4.1. Main Findings
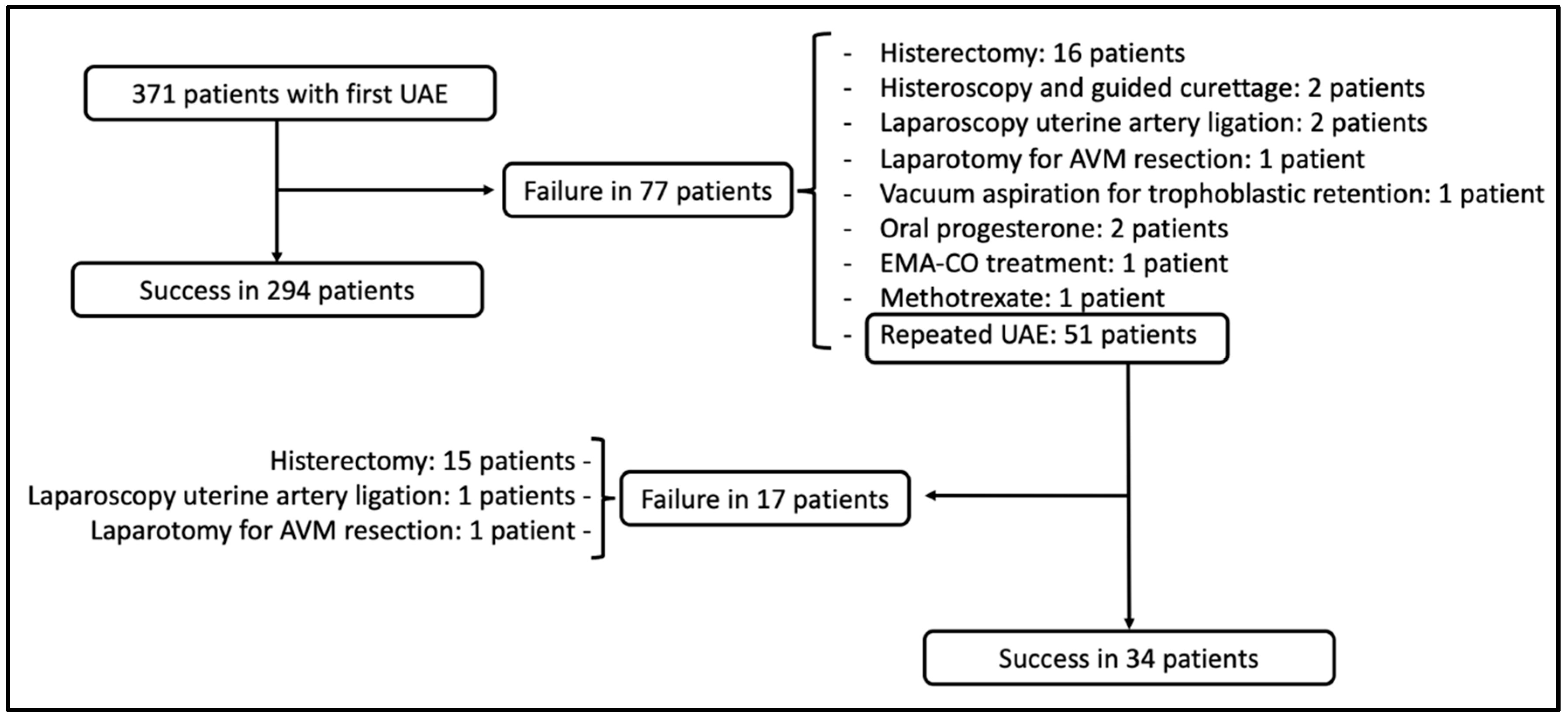
In this systematic review of 95 studies, we evaluated data for 371 patients who received UAE for treatment of UAVM. The global success rate after embolization treatment was 88.4%, with 79.2% after first embolization and 66.7% after repeated embolization. As well, 91.6% of the patients with UAVM had a history of an obstetric event, the most frequent being a history of abortion (48% of the patients). Only 1.6% of the patients presented major complications associated with UAE, especially in the form of pulmonary embolism. Finally, 77 patients (20.7%) who had a pregnancy after UAE for UAVM were collected, 77% of whom had no complications and there was no recurrence of UAVM in any case.
The profile of the patient who underwent UAE by UAVM was that of a young patient (31 years old) of reproductive age with a mean parity of 1.19. These data highlight that embolization is a treatment that preserves fertility and, therefore, is especially indicated in young patients who may have a future reproductive desire.
The primary UAE success rate after first embolization (79.2%) described in our study is above the rate of 61% provided by the previous systematic review that included patients from 2003 to 2013 [
10]. We have verified that in the articles published in the last 10 years, a significant improvement in success has been observed compared to the previous period (
p < 0.05), which could be related to an improvement in technical equipment, embolizing material, and the increased experience of professionals performing this treatment more frequently in recent years. The fact that the success rate after the first embolization is higher than after repeated embolizations (79.2% vs. 66.7%) indicates that the longer it takes to correct the bleeding, the less successful the embolization is. The time factor has been associated with the failure of other obstetric hemorrhage treatments, such as the Bakri balloon [
13]. There have been no studies comparing the effectiveness of repeat embolization versus medical therapy or hysterectomy for persistent bleeding after initial embolization. Clinical factors that predict the success or failure of embolization should be sought, but the studies published to date provide heterogeneous data that are very difficult to systematize in order to carry out this analysis.
In 2021, a systematic review on the medical treatment of UAVM (32 studies, 121 women) was published, presenting an overall success rate of 88%—a figure similar to that obtained in our systematic review with embolization [
8]. This review included studies with a definition of UAVM that relied on the investigators’ individual description and a transfusion rate of 2.5% after initiation of medical therapy. However, in our work, the included studies were selected after the gold standard diagnosis of UAVM by angiography and there was a 20% transfusion rate. With these data, it is confirmed that the clinical severity of the patients and their heterogeneous selection mean that they are not comparable populations. Although both treatments are a fertility-sparing option, medical treatment would be useful in stable patients with minimal bleeding, while UAE remains the treatment of choice in patients who are hemodynamically unstable or have significant uterine bleeding. The vast majority of patients with UAVM included in our review had a more-or-less recent obstetric history, with abortion treated by curettage being the most common. This is clearly in line with what has already been published in previous systematic reviews [
10,
14]. Some authors comment that hormonal changes associated with pregnancy may play a role in the proliferation of latent UAVMs through an unknown mechanism [
10,
15], but the variables that would allow us to identify patients with a higher risk of developing a UAVM, to perform an early and close follow-up to avoid the associated complications, are unknown. The general findings of our review indicate that in the event of abnormal uterine bleeding in a patient with a recent diagnosis of abortion or another obstetric event, we should rule out UAVM from among the possible diagnoses. Given that they have different management and treatment procedures, it is essential to make a differential diagnosis between acquired UAVM (currently called by many authors as enhanced myometrial vascularity (EMV) [
16]) and retained products of conception (RPOC). For this reason, works are emerging to help differentiate it by color Doppler ultrasound [
17], representing a non-invasive means of diagnosis and determination of management. However, most authors continue to consider angiography the gold-standard method for the diagnosis of UAVM and, therefore, we use this criterion to carry out the bibliographic search.
Despite the fact that EMV is the term used recently to describe acquired UAVM, most authors continue to refer to the UAVM name in their works. For this reason, we believe that not including this term in our bibliographic search could have minimally affected the collection of articles.
Thanks to the data collected in our review that confirm a rate of major complications of UAE of 1.6%, it can be stated that UAE is a very safe treatment for patients with UAVM. Other systematic reviews [
18,
19] analyzing the complications of UAE used as a treatment for other pathologies, such as postpartum hemorrhage, agree with the high safety of this treatment.
Despite the fact that many authors included in our systematic review did not document data on fertility after UAE for UAVM, we managed to collect 77 patients with documented pregnancy after UAE. Seventy-seven percent of pregnancies were uneventful, and elective or spontaneous abortion was the most frequently described gestational complication. The ischemic injury of the endometrium caused by UAE may play a role in subsequent pregnancy loss, although more studies would be necessary to confirm this association. Previous works have related UAE with an increased risk for placental abnormalities in subsequent gestations. Ref. [
20] (specifically placenta accreta) does not seem to be confirm the data collected in our work. Soro et al. [
21] indicated that UAE has no direct effect on the placental blood supply and fetal growth because the formation of collateral circulation develops very quickly after UAE. There are some studies suggesting a higher rate of infertility, premature ovarian failure, and uterine synechia [
22], but they present heterogeneous data and a small number of patients, so this association has a very low degree of evidence.
4.2. Strengths and Limitations
Our systematic review includes the largest sample of patients with UAVM treated by UAE to date with 95 studies (published from 2000 to 2021) involving 371 patients spread over all continents. Yoon et al. [
10] published a systematic review on this topic that included 40 studies (published from 2003 to 2013) with 54 patients. In our work, 62% of the included studies were published after 2013, which reflects the growing use and interest in this treatment in the literature and the need to update the data given the striking increase in articles in the literature. The greater number of patients in our review has allowed us to carry out a temporal and geographical analysis of the success rate of UAE, which has not been carried out in the literature to date. In the previous review, Yoon et al. performed a unilateral/bilateral analysis of embolization and embolic agents used and concluded that the published data is very heterogeneous (in terms of numerous combinations and options in embolic agent utilized, UAVM size, and clinical symptoms) and there were no significant differences in the necessity for repeat embolization. Nowadays, no controlled studies have been performed to evaluate the effectiveness of a unilateral versus bilateral treatment approach or comparing the efficacy of each embolic agent or combination of agents.
Given the rarity of UAVM, most of the studies identified were retrospective case report and case series studies of a few patients with mostly positive outcomes. Publication bias is very likely because small studies with negative results are often not published. The data included in the articles is very heterogeneous in terms of clinical scenario, embolic agent used, and unilateral or bilateral approach, making it impossible to carry out comparison studies to evaluate the effectiveness of different treatment approaches. In addition, the case series provide global data that prevent a detailed study of the cases. Although more evidence is needed on this topic with studies of higher methodological quality, the rarity of UAVM leaves study options limited, and reports such as ours are likely to be the highest available evidence from which to draw guidance for clinical decision making.


 ,
, 


{kind=link}