192. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.H.; Lee, T.H.; Chang, P.Y.; Chang, C.H.; Wu, H.C.; Chang, T.Y.; Huang, K.L.; Cheng, C.K.; Chang, Y.J. Changes in E-Selectin Levels Predict Carotid Stenosis Progression after Carotid Artery Stenting. Curr. Neurovascular Res. 2018, 15, 18–25. [Google Scholar] [CrossRef]
- Liu, C.H.; Chang, C.H.; Chang, T.Y.; Huang, K.L.; Lin, J.R.; Chen, Y.W.; Yip, B.S.; Ryu, S.J.; Chang, Y.J.; Lee, T.H. Carotid artery stenting improves cerebral hemodynamics regardless of the flow direction of ophthalmic artery. Angiology 2015, 66, 180–186. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Alexandrov, A.V.; Tegeler, C.H.; Hobson, R.W., 2nd; Dennis Baker, J.; Hopkins, L.N. Guidelines for screening of extracranial carotid artery disease: A statement for healthcare professionals from the multidisciplinary practice guidelines committee of the American Society of Neuroimaging; cosponsored by the Society of Vascular and Interventional Neurology. J. Neuroimaging 2007, 17, 19–47. [Google Scholar] [CrossRef]
- Jacobowitz, G.R.; Rockman, C.B.; Gagne, P.J.; Adelman, M.A.; Lamparello, P.J.; Landis, R.; Riles, T.S. A model for predicting occult carotid artery stenosis: Screening is justified in a selected population. J. Vasc. Surg. 2003, 38, 705–709. [Google Scholar] [CrossRef] [Green Version]
- Dorth, J.A.; Patel, P.R.; Broadwater, G.; Brizel, D.M. Incidence and risk factors of significant carotid artery stenosis in asymptomatic survivors of head and neck cancer after radiotherapy. Head Neck 2014, 36, 215–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zuo, J.J.; Tao, Z.Z.; Chen, C.; Hu, Z.W.; Xu, Y.X.; Zheng, A.Y.; Guo, Y. Characteristics of cigarette smoking without alcohol consumption and laryngeal cancer: Overall and time-risk relation. A meta-analysis of observational studies. Eur. Arch. Oto-Rhino-Laryngol. 2017, 274, 1617–1631. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, P.; Singh, A.; Chien, C.Y.; Warnakulasuriya, S. Tobacco related oral cancer. BMJ 2019, 365, l2142. [Google Scholar] [CrossRef]
- Lin, J.H.; Wen, C.P.; Jiang, C.Q.; Yuan, J.M.; Chen, C.J.; Ho, S.Y.; Gao, W.; Zhang, W.; Wang, R.; Chien, Y.C.; et al. Smoking and nasopharyngeal cancer: Individual data meta-analysis of six prospective studies on 334 935 men. Int. J. Epidemiol. 2021, 50, 975–986. [Google Scholar] [CrossRef] [PubMed]
- Song, P.; Fang, Z.; Wang, H.; Cai, Y.; Rahimi, K.; Zhu, Y.; Fowkes, F.G.R.; Fowkes, F.J.I.; Rudan, I. Global and regional prevalence, burden, and risk factors for carotid atherosclerosis: A systematic review, meta-analysis, and modelling study. Lancet Glob. Health 2020, 8, e721–e729. [Google Scholar] [CrossRef]
- McClintock, T.R.; Parvez, F.; Wu, F.; Wang, W.; Islam, T.; Ahmed, A.; Shaheen, I.; Sarwar, G.; Demmer, R.T.; Desvarieux, M.; et al. Association between betel quid chewing and carotid intima-media thickness in rural Bangladesh. Int. J. Epidemiol. 2014, 43, 1174–1182. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.H.; Kim, Y.D.; Park, C.S.; Han, K.D.; Joo, Y.H. Hypertension is associated with oral, laryngeal, and esophageal cancer: A nationwide population-based study. Sci. Rep. 2020, 10, 10291. [Google Scholar] [CrossRef]
- Kim, S.Y.; Han, K.D.; Joo, Y.H. Metabolic Syndrome and Incidence of Laryngeal Cancer: A Nationwide Cohort Study. Sci. Rep. 2019, 9, 667. [Google Scholar] [CrossRef]
- Zucchetto, A.; Taborelli, M.; Bosetti, C.; Montella, M.; La Vecchia, C.; Franchin, G.; Libra, M.; Serraino, D.; Polesel, J. Metabolic disorders and the risk of nasopharyngeal carcinoma: A case-control study in Italy. Eur. J. Cancer Prev. 2018, 27, 180–183. [Google Scholar] [CrossRef]
- Guo, G.; Fu, M.; Wei, S.; Chen, R. Impact of diabetes mellitus on the risk and survival of nasopharyngeal carcinoma: A meta-analysis. Onco. Targets Ther. 2018, 11, 1193–1201. [Google Scholar] [CrossRef] [Green Version]
- Gellrich, N.C.; Handschel, J.; Holtmann, H.; Kruskemper, G. Oral cancer malnutrition impacts weight and quality of life. Nutrients 2015, 7, 2145–2160. [Google Scholar] [CrossRef]
- Manzoor, N.F.; Russell, J.O.; Bricker, A.; Koyfman, S.; Scharpf, J.; Burkey, B.; Khan, M.J. Impact of surgical resection on survival in patients with advanced head and neck cancer involving the carotid artery. JAMA Otolaryngol. Head Neck Surg. 2013, 139, 1219–1225. [Google Scholar] [CrossRef] [Green Version]
- Meilhac, A.; Cautela, J.; Thuny, F. Cancer Therapies and Vascular Toxicities. Curr. Treat. Options Oncol. 2022, 23, 333–347. [Google Scholar] [CrossRef] [PubMed]
- van Aken, E.S.M.; van der Laan, H.P.; Bijl, H.P.; Van den Bosch, L.; van den Hoek, J.G.M.; Dieters, M.; Steenbakkers, R.; Langendijk, J.A. Risk of ischaemic cerebrovascular events in head and neck cancer patients is associated with carotid artery radiation dose. Radiother. Oncol. 2021, 157, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.H.; Cheng, J.Y.; Huang, B.S.; Luo, S.D.; Lin, W.C.; Chou, S.Y.; Juang, P.J.; Li, S.H.; Huang, E.Y.; Wang, Y.M. Significant Reduction in Vertebral Artery Dose by Intensity Modulated Proton Therapy: A Pilot Study for Nasopharyngeal Carcinoma. J. Pers. Med. 2021, 11, 822. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.H.; Kwon, S.U.; Kim, J.S. Radiation-induced angiopathy in acute stroke patients. J. Stroke Cerebrovasc. Dis. 2002, 11, 315–319. [Google Scholar] [CrossRef]
- Bavle, A.; Srinivasan, A.; Choudhry, F.; Anderson, M.; Confer, M.; Simpson, H.; Gavula, T.; Thompson, J.S.; Clifton, S.; Gross, N.L.; et al. Systematic review of the incidence and risk factors for cerebral vasculopathy and stroke after cranial proton and photon radiation for childhood brain tumors. Neurooncol. Pract. 2021, 8, 31–39. [Google Scholar] [CrossRef]
- Embring, A.; Onjukka, E.; Mercke, C.; Lax, I.; Berglund, A.; Bornedal, S.; Wennberg, B.; Dalqvist, E.; Friesland, S. Re-Irradiation for Head and Neck Cancer: Cumulative Dose to Organs at Risk and Late Side Effects. Cancers 2021, 13, 3173. [Google Scholar] [CrossRef]
- Lee, A.; Kang, J.; Yu, Y.; McBride, S.; Riaz, N.; Cohen, M.; Sherman, E.; Michel, L.; Lee, N.; Tsai, C.J. Trends and Disparities of Proton Therapy Use among Patients with Head and Neck Cancer: Analysis from the National Cancer Database (2005–14). Int. J. Part. Ther. 2019, 5, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Kitpanit, S.; Lee, A.; Mah, D.; Sine, K.; Sherman, E.J.; Dunn, L.A.; Michel, L.S.; Fetten, J.; Zakeri, K.; et al. Toxicity Profiles and Survival Outcomes Among Patients With Nonmetastatic Nasopharyngeal Carcinoma Treated With Intensity-Modulated Proton Therapy vs Intensity-Modulated Radiation Therapy. JAMA Netw. Open 2021, 4, e2113205. [Google Scholar] [CrossRef]
- Kato, T.; Fuwa, N.; Murakami, M. Dose-Volume Comparison of IMRT and PSPT Treatment Plans for Early-Stage Glottic Cancer. Int. J. Part. Ther. 2020, 7, 42–50. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, K.; Minatogawa, H.; Dekura, Y.; Takao, S.; Tamura, M.; Tsushima, N.; Suzuki, T.; Kano, S.; Mizumachi, T.; Mori, T.; et al. Analysis of acute-phase toxicities of intensity-modulated proton therapy using a model-based approach in pharyngeal cancer patients. J. Radiat. Res. 2021, 62, 329–337. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Lee, A.; Cohen, M.A.; Sherman, E.J.; Lee, N.Y. Past, present and future of proton therapy for head and neck cancer. Oral Oncol. 2020, 110, 104879. [Google Scholar] [CrossRef] [PubMed]
- Chuong, M.; Bryant, J.; Hartsell, W.; Larson, G.; Badiyan, S.; Laramore, G.E.; Katz, S.; Tsai, H.; Vargas, C. Minimal acute toxicity from proton beam therapy for major salivary gland cancer. Acta Oncol. 2020, 59, 196–200. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| NPC (n = 201) | Non-NPC (n = 295) | p | |
|---|---|---|---|
| Demographics | |||
| Age (years) | 50.01 ± 10.84 | 58.42 ± 9.74 | <0.01 † |
| Sex (% male) | 165 (82.5%) | 269 (91.2%) | <0.01 † |
| Hypertension (%) | 28 (13.9%) | 58 (19.9%) | 0.08 |
| Diabetes mellitus (%) | 17 (8.5%) | 34 (11.6%) | 0.41 |
| Dyslipidemia (%) | 34 (16.9%) | 46 (15.8%) | 0.73 |
| Coronary artery disease (%) | 4 (2.0%) | 8 (2.7%) | 0.60 |
| Chronic kidney disease (%) | 1 (0.5%) | 1 (0.3%) | 0.91 |
| Previous ischemic stroke (%) | 0 (0.0%) | 3 (1.0%) | 0.27 |
| Smoking (%) | 77 (38.3%) | 166 (56.8%) | <0.01 † |
| Betel quid chewing (%) | 28 (14.0%) | 125 (42.8%) | <0.01 † |
| RT dose (centigrays) | 6808.82 ± 997.26 | 6624.07 ± 688.90 | 0.02 † |
| Proton beam therapy (%) | 85 (42.3%) | 47 (15.9%) | <0.01 † |
| Re-irradiation | 12 (6.0% | 19 (6.4%) | 0.84 |
| Cancer types | - | ||
| NPC | 201 (100%) | 0 (0%) | |
| Oral cavity/oropharyngeal cancer | 0 (0%) | 206 (69.8%) | |
| Laryngeal cancer | 0 (0%) | 23 (7.8%) | |
| Hypopharyngeal cancer | 0 (0%) | 59 (20.0%) | |
| Others | 0 (0%) | 7 (2.4%) | |
| Laboratory data | |||
| Glycated hemoglobin (%) | 5.66 ± 0.55 | 6.29 ± 0.58 | 0.29 |
| Creatinine (mg/dL) | 1.02 ± 1.08 | 1.04 ± 1.02 | 0.92 |
| LDL (mg/dL) | 125.54 ± 44.50 | 109.84 ± 44.66 | <0.01 † |
| HDL (mg/dL) | 54.81 ± 16.08 | 49.55 ± 15.39 | <0.01 † |
| Triglyceride (mg/dL) | 128.52 ± 93.58 | 147.54 ± 97.73 | 0.05 |
| Free T4 (ng/dL) | 1.25 ± 3.71 | 1.35 ± 6.67 | 0.86 |
| CDU data at enrollment | |||
| Mean IMT (left), mm | 0.93 ± 2.84 | 0.82 ± 0.42 | 0.54 |
| Mean IMT (right), mm | 0.68 ± 0.24 | 0.76 ± 0.36 | 0.01 † |
| Total plaque scores | 1.21 ± 2.48 | 2.73 ± 4.13 | <0.01 † |
| Time from RT to the first CDU (months) | 22.82 ± 14.35 | 21.79 ± 14.14 | 0.44 |
| Time from RT to the last vascular follow-up (months) | 33.16 ± 15.34 | 31.57 ± 16.37 | 0.28 |
| Outcome | NPC n = 201 (%) | Non-NPC n = 295 (%) | NPC vs. Non-NPC | |
|---|---|---|---|---|
| Adjusted HR (95% CI) | p-Value | |||
| Primary analysis # | ||||
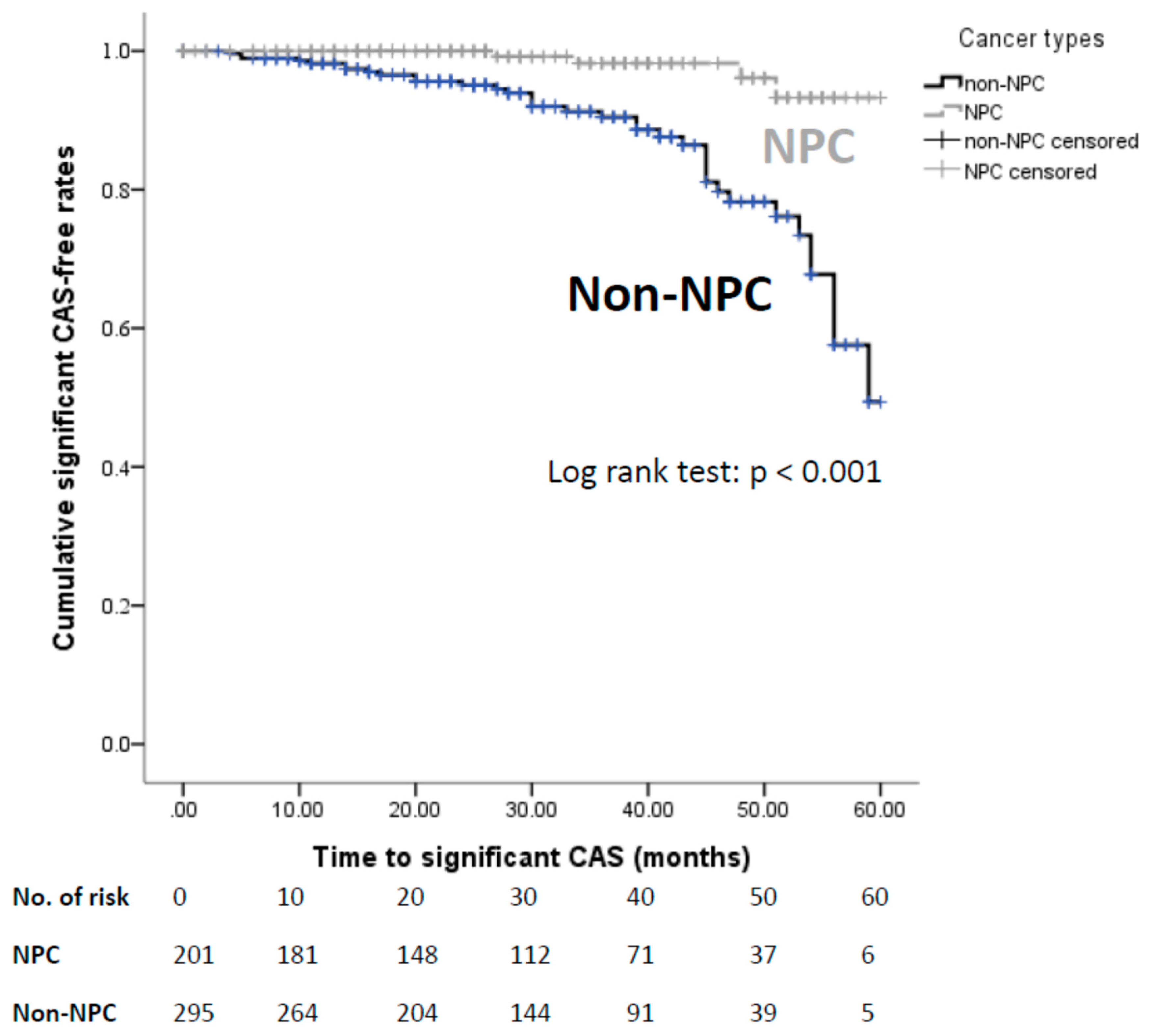
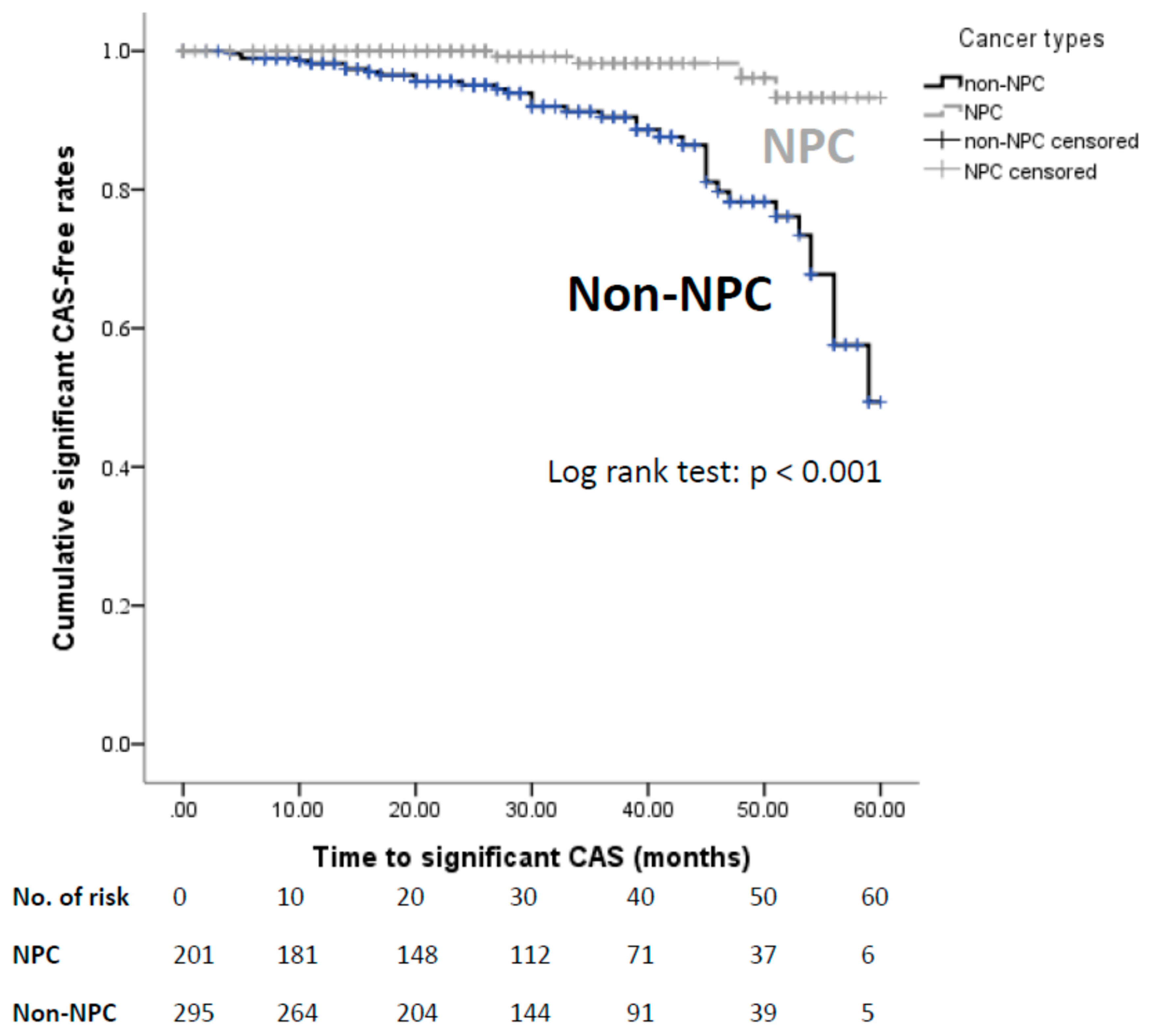
| Diagnosis of significant CAS | 4 (2.0) | 37 (12.7) | 0.17 (0.05, 0.57) | 0.004 † |
| Secondary outcomes * | ||||
| Significant VA stenosis | 2 (1.0) | 5 (1.7) | 0.71 | |
| ICAS | 7 (3.5) | 7 (2.4) | 0.47 | |
| Ischemic stroke | 2 (1.0) | 1 (0.3) | 0.57 | |
| Carotid artery interventions | 0 (0.0) | 2 (0.7) | 0.52 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, C.-H.; Huang, B.-S.; Lin, C.-Y.; Yeh, C.-H.; Lee, T.-H.; Wu, H.-C.; Chang, C.-H.; Chang, T.-Y.; Huang, K.-L.; Jiang, J.-L.; et al. Head and Neck Cancer Types and Risks of Cervical–Cranial Vascular Complications within 5 Years after Radiation Therapy. J. Pers. Med. 2022, 12, 1060. https://doi.org/10.3390/jpm12071060
Liu C-H, Huang B-S, Lin C-Y, Yeh C-H, Lee T-H, Wu H-C, Chang C-H, Chang T-Y, Huang K-L, Jiang J-L, et al. Head and Neck Cancer Types and Risks of Cervical–Cranial Vascular Complications within 5 Years after Radiation Therapy. Journal of Personalized Medicine. 2022; 12(7):1060. https://doi.org/10.3390/jpm12071060
Chicago/Turabian StyleLiu, Chi-Hung, Bing-Shen Huang, Chien-Yu Lin, Chih-Hua Yeh, Tsong-Hai Lee, Hsiu-Chuan Wu, Chien-Hung Chang, Ting-Yu Chang, Kuo-Lun Huang, Jian-Lin Jiang, and et al. 2022. "Head and Neck Cancer Types and Risks of Cervical–Cranial Vascular Complications within 5 Years after Radiation Therapy" Journal of Personalized Medicine 12, no. 7: 1060. https://doi.org/10.3390/jpm12071060
APA StyleLiu, C. -H., Huang, B. -S., Lin, C. -Y., Yeh, C. -H., Lee, T. -H., Wu, H. -C., Chang, C. -H., Chang, T. -Y., Huang, K. -L., Jiang, J. -L., Chang, J. T. -C., & Chang, Y. -J. (2022). Head and Neck Cancer Types and Risks of Cervical–Cranial Vascular Complications within 5 Years after Radiation Therapy. Journal of Personalized Medicine, 12(7), 1060. https://doi.org/10.3390/jpm12071060